
A New Approach to the Transition from Paper to Electronic
Medical Records
Ghada Khojah
Business school, Salford University, Manchester, U.K.
Keywords: Electronic Medical Records, Dooyeweerds’ Aspects, Down-To-Earth Issues Approach.
Abstract: Electronic medical records (EMR) offer much potential. However, various problems have made the
widespread use of EMR an unachieved reality (West and Blake, 2009). The problems reached such levels
that in some countries, the transition from paper to electronic version has slowed down, if not stopped. For
example, the U.K. NHS abandoned some of its ambitious plans for full transition from paper to electronic
medical records (Daily Mail, 2011 Aug 03). In other countries, like Saudi Arabia, some started questioning
the wisdom of electronic systems, and seek new methods of implementations, that do away from the
previous mistakes. To address these issues, one needs to discover what went wrong. The myriads of issues
involved, is proving rather complex, needing a sophisticated approach to expose them. Ahmad (2012) has
explored an approach called Down-To-Earth (DTE) which provides a rich picture of information systems
(IS) use. This paper adopts Ahmad approach to gain a richer picture of medical records. The DTE approach
is based on what is called Dooyeweerd's aspects, which is a set of distinct ways in which things like medical
records function and are meaningful. The main aim of this paper is to explore the potential of the Down To
Earth approach with Dooyeweerd's aspects as a way to better understanding health-care giver behaviour
with medical records, as a prelude to discussing how to effect more appropriate transition to EMR. By
health-care giver we include: physician, nurse, technician and administration.
1 INTRODUCTION
Electronic medical records (EMR) offer much
potential, over paper ones, but they have problems,
which made their widespread use an unachieved
reality (West and Blake, 2009), and reached such
levels that in some countries, the transition from
paper to electronic version has slowed down, if not
stopped. For example, in the U.K. the NHS has
abandoned its ambitious transition plans, (Daily
Mail, 2011 Aug 03). In Saudi Arabia, some started
questioning the wisdom of electronic systems, and
are seeking new methods of implementation.
There are myriads of issues involved, needing a
sophisticated approach to expose them. Ahmad
(2012) has explored an approach called Down-To-
Earth (DTE), which is based on Dooyeweerd's
aspects - a set of distinct ways, or viewpoints, from
which things are look at - which provides a rich
picture of information systems (IS) use, and hence
was adopted by this study.
The main aim of this paper is to explore the
potential of DTE, in extracting hidden EMR issues
that will improve the transition to EMR process.
2 LITERATURE REVIEW
This literature review confines itself to a summary
of discussion about the potential and problems of
electronic medical records (used here synonymously
with 'electronic health records.
2.1 The Potential of Electronic Medical
Record
Paper medical records are often incomplete, out of
date, illegible or difficult to read, leaving clinicians
without crucial information when trying to make
decisions on treatment protocols and medications
(Bliemel and Hassanein, 2004). EMR, as Ofri
(2010) suggests, are: more efficient; safer (see also
Fetter, 2009); can solve record movement issues
(McDonald, 1997); enhance physician order entry,
hence preventing serious medication errors
(Mukherjee and McGinnis, 2007) and help to reduce
277
Khojah G..
A New Approach to the Transition from Paper to Electronic Medical Records.
DOI: 10.5220/0004362502770283
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2013), pages 277-283
ISBN: 978-989-8565-37-2
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

duplication of patient records, (Hardiker et al.,
2000). All such issues are time savers.
Stausberg, et al., (2003) have noted that paper
and electronic-based records, of patients, are
generally used in unison, for the benefit of
implementing different tasks.
2.2 Problems with EMR
Some problems arise from the design of the EMR
system. McDonald (1997) draws attention to
hardware problems, such as interference between the
EMR system and electronic equipment. Berg (1997)
raises the 'rush hour' problem, where many
information sources exchange procedures of
laboratory results and other information at the same
time causing "important obstacles to the network's
smooth functioning".
Often the user interface is of a design that does
match the users' needs or the way they work.
Traditionally information is entered by filling pre-set
fields, but Pallav (2006) mentioned that a narrative
format is preferred by some doctors, especially some
psychiatric practitioners. Walsh (2004) explains,
"every patient tells a story...", and "the patient is
seen as a page ….and the doctor becomes the author
of stories within the medical record". However, as
Pallav (2006), points out, narrative style might make
design and implementation of EMR more difficult,
both in specific data of patient and the structure of
the data in the system. Standardization of not just
format but also of the exact meaning of pieces of
information becomes a challenge (Altiwajiri, 2010).
IT skills is a major complex problem (Walsh
2004). Devitt and Murphy (2004) stated that doctors
needed to be taught, or to have, information skills,
and Altiwajiri (2010) confirms that there is a general
illiteracy of IT-related issues among health care
people.
As there are many stake-holders in EMR, (Berg
and Bowker, 1997), (Berg, 1997) suggested that
physicians need to be made part of the IS, to
overcome their "learning to type" objections.
Dick and Steen (1991 cited by berg, 1997) draw
attention to costs, and Miller and Sim (2004) argue
that there are financial barriers to the use of EMR.
There are also important legal and ethical issues that
need addressing (Davis and Konikoff, 1998), as well
as, as Berg and Bowker (1996) argued, that potential
of sociological perspectives that has not been
sufficiently recognised.
Ilie, Courtney and Slyke (2007) analysed the
reactance of physicians to usage, and eventual,
acceptance of EMR. Altiwajiri (2010), also shares
this point in Saudi Arabia, where his research was
conducted. Timmons (2003) notes this reaction is
not limited to physicians but also includes nurses.
He finds that resistance is to both the
implementation and use of computer systems, and to
both the ideas and the ways of working of such
systems, and cites Dowling as giving the following
types, or forms, of resistance: passive resistance
(non-cooperation), oral defamation, data sabotage
and refusal to use. Pallav (2006) claims that "many
EMR system[s] are rejected by clinician because
they are not based on a story metaphor".
On the other hand, 'Learning to type' is not just a
matter of training, but an issue of self-belief and
vision for one's work. Physicians argue that
'learning to type' is not they are trained to do.
Altiwajiri (2010)'s study also encountered a
multitude of religious-related issues.
2.3 The Need for a New Approach
The picture given in the literature is one of
confusion, with a wide variety of advantages of
EMR but also a wide variety of problems. Because
of this, Stausberg et al., (2003) suggest that paper-
based and electronic-based patient records are often
used in unison, to support a variety of tasks.
Problems cited by many studies cannot be relied
upon because the research methods used are not
made clear. Few studies give much attention to the
patient, for instance, and Davis & Konikoff (1998)
survey medical students.
Ahmad (2012) argues that the traditional
approaches to IS use in general (of which EMR is
one specific type) cannot address the problems that
really matter to bring about high quality IS use. She
suggested that there are a number of deeper
problems with the way in which traditional
approaches view IS use.
First, the problem is of wrong perspective. Most
discussion of IS use is in terms of what
management, ICT suppliers, academics etc. find
meaningful, rather than in terms of what the users
'on the ground' find meaningful. Altiwajiri's (2010)
study is an example of this. He discusses a range of
issues, including IT-illiteracy, standardization,
resistance and general religious issues, but he
explicitly states that these issues are from the
perspective of the designer, management or
government. According to Ahmad, taking the
perspective of the user is one reason why IS’s failure
is so common. Judging by resistance of nurses, and
some physicians, this is the case in EMR too. This
problem was touched by Timmons's (2003) study,
HEALTHINF2013-InternationalConferenceonHealthInformatics
278

which mentioned that "Resistance was as much
about the ideas and ways of working ... as it was
about the actual technology being used".
Resistance by nurses has not been thoroughly
studied from a sociological perspective (Berg and
Bowker, 1997), so many sociological issues remain
hidden.
The plethora of problems discussed by Ahmad
(2012) has shown the potential for being directly
related to EMR. There is one problem she discussed
that might not apply. In many extant theories of IS
use, the issues tend to be of narrow scope and focus,
for example technical or economic issues.
2.3.1 Toward a New Approach: The
Down-To-Earth (DTE) Approach
DTE is a paradigm for research, has a philosophical
underpinning, and provides a methodology for
analysis. Under the DTE paradigm, the issues that
matter are those of the everyday activity of people
that relate to their use of IS, rather than those of ICT
suppliers, academics or management.
The method devised by Ahmad employs open
interviews, with the interview transcripts being
analysed by reference to aspects. During analysis
phase, Ahmad first employed a standard qualitative
analysis technique, but then used Dooyeweerd's
aspects to extract DTE issues from transcripts.
There are three ways by which meaningful issues are
revealed in the transcript text: first directly from the
words used, second making inferences by deduction,
third looking for indirect effects while looking at
interviewee's background. Using aspects helps to
reveal multiple meanings of the situation to the one
respondent.
In this way the diverse complexity of medical
records use can be investigated more systematically.
It matters now whether the medium of the IS is
paper or electronic is of secondary importance to the
human activity with the information itself.
2.3.2 Dooyeweerd's Aspects:
Dooyeweerd suggested that there are, at least, fifteen
diversified aspects, or ways of being meaningful,
which one can utilise to look at reality. Appendix 1
lists them. The first three aspects - quantitative,
spatial and kinematic - are what Dooyeweerd called
mathematical aspects. The next three - physical,
biotic and psychic/sensitive - are pre-human aspects,
in that they govern material, plants and animals. The
next three - analytical, formative and lingual - are
aspects of individual, cognitive human life. The next
three - social, economic and aesthetic - are
organisational aspects of living together. The final
three aspects - juridical, ethical and pistic/faith - are
of global or societal reality. It must be said that,
Dooyeweerd did not think of these aspects as
exclusive, but rather a mere proposal.
2.3.3 Using Dooyeweerd's Aspects to
Understand Potential and Problems
As an example, the potential and problems of EMR
will be analysed by reference to aspects. Each is a
potential and problem precisely because it is
meaningful in a certain way, as shown in Table 1.
For example, costs are meaningful by virtue of the
economic aspect, not any other aspect.
3 VALIDATING THE APPROACH:
INITIAL RESULTS
40 interviews were undertaken in four hospitals in
Saudi Arabia, involving health-care givers in four
hospitals. The interviews have been transcribed and
are in the process of being analysed for Down-to-
Earth issues that are meaningful to the interviewees.
In some hospitals some EMR is in place while others
still use paper records. The aim of the interviews
was to discover kinds of DTE issues that relate to
using medical records of either type, in order to
disclose what is important in such use, so that such
issues can be taken into account in any transition to
EMR.
The following is a selection of small parts of the
transcript, to demonstrate the method by which DTE
analysis using aspects is carried out. The method is
to seek to find, from within the respondent's answer
to the researcher's question, what the health-care
giver on the ground finds meaningful. As will
become plain, and in most cases, the respondent
goes beyond merely answering the question
bringing-in other material that is meaningful to
them. Sometimes they bring in something they
grumble about, and sometimes they branch off onto
other matters that occur to them while speaking.
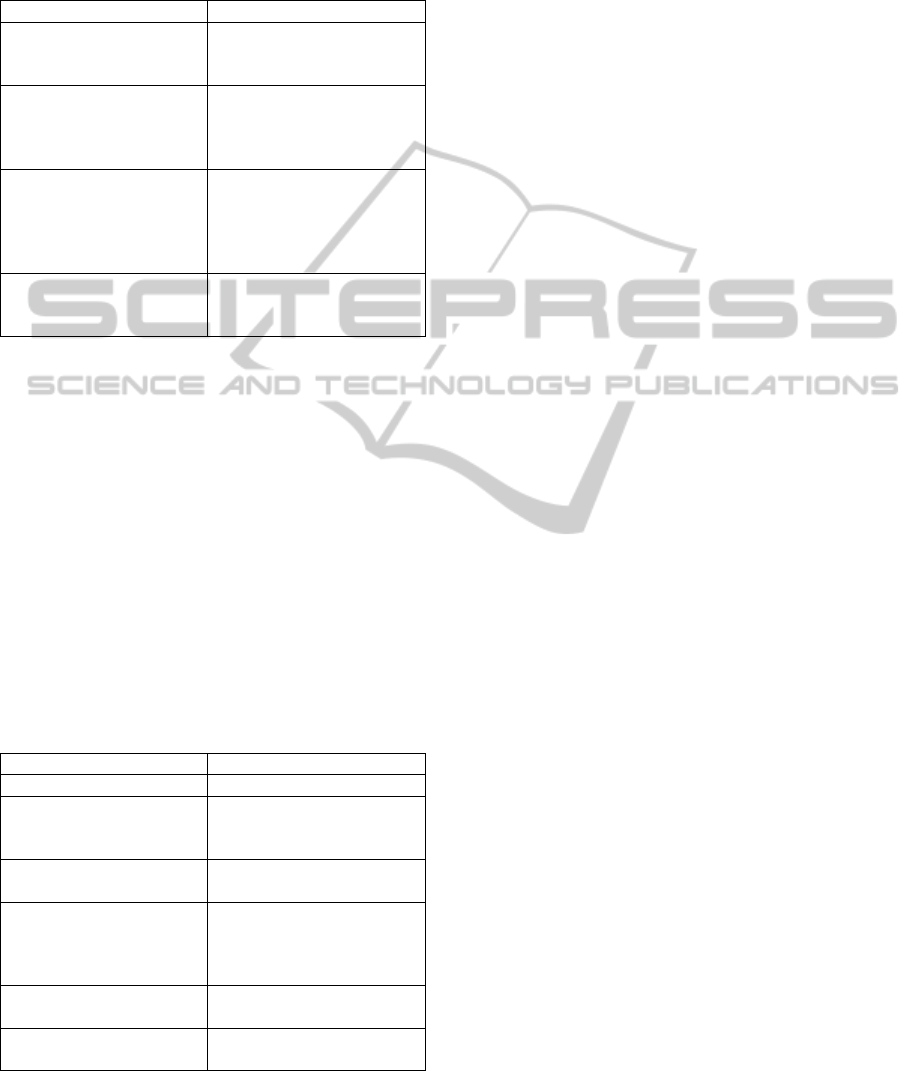
Tailing each Q&A is a table of DTE issues involved,
in each Q&A session, as in Table 2.
Q: which is better to work on, the paper file or on
the electronic file?
A: both are good, but both must be correctly used.
Because I cannot tell you which is better, because
this requires study. Therefore, in order to know
which is better, we must do brain storming. And all
concerned parties must meet to take such a
ANewApproachtotheTransitionfromPapertoElectronicMedicalRecords
279
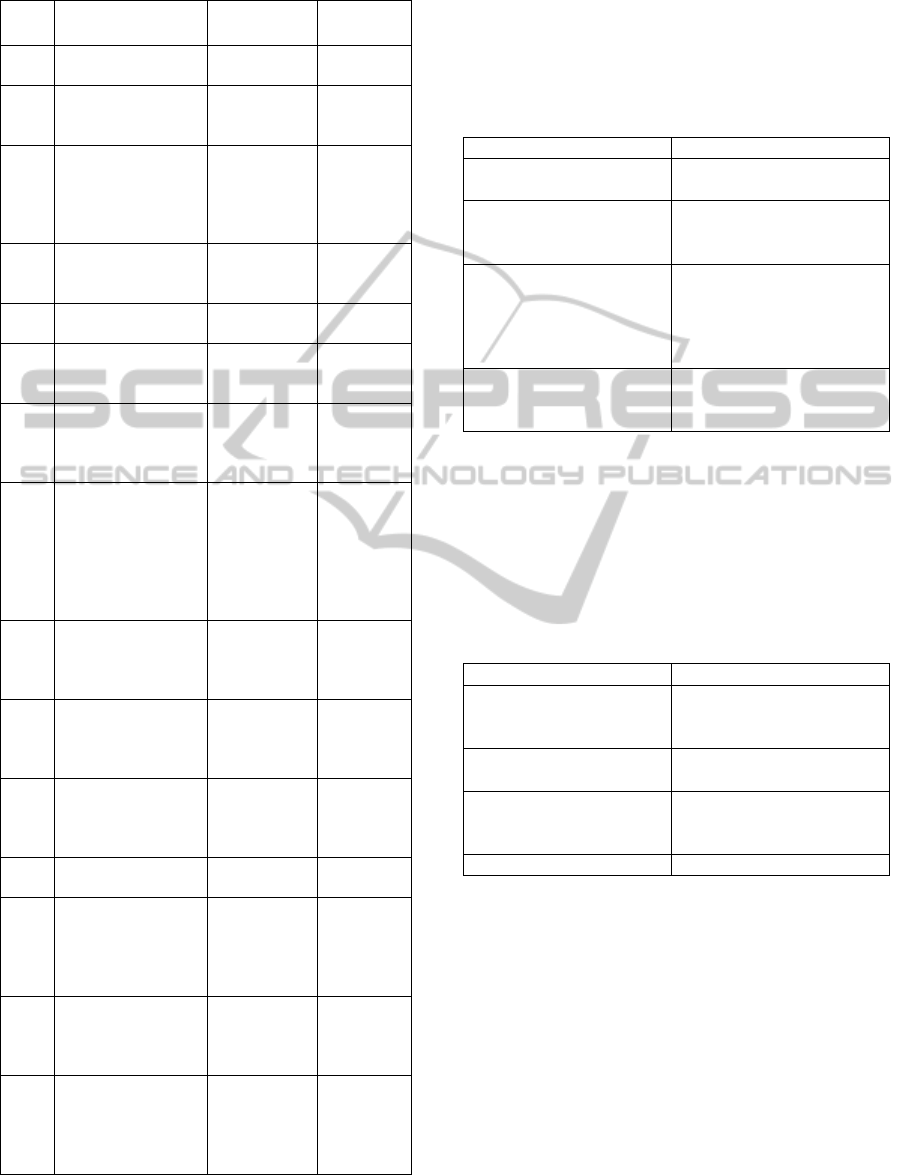
Table 1: A list of Dooyweerds’ aspects is shown.
Aspect
Potential o
f
EMR
Problem
of EMR
1
Quantitative
(Discrete amount).
2
Spatial
(Continuous
extension)
3
Kinematic
(Flowing movement)
The presence
of other
extant
electronic
data sources.
4
Physical
(Fields, Energy,
mass.)
5
Biotic/organic
(Life, organism)
6
Sensitive/psychic
(Sensing, feeling,
emotion)
7
Analytical
(Distinction,
concepts
Abstraction, logic)
8
Formative
(Deliberate shaping,
Technology, skill,
history)
EMR
Productivity
-Narrative
format.
-
technological
barriers for
the use of
EMR
9
Lingual
(Symbolic
signification)
Narrative
format is
preferred by
some doctors.
10
Social
(Relationships, roles)
a multitude
of culture-
related
issues.
11
Economic
(Frugality, resources;
Management)
EMR is safer
than paper.
financial
barriers for
the use of
EMR
12
Aesthetic aspect
Harmony, delight
13
Juridical
(Due',
appropriateness;
Rights,
responsibilities)
EMR is more
efficient work
legal issues
14
Ethical
(Attitude, Self-giving
love)
Resistance
from nurses
and
physician
15
Pistic/Faith
(Faith, commitment,
belief;
Vision of who we
are)
Physicians
learning to
type
decision and to take the appropriate decision about
which is better. I, on my own, cannot decide that,
but there are some documentations that i can do for
them minimizing and they become wireless.
Table 2: A DTE issues list, stemming out of the Q&A,
above is shown.
Aspect DTE Issues
Juridical
both are good, but both
must be correctly used.
Analytic
in order to know which is
better, we must do brain
storming.
Social
-all concerned parties must
meet to take such a
decision.
- I, on my own, cannot
decide that.
Formative
I can do for them
minimizing and they
become wireless
Q: who is responsible to print the lab results?
A: it’s both the nurse and physician can do it but
90% nurses do it like me. Some doctors will initially
look at the system but they will eventually print it
out. It’s a habit formative. A DTE list, of this Q&A
session, is shown in Table 3.
Table 3: A DTE issues list, stemming out of the Q&A,
above is shown.
Aspect DTE Issues
Juridical
it’s both the nurse and
physician can do it but
90% nurses do it like me
Lingual
Some doctors will initially
look at the system
Economic
but they will eventually
print it out. (waste of paper
)
Formative It’s a habit
Q: Why does the nurse writes the nurses note in a
form of a story?
A: its mean explain the details of the patient's
condition written in a form of a story. I already told
you that lack of improvement and development
caused shortage and the absence of update.
Documentation that is particular for nurse is
supposed to developed and updated by the ministry
because since 8 years ago nothing has changed and
never developed. And when we ask for position
paper, I think it does not l exist, especially the nurse
that makes the position of the patient. Also, as for
the emergency nurses’ notes, we still update them
through personal efforts from emergency
HEALTHINF2013-InternationalConferenceonHealthInformatics
280
management. A DTE list, of this Q&A session, is
shown in Table 4.
Table 4: A DTE issues list, stemming out of the Q&A,
above is shown.
Aspect DTE Issues
Lingual
its mean explain the details
of the patient's condition
written in a form of a story
Economic
The lack of improvement
and development caused
shortage and the absence
of update
Juridical
since 8 years ago nothing
has changed and never
developed (implies they
did not do what they
should do )
Ethical
the emergency nurses’
notes, we still update them
through personal efforts
Q: Do you think can stop to print the lab results?
A: it will be very useful. But sometimes doctors
are too busy to sit in front of the computer all the
time. It’s only a matter of getting used to it. Do you
want to know how many pages we fill up? I will
show you later the ICU sheet. This is just one thing
they fill everything, every sheet. Now these are
loads of pages. Aside from this one there are other
papers as well. So it’s all about documentation. We
don’t spend too much time with the patient. This is
time consuming.
Sometimes, my staff look at me and cry. Even
after going home I am working, for 14 hours. A
DTE list, of this Q&A session, is shown in Table 5.
Table 5: A DTE issues list, stemming out of the Q&A,
above is shown.
Aspect DTE Issues
Aesthetic it will be very useful
Economic
sometimes doctors are too
busy to sit in front of the
computer all the time.
Faith
It’s only a matter of
getting used to it.
Lingual
This is just one thing they
fill everything, every
sheet. Now these are loads
of pages.
psychic
Sometimes my stuff look
at me and cry
Juridical
Even after going home I
am working, for 14 hours
In making the aspectual analysis, the analyst
looks for which aspect makes what they say
meaningful, usually sentence by sentence but
sometimes by phrase or by group of sentences. The
analyst asks themselves "Why did the respondent
say this rather than keeping silence or saying
something else; which is the main aspect that makes
this utterance meaningful?"
4 REFLECTION ON ANALYSES
These are demonstration analyses, but are similar to
those made by Ahmad (2012). We do not claim that
they are representative of the entire plethora of
meaningful issues, but merely seek to highlight
some of the ways that using aspects can facilitate
understanding DTE issues:
Aspects help us appreciate the diversity of
issues that are meaningful to health-care givers
concerning medical records. This is because
they help us distinguish one way of being
meaningful from another, using a
philosophically sound set of spheres of
meanings. Thus, for example, from the
analyses above, we find: 1 psychic aspect, 1
analytic, 2 formative, 3 lingual, 1 social, 3
economic, 1 aesthetic, 4 juridical, 1 ethical and
1 faith aspect. This confirms that DTE issues
are of many kinds, even more than was
apparent through the literature review.
Aspects provide support for that which is
intuitively felt as important to health-care
givers, which might not be revealed in normal
interviews or questionnaires. This is because
they are allowed to bring out any matters that
occur to them, and aspects provide the analyst
with a way of judging why they might be
meaningful (rather than merely verbal
padding). In this way, things that the
respondent might have felt were trivial, or
embarrassing, are revealed, as was found by
Kane (2005).
In such ways, aspects give priority to the
respondents' answers over the researcher's
questions. In this way, DTE issues are
disclosed that the researcher might not have
thought about. Aspects give incentive to take
what the respondent says at face value.
Aspects can stimulate the researcher to make
deductions about meaningful issues, not on the
basis of bias, but of shared ways of being
meaningful. This discloses DTE issues that
would ordinarily be hidden (taken for granted
or indirect).
Aspects provide a way of broadly classifying
ANewApproachtotheTransitionfromPapertoElectronicMedicalRecords
281

issues. Admittedly this is quite broad when
taken to one level, but Dooyeweerd provides
points to more sophisticated analyses, at
several levels, and employing notions of
aspects with special roles: qualifying, leading
and founding. These will be investigated
during the main study.
Aspectual profiles can be generated by counting
things in each aspect and comparing counts.
We might, for example, compare the counts
from above analyses with a count of the
number of times each aspect is deemed
important in the extant literature.
Guidelines for transition to EMR can be obtained
both from the list of DTE issues revealed, collated
under aspects, and also from the general form of
aspectual meaningfulness. In each aspect we can
expect that a number of issues will have surfaced,
but not all. The revealed issues can form the core
for proposals, but the possibility of still-hidden
issues will motivate flexibility in design. The design
of both technical system and human context are
important, and aspects provides for their integration.
5 CONCLUSIONS
This paper has applied Down-to-Earth issues
technique to medical records, in the hope of
facilitating better transition from paper to electronic
records. Medical records are seen as a kind of
information system (IS), which needs to be
considered from the perspective of its users 'on the
ground' (health-care givers), which possesses many
hidden issues, the wide variety of which needs to be
understood and managed. Dooyeweerds’ aspects
provide the core idea, which are spheres of
meaningfulness in which all MR activity functions,
and which are all important. The potential of
aspects has been demonstrated by aspectual analysis
of several interview transcripts.
There are several venues for future work. This
research will continue analysing the 40 transcripts to
find more multiple and hidden meanings from a
users' perspective. Aspectual profiles will be
formed, by cohort, by hospital type, and overall, to
ascertain the kinds of issues that each tends to find
meaningful and, more importantly, to identify the
kinds of issue that each might have overlooked.
These profiles will be compared and contrasted with
cohorts in the literature, to identify over- and under-
emphasis on issues therein. The DTE issues that
emerge from transcript analysis can be collated
under their aspects to provide a comprehensive view
of what needs to be discussed when planning
transition to EMR. Exactly how this will be carried
out has yet to be explored.
6 CONTRIBUTIONS
The DTE method (Ahmad, 2012) have contributed
to the analysis methods, in situations fogged by a
plethora of issues. DTE exposed hidden issues and
orientated toward a user's perspective.
The notion of Down-to-earth issues, with its
philosophical underpinning in Dooyeweerds’
aspects, can contribute to a theory surrounding
medical records, ranging from Weed's early work,
through theories of resistance to technology and
narrative form. The DTE approach can provide a
basis for their integration, so that insights from
different theories can be seen as part of a wider
picture. Identifying which kinds of issues are over-
and under-emphasised in research literature, can
provide strategic guidance to research and academic
discourse about EMR.
The method for revealing DTE issues promises
to ease the study of problematic medical record
situations. It can guide managers and system
designers in drawing-up guidelines for the benefit of
the transition process from PMR to EMR. It can
guide government organizations in drawing-up
relevant, useful and easy to follow policies on all
EMR pertaining issues, from an everyday life
perspective. These tasks would build on the DTE
aspects, thus avoiding pitfalls that other
implementation exercises have faced. These
contributions are relevant to all cultures and
countries, but could be particularly useful for those
like KSA, when embarking on feasibility studies, or
are just about ready to start implementing such
transitions.
REFERENCES
Ahmad, H. 2012. Down-to-earth issues in (mandatory) IS
use. PhD Thesis, University of Salford, Salford, U.K.
Altiwajiri, M. 2010. 30 Connected e-hospitals in 24
months Saudi cases study. HIMMS Middle East
conference, Middle East.
Berg, M. 1997. Of forms, containers, and the EMR: tools
for a sociology of the formal science, technology &
human values. SAGE, vol 22, p. p. 403.
Berg, M., Bowker, G. 1997, The multiple bodies of the
medical record: Towards a sociology of an artifact.
The Sociological Quarterly, 38(3), pp. 513-537.
HEALTHINF2013-InternationalConferenceonHealthInformatics
282

Bliemel, M., Hassanein, K. 2004. E-health: applying
business process reengineering principles to healthcare
in Cnada. International Journal of Electronic Business,
vol 2, no. 6, pp. 625-643.
Chris, D. 2010, EHRs prove a difficult witness in court.
Journal of AHIMA, no. 24th Sept 2010.
Ofri, D. 2010. Doctor vs. the computer. The New York
Times, 30 Dec 2010.
Davis, F. (1989) Perceived usefulness, perceived ease of
use, and user acceptance of information technology,
MIS Quarterly, 13:3, 319-339.
Davies, L., Domm, J. A., Kinokoff, M., Miller, R. A.
1998. Attitudes of first-year medical students toward
the confidentiality of computerized patient records. J
Am Med Inform Assoc, no. 6:1, pp. 53-60.
Devitt, N., Murphy, J. (2004). A survey of information
management and technology training needs of doctors
in an acute NHS trust in the United Kingdom. Health
Information & Libraries Journal. Vol 21(3): 164-172.
Dooyeweerd, H. 1955. A new critique of theoratical
thought, 1975 edn, Paideia Press, Jordan Station,
Ontario, USA.
Fetter, M. S. 2009. Improving information technology
competencies: implications for psychiatric health
nursing. Issues in Mental Health Nursing (Informa
Healthcare), vol 3, p. 13.
Hardiker, N. R., Hoy, D., Casey, A. 2000. Standards for
Nursing Terminology. J Am Med Inform Assoc
2000;7:6 523-528.
Ilie, V., Courtney, J., Van Slyke, C. 2007. Paper versus
Electronic: Challenges associated with Physicians'
Usage of Electronic Medical Records, Proceedings of
the Hawai'i International Conference on System
Sciences.
McDonald, C. J. 1997. The barriers to electronic medical
record systems and how to overcome them. J Am Med
Inform Assoc, vol 4, no. 3, pp. 213-221.
Miller, R. H., Sim, I. 2004. Physicians' use of electronic
medical records: barriers and solution. Health Aff
(Millwood ) 2004;23(2):116-26.
Mukherjee, A. McGinnes, J. 2007. E-healthcare: an
analysis of key themes in research. International
Journal of Pharmaceutical and Healthcare Marketing,
vol 1, no. 4, pp. 349-363.
Pallav, S. 2006. Customizing clinical narrative for EMR
interface using cognitive method. International Journal
of Medical Informatics, vol 75, pp. 346-368.
Stausberg, J., Koch, D., Ingenerf, J. Betzler, M. 2003.
Comparing paper-based with electronic patient
records: lessons learned during a study on diagnosis
and procedure codes. J Am Med Inform Assoc, vol 10,
no. 5, pp. 470-477.
Sullivan, J., Sullivan, F. 2005. ABC of health informatics
what is health informatics. BMJ, vol 331, p. 1391.
Tange, H. J., Dressen, V. A. B., Hasman, A., Donkers,
H.H.L.M. 1997. An experimental EMR system with
multiple views on med. narrative. ELSEVIER Journal
of Computer Methods & Programs in Biomedicine,
vol 54, pp. 157-172.
Timmons, S. 2003. Nurses resisting information
technology. Wiley Online Library, pp. 257-269,
viewed 15 Sept 2012.
Walsh, S. 2004. The clinical perspective on EMR & how
they can affect patient care?. BMJ, vol 328, p. 1184.
West, S., Blake, C. 2009. Reflections on the use of
electronic health record data for clinical research.
Health Informatics Journal, vol 15, no. 2, pp. 108-121.
ANewApproachtotheTransitionfromPapertoElectronicMedicalRecords
283
