
How to Build an Agent-based Model to Assess the Impact
of Co-payment for Health Services
Angela Testi, Michele Sonnessa and Elena Tànfani
Department of Economics, University of Genova, Via Vivaldi 5, Genova, Italy
Keywords: Agent-based Models, Economic Simulation, Health Care Financing.
Abstract: Some forms of co-payment are required in insurance markets to avoid moral hazard that in health sector
entails excessive consumption and costs. Literature and empirical findings, however, do not agree about the
effectiveness of co-payment in practical situations. Moreover, in health systems co-payment seems to be
more aimed to help in financing than to reduce moral hazard. The final impact of co-payment is rather
difficult to predict due to these conflicting aims. Assessing the impact of a co-payment policy is, however,
very important, because it affects also the principles of universalistic health systems threatening equity
attainment. The specific aim of this paper is to propose an Agent-based simulation model that allows both i)
to take into account all these contradictory effects at the same time, ii) to compare different co-payment
models. The model development is presented mixing empirical data with some stochastic assumptions the
authors intend to test.
1 INTRODUCTION
Insurance companies use co-payments to share
health care costs and prevent moral hazard, that is
post contractual opportunistic behavior to transfer
more risks to insurance company. In absence of
some co-sharing tools, this behavior leads to
inefficient situations, excessive consumption and
higher costs. Though co-payment is often a small
portion of the actual cost of the medical service, it is
meant to prevent people from seeking medical care
that may not be necessary. The underlying
philosophy is that with no co-payment, people will
consume much more health care services than they
otherwise would if they were paying for all or some
of them. Co-payment may, however, be ineffective
in presence of relevant Supply-Induced-Demand
effect, i.e. when services are not demanded directly
by the patient, but by the physician, acting as patient
"agent". In this case excessive consumption, due to
moral hazard, will not be reduced and even we could
predict a further increase (Ellis and McGuire, 1993).
However, also in case of moral hazard reduction, the
crucial issue is that co-payment should reduce only
not essential consumption, without discouraging
people from seeking necessary medical care. This
can be done, applying co-sharing measures (e.g.
tickets or ceiling, or caps) on more elastic
consumption items.
The above described mechanism is, however,
based only on a theoretical model. From an
empirical point of view, co-payment acts as a
rationing device preventing access to care in
universalistic systems as literature shows (Louckx,
2002). And even if no definite result is given, many
empirical papers, from the more complete and cited
(Manning et al, 1988), predict effects of
consumption restriction of the more frail and
deprived people, engendering negative effects on
their health status. It seems that co-payment gives
rise to the classical trade-off between equity and
efficiency, where the only demonstrated effects are
the negative ones on equity, because gains in terms
of efficiency and cost containment are not clearly
verified by empirical literature (Carrieri, 2010).
What makes things more difficult is, however,
that in practical application, co-payment is not
utilized, as theory prescribes, to reduce moral
hazard, but almost exclusively as a tax to finance
public budget. This is, however, a practical aim
opposite to the theoretical one, entailing that to be
more effective, co-payment should not change
consumption, which is exactly the opposite of co-
payment intended to reduce moral hazard.
If co-payment should improve public balance, it
should be imposed on the "less" elastic items, not to
556
Testi A., Sonnessa M. and Tànfani E..
How to Build an Agent-based Model to Assess the Impact of Co-payment for Health Services.
DOI: 10.5220/0004166205560563
In Proceedings of the 2nd International Conference on Simulation and Modeling Methodologies, Technologies and Applications (HA-2012), pages
556-563
ISBN: 978-989-8565-20-4
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

the "more" elastic ones: this means on the more
essential services, the ones that patient do not reduce
even if their price increases. In this case negative
effects on equity are still larger, because being a
form of financing not linked to the ability to pay, but
rather to the use of services, it requires greater
contribution from the least well-off (Wagstaff et al.,
1999), even if to attenuate partially this undesirable
effect some exemption rules are usually
implemented.
As far as we know the impact on the public
budget of the introduction of a co-payment system
has never been studied in detail, nor who bears the
greatest disadvantage. We can predict that as co-
payment is perceived as a price by the patient, a
price increase means reducing demand, but how
much demand reduces depends on elasticity.
Following traditional microeconomics, we know that
elasticity depends on price effect, which, in its turn
is composed by a substitution and an income effect.
The first effect depends on how many substitutes
exist, while the income effect on how large the
income is in absolute term and how large health
expenses are in relative term with respect to other
goods. If the aim is to finance health services, co-
payment should be applied to services with a rigid
demand, that is were no substitution effect exists and
health expenses are high during a year, for instance
in chronic conditions. This is, of course,
contraindicated for equity, so, before recurring to co-
payment in universalistic systems, decision makers
should know in advance: i) whether increasing co-
payment will make people reduce their demand for
services and / or getting no consistent fiscal return
and ii) what is the best exemption structure to
correct excessive payment from chronic or deprived
patients.
In particular, since 2000, the Italian experience,
developed in some different ways following the
regional policies, includes diverse experiences of co-
payment on drugs, diagnostic and specialist visits,
differently designed in the Italian regions. From a
point of view aggregate and almost exclusively for
drugs there are some data showing what has been the
impact (http://www.agenziafarmaco.gov.it/it/content
/osservatorio-sull%E2%80%99impiego-dei-medici
nali-osmed). Data on specialist visits, diagnostic and
revenue that has been obtained during the years are,
however, missing, even if some preliminary
information were given during a national Conferen-
ce in Rome, last May (http://www.agenas.it/agenas_
pdf/Dossier%20Co-payment_aprile2012.pdf). The
same happens for the effects on different categories
of exempt people. In this research still in course, it
appeared that, generally, the patients who cannot
profit by exemption consume less medicines,
diagnostic and specialist visits than the exempted
ones. From this strong, and not yet published
evidence of under treatment, the empirical aspect of
this study took start.
In this paper, we propose an Agent-based
modeling framework aimed at investigating the
effects of different co-payment rules.This model can
represent a useful support to decision makers,
increasing the capacity to control the adverse
consequence of co-payment on equity of access.
The reminder of the paper is as follows. In
Section 2 an agent-based simulation model is
described intended to be a tool for better decision
making about definition of more effective co-
payment policy. Section 3 provides an overview of
the LigurNet database the model is built upon.
Section 4 indicates conclusion and further work.
2 AGENT-BASED MODEL
In economic research increasing attention is given to
agents' characteristics and their interaction to
determine aggregate results. This is crucial in
complex situation as co-payment is. Since it is
impossible to verify single economic theory, agent
based models seem to be preferable because they
can predict the results of conflicting aims and
behaviors. Aggregate levels of the main decision
variables, such as total expenditure, co-payment
returns, consumption, and so on, are derived starting
from the individual behaviors.
In fact, as stated in Ostrom (1988), and to some
extent in Gilbert and Terna (2000), computer
simulation can combine the extreme flexibility of a
computer code where we can create agents who act,
make choices, and react to the choices of other
agents and to the modifications of their environment
and its intrinsic computability.
Economic policy advice requires a thorough
understanding of the relevant individual choices that
are responsible for the effects of policy measures in
the economy, as well as in the public health system.
Theoretical work based on certain model
structures accompanied by empirical evidence aims
at giving us guidance on the causal relationship of
key economic variables.
Agent-based models can improve the
possibilities of a modeler to capture economic
phenomena that seem relevant to policy makers and
extend the set of questions that can be asked about
policy effects.
How to Build an Agent-based Model to Assess the Impact of Co-payment for Health Services
557
The choice of agent based paradigm for studying
the co-payment system is mainly due to two reasons:
its algorithmic flexibility and the need for a
multilevel interaction.
The rules to value the co-payment of each
prescription are based on algorithms and legislators
often change them deeply. So in order to effectively
adapt the model to different co-payment scenarios,
we opted out for the agent based modeling
technique. Moreover, we are interested in
understanding how interaction phenomena can affect
the individual choices, in terms of selection of public
or private health provider by citizens. As also stated
in Howitt et al. (2008), an agent-based model is a
way to create virtual worlds that can be used as test
beds to study macroeconomic phenomena,
considering interactions among agents
simultaneously with agent decisions.
2.1 General Structure of the Model
The Agent-based modeling is a strongly micro-
founded approach to study economic dynamics. It is
interested in detecting the patterns at aggregated
levels of analysis that origin from the interaction of
agents, who follow particular behavioral rules and
may be constrained in their choices by various
institutional arrangements.
Nevertheless, the aggregate behavior of the
system can be well depicted in terms of cause-effect
structure, where the final result depends on agents
characteristics, their incentive design mechanism
and co-payment structure.
The agent-based model introduced in present
work is aimed at modeling individual behavior and
interactions among three classes of agents (patients,
physicians and public decision-makers). The general
macro structure of the model can be described by the
cause-effect diagram in Figure 1.
The model controls three relevant variables:
public budget, prescription level and co-payment
level.
Public Budget depends on prescription level and
is defined by two tools: "moral suasion" exerted by
Health Authorities on physicians" and "co-payment
level". It represents the key driver in the policy
maker decision function.
Prescription Level depends on the behavior of
two agent types: the physician (propensity to
prescribe) and the patient rate of demand for
prescription. The level of prescription determines
both the public budget level as well as the patient
utility.
Co-payment Level depends on the policy maker
decision, taking into account public budget as
budgetary constraint and the patient utility, as
directly connected with public consensus. Given the
health status of the patient, the co-payment level
determines the propensity to demand health services;
the difference between what the patient expects on
the basis on his health status and what the doctor
prescribes determines the patient utility.
The patient utility depends on the number of
prescriptions requested (the so called "expressed
demand"), following their perceived "want", and on
the number of prescriptions really delivered by
physicians, following what they think is the patient's
"need" (Culyer and Wagstaff, 1993).
Public
balance
Moral
suasion+
Prescription
propensity
-
Prescription
demand rate
Prescriptions
+
+
Co-payment
Prescription
demand propensity
+
+
-
Patient
utility
+
-
+
Patient
expense
-
+
Figure 1: Cause-effect diagram.
SIMULTECH 2012 - 2nd International Conference on Simulation and Modeling Methodologies, Technologies and
Applications
558
2.2 Model Implementation
The model is closely linked to a large empirical
dataset (see Section 3), so it has been implemented
in native Java language using JAS libraries
(described at http://jaslibrary.sourceforge.net). This
choice grants an efficient interaction with the
database, containing the population and the
prescriptions of the last ten years. In fact, as stated in
Boero and Squazzoni (2005), "...attention has been
paid to the need of integrating ABMs (and
simulation models generally speaking) and methods
to infer data from empirical reality, such as
qualitative, quantitative, experimental and
participatory methods […]. The link between
empirical data, model construction and validation
needs to be thought and practicised as a circular
process for which the overall goal is not merely to
get a validation of simulation results, but to
empirically test theoretical mechanisms behind the
model. Empirical data are needed both to build
sound micro specifications of the model and to
validate macro results of simulation. Models should
be both empirically calibrated and empirically
validated. This is the reason why we often enlarge
our analysis to the broader quest of the use of
empirical data in ABMs, with respect to the narrow
quest of the empirical validation".
The approach we follow in implementing the
model consists in utilizing both current empirical
data and integrating them with strong hypothesis for
variables that cannot be directly observed from
available data.
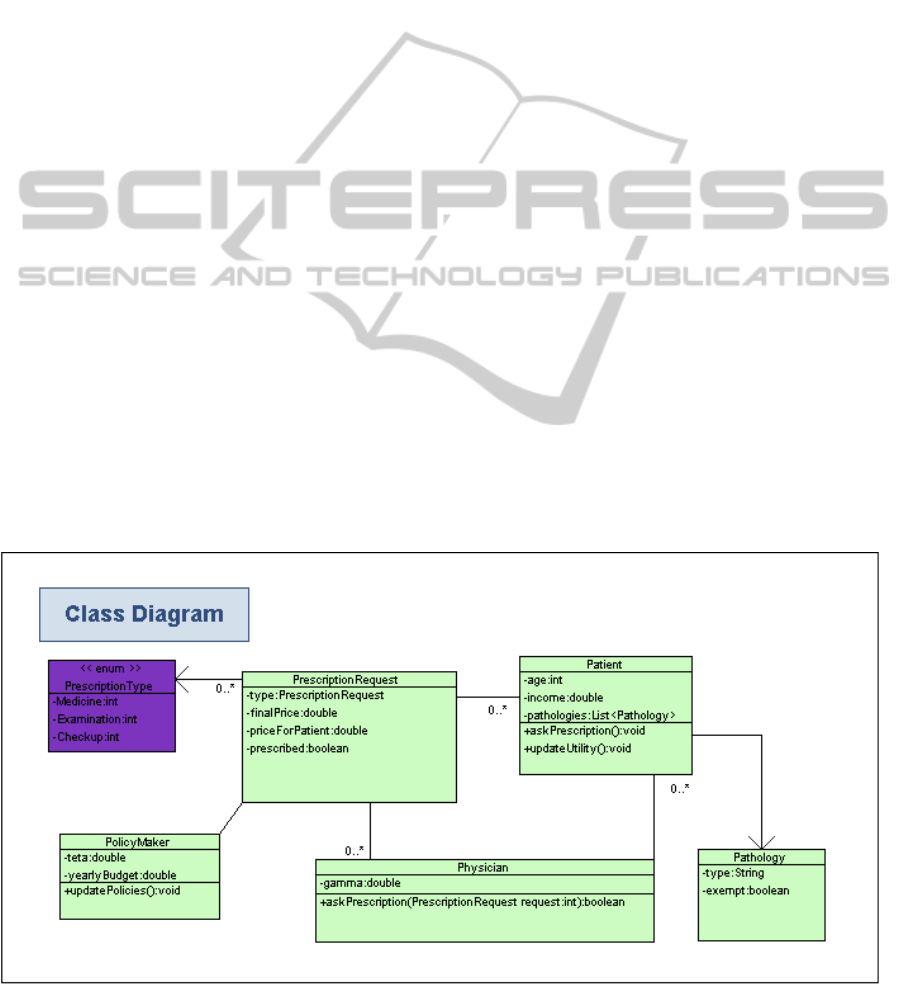
According to the methodology proposed in
Richiardi et al. (2006), the general structure of
classes, entities and schedule is represented in terms
of class diagram (Figure 2) to represent the agent
characteristics as well as the information/documents
they create and exchange and in terms of time-
sequence diagram to describe when things happen
within a simulation experiment (see Section 2.3).
Taking into account the general structure of the
model, three classes of agents are introduced. The
characteristics and properties of each agent class are
described in the next subsections. The model also
defines the list of the patient’s pathologies with
corresponding exemptions if any and a collection of
PrescriptionRequests, i.e. objects that trace the
lifecycle of a single prescription request, to collect
aggregate variables such as patients’ utility, patient
expense and general regional expenditure.
The prescription request object is characterized
by the following properties:
Prescription type (Medicine, Specialist Visits,
Exams and controls);
Final price for National Health Service;
Price for patient (taking into account co-
payment amount);
Prescribed (boolean value).
Moreover, the following general parameters are
defined:
Number of patients;
Number of physicians;
Co-payment level and design (e.g. fixed
amount, percentage of the price of the service,
Figure 2: Class diagram of the model.
How to Build an Agent-based Model to Assess the Impact of Co-payment for Health Services
559

ceiling, etc.)
Income distribution of patients.
: it is a parameter of the patient: it defines the
share of health spending relative to income,
which represents utility of 0. In other words, it
is the sum of what has been paid within a year
compared to one's income that is considered
acceptable. This coefficient is assumed to be
equal for all patients.
m
is a parameter of the physician. It represents
the tendency to meet patient demand for
prescription.
2.2.1 Patient Agent Class
Every patient agent is characterized by following
own properties:
Age [E];
Income [R];
Pathologies [M];
Exemptions [Me];
We assume that agents require prescriptions
depending on their health status (i.e. the number of
pathologies directly influences the number of
required prescriptions) and their level of income.
The individual demand function, for a given class of
patient age and health status, has the form shown in
Figure 3.
Figure 3 Individual demand function.
For different combinations of ages and number
of pathologies we can define different demand
functions and test their correspondence in empirical
data.
The demand for prescription depends on: i) the
health status (proxied by the number of pathologies)
which is introduced into the model using empirical
data and can change over simulation time; ii) the
yearly income.
The particular form of the demand curve
depends on the trade-off between the two
components: the level of pathologies increases the
prescription demand, while the level of income
decreases it, since rich people are supposed to use
more private health services than poor ones. The
position of the demand curve depends on the
individual exemption regime: different exemption
facilities may have different impact on the individual
income and, therefore, at parity of total income
increase or decrease the number of required
prescription (shift the curve upwards or downwards),
given the same health status.
Every simulated year, agents compute their own
utility level, depending, negatively, on the
expenditure and, positively, on the prescriptions
received by the physician. More in detail, the utility
level for patient i at time t is computed by the
following equation:
rp
rqop
X
U
i
i
t
i
t
(1)
Note that, the utility is made up of two components:
the difference between
(percentage of health
expenditure, giving a null level of utility) and
the individual expenditure quota for health
services, computed as the ratio between
j
i
t
PX
, where P
j
is the price paid for
prescription j by patient I, and the total income
i
of patient i;
the percentage difference between the obtained
prescriptions (op). and the requested ones (rp).
The price P
j
is intended as the final price for patient,
including the effect of co-payment and exemptions.
We assume that, the percentage does not depend
on the individual level of income. Moreover, it
possible to relax this assumption and modeling the
relationship between the parameter and the
individual income. On the contrary, patient
behaviour evolves over simulation time, since its
status in terms of pathologies and exemptions can
change over time.
The agent population is built from empirical data
collected in the GP LigurNet database (see next
section for detailed description). The data set
provides identities of agents, with the list of
pathologies and exemptions they obtained in the
past. Unfortunately, the income level is not available
in database, so it is randomly assigned by the
simulation model based on a normal distribution
according official data of ISTAT Multiscopo Survey
(www.istat.it) and Banca Italia Survey on Income of
the Italian families (www.bancaditalia.it/statistiche
/ibf).
At each simulation step, the agent decides if a
SIMULTECH 2012 - 2nd International Conference on Simulation and Modeling Methodologies, Technologies and
Applications
560
new prescription should be asked to its physician.
This choice is mainly driven by the empirical
dataset. The prescription request is communicated to
the patient’s physician and internal accounting is
modified according to its response.
2.2.2 Physician Agent Class
Physician is characterized by the tendency to go
along with patient demands [
m
]. The agent is able to
react to patients’ prescription requests. For each
request, the physician has to decide if to prescribe it
or not.
Prescription rate depends on physician individual
tendency to go along with patient requests, affected
by general level of moral suasion coming from the
policy maker. For each prescription request a
uniform random sample is generated in the range
[0,1]. If the sample is greater than the threshold
level, computed as
m*
, the prescription is granted.
The
m
parameter is introduced according the
principle of “defensive medicine” leading to
"supply-induced demand": the physician generally
tends to give into patients requests, to avoid legal
risks. This phenomenon is modified by moral
suasion level applied by legislator. We assume that
physician behaviour does not evolve over simulation
time. The individual values of the
m
parameter are
randomly generated from a normal distribution.
Physician agents react to external stimuli. In
particular, they are waiting for patients’ requests and
decide if according them or not. This
implementations reflects real physician strategy. In
fact they respond to the so called “waiting medicine”
criteria. They are not supposed to be active in
contacting patients and stimulating care.
2.2.3 Policy Maker Agent Class
The policy maker represents a single agent instance
able to influence the whole system with its actions.
It modifies its choices observing aggregate
endogenous variables deriving from other agents’
behaviour, in particular by the patients’ utility.
Policy maker is characterized by own following
properties:
yearly budget [B];
moral suasion level [].
In the first version no evolutive behaviour are
provided. This means that Policy maker does not
change its parameters during each simulation run.
Different parameter combinations are tested
comparing different simulation run outcomes.
Through the collection of system responses to
changes in policy parameters, we can provide a
sensitivity analysis of the key variables the policy
maker can act upon, to reduce public expense and
increase overall patients’ utility.
It the first model configuration policy maker is
characterized by a fixed behaviour which is initially
determined as a simulation parameter. Future model
improvements should take into account the
possibility that policy maker’s choices, in terms of
moral suasion and co-payment, can change over
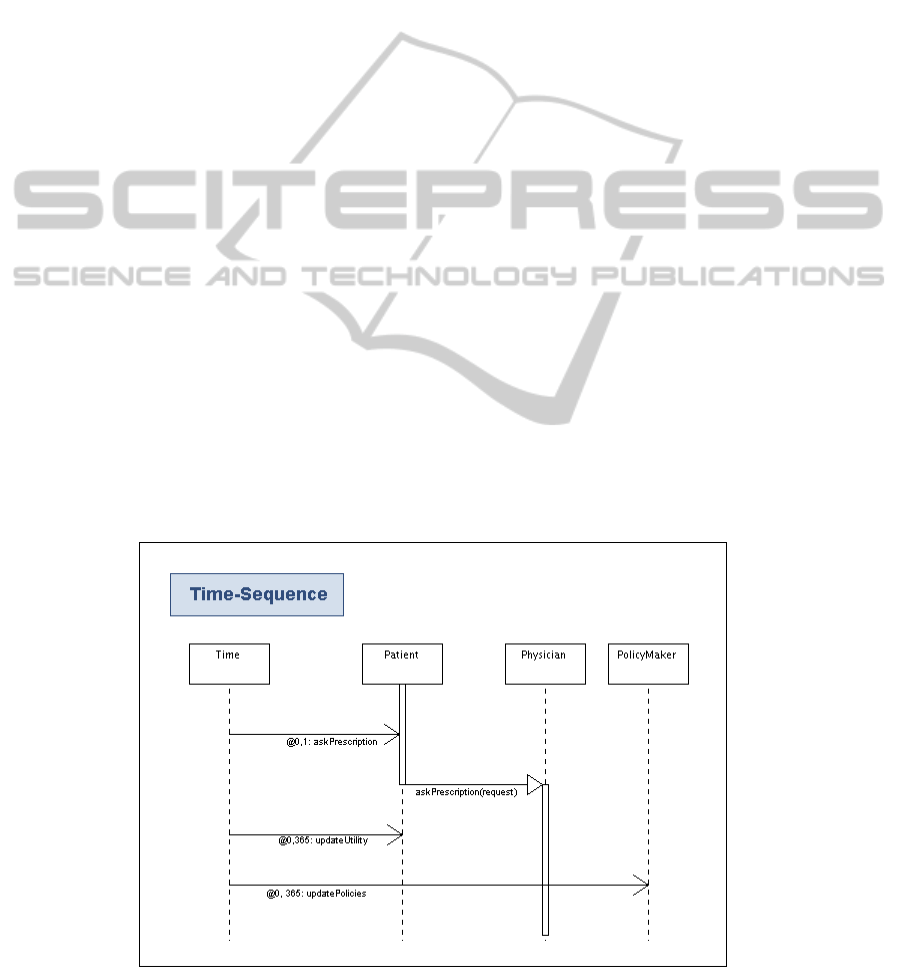
Figure 4: Time-sequence diagram of the model.
How to Build an Agent-based Model to Assess the Impact of Co-payment for Health Services
561

simulation time according to balance trends and
aggregate patient utility.
2.3 Simulation Time Schedule
The dynamic of the model (Figure 4) is trivial. For
each simulation step all patients decide whether to
require a prescription, according the general
probability and their own individual characteristics.
In case a request is generated it is processed by the
physician, who can approve it or not.
Every simulated year of simulation, the model
updates the statistics and eventually asks the policy
maker to guess changes in regulation.
3 DATA COLLECTION
As said above, the model is closely linked to a large
empirical dataset available thanks to the
collaboration of GP-LIGUR.net, the Primary care
Observatory of Regione Liguria, collecting clinical
and prescription data of 188,568 citizens, by 134
physicians for the period June 2000-June 2011.
In Italy to accede the second and third level of
publicly delivered care, the prescriptions of family
doctors, or General Practitioners (GP), are required.
They record prescriptions by using the same
software (www.Millewin.it). Even if the registration
does not constitute compulsory information debt by
GP, therefore, the database is a huge mine of
information, that until now, have never been used by
policy makers. Moreover, data are particularly
valuable as it is possible to build the history of every
patient, which is important for implementing our
model.
The original database was corrected according to
quality requirements following a set of indicators
fixed with the help of the physicians. This meant
reducing the number of doctors from 134 to 81 and
the prescriptions from about 37 millions to about 12
millions.
3.1 Methodology of Data Extraction
Three groups of pathologies were taken into
consideration.
Oncological diseases - breast K, K prostate
Chronic cardiovascular and metabolic diseases
Depressive syndromes
The first two groups (oncologic and
cardiovascular) may give right to exemptions from
ticket payment in particular conditions of income
and age, as specified in (Table 1), that are a mix of
income, age, and pathology conditions. The third
group, is a chronic pathology not recognized by
exemption rules except for a tiny subgroup
(psychosis).
Note that exemption conditions reported are the
ones currently applied in Regione Liguria. Italian
citizens, in fact, can benefit of different conditions
depending on which Region they live (Il
sole24oreSanità, 2012).
3.2 Database Role for the Model
The database allows to define a population of agents
characterized by all those properties that are
important for the construction of the agent-based
simulation model. In particular, the propensity to
demand prescription of patients, the exemption
choices that reduce the expected return from co-
payment, the prescription policy of the physician
and so on.
From a first inspection of database, we can
affirm that current situation is affected by a deep
iniquity that should be corrected. There is strong
evidence, for instance, of "foregone" care at the
expenses of not exempted. The last have
systematically less access to essential care. This is
particularly serious for cancer patients, who require
maximum adhesion to treatment and could, in the
event of noncompliance, have an immediate and
serious impact on their health. It is, however, serious
also for chronic cardiovascular and metabolic
Table 1: The current situation of exemption in Regione Liguria.
POOR: Family income <36.150 Euro
RICH: Family income >36.150 Euro
YOUNG: age <65
Co-payment is due on every prescription
Co-payment is due on every prescription
OLD: age > 65
No co-payment on every prescription
Co-payment is due on every prescription
ILL+YOUNG: Recognized chronic pathology and
age < 65
No co-payment on every prescription
Co-payment is due only on drug.
No co-payment on specialist and exams
ILL+OLD: Recognized chronic pathology and age
> 65
No co-payment on every prescription
Co-payment is due on every prescription
SIMULTECH 2012 - 2nd International Conference on Simulation and Modeling Methodologies, Technologies and
Applications
562

diseases, even if as we expect that patient affected
by the three prevalent chronic diseases (diabetes,
hypertension and ischemic heart disease) are less
adherent with respect to the first group as they may
perceive their pathology less important than cancer.
In addition, with regards to this third group, the
database proves large undertreatment, which
indicates that probably most of them exit the public
system, given that they not only cannot be exempted
but also they are consumer of class C drug (that is
not supplied free by NHS). We can imagine that a
further utilization of the model could be assessing
the impact on public budget of enlarging the list of
the recognized chronic pathologies. At present, there
are, due to population aging, other pathologies that
could be included, such as, for instance, depression,
arthritis, venous insufficiency.
4 CONCLUSIONS AND FUTURE
WORK
In this paper we argue that agent-based modelling
applied to policy making in the public health system
needs a methodological protocol allowing to mix
empirical data with theoretical assumptions about
individual behaviour and preferences.
In this respect, we wish to introduce formalised
approach to mix behaviour modeling, real data
coming from regional health system and co-payment
rule algorithms into an agent based model.
The approach is aimed at showing that feeding a
model with empirical data can improve the
awareness and guide policy makers towards better
choices in terms of co-payment rules, as well as,
connect the model more closely to the real world
that it intends to simulate.
In further research, we plan to computationally
develop the prototype and use the appropriate
techniques to explore changes into the structure of
the prototype, in order to find more deep theoretical
insights and validate assumption about correlation
between patient income and their behavior in terms
of exemption and the possibility they look at private
health system.
Throughout an appropriate validation of
individual behaviour, more reliable assuptions about
the right co-payment system can be provided.
ACKNOWLEDGEMENTS
We wish to thank GP Ligurnet and, in particular, Dr
Pierclaudio Brasesco for collaboration in supplying
data. All the authors participate and acknowledge
support from the Italian Ministry of Education,
University and Research (MIUR), under the grant n.
RBFR08IKSB - FIRB PROJECT.
REFERENCES
Boero, R. and Squazzoni F. (2005). Does Empirical
Embeddedness Matter? Methodological Issues on
Agent-Based Models for Analytical Social Science.
Journal of Artificial Societies and Social Simulation,
8(4). Retrieved from: http://jasss.soc.surrey.ac.uk/8/4/
6.html.
Carrieri, V. (2010). The Effects of Cost-Sharing in Health
Care: What Do We Know From Empirical Evidence?.
Economia Politica:Journal of Analytical and
Institutional Economics, 27(2), 351-374.
Culyer, A. J. and Wagstaff, A. (1993), Equity and equality
in health and healthcare. Journal of Health Economics,
12(4), 431-457.
Ellis, R. P. and McGuire, T. G. (1993). Supply-Side and
Demand-Side Cost Sharing in Health Care. The
Journal of Economic Perspectives, 7(4), 135-151.
Gilbert, N. and Terna P. (2000). How to build and use
agent-based models in social science. Mind & Society,
1(1), 57-72. http://www.agenas.it/agenas_pdf/Dossier
%20Co-payment_aprile2012.pdf
Howitt, P., Kirman A., Leijonhufvud A., Mehrling P. and
Colander D. (2008). Beyond DSGE Models: Toward
an Empirically Based Macroeconomics. Middlebury
College Economics Discussion Paper No. 08-08.
Il sole24oreSanità, (2012), Focus, 24-30 april 2012 -
pp.11-15- and 17-23 april 2012- Focus pp 9-13
Louckx, F. (2002). Patient cost sharing and access to
healthcare. In Mackenback J., and Bakker M. (eds),
Reducing inequalities in health. A European
perspective. London: Routledge, pp 188-198
Manning, W. G., Newhouse, J. P., Duan, N., Keeler, E. B.,
Benjamin, B., Liebowitz, A. et al. (1988). Health
insurance and the demand for medical care. Evidence
from a randomized experiment. Santa Monica, CA:
RAND Corporation, 1988. Report R-3476-HHS. ISBN
0-8330-0864-1. An abridged version of this report.
was published in Manning, W.G. et al.(1987) Health
insurance and the demand for Medical Care: evidence
from a randomized experiment. American Economic
Review, 1987, 77, 3:251-277
Ostrom, T. (1988). Computer Simulation: the Third
Symbol System. Journal of Experimental Social
Psychology, 24, 381-392.
Richiardi M., Leombruni R., Saam N. and Sonnessa M.
(2006). A Common Protocol for Agent-Based Social
Simulation. Journal of Artificial Societies and Social
Simulation, 9(1). Retrieved from http://jasss.soc.
surrey.ac.uk/9/1/15.html
Wagstaff A. et al. (1999). Equity in the finance of health
care: some further international comparisons, Journal
of Health Economics, 1999, 18, 3:263-290.
How to Build an Agent-based Model to Assess the Impact of Co-payment for Health Services
563
