
Phase-Rectified Signal Averaging to Evaluate ANS Development in
Premature Infants
Maristella Lucchini
1
, Devy Widjaja
1,2
, Carolina Varon
1,2
, Katrien Jansen
3
and Sabine Van Huffel
1,2
1
Department of Electrical Engineering, ESAT-SCD, KU Leuven
Kasteelpark Arenberg 10, box 2446, 3001 Leuven, Belgium
2
iMinds Future Health Department, Kasteelpark Arenberg 10, box 2446, 3001 Leuven, Belgium
3
Department of Pediatric Neurology, University Hospitals Leuven, Herestraat 49, 3000 Leuven, Belgium
Keywords: Phase-Rectified Signal Averaging, Heart Rate Variability, Autonomic Nervous System, Quasi-Periodicities,
Non-Stationary Signals.
Abstract: Aim: Heart Rate Variability (HRV) is determined by the autonomic nervous system (ANS) and a low value
of this parameter is related to neurological pathologies and infants mortality. This study aims to assess the
utility and the advantages of HRV analysis by means of phase-rectified signal averaging (PRSA), a
technique that obtains curves that are useful to determine the development of the ANS in preterm infants,
with less obtrusive monitoring compared to electroencephalography.
Methods: For a preliminary study, 24-hour ECGs were taken in NICU at the University Hospital in Leuven,
from 12 babies: 4 were term, 4 were born preterm but reached a term postmenstrual age, and 4 were
preterm. Heart rate tracks of segments of 27 minutes were extracted and analyzed with the PRSA technique.
The curves obtained were quantified by the slope and by an acceleration/deceleration related parameter
(AC/DC). Two independent analyses on acceleration and deceleration were carried out to visualize the
effects of the sympathetic and parasympathetic system separately. Moreover, the immediate response and
the response after 5 seconds were taken into account.
Results and Conclusion: All the results were compared and validated with traditional HRV parameters. The
results of slope and AD/DC in both types of analysis are promising in providing a simple parameter to
assess neurological development deficiency in order to allow faster and preventive intervention. Further
studies are needed in a larger population.
1 INTRODUCTION
In recent years, the study of heart rate variability
(HRV) has gained growing importance. As a matter
of fact, the cardiac rhythm is a crossroad of
numerous systems of physiological control operation
on different temporal scales: breathing, hormones,
the autonomic nervous system (ANS), etc. The
parasympathetic nervous system has the ability to
decrease the heart rate, while the sympathetic one
usually reacts to acute situations by increasing the
rhythm. Researchers have shown that, in adults, a
stable and predictable HR is usually associated with
ongoing and upcoming pathologies (Rajendra et al.,
2005). This fact opens up a new conception of
homeostasis: in reality our body does not tend to a
fixed situation but keeps its parameter in a range of
fluctuation that allows it to properly respond to
external stimuli (Bauer et al., 2006a).
An interesting aspect of HRV is that it can be
acquired from non-invasive measurements like the
electrocardiogram (ECG). Due to this fact, HRV is
suitable to monitor premature babies, who are
usually very sensitive and unstable, and to
investigate their ANS development, which is a
crucial issue in these kinds of patients. We
hypothesize that babies affected by
underdevelopment of the ANS, will be less capable
of varying their HR in response to external and
internal factors.
The specific aim of this study is to analyze
recordings from term and preterm infants using the
Phase-Rectified Signal Averaging (PRSA) method
(Bauer et al., 2006b). This algorithm is capable of
synchronizing the phase of all periodic components
of a noisy, non-stationary signal with respect to their
203
Lucchini M., Widjaja D., Varon C., Jansen K. and Van Huffel S..
Phase-Rectified Signal Averaging to Evaluate ANS Development in Premature Infants.
DOI: 10.5220/0004240702030208
In Proceedings of the International Conference on Bio-inspired Systems and Signal Processing (BIOSIGNALS-2013), pages 203-208
ISBN: 978-989-8565-36-5
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

frequencies and time scales. Moreover, it is a
powerful tool to separately analyze the acceleration
and deceleration of the HR, having thus the
possibility to visualize the influence of the vagal and
sympathetic system separately (Huhn et al., 2011).
In this research, we will focus on the acceleration
and deceleration of the HR, giving a qualitative
description of the obtained PRSA signals and
proposing parameters to evaluate the maturity of the
ANS.
2 DATA AND METHODS
2.1 Data Acquisition and Preprocessing
In this research, 12 ECGs (sampling frequency f
s
=
250 Hz) are analyzed: 4 signals are taken from
premature babies (gestational age at birth < 37
weeks), 4 from prematurely born babies that reached
a term postmenstrual age (PMA > 40 weeks) and 4
from term babies (gestational age at birth > 40
weeks), all hospitalized in the pediatric neurology
department at the University Hospital in Leuven.
From 24-hour ECG recordings, a segment of 27
minutes was extracted for each patient. After that,
the tracks were preprocessed in three steps: at first,
the ECG segments were resampled to 1000 Hz using
cubic spline interpolation to gain a better quality
during the analysis, secondly they were filtered at 50
Hz to remove power line interference. In the third
step, the heart beats were extracted using the Pan-
Tompkins algorithm (Pan and Tompkins, 1985).
Based on the time between consecutive beats, it was
possible to calculate the heart rate.
2.2 Description of the PRSA Technique
The heart rate signals were processed using the
PRSA technique, with the aim of compressing the
signal into a shorter sequence without losing any
relevant quasi-periodicities, and eliminating at the
same time non-stationarities, artifacts, and noise.
This technique consists of 3 simple steps outlined in
Figure 1 (Bauer et al., 2006b).
At first, anchor points (AP) are chosen based on
a certain property of the signal x
i
. In this study,
increases or decreases in the signal are taken into
account, as well as averages of T values of the time
series.
1
ii
xx
(1
)
Figure 1: Illustration of the PRSA technique (Bauer et al.,
2006b). (a) Anchor points are selected from the original
signal x
i
; here increase events are selected according to
Equation 1. (b) Windows of length 2L are defined around
each anchor point, here are shown the first four anchor
points. (c) The surroundings of many anchor points (all
located in the centre) are shown on top of each other. (d)
The PRSA curve x
k
resulting from averaging over all
surroundings is shown.
1
ii
xx
(2
)
T
j
ji
T
j
ji
x
T
x
T
1
1
0
11
(3
)
T
j
ji
T
j
ji
x
T
x
T
1
1
0
11
(4
)
We have applied Equations (1) and (2) to see the
beat-to-beat response and (3) and (4) to visualize the
5 seconds (on average 14 beats) response.
Typically half of all points of the signal will be
APs by these definitions. The parameter T sets an
upper frequency limit for the detection of
periodicities, because taking a mean over T samples
is equal to applying a low-pass filter. The capability
of resetting of this method comes from the fact that
when we fix the AP in the increasing (decreasing)
point, they will be in the phase of the steepest ascent
(decent), which means when the phase of the
oscillation is close to 0 (π). Thanks to this process
we can extract the phase information of the
oscillations from the signal itself (Bauer et al.,
2006b). Heart rate accelerations and decelerations of
more than 25% are excluded to suppress errors due
to artifacts.
BIOSIGNALS2013-InternationalConferenceonBio-inspiredSystemsandSignalProcessing
204

Afterwards, windows of length 2L, in this case
L=100 samples, are defined around each AP. APs
where no full surroundings of this length are
available are excluded from the analysis. Since most
of the APs are closer than 2L, most of the windows
will overlap. It is important to make a proper choice
for the parameter L; it should be larger than the
period of the slowest oscillation that one wants to
detect.
Lastly, the windows are aligned at the AP and
the PRSA curve
x
k
is obtained by averaging the
aligned windows. Thanks to this average,
components that are not phase synchronized with the
AP, will have zero mean and thus they will cancel
out; instead, the events that have a fixed phase
relationship with the AP in all the 2L windows will
have the same pattern and thus will be kept in the
average.
From each signal, the average was subtracted to
highlight the variation around the mean and to
facilitate the comparison between signals with
different means.
2.3 Measures for the Quantification of
PRSA Curves
For each HR signal, 4 PRSA curves x
k
were
calculated using Equations (1) to (4), with T=14 for
Equations (3) and (4).
In
x
k
the central peak retains the information of
all the quasi-periodicities of the HR tracks.
Depending on the criteria for the selection of the AP,
the central spike will quantify the mean capacity of
the ANS to accelerate or decelerate the HR.
For the curves obtained with Equations (1) and
(3), the following parameters were calculated:
AAC: the Average Acceleration Capacity is
the subtraction of the average of the signal
after the AP from the average of the signal
before the AP (Huhn et al., 2011);
AC: the Acceleration Capacity is defined as
the change around the anchor point that
corresponds to computing the AAC for just
3 points before and after the AP (Bauer et
al., 2006);
SLOPE_A: the slope of the straight line
connecting the point before and after the
central anchor point is derived.
The same parameters were extracted for the
curves obtained using Equations (2) and (4), taking
into account the deceleration (respectively ADC,
DC, SLOPE_D).
2.4 Time Domain HRV Measures
To validate the results obtained with PRSA, 5 well-
known HRV time domain parameters were
computed (Task Force of The European Society of
Cardiology and The North American Society of
Pacing and Electrophysiology, 1996):
MeanNN: mean interval between
consecutive QRS complexes (called NN
intervals, i.e. all intervals between adjacent
QRS complexes, obtained from sinus node
depolarizations);
SDNN: standard deviation of the NN
intervals, i.e. the square root of the
variance. SDNN is a measure for cyclic
components that are present during the
recordings;
RMSSD: the square root of the mean
squared differences of successive NN
intervals. This measure quantifies
parasympathetic modulation;
pNN25: the percentage of NN intervals that
differ more than 25 ms with respect to the
preceding NN intervals, compared to the
total number of NN intervals. This is also a
measure for parasympathetic activity;
SDSD: standard deviation of the differences
between successive NN intervals. SDSD
presents short-term variations and is highly
correlated with RMSSD and pNN25.
3 RESULTS AND DISCUSSION
3.1 PRSA Curves
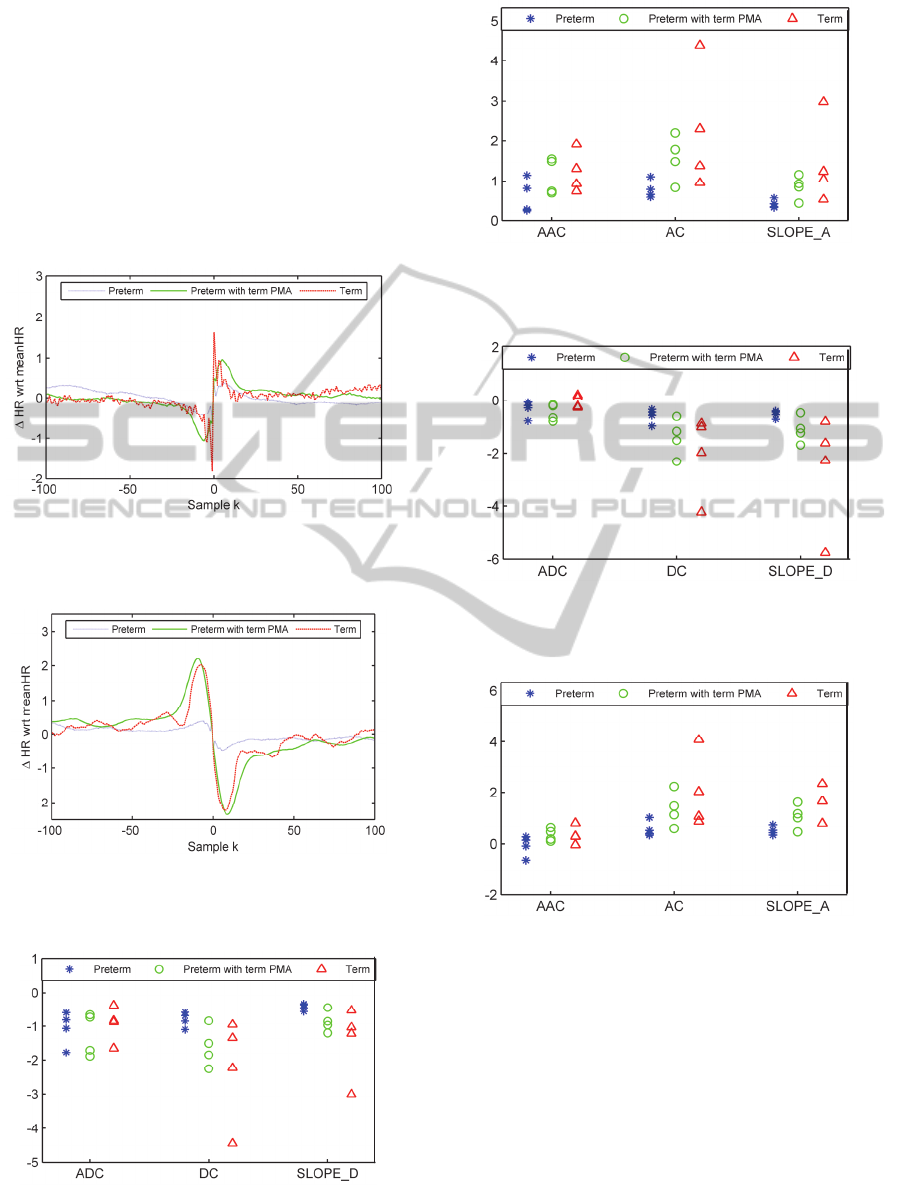
Figure 2 presents the mean PRSA curves for heart
rate acceleration in beat-to-beat analysis. In Figure
3, the mean PRSA curves for heart rate decelerations
in 14 beats analysis are shown. Both figures clearly
show how the PRSA curves of term babies have
larger amplitudes for all the experiments. In
addition, beat-to-beat curves of terms are more
unstable and unpredictable, whereas the signals of
preterms show a smoother behaviour, indicating less
variation in their HR. The curves obtained from
prematurely born babies that reached a term PMA
show a limited capacity of variation with respect to
term babies of their age.
Figures 4 and 5 and Table 1 show the values of
all the parameters compared among 12 patients for
14 beats analysis and Figures 6 and 7 and Table 2
for beat-to-beat.
Phase-RectifiedSignalAveragingtoEvaluateANSDevelopmentinPrematureInfants
205
In both experiments, it is observable that AAC and
ADC are not suited parameters to describe the curve,
since the difference between the 3 populations is
minimal. This can be explained by the fact that in
beat-to-beat and 14 beats analyses most of the length
of the 2L window contains information not directly
related to the instantaneous acceleration or
deceleration capability of the HR. For this specific
reason, parameters, which take into account the
entire length of the signal, are considered irrelevant
for this type of study.
Figure 2: Mean PRSA curves for acceleration in beat-to-
beat analysis. Premature infants are shown in blue,
preterm with term PMA in green, term babies in red.
Figure 3: Mean PRSA curve for deceleration in 14 beats
analysis. Premature infants are shown in blue, preterm
with term PMA in green, term babies in red.
Figure 4: PRSA parameters related to deceleration for 14
beats analysis. Premature infants are shown in blue,
preterm with term PMA in green, term babies in red.
Figure 5: PRSA parameters related to acceleration for 14
beats analysis. Premature infants are shown in blue,
preterm with term PMA in green, term babies in red.
Figure 6: PRSA parameters related to deceleration for
beat-to-beat analysis. Premature infants are shown in blue,
preterm with term PMA in green, term babies in red.
Figure 7: PRSA parameters related to acceleration for
beat-to-beat analysis. Premature infants are shown in blue,
preterm with term PMA in green, term babies in red.
On the contrary, SLOPE_A and SLOPE_D, and
AC and DC reveal to be valuable parameters; they
describe to which extent the heart is capable of
increasing or decreasing its beating rate, taking this
information from the central amplitude on the y-
axis. At the same time, they take into account the
velocity with which the heart manages to reach the
required beating rate in response to external factors,
weighing the time information from the x-axis.
BIOSIGNALS2013-InternationalConferenceonBio-inspiredSystemsandSignalProcessing
206

Table 1: Mean (± standard deviation) PRSA parameters in 14 beats analysis.
14 Beats Preterm Preterm born
with term PMA
Term
AC 0.79 ± 0.23 1.58 ± 0.57 2.26 ± 1.55
SLOPE_A
DC
SLOPE_D
0.42 ± 0.11
- 0.80 ± 0.22
- 0.26 ± 0.40
0.84 ± 0.30
- 1.61 ± 0.60
- 0.86 ± 0.32
1.45 ± 1.07
- 1.57 ± 2.42
- 1.44 ± 1.08
Table 2: Mean (± standard deviation) PRSA parameters in beat-to-beat analysis.
BTB Preterm Preterm born
with term PMA
Term
AC 0.57 ± 0.35 1.35 ± 1.53 2.01 ± 1.47
SLOPE_A
DC
SLOPE_D
0.50 ± 0.17
- 0.59 ± 0.28
- 0.53 ± 0.14
1.06 ± 0.47
- 0.82 ± 0.32
- 1.12 ± 0.50
2.59 ± 2.09
- 2.02 ± 1.55
- 2.62 ± 2.18
Table 3: Mean (± standard deviation) time domain HRV parameters for beat-to-beat analysis.
Patients meanNN (ms) SDNN (ms) RMSSD (ms) pNN25 (%) SDSD (ms)
Preterm
408.57 ± 48.65 19.45 ± 8.93 4.72 ± 6.42 0.39 ± 0.47 3.92 ± 6.39
Preterm born with
term PMA
397.51 ± 54.33 18.54 ± 11.80 7.06 ± 2.37 0.36 ± 0.60 5.92 ± 2.51
Term babies
563.82 ± 134.92 44.55 ± 23.68 28.90 ± 25.09 19.89 ± 25.63 21.24 ± 17.96
For all the cases we analyzed, premature values,
taken as absolute, were smaller than the ones from
term babies. Preterm born babies with a term PMA,
although they have the same PMA as the term
babies, do not show similar characteristics, but
behave between terms and preterms.
This fact is consistent with our primary
hypothesis: lower values for these parameters
indicate a reduced capability to respond to stimuli
properly and in time, showing how a premature
nervous system is less efficient and more at risk.
3.2 Comparison with Time Domain
HRV Parameters
In Table 3, the mean time domain HRV parameters
for each group of babies, are listed.
The heart rate of prematurely born babies is
higher than the one of control subjects. It is also
possible to see that the SDNN of preterms is lower
than for the term babies. This is an indication of a
more fixed heart rate, meaning that premature babies
react slower to acute situations than the normal
subjects. Another important observation is that
RMSSD, pNN25 and SDSD, all markers for
parasympathetic activity, are clearly reduced in
prematurely born infants. This proves again that
prematurity strongly reduces the development of the
ANS. Moreover, preterm born babies with a term
PMA show that the development of their ANS has
not yet reached the same maturity as the term born
babies. With these results, it is possible to confirm
the results obtained with PRSA, where it is observed
that the premature babies present a more fixed heart
rate and a slower reaction to acute situations.
4 CONCLUSIONS
The aim of this investigation was to analyze the
development of the ANS of full-term, prematurely
born that reach term PMA and preterm babies by
means of a computational analysis of HR recordings
using the PRSA technique. A set of parameters
Phase-RectifiedSignalAveragingtoEvaluateANSDevelopmentinPrematureInfants
207

capable of describing the PRSA curves was defined.
HR was chosen as an indicative parameter of
neurological development because its variability is
regulated primarily by the ANS. Additionally, it can
be taken from the ECG, which needs fewer
electrodes than other techniques, such as
electroencephalography.
The PRSA method was selected because it is
proficient in condensing the signal into a shorter
sequence, keeping any relevant quasi-periodicities
but cancelling out all non-stationarities, artifacts,
and noise. Moreover, it is a very straightforward
algorithm which does not require a long
preprocessing of the raw data.
In order to achieve the goals of this work, two
types of PRSA investigations were developed in
parallel: the first looked at the acceleration and
deceleration on a beat-to-beat scale, the second one
on a 14 beats scale. This separation is due to the fact
that the two branches of the ANS, the sympathetic
and parasympathetic have shown to have different
time responses to external factors.
To quantify the difference among three groups of
babies, a few parameters were implemented: AAC,
ADC, SLOPE_A, SLOPE_D, AC and DC.
The last four revealed to be useful in PRSA
interpretation, since they are able to interpret to
which extent the heart is capable to increase or
decrease its beating rhythm from one beat to the next
one and how long it takes for this process to happen.
This is possible thanks to an analysis that focuses on
the beats just before and after the anchor point,
which identifies the moment of increase/decrease of
the signal. These parameters can be considered a
relevant first screening method to have a rapid idea
of the neurological condition of the patients,
indicating where it is necessary to run further
investigations.
The findings based on the PRSA technique were
also compared and validated using traditional time
domain HRV parameters. PRSA parameters proved
to be consistent with the traditional ones, having the
advantage of being less influenced by the noise or by
physiologic regulatory events and thus are more
robust and trustable. Additionally, the parameters
proposed provide complex information in one
number, taking into account the maximum range of
HRV and the time required for the heart to reached
the necessary HR. Moreover the possibility of
varying the two parameters L and T and the criterion
of choice of the AP, make this technique extremely
versatile.
To conclude, the PRSA technique revealed to be
an innovative and promising approach. Nonetheless
it is necessary to confirm our conclusion on a larger
population that will allow us to conduct statistical
analysis and to define threshold values for the
implemented parameters to distinct healthy and
underdeveloped infants.
REFERENCES
Rajendra Acharya U., Paul Joseph K.,Kannathal N., Choo
Min Lim, Suri Jasjit S., 2005. Heart rate variability:
a review
Bauer A., Kantelhardt J. W., Barthel P., Schneider R.,
Mäkikallio T., Ulm K., Hnatkova K., Schömig A.,
Huikuri H., Bunde A., Malik M., Schmidt G., 2006a.
Deceleration capacity of heart rate as a predictor of
mortality after myocardial infarction: cohort study,
The Lancet.
Pan J., Tompkins W. J., 1985. A Real-Time QRS Detection
Algorithm, IEEE Transactions on Biomedical
Engineering.
Huhn E. A., Lobmaier S., Fischer T., Schneider R., Bauer
A., Schneider K. T., Schmidt G., 2011. New
computerized fetal heart rate analysis for surveillance
of intrauterine growth restriction, University Hospital
Basel, Basel, Switzerland,
Bauer A, Bunde A, Barthel P, Schneider R, Malik M,
Schmidt G., 2006b. Phase rectified signal averaging
detects quasi-periodicities in non-stationary data
Task Force of The European Society of Cardiology and
The North American Society of Pacing and
Electrophysiology, 1996. Heart rate variability,
Standards of measurement, physiological
interpretation, and clinical use, European Heart
Journal
BIOSIGNALS2013-InternationalConferenceonBio-inspiredSystemsandSignalProcessing
208
