
The Usability of an Exercise-based Tele-rehabilitation Service
A Hybrid Methodology
M. H. A. Huis in ’t Veld, S. M. Jansen-Kosterink
Roessingh Research and Development, Roessinghbleekweg 33b, Enschede, The Nederlands
S. Scattareggia, D. Wever
SignoMotus, via Panoramica dello Stretto, 340, Sicily, Italy
Roessingh Centre for Rehabilitation, Roessinghbleekweg 33, Enschede, The Netherlands
F. Benvenuti, W. Glinkowski
Azienda Unità Sanitaria Locale 11 di Empoli, Regione Toscana, Italy
Medical University of Warsaw, 61 Żwirki i Wigury Str. Warsaw, Poland
R. Sánchez-Carrión, S. Doménech
Fundació Privada Institut de Neurorehabilitació Guttmann. Camí de Can Ruti s/n, 08916 Badalona, Spain
Institut de l’Envelliment de la Universitat Autònoma de Barcelona
Sant Antoni Maria Claret 171. 08041 Barcelona, Spain
H. J. Hermens, M. M. R Vollenbroek-Hutten
Roessingh Research and Development, Roessinghsbleekweg 33b, Enschede, The Nederlands
University of Twente, Faculty of Electriclal Engineering, Mathematics and computer Science, Enschede, The Netherlands
Keywords: Usability, Exercise-based Tele-rehabilitation, Problem Software Reports, Change Requests, Methodology.
Abstract: Having usable technology is an imperative, especially for contemporary (elderly) patients with disabilities.
The aim of the present document is to examine the usability of our exercise-based tele-rehabilitation service
based on a hybrid approach in four different impaired user groups (elderly people with cognitive and/or
movement and postural problems) and in its context (as a tele-rehabilitation service during rehabilitation
treatment). A hybrid approach consisted of a task-oriented patient usability test and a one-year pilot-
implementation during which problem software reports and change requests were collected from
professionals. Across Europe, in total n=60 patients were included in the usability test suffering from
pulmonary diseases, stroke, orthopeadic patients and patients suffering from Alzheimer. In addition, during
the one-year pilot-implementation period in four European clinical centers (NL, PL, IT, ES), in total n=81
Software Problem Reports (SPR’s) have been collected and n=43 Change Requests (CRs). In conclusion,
this hybrid methodology allowed usability data to be retrieved from both an episodic and a longer period of
use, controlled use and use in routine care, and focus on both the tele-rehabilitation software and service
delivery, i.e tele-treatment protocols. Moreover, both the patient as well the professional perspective was
incorporated.
36
Sánchez-Carrión R., Jansen-Kosterink S., Huis in ’t Veld R., Doménech S., Wever D., Vollenbroek M., Benvenuti F., Scattareggia S., Glinkowski W. and
Hermens H. (2012).
The Usability of an Exercise-based Tele-rehabilitation ServiceA Hybrid Methodology.
In Proceedings of the Sixth International Symposium on e-Health Services and Technologies and the Third International Conference on Green IT
Solutions, pages 36-43
DOI: 10.5220/0004473800360043
Copyright
c
SciTePress

1 INTRODUCTION
The ageing of the population which leads to an
aggravation of chronic conditions, the growing need
for patients to become actors in their own health,
and the necessity of controlling health care whilst
maintaining high quality of care, place challenging
demands on our current health care system. Within
the European CLEAR project (= Clinical Leading
Environment for the Assessment of Rehabilitation
protocols in home care), an exercise based tele-
rehabilitation service and clinical protocols have
been developed and pilot-implemented in four
clinical centers across Europe to treat (elderly)
patients affected by pulmonary disease, stroke,
Alzheimer, and orthopedic problems (requiring often
total joint replacement) (www.habiliseurope.com).
Having usable technology is an imperative,
especially for contemporary (elderly) patients with
disabilities (Alexander and Staggers, 2009). The
common goals of usability research are to improve
the effectiveness, efficiency and satisfaction of
people interacting with tools (Hornbæk 2006).
Effectiveness includes the usefulness of a tool to
complete (work) tasks. Examples of efficiency
include time to complete specific tasks, the number
of clicks to perform tasks or the amount of time
needed. Satisfaction can include the perception of
any aspect of the tool typically includes perceptions
of the workload or the effectiveness of the specific
design (Alexander and Staggers 2009).
Concerning the ISO 9241 definition, usability
deals with the extent to which a product can be used
by specified users to achieve the before mentioned
specified goals (effectiveness, efficiency, and
satisfaction) in a specified context. The users, goals
(tasks) and context of our exercise-based tele-
rehabilitation program are defined in Table 1.
Table 1: Specified users, goals and context.
Users Patients suffering from pulmonary diseases,
Alzheimer, Stroke and Arthritis
Rehabilitation physicians, psychologists,
physiotherapists
Goals To enable multiple patients to exercise/train
simultaneously in their own relevant context
(either at home or at the clinic) under the
remote supervision of an expert professional
Context The location where the tele-rehabilitation is
provided: at home, at the clinic or outpatient
treatment facility
The country where the tele-rehabilitation
service is provided: The Netherlands,
Poland, Italy and Spain
How to measure usability, by which tests and
which parameters to be selected are important
challenges in human-computer-interaction research
(ISO, 1998; Frøkjær, 2000). The innovative and new
context of tele-rehabilitation services even more
increases the challenges associated with usability
examination because it involves new technologies,
new protocols for health care delivery (i.e. at home)
and (often) impaired user groups (Monk, 2002).
Expanding the knowledge on usability issues in the
field of tele-rehabilitation would enable better fit
between users (patients and professionals) and
technology, thereby possibly maximizing the
chances of successful adoption of tele-rehabilitation
services in routine care.
The aim of the present document is to examine
the usability of our exercise-based tele-rehabilitation
service based on a hybrid approach in four different
impaired user groups. This methodology is aimed at
evaluating the usability of the service in its context
(as a tele-rehabilitation service during treatment),
thus the usability of the protocol for home-based
treatment and keeping in mind a specific impaired
target group (elderly people with cognitive and/or
movement and postural problems).
2 METHOD
2.1 Exercise Tele-rehabilitation Service
The exercise tele-rehabilitation service consists of a
notebook with webcam, with newly developed
software giving access to a database of exercise
videos and a teleconference service to facilitate
contact between the patient and professional. With
this new service the professional can compose a
tailored exercise program for his patient. The patient
can carry out the program on a self-scheduled time
at the clinical at home or. The patient can record an
exercise with the webcam and the recorded exercise
can be assessed by the professional. Patient and
professional can contact each other by
teleconference to discuss the rehabilitation progress.
The professional can schedule, add and delete
exercises in the exercise program of the patient
during the rehabilitation. The exercise tele-
rehabilitation service enables patients to exercise at
home at moments preferred by the patients, which
fits in the current trend of self management of the
patient. Screenshots of the patient GUI is presented
in Appendix 1.
The Usability of an Exercise-based Tele-rehabilitation Service - A Hybrid Methodology
37

Table 2: Patient usability test: evaluation parameters based on framework of Hornbæk (2006).
2.2 Methodology
A hybrid methodology was used in evaluating the
usability of the exercise-based tele-rehabilitation
service.
(1) Patient usability test: consisting of a task-ori-
ented examination of the usability during episodic
use of the program in a laboratory setting
(2) Pilot-implementation: collecting problem soft-
ware reports and change requests during a one-year
period among professionals in order to provide
information on usability issues during routine use in
rehabilitation setting.
2.2.1 Patient Usability Test
Four different patient populations were invited to
participate in the usability study namely patients
with pulmonary diseases (The Netherlands), stroke
(Italy), orthopeadic patients (Poland) and patients
suffering from Alzheimer (Spain). All patients were
invited to local institutes to participate in a 2-hour
usability test during which they have to complete
four pre-defined concrete tasks being (1) start your
computer and log in, (2) start the patient exercise
module and watch tutorial, (3) Execute an exercise
and record the execution with video, (4)
communicate with the therapist by
videoconferencing. The usability parameters defined
by Horbæk (2006) were operationalized into
concrete parameters for this study (see Table 2).
2.2.2 Pilot-implementation Test
The exercise-based tele-rehabilitation program was
pilot-implemented as part of the traditional care
service for a period of one year. Besides
investigating the clinical impact, the scope of this
pilot-implementation was to collect in systematic
way relevant information regarding the requested
improvements of the service as a result of actual use
in a daily setting for a long(er) period of time.
The feedback collected have been divided in two
main categories (a) Software Problem Report (SPR)
and (b) Change Requests (CR). SPR’s deal with
information related to software malfunctions of the
service that prevent the proper delivery of the
service. These are mainly related to bad functioning
of modules noticed by the health care professionals
during their activities with the software. CRs deal
with a request of modification that is related to the
particular service model in use. These requests deals
EHST/ICGREEN 2012
38
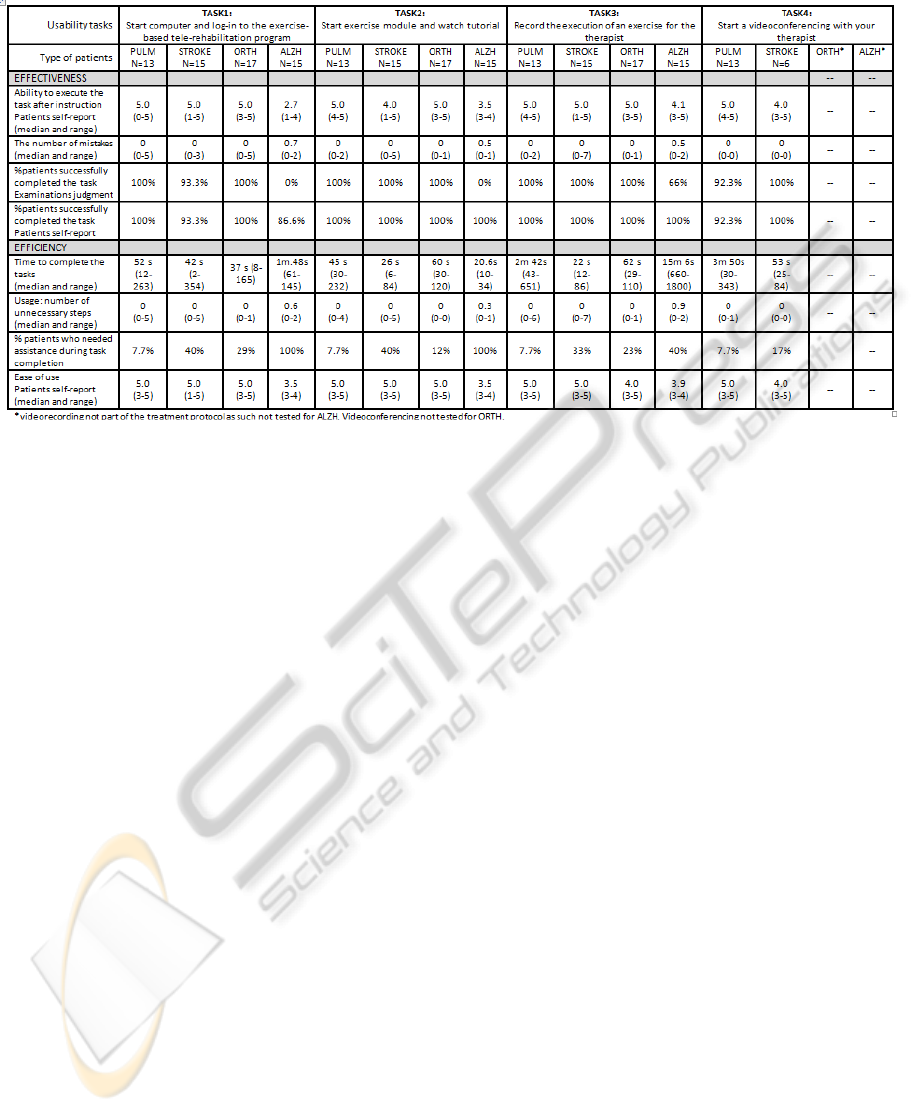
Table 3a: Patient usability test results for effectiveness and efficiency.
mainly with improvements request of a particular
module or function that is not optimal for the scope,
addition of new functionalities, interoperability
aspects related to integration with the Hospital
Information System (HIS) in use in the concerned
centre.
2.3 Statistical Analyses
All analysis will be conducted on a group-level. For
the usability parameters containing ordinal
answering scales derived from the patient test, non-
parametric descriptive statistics (median and range)
will be calculated. For the usability parameters
containing a dichotomous answering format,
percentages will be calculated. For the pilot-
implementation the amount of SPRs and CRs will be
presented as well as a summative description of the
categories for which SPRs and CRs will be
provided.
3 RESULTS
3.1 Patient Usability Test
In total n=60 patients participated in the usability
test. Among these are n=24 males and n=36 females.
The mean age of the participants is 63.6 years (range
31-94). The results of the patient usability test are
presented per parameter per task per pathology in
Table 3a.
3.1.1 Effectiveness
Except for the patients suffering from cognitive
impairments due to Alzheimer’s disease, participants
were confident about their ability to remember how
to execute the different tasks. Interestingly, on
average few mistakes were made in the completion
of the tasks by the participants. However, the ranges
indicate that mistakes were made. Typically,
mistakes were associated with remembering
passwords or typing errors (task 1), forgetting to
click the start (Task 2, 3) and/or stop button (Task
3). In addition, as illustrated by the percentage of
patients who not completed the tasks successfully
the tele-rehabilitation software also contained some
problems. For instance, webcam connectivity
problems were faced as well as poor image quality
during videoconferencing (Task 4). As indicated by
the discrepancy in % interpretation of successful
completion between the examinator and
patients’self-report, Alzheimer patients’ seem to be
not fully aware whether or not they completed the
tasks successfully.
3.1.2 Efficiency
As shown in Table 3a, the duration to log in (Task 1)
and to start and watch the exercise tutorial (Task 2)
was rather comparable between patients suffering
from pulmonary diseases, stroke and orthopedic
problems. Patient suffering from Alzheimer’s
disease needed more time to log in. For task 3, large
differences existed between the patient populations.
The Usability of an Exercise-based Tele-rehabilitation Service - A Hybrid Methodology
39

Table 3b: Results of the laboratory usability for satisfaction of use (n=60).
These data can however not be directly compared
between the populations since they all recorded
different exercises, relevant to their pathologies. The
relatively long duration to set up a
videoconferencing by patients with pulmonary
diseases could be explained by connectivity
problems (one patient had to wait three minutes).
One patient forgot to put on the headset which was
necessary to communicate by voice/audio with the
therapist. Remarkably, despite the fact that patients
were rather satisfied about the ease of use (>3.5) of
the tele-rehabilitation program none of the patient
groups was able to complete the tasks without help
(to a greater or lesser extent). As could be expected,
patients suffering from Alzheimer had an inefficient
use pattern of the software which is (again) probably
due to their cognitive impairments
3.1.3 Satisfaction
The results of the satisfaction parameters are
illustrated in Table 3b for the different pathologies.
On average, patients were satisfied with the text
length and understandability of the instructions as
well as the quality of the navigation, text size, colors
and pictograms (median satisfaction scores > 3.0).
The quality of the interaction with the software was
perceived sufficient to excellent varying from grade
6.0 by patients suffering from pulmonary diseases to
a score of 9.0 by patients suffering from orthopedic
problems. In general, the majority of patients (>
69.2%) patients stated that they would recommend
the software to another patient or friend.
However, the variance in percentage of patients
who preferred tele-rehabilitation over traditional
care is high between the pathologies. In our opinion,
this variance could be explained by the difference in
treatment protocols, i.e. the extent to which the tele-
rehabilitation service substitutes traditional care.
For instance, 80% of the orthopedic patients prefer
tele-rehabilitation versus 15.4% of the pulmonary
patients. In the latter group, tele-rehabilitation
partially substituted traditional care whereas in the
orthopedic group tele-rehabilitation was provided
supplementary to traditional care.
3.2 Pilot-implementation Test
During a one-year pilot-implementation period in
four European clinical centers (NL, PL, IT, ES), in
EHST/ICGREEN 2012
40

total n=81 Software Problem Reports (SPR’s) have
been collected and n=43 Change Requests (CRs).
The exact nature of the SPR’s and CRs are too
specific for the technology used to describe and
analyze in detail in the current paper.
In general, the SPRs sent by the clinical centers
concern hanging applets, usability of log in and
tutorials for patients and professionals, bugs, more
flexible use of the tutorial management (should be
possible to add new exercises or remove ones and
show adequate sequence of exercises), connectivity
and/or audio quality of the videoconferencing,
patient exercise interface, webcam management, and
browser interactions.
In general, the description of the CRs concern
viewing back a just recorded exercise, delete a just
recorded exercise and replace by a new one, add
mandatory fields in forms, network policies, to allow
therapists to define a proper order in which the
selected tutorial will be shown to the patient,
increase the size of the log out button, bandwidth
issues, a videoconferencing call should not be able
to interrupt the patient during exercising, translation
of content to different languages, add personalized
exercise instructions, and client stations should be
allowed to access the service without the needs of a
VPN connection.
4 CONCLUSIONS
The current study investigated the usability of an
exercise-based tele-rehabilitation service in four
different countries, representing four different
patient populations being patients suffering from
pulmonary diseases, stroke, orthopeadic problems or
Alzheimer’s disease. Patients (n=60) were
characterized by physical and/or cognitive
impairments typically associated with their
pathologies and relatively high age. A hybrid
usability methodology was embraced consisting of
(1) a laboratory patient usability test and (2) a pilot-
implementation period of one year duration.
For the usability test, the patients had to execute
four predefined tasks (start up PC and log in to the
service, start and view exercise tutorial, record an
exercise, start and conduct a videoconferencing with
a therapist). The usability parameters examined were
derived from the framework of Hornbæk (2006).
During the one-year pilot implementation the
usability of the service was examined by means of
collecting n=81 Software Problem Reports (SPRs)
and n=43 Change Requests (CR).
The innovativeness and strength of our hybrid
methodology lies in the retrieval of usability data
from both an episodic and a longer period of use,
controlled use and use in routine care, and focus on
the tele-rehabilitation software and service delivery,
e.g. tele-treatment protocols. Moreover, both the
patient as well the professional perspective was
incorporated in this methodology. In addition, our
operationalization of the framework of Hornbæk
(2006) into concrete parameters could be valuable
for other researchers in the field of evaluating the
usability of similar services.
Because of the fact that the patient study and
pilot-implementation contained different
methodologies and parameterizations not all results
may be easily comparable. In our view, this should
not be considered to be a weakness of the
methodology but a valuable strength. Together this
information provides a broad(er) perspective on
usability and recommendations to improve it.
Interestingly, commonalities in usability issues were
found between the patient usability test and the pilot
implementation. These commonalities dealt with
log in and log out problems and issues with respect
to the videoconferencing module and connectivity.
The methodology could be improved by
repeating the patient usability test over time during
the (pilot-) implementation (Hornbæk, 2006).
Another recommendation for methodology
improvement is to extend the measure of satisfaction
by post-use Likert-scales as done in the current
study by validated and standardized questions. As
illustrated by the ‘regression to the mean’ trend,
results of the satisfaction questionnaire tended
towards ‘socially desirable’ answers by the users.
Lastly, the parameters used are not intended to
serve as an exclusive list of usability parameters.
Instead, according to Hornbæk (2006), it provides
usability researchers an overview of the possible
parameters that can be applied. Researchers should
select the parameters to be most relevant for their
own research purposes and concretized for the
service they want to evaluate.
As could be expected on advance, patients with
Alzheimer’s disease had more difficulty in using the
tele-rehabilitation service compared to patients
suffering from pulmonary diseases, orthopaedic
problems and stroke. This is probably due to their
severe cognitive impairments of the Alzheimer
population included in the present study. This result
does reveal the recommendation for other
investigators to take into account the characteristics
of the target users and their pathologies when
designing innovative technology-based treatment
The Usability of an Exercise-based Tele-rehabilitation Service - A Hybrid Methodology
41

concepts. For instance, instead of remembering
passwords fingerprints log in would have been more
suited for patients with cognitive impairments.
Results showed that the majority of patients were
able to complete the tasks successfully without many
unnecessary actions and mistakes. However, despite
the fact that all patients were trained in using the
service under study prior to participation (some of
them actually used the service during their rehab
treatment!) and that patients reported to be rather
satisfied about its ease of use, the majority of them
still needed help/assistance. Apparently, it is not
realistic to assume that patients who passed the
training and believe they are confident to use the
service are actually able to use the service
adequately independently. This result has major
clinical implications. Without having insight into the
effectiveness and efficiency of use of software by
patients, therapists will hardly be able to explain
(poor) clinical impact due to inadequate use and the
(content of the) treatment. This lack of insight in the
use can be addressed by the technology and/or the
service delivery. From a technology perspective,
automatic usage logs and compliance measures
could be integrated in the system. From a service
delivery perspective, it is strongly recommended to
organize assistance for patients while interacting
with the service e.g. by therapists (when interacting
inside the rehab facility) or informal caregivers
(when interacting at home).
Results showed that the majority of patients
would recommend the service to other patients or
friends. Major reasons for recommending the service
is the fact that it offers the opportunity to receive
additional specific instructions during training (at
home or at the rehab facility) as a mnemonic.
Nevertheless, the patients groups differed in the
degree to which they preferred the tele-rehabilitation
service compared to regular in-person care (with
lowest preference score for patients with pulmonary
diseases and highest score for patient with
Alzheimer disease). These differences could be
explained by the differences in the way the tele-
rehabilitation is embedded in regular in-person care
during the pilot-implementation between the groups.
For instance, for pulmonary patients, tele-
rehabilitation is offered as a (partly) replacement of
traditional in-person care, i.e. service delivery
whereas for patients with Alzheimers’ disease the
tele-rehabilitation service is used as an extra training
modality inside the rehabilitation facility.
Consequently by carefully considering an optimal
design for the service delivery for tele-rehabilitation
innovations one could be able to affect the users’
attitude and possibly the degree of (future) adoption
by these users.
A recent systematic review showed that the
usability evaluations differed in methodologies and
quality indicators for usability making it difficult to
reveal abstractions, i.e. commonalities in failures
and facilitators for usability of clinical technology
that can be used by others (Alexander and Staggers,
2009). However, it can be concluded that the present
study revealed at least three recommendations for
usability design for exercise-based tele-rehabilitation
services. First, one should carefully consider the
characteristics (e.g. cognitive versus physical
impairments) of the pathologies of users involved.
Our results showed different usability issues for the
different pathologies. Second, insight in adequate
use of the technology is crucial when evaluating the
clinical impact. Our results showed that the majority
patients were not capable of using the program
adequately despite them having successfully passed
their instruction session. Third, careful consideration
of how the tele-rehabilitation is embedded in regular
in-person care, i.e. the service delivery, affects the
attitude of patients toward and possibly the
successful adoption of these innovative
interventions.
REFERENCES
Habilis Europe http://www.habiliseurope.eu/
Hornbæk K 2006, Current practice in measuring usability:
challenges to usability studies and research,
International Journal of Human-Computer Studies,
64, 79-102
Alexander G and Staggers N (2009), A systematic review
on the designs of clinical technology: findings and
recommendations for future research, ANS Adv Nurs
Scie, 32 (3), 252-279
ISO, 1998, Ergonomic requirements for office works with
visual display terminals (VDTs) – Part 11 guidance
on usability (ISO 9241-11)
Frøkjær E, Hertzum M, Hornbæk, 2000, Measuring
usability: are effectiveness, efficiency, and satisfaction
really correlated. In: Proceedings of ACM Conference
on Human Factors in Computer Systems, ACM Press,
New York, 354-352
Monk A 2002. Noddy’s guide to usability. Interfaces 50,
31–33
APPENDIX 1
Screenshots of the tele-rehabilitation service
EHST/ICGREEN 2012
42

C
Re
m
Chat
V
A
Hospital
Logo
C
onnect
m
ote video:
Disconnect
V
ideoconferenc
i
A
ssigning exer
c
Example
Local video:
Record
i
ng therapist -
p
c
ise from librar
y
of an exercise
v
Send
Home | Print | Help
Frame Rate Quality
Close
p
rofessional
y
to patient
v
ideo
The Usability of an Exercise-based Tele-rehabilitation Service - A Hybrid Methodology
43
