
Process-oriented Home Care System Transformation
in Central Finland
Jing Tang
1
, Toni Ruohonen
2
, Junichi Iijima
1
and L. G. Pee
1
1
Department of Industrial Engineering and Management, Tokyo Institute of Technology,
2-12-1 Ookayama, Meguro-ku, Tokyo, Japan
2
Agora Center, University of Jyvaskyla, Mattilanniemi 2, Jyvaskyla, Finland
Keywords: Business Process Modeling, Central Finland, DEMO, Home Care.
Abstract: Due to aging population and rising expenses in health care, Central Finland’s local governments and author-
ities are increasingly promoting home care rather than relying solely on institutional care. To increase the
adoption of home care, it is necessary to create a mutual understanding of the current home care system, and
to improve the cooperation of stakeholders. From the process perspective, after analysing 6 related organi-
zations in Central Finland, this study created a general model of the current home care system in Central
Finland by using DEMO Construction Model, and pointed out several problems in its real implementation.
This study demonstrates that DEMO is applicable to the examination of essential processes in health care
systems and can offer suggestions for improvement.
1 INTRODUCTION
The trend of aging population creates increasing
demand for various resources in a healthcare system
such as financial resources, staff, and facilities.
However, the limited capacity of nursing homes and
hospitals does not allow a universal coverage of in-
stitutional care, even in developed countries. There
are also many senior citizens who prefer to live at
home together with families, or even alone. Home
care is therefore becoming an alternative to institu-
tional healthcare. However, seniors in home care are
often monitored less closely and they often face
higher risks of falls, strokes, and heart attacks. It
calls for a relative system transformation to support
home care, especially the caring relationship be-
tween care professions and the aging people even at
their home.
In Finland, local governments manage health
care system. As Central Finland is sparsely populat-
ed, healthcare facilities are often located far from the
patient’s home and are not well equipped. Moreover,
Finland is experiencing the problem of aging popu-
lation (CIA, 2012), because of low birth rate and
increase of life expectancy (Kunz, 2007). Therefore,
it is vital to improve the effectiveness of healthcare
and reduce the burden on institutional healthcare.
The municipal authority of health care is aiming to
increase the usage of home care to cover 90% of the
domestic aging people. In this study, we selected
DEMO (Design & Engineering Methodology for
Organization) to create a general model for home
care system in Central Finland. Based on it, we iden-
tified areas for improvement in the current imple-
mentation and provide suggestions for home care
system transformation.
2 DEMO
Design & Engineering Methodology for Organiza-
tions (DEMO) is a cross-disciplinary method that is
used to studies communication, information, and
action within the context of an organization, based
on PSI-Theory (Dietz, 2006). Unlike previous meth-
odologies, DEMO considers communication as links
to connect processes within or across organizations.
DEMO is used in this study to describe authority and
responsibility of abstracted actor roles, create a mu-
tual understanding of business processes among the
stakeholders, and compare similarities and differ-
ences of organizations. Comparing with other busi-
ness process models, DEMO base on ontological
modelling and has no limitation of requirement for
detailed information in the implementation level. In
addition, DEMO has also been applied to the domain
455
Tang J., Ruohonen T., Iijima J. and Pee L..
Process-oriented Home Care System Transformation in Central Finland.
DOI: 10.5220/0004179704550460
In Proceedings of the International Conference on Knowledge Engineering and Ontology Development (SSEO-2012), pages 455-460
ISBN: 978-989-8565-30-3
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

of healthcare in prior studies such as Habing et al.
(2001), and Maij et al. (2000).
Based on Dietz (2006), DEMO contains methods
for developing ontological models. The ontological
aspect models consist of Construction Model (CM),
Process Model (PM), Action Model (AM), and State
Model (SM), which are highly correlated and inter-
dependent. The CM explains the identified transac-
tion types and their tree logic, as well as the associ-
ated actor roles. It defines the authority and respon-
sibility of actor roles. The CM is also the most basic,
concise and easy-to-understand model among the
four aspect models. It is widely used in previous
case studies and business consulting.
3 CASE STUDY BACKGROUND
In Central Finland, while the population is more than
270 thousands, 17.8% are aging people (i.e., >65
years old). The ratio of healthcare staffs to the popu-
lation is only 1%. As a rule, the national health in-
surance, provided by KELA (Social Insurance Insti-
tute of Finland), basically covers all permanent resi-
dents of Finland, but Finnish health care system has
been criticized for being inefficient due to the exces-
sive number of units, health centres, hospitals, diag-
nostic services, and the density of administrative
units in the system (Kokko, 2009). Health care is a
critical and expensive service managed and financed
by local municipal authorities. They decide domestic
basic rules and laws. And they are also main contac-
tors to access health care services under the cover-
age of national health insurance. Most of public
health care institutions (e.g., hospitals, nursing
homes, and home cares) are sub-organizations of
municipal authorities. Nowadays, private health care
gradually becomes the alternative to overcome the
limitation of service availability from the public sec-
tors.
In Central Finland, home care services under
the coverage of national for demanders need to ap-
ply from the municipal authority of health care. Its
main responsibility is to establish a home care policy
(e.g., period, basic services, devices, potential care-
giver list, and fee) according to the health and living
situation of demander, together with the local annual
budget for home care. After that, a home care care-
giver (public or private) from potential caregiver list,
selected by the demander, will execute the home
care policy.
4 RESEARCH DESIGN AND
ANALYSIS
4.1 Research Design
In order to create a general model for home care
system in Central Finland, we mainly studied six
related organizations (one municipal authority of
health care, three public home cares, and two private
home cares), based on interviews and document re-
views. In each organization, we interviewed two to
three managers, team leaders and key staffs about
key business processes and their daily works. We
also matched the data from the interviews with the
provided documents. Interviews and documents are
mainly in Finnish, and cooperated Finnish research
team translated team into English. According to
these, we created CMs for each organization. Then,
by comparing the similarities and differences in
these six models, we generated the general CM for
the home care system. This general CM was final
validated by the Finnish research team and home
care workers. In next part of this paper, we describe
the general model by using Actor Transaction Dia-
gram (ATD) and Transaction Result Table (TRT).
TRT is considered from both ontological and im-
plemental level by including the real initiator and
real executor of each transaction.
4.2 General Construction Model for
Home Care System in Central
Finland
Figure 1 and Table 1 show the general CM for home
care system in Central Finland by demonstrating key
transactions, actor roles and information bask. Ac-
cording to the Finnish rule, it has been split into two
parts: (1) health care policy establishment, executed
by the municipal authority of health care; and (2)
home care policy execution, executed by a public or
private home care caregiver.
For the municipal authority of health care, the
whole process is started by the health care demander
(CA01), who is the aging people, requesting health
care policy establishment form the health care policy
establish manager (A01) by phone calls, emails, or
face-to-face visits. Moreover, other people, such as a
relative of the patient, social workers, and doctors
etc., can also contact the authority on behalf of the
patient in some cases. After received the require-
ment, for new demanders (CA01), the health care
policy establish manager (A01) will build a new
health care client account in the health care clien
KEOD2012-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
456
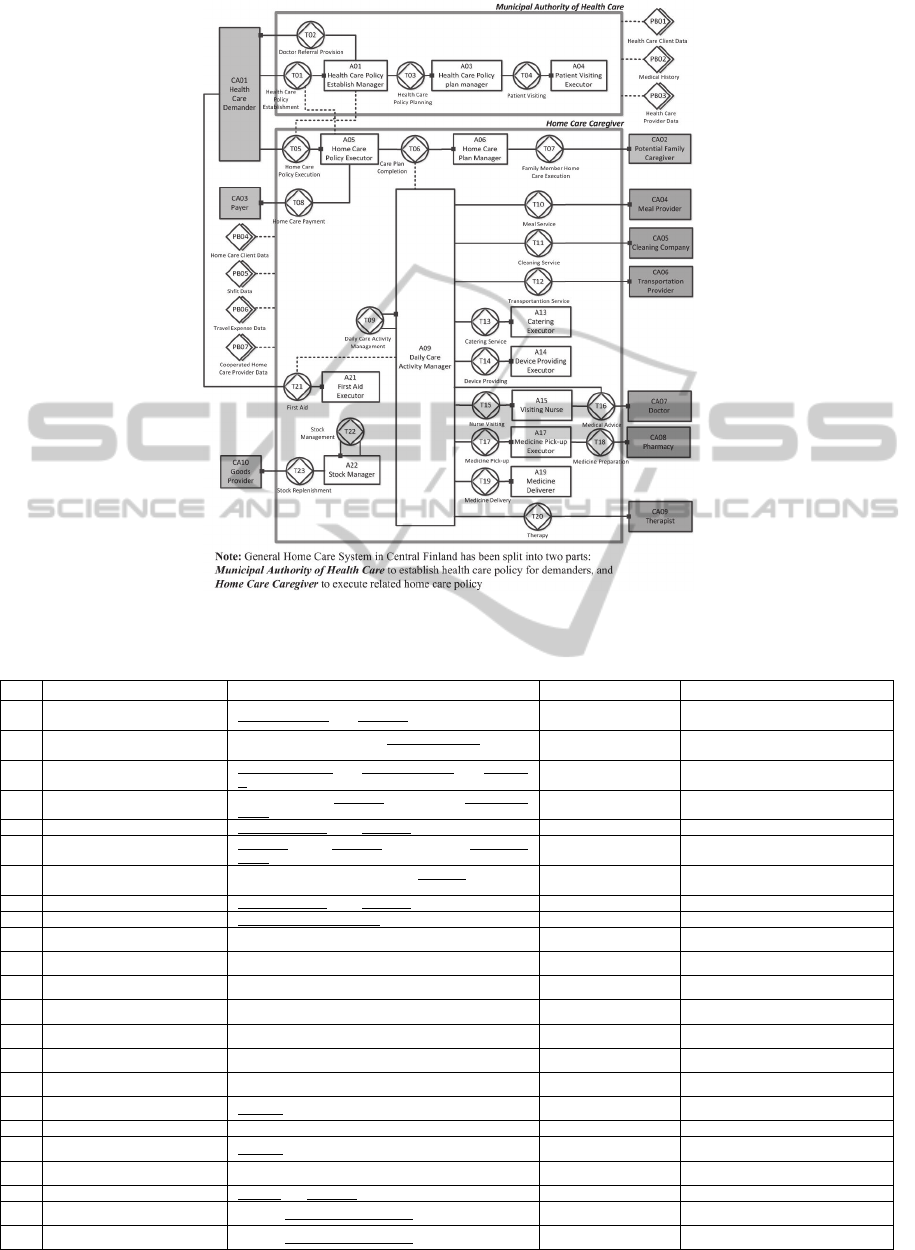
Figure 1: Action Transaction Diagram of Home Care System.
Table 1: Transaction Result Table of Municipal Authority of Health Care.
No Transaction Type Result Type Real Initiator Real Executor
T01 Health Care Policy Establishment Health Care Policy p for Demander d has been established
Demanders or Relative
or Social Worker etc.
Care Manager
T02 Doctor Referral Provision
Doctoral Referral to establish Health Care Policy p for has
been received
Care Manager Demander or Relative or Doctor
T03 Health Care Policy Planning
Special Care Policy sp in Health Care Policy p for Demand-
er d has been established
Care Manager Special Case Handler
T04 Patient Visiting
Patient visiting of Demander d to establish Special Care
Policy sp was finished
Special Case Handler Special Care Handler or other
T05 Home Care Policy Execution Home Care Policy hp for Demander d has been executed Demander or Relative Service Manager
T06 Care Plan Completion
Care Plan cp for Demander d according to Home Care
Policy hp has been completed
Service Manager Service Manager
T07
Family Member Home Care
Execution
Family Member Home Care care in Care Plan cp has been
executed
Service Manager Relatives or Neighborhood
T08 Payment Home Care Policy hp for Demander d has been paid Service Manager Aging People and Insurance Company
T09 Daily Care Activity Management Daily Care Activity Schedule s has been managed (Vice) Service Manager (Vice) Service Manager
T10 Meal Service Meal service has been provided
(Vice) Service Manager
Municipal Kitchen or other
T11 Cleaning Service Cleaning service has been provided
(Vice) Service Manager
Cleaning Company
T12 Transportation Service Transportation service has been provided
(Vice) Service Manager
Taxi Company or other
T13 Catering Service Catering service has been provided
(Vice) Service Manager
Nurse or other
T14 Device Providing Necessary device has been provided
(Vice) Service Manager
Nurse or other
T15 Nurse Visiting Nurse visiting has been provided
(Vice) Service Manager
Visiting Nurse
T16 Medical Advice Medical advice has been provided
(Vice) Service Manager
Doctor
T17 Medicine Pick-up Medicine m has been picked up from pharmacy
(Vice) Service Manager
Nurse or other
T18 Medicine Preparation Medicine m has been prepared Nurse Pharmacy
T19 Medicine Delivery Medicine m has been delivered to client
(Vice) Service Manager
Nurse or other
T20 Therapy Therapy has been provided
(Vice) Service Manager
Therapist
T21 First Aid First Aid f for Demander d has been provided Aging People Nurse (Day) Taxi Company (Night)
T22 Stock Management Stock for Stock Management Period st has been managed
(Vice) Service Manager
(Vice) Service Manager
T23 Stock Replenishment Stock for Stock Management Period st has been replenished
(Vice) Service Manager
Goods Provider
Process-orientedHomeCareSystemTransformationinCentralFinland
457

data (PB01) for them. If the necessary information
of personal medical history (PB02) and health care
provider availability (PB03) is not available, the
health care policy establish manager (A01) have to
request them from the information taker, on a case-
by-case basis. The doctor referral provision (T02) is
also required in some specific cases to check the
patient’s health condition. Based on all these infor-
mation, for a simple case or a temporary care case
that requires common health care package they have,
the health care policy establish manager can estab-
lish the health care policy (T01) directly. More com-
plicated cases are passed to the health care policy
plan manager (A03) for more detail health care poli-
cy planning (T03). If necessary, the health care poli-
cy plan manager (A03) may request a patient visit-
ing executor (A04) to visit the demander at home or
care institute (T04) to examine his/her actual health
and living situation. When the health care policy
establishment (T01) is completed, the health care
demander will be informed about the type and peri-
od of service he/she can receive, the potential pro-
viders, and the fee for the service.
According to the health care policy, if the policy
assigns the health care demander (CA01) needs
home care, he/she should select one of caregivers
from the potential providers list, and contact or meet
an officer there. The home care policy executor
(A05) will check whether the demander has com-
pleted the processes at the administrative office from
municipal authority of health care before executing
the home care policy (T05). The home care plan
manager (A06) will then be requested to complete
the care plan (T06) for demander. In some cases, the
home care plan manager may request potential fami-
ly caregiver (CA02), to execute the family member
home care (T07) at home. When the home care ser-
vice finished or the end of each month, the payment
(T08) is then paid by the payer (CA03) (e.g., insur-
ance company, and demander). For the daily job, the
daily care activity is managed (T09) by the daily
care activity manager (A09). Based on the daily care
activity schedule, the daily care activity manager
(A09) will assign the job to nurses or outsource the
job to other companies (e.g., meal provider, cleaning
company). Meal provider (CA04) serves meal (T10)
according to the request from the daily care activity
manager (A09). Cleaning service (T11) is done by
the cleaning company (CA05). When the aging peo-
ple need transport (e.g., shopping), transportation
provider (CA06) will provide transportation service
(T12) according to the booking appointment. The
catering executor (A13), who may be a nurse in pub-
lic home care or a non-medical worker in private
home care, executes the catering service (T13) such
as taking a shower for the aging people, feeding
food, and giving medicine, etc. Devices for aging
people such as forearm crutch, wheelchair, etc. are
provided (T14) will be delivered and set up by the
device providing executor (A14). The visiting nurse
(A15) does temporary or regular nurse visiting (T15)
to give medical checking and basic treatment for
demanders. If the health situation of a demander
changed, the home care workers need to contact to
the doctor (CA07) for medical advice (T16). In some
organizations, the visiting nurse (A15) will also reg-
ularly communicate the doctor (CA07). It can be
seen that most of the medical jobs are carried out by
the visiting nurse. Medicine pick-up executor (A17)
will go to pharmacy to pick up the medicine (T17)
for health care demanders. The pharmacy (CA08) is
responsible for preparing and packing the medicine
(T18). Then, the medicine deliverer (A19) will be
requested to deliver the medicine (T19) to the de-
mander. In most of cases, a nurse is assigned to de-
liver medicine when he/she provides other home
care services for the same demander. The cooperated
therapist (CA09) does the home visit therapy (T20)
for demanders when required. After all the home
care workers finish their job everyday, they have to
update client data (PB04) and report transportation
fee (PB06). In addition, most of home care demand-
ers will be provided an emergency alarm at home.
When there is any emergency case, the first aid ex-
ecutor (A21) will provide first aid service (T21) to
the health care demander (CA01), and then report
the result to daily care activity manager (A09). Dur-
ing the daytime, there are some nurses in charge of
picking up the phone call. But at the nighttime, the
first aid service (T21) is always outsourced to other
institutes, which provide 24 hours services, as the
private nursing home or the taxi company. The taxi
company will be called to send a taxi to the aging
people’s house. For the serious case, the taxi has to
go to the hospital to take the night nurse to the de-
mander’s house. The stock manager (A22) is in
charge to manage the stock of goods (T22), and or-
der goods from providers (CA10) to replenishment
the stock (T23). There are four information banks
inside: home care client data (PB04), shift data
(PB05), travel expense data (PB06), and cooperated
home care provider data (PB07).
In addition, in the implementation, a key differ-
ence between the public home care and the private
home care is that the private one tends to outsource
all medical services (T15, T16, T17, T18, and T19)
to others, as private clinics or private visiting nurses.
KEOD2012-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
458

5 DISCUSSIONS
In previous section, we identified the general model
of home care system in Central Finland based on
DEMO. It provides a mutual model for us to under-
stand the main transactions in the home care policy
establishment and execution, as well as their inter-
dependencies (illustrating by two information links).
In Figure 1, the information link from T01 to A05
refers to that health care policy establishment (T01)
in municipal authority of health care is the premise
for home care policy executor (A05) to provide
home care services to demanders. And the infor-
mation link from T05 to A01 demonstrates that
home care policy execution (T05) is critical re-
sources for health care policy establish manager
(A01) to follow up the current situation of demand-
ers to improve the health care policy.
5.1 Problems in the Implementation
One benefit of DEMO is to abstract essential trans-
actions and related actor roles in the ontological lev-
el, which define the authority and responsibility of
actor roles. In turn, it helps to assess the real imple-
mentation related to define and distribute responsi-
bilities across functions. In this part, using the vali-
dated general CM model as a stepping stone, we will
discuss several critical issues in the implementation
of the previous general construction model.
First, in the implementation, necessary infor-
mation related to one transaction can be provided by
the real initiator or found out by the real executor.
For the transaction, the home care policy execution
(T05), the initiator of this transaction is the home
care demander. Because of that the demander, espe-
cially aging people, is lack of capability to fully un-
derstand and explain the health situation of him-
self/herself, the executor, home care policy executor
(A05), has to find out information. Moreover, it is
also difficult for home care nurses to assess it from
the appearance and behavior of demanders. In addi-
tion, because of the security consideration and the
difference of e-health record system among organi-
zations, the exchanging of data across organizations
is difficult (Invest in Finland, 2011). So, before
promising the home care policy execution (T05), the
home care policy executor (A05) has to contact with
related information holders to access the data. It is
an extremely time consuming step in most of our
examples.
Second, as the general CM of home care systems
has been split out into two parts. Not only their sepa-
rated domain, a mutual understanding and definition
of their interdependency is also critical for the
alignment. However, it has been missed in the cur-
rent home care system of Central Finland. The in-
formation sharing efforts have not been standardized
and highlighted between the municipal authority of
health care and the home care caregiver.
Third, the home care demander can get the regu-
lar treatment and health checking from the visiting
nurses (A15) at home. For better service, the visiting
nurse (A15) needs to communicate with the doctor
(CA07). Currently, there are multiple ways as e-
mail, phone call, or the Pegasos, instead of face-to-
face visiting. Pegasos is a patient information system
widely used in Finnish public health care sector (In-
vest in Finland, 2011). However, because of the in-
charge visiting nurse and doctor are usually not
fixed for each home care demander, the transaction,
the medical advising (T16), is still full of challenges.
It needs to emphasize the responsibility of the visit-
ing nurse to initiate T16, and to develop better
methods and technologies for better health situation
control and more efficient communication between
the visiting nurse and the doctor.
Fourth, the process of delivering medicine (T19)
to the demander (CA01) seems to involve various
actor roles such as the medicine pick-up executor
(A17) and medicine deliver (A19). The long and
multi-actor process may increase the possibility of a
drug misadventure (i.e., (1) “an inherent risk when
drug therapy is indicated”; (2) “incident created
through either omission or commission by the ad-
ministration of a drug or drugs during which a pa-
tient is harmed”; (3) “incident whose outcome may
or may not be independent of pre-existing disease
process”; (4) “incident which may be attributable to
error, immunological response, or idiosyncratic re-
sponse”; and (5) “incident which is unexpected and
thus unacceptable to patient and prescriber”
(Schommer, 2000)). Therefore, it is better to enforce
clear steps on the process to reduce the risk.
Fifth, emergency management is a key aspect of
home care system. Because of the real executors of
first aid (T21) at the daytime and night time are dif-
ferent, as well as some non-professional caregivers
such as taxi drivers are included, it is a transaction
integrating multiple actors. It not only needs a high
coverage of the new equipment, as emergency
alarms, but also requires a clearer description of ac-
tor’s responsibility and action steps.
Additionally, according to Table 1, a nurse is as-
signed to complete the jobs as catering (A13) and
medicine deliver (A19). This can be a hidden prob-
lem. Based on the expertise from special training,
nurses can carry out various medical and non-
Process-orientedHomeCareSystemTransformationinCentralFinland
459

medical tasks. For example, serving meals, taking a
shower for aging people, and cleaning the stuffs, We
can see that instead of doing more medical related
tasks, nurses need to spend time on many non-
medical tasks, which do not require their profession
and expertise.
5.2 Suggestions for Home Care
Transformation
Based on previous discussion, the following sugges-
tions are proposed.
First, in order to support the information shar-
ing among stakeholders in the home care, we sug-
gested establishing the national healthcare database
for all the residents to provide a basic standard. By
applying this method, both public and private home
care caregivers as well as home care demanders can
access the same database and retrieve the necessary
information such as medical history and health situa-
tion. For the security consideration, the related
health card can be launched as a method for stake-
holders to access the national healthcare database.
Especially, it is likely to increases the efficiency of
ordering phase (including request and promise) in
the demander-initiated health care process, as T01
and T05 in Figure 1.
Second, as mentioned before, in current home
care system, a main difference between public and
private home care caregivers is that the private ones
tend to outsource all of their medical services to oth-
ers and the nurses who have a rich medical expertise
and capacities have to do many non-medical tasks.
Therefore, the effectiveness of the whole home care
system is likely to improve if the public and private
sectors can collaborate to complement each other in
providing medical and non-medical services. Fur-
thermore, it can solve the problem of informational
sharing from public sectors to private sectors as an
alternative to the national healthcare system, because
the public sectors can access the client information
from Pegasos while the private ones cannot. They
may start exploring how to collaborate by consider-
ing and resolving issues related to law, culture, pri-
vacy, etc.
6 CONCLUSIONS
As Michael Porter pointed out, the health care in 21
st
century is currently delivered by the business model
of the 19
th
century (Porter and Teisberg, 2006).
Health care services and systems need to keep up
with shifting technological improvements, medical
development, and changing aging people needs. It is
also essential to establish a mutual understanding
about the home care system. Based on the interview
and document, we identified CMs for six home care
institutes in Central Finland, and then extracted the
general model of home care system. Next, we also
assessed the home care implementation related to the
attribution of responsibilities among real actors. This
study contributes to practice by creating general
construction model, identifying some critical issues
in practice, and showing some potential solutions to
enhance the home care system in Central Finland. In
this study, only the construction model has been
developed, other DEMO aspect models can be fur-
ther analyse. They may give some foundations of an
integrated model of healthcare services.
REFERENCES
Central Intelligence Agency (CIA)., 2012. The World
Factbook-Finland, available at
https://www.cia.gov/library/publications/the-world-
factbook/geos/fi.html (accessed June 2012).
Dietz, J. L. G., 2006. Enterprise Ontology - Theory and
Methodology. Springer. Heigelberg.
Habing, N., Dietz, J., Zwetsloot-Schonk, B., 2001. Activi-
ty Patterns in Health Care-Identifying Building Blocks
for the CPR. SIGGROUP Bulletin, 22(2), 9-15.
Invest in Finland., 2011. E-health in Finland. Invest in
Finland. Helsinki.
Kokko, S., 2009. Integrated primary health care: Finnish
solutions and experiences. International Journal of In-
tegrated Care, 9(25), 1-9.
Kunz, J., 2007. Population Aging – Problem or Opportuni-
ty? Lessons from the Case of Finland. Journal of So-
ciology, 1(1),
Maij, E., Reijswoud, V. E., Tousaint P. J., Harms, E. H.,
Zwetsloot-Schonk, J. H. M., 2000. A Process View of
Medical Practice by Modeling Communicative Act.
Methods of Information in Medicine, 39, 56-62.
Porter, M. E., Teisberg, E. O., 2006. Redefining health
care: creating value-based competition on results.
Harvard Business School Press, Massachusetts.
Schommer, J. C., 2000. Pharmacists’ New Communicative
Role: Explaining Illness and Medicine to Patients. In:
Whaley, B. B., editor. Explaining Illness: Research,
Theory and Strategies. Lawrence Erlbaum Associates.
New Jersey, 209-233.
KEOD2012-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
460
