
Contextualized Access to Electronic Health Records
Application to Hospital Interoperability
Bel´en Prados-Su´arez
1
, Carlos Molina
2
, Miguel Prados de Reyes
1
and Carmen Pe˜na-Ya˜nez
3
1
Department of Software Engineering, University of Granada, Granada, Spain
2
Department of Computer Sciences, University of Ja´en, Ja´en, Spain
3
Computer Science Department, San Cecilio Hospital, Granada, Spain
Keywords:
Contextualized Access, Interoperability, EHR, Electronic Health Records.
Abstract:
Everyday more hospitals develop their own Electronic Health Record (EHR) Systems to improve the accessi-
bility to the information on it. There are some standards and proposals to homogenize the structure of these
EHR, but they use to be so generic, that the final EHR structure has so many particularities that is different
in each hospital. This situation has created a huge problem of interoperability, since Hospital Information
Systems (HIS) are not capable of communicating nor understanding each other. At this point it seems very
difficult that all the Hospital Information Systems change their EHR structures into a common one, to get this
communication capability. Proposals to solve this issue require to create a common EHR or to translate all
the existing EHR structures into a common one, and both cases seem to be unapproachable. This is why we
propose a different approach based on the contextualized access to the information. The underlying idea is that
the assistance acts, i.e. situations or contexts, where the information is acceded, as well as the data required
for each, i.e pertinent information, is almost the same independently of the hospital where you are. Hence, it
is not necessary to establish a correspondence between the EHRs, we only need to identify the context of the
extern access and retrieve and send the information pertinent to it. In addition, our proposal also allows the
adaptation to the needs of information of each medical doctor in each Hospital, as well as solves the problem
of EHR fragmentation.
1 INTRODUCTION
Everyday more hospitals join to the digitalization
of the medical records, which is giving room for a
wide variety of proposals to structure the information
into the Electronical Health Records (EHR). Some
of them are specific for concrete medical specialities
(Karahoca et al., 2010) or for the sanitary system of
a given country (Stan et al., 2011). This variety of
proposals has shown up the necessity of standardiza-
tion, and this is where the standards HL7, Open EHR,
SNOMED-CT, DICOM and the proposal of the Euro-
pean Committee for Standardization, the ISO 13606
regulation, come into play.
However these proposals are so generic, flexible
and abstract, to allow the versatility of the informa-
tion to be stored into the EHR, that the concrete im-
plementations in each hospital end up being quite dis-
similar. Is has made arise serious interoperability is-
sues: on the one hand several venues of the same hos-
pital can’t access the EHR stored at the other; on the
other hand there are no good connections between the
part of the EHRs stored in the primary attention cen-
ters and the hospital EHR; and in addition, when a
patient moves from one hospital (with its own EHR
structure) to a different one (with a different EHR im-
plementation) there is no way to access the from one
of them the information generated in the other one,
generating the EHR fragmentation problem.
Up to the moment the interoperability issue has
been faced in the literature from different points of
view:
• At the machine or communication protocol level,
viewing the problem as the integration into an
EHR structure the information produced from
the different medical equipments and devices like
PACs (Liu et al., 2011; Hu et al., 2011).
• From the security point of view, remarking the
need of authentication methods and identity man-
agement when the different Hospital Information
Systems (HIS) try to communicate (Campos et al.,
2011).
272
Prados-Suárez B., Molina C., Prados De Reyes M. and Peña Yañez C..
Contextualized Access to Electronic Health Records - Application to Hospital Interoperability.
DOI: 10.5220/0004453602720279
In Proceedings of the 15th International Conference on Enterprise Information Systems (ICEIS-2013), pages 272-279
ISBN: 978-989-8565-59-4
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

• As the need of knowledge mobilization, to be able
to access only the relevant parts of the EHR for
the emergency situations where mobile devices
are used (DePalo and Song, 2011).
• The problem of EHR fragmentation (Vergari
et al., 2011) and the need of making the EHR
more “person centric” by using cloud storage and
computing (Van Gorp and Comuzzi, 2012) or in-
tegrated databases (de la Torre-Diez et al., 2013),
but with the inconveniences of the personal data
protection and database matching issues respec-
tively.
• It is also essential to deal with the issue of the
semantic understanding between different HIS,
which has been approached in two different ways:
as the construction of an Ontology to share the
information (Arch-Int and Arch-int, 2011), or by
means to the transformation of the OpenEHR
archetypes into ISO EN 13606 and vice versa
by combining Semantic Web and Model-driven
Engineering technologies (Martinez-Costa et al.,
2010). However, although these proposals allow
logical and structured access to the information,
they don’t describe how to exploit the Ontology
nor the Archetypes to get interoperability between
systems, nor they avoid the uncomfortable se-
lections steps and the successive screen-shots to
reach the desired information (Miguel Prados de
Reyes and Su´arez, 2006).
Only a few proposals are capable of facing some
(not all) of these problems at once, and they are
mainly based of the use of frameworks that work as
intermediaries between HIS, working in two stages
as Halevy suggests in (Halevy, 2011). His proposal
is to first translate all possible clinical terminologies
and definitions of all the EHR to communicate into a
common format that will be used as local EHR. Then,
in the second stage, the interoperability system will
semantically organize the information to ensure that
its meaning stays true in whatever environment the
record is used. This is a theoretical proposal similar to
the previous one of Sunil Kumar (Sunil Kumar et al.,
2010), consisting on the creation of their own EHR
structure, and the translation of every EHR of the HIS
to communicate into their EHR proposal. Once done
it, they have developed a healthcare information ex-
change software based on a proposed adaptable stan-
dard. This way they create a complete EHR of patient
which is interoperable in healthcare systems accord-
ing to their information exchange standard. Never-
theless these proposals have two main drawbacks: the
need to translate each EHR of each different HIS into
the local or proprietary one, and the above mentioned
problem of the limited agreement on the standards to
be used in the second communication stage.
In addition, none of the existing proposals face the
problem as a whole, considering simultaneously all of
the above mentioned implications and supplying an
integrated solution, which doesn’t require the change
or translation of different EHR structures. This is pre-
cisely our aim here. In (Prados-Su´arez et al., 2012;
Prados-Suarez et al., 2012) we proposed to improve
the accessibility of the information based on the iden-
tification of the context of the access and the informa-
tion pertinent to it, that we have developed in collab-
oration with the University Hospital San Cecilio from
Granada. Here we extend this proposal to solve the
problem of the interoperability.
In section 2 we summarize the characteristics of
the system that we take as example and reference, so
it can be seen that it is common to the majority of
the HIS, and hence our proposal is easily applicable.
Then, in section 3, we show our proposal to access
the information based on the contextualization of the
situation from which it is required, and how to de-
terminate the pertinent information for each context.
In section 4 we propose how to exploit this contex-
tualized access to solve the interoperability problem.
Finally, in section 5, we summarize our conclusions.
2 BACKGROUND AND SYSTEM
DESCRIPTION
Next we briefly describe the ISO 13606 standard and
the main characteristics of the HIS that we have taken
as reference.
2.1 CEN/ISO ISO 13606
The ISO 13606 (ISO-13606, 2008) proposes a dual
model. The first one is the reference model and estab-
lishes a basic structure for the data using an object-
oriented paradigm defining the main classes with the
characteristics to store for each one. The second
model sets the Archetypes as a way to define the clin-
ical concepts or sets of clinical information items,
managed by the systems and with a concrete clini-
cal meaning (from the pregnancy protocol to the bio-
chemistry information or HDL-cholesterol item in-
side an analysis).
2.2 EHR Information System
The HIS of the San Cecilio Hospital stores around
800.000 EHR, containing more than 50 millions doc-
uments, and it is having a fast increase in size due
to the inclusion of new types of documents from two
ContextualizedAccesstoElectronicHealthRecords-ApplicationtoHospitalInteroperability
273
sources: old documents that still have not been dig-
italized (scanned images, MRI, etc.) and new doc-
uments generated from newly acquired devices and
equipments like PACs.
This HIS gives service, not only to the Hospital
itself, but also to several venues disperse in the city of
Granada, including primary attention centers.
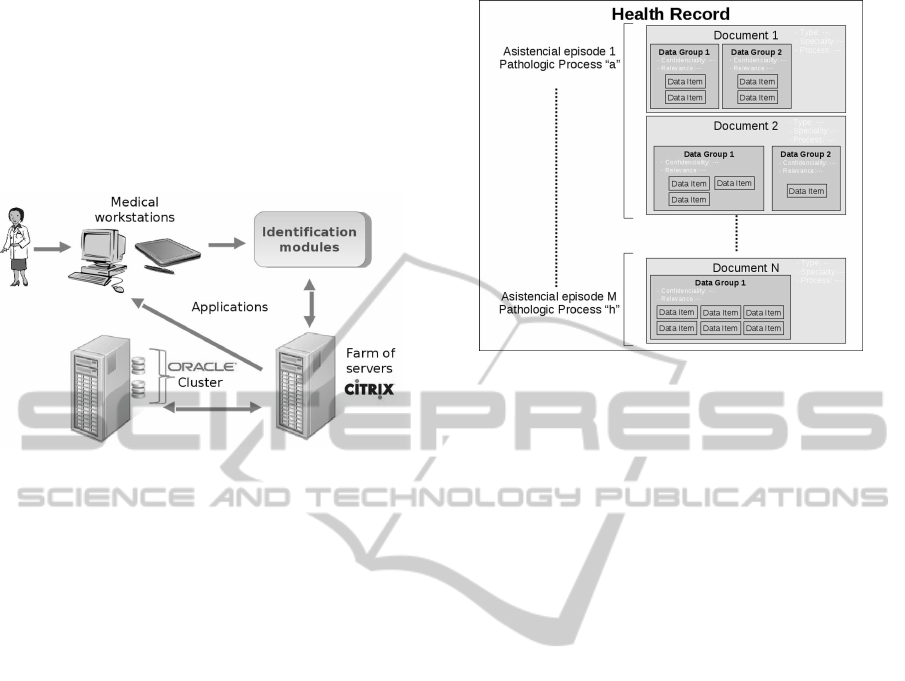
In Figure 1 we show the structure of the system.
Figure 1: Structure of the system.
This system, as legally demanded, stores each ac-
cess to the EHR and the data acceded, including the
staff member acceding and the assistance situation
(called “controlled assistance situation”) in which
the access occurs. In case of modification, it also
stores the modified data. From now on, we will call
this access data base as Retrospective Access Data
Base (RADB). The number of records stored in the
RADB is in the order of hundreds of millions. Our
proposal is based on the analysis of the registers of
this RADB since, it allows us to know which infor-
mation has been acceded and the related context.
2.2.1 Electronic Health Records Structure
As given by the ISO13606 Reference Model the EHR
structure is organized according to an Ontology with a
class structure with the classes Folder, Section, Entry,
Cluster and Element.
The EHR gathers all the documents of any type
generated in each assistance act of a patient, follo-
wing the structure shown in Figure 2). In (Prados-
Su´arez et al., 2008), can be found the properties used
to characterize each document in the EHR, which are
organized according to assistance episodes and classi-
fied considering 1500 different documents classes in
the system.
Items inside the documents can be grouped into
data groups: small logical units related under a clini-
cal point of view. Each data group has its own specific
properties, but also inherits the general properties of
the document where it is contained. The “special”
data group with the EHR’s and patient’s identifica-
Figure 2: Logical Organization of the EHRs.
tion, common to all the documents is discarded from
the processes explained later.
3 CONTEXT-BASED ACCESS TO
EHRS
In this section we briefly show the context-based
mechanism of access, but in (Prados-Su´arez et al.,
2012; Prados-Suarez et al., 2012) can be found a more
detailed explanation of this system.
Definition 3.1. We call Context to a situation in
the doctor-patient relationship inside an assistance
act, requiring an access to the information previously
stored in the EHR.
We set three criteria according to which it is ob-
jectively reasonable to identify the set of contexts:
pathological process, medical specialty and kind of
assistance.
To automatically detect the situation or context
where a medical doctor accesses an EHR we consider
the following variables: type of medical staff (spe-
cialty and position), type of the medical workstation
(type of terminal, medical unit associated and physi-
cal location) and type of the present and last patient’s
appointments.
To identify the data groups for each context we
introduce the concept of pertinence:
Definition 3.2. We define the pertinence of a concrete
data group for a given context as its relevance: the
more needed or interesting the data group is for the
context, the higher its pertinence to the context is.
This pertinence is calculated considering a the fo-
llowing factors:
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
274
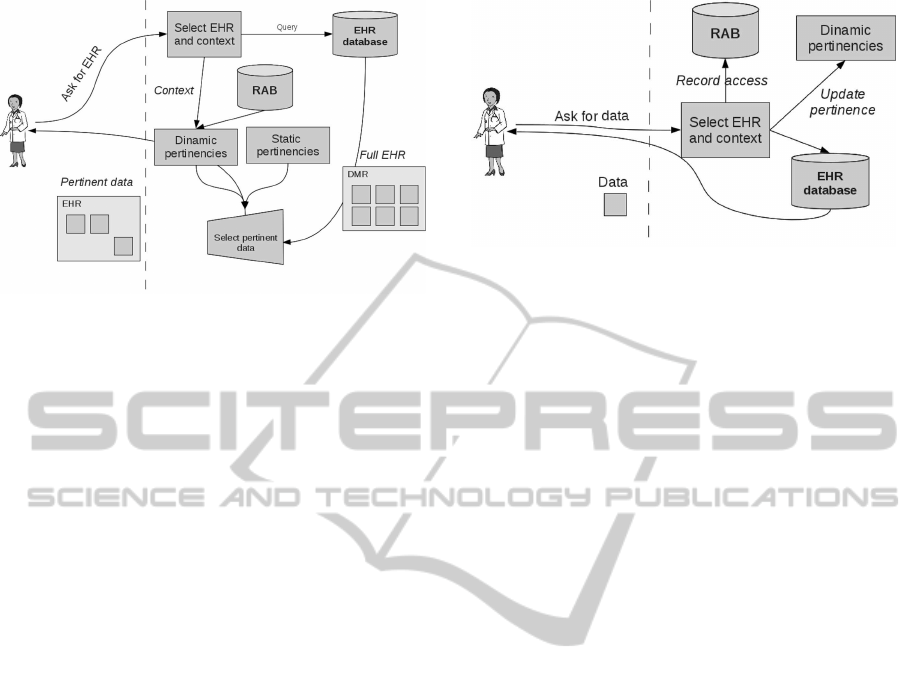
Figure 3: Scheme of the contextualized query process.
• The regulations about each clinical process: P
R
Dc
.
• The opinion of the concrete doctor: P
C
Dc
.
• The data groups with a great and especial impor-
tance for a given patient: P
P
Dc
.
• The aging of the information (loose of validity as
the time passes) or time pertinence: P
T
(D).
• The access patterns or restrospective pertinence,
obtained according to the accesses stored in the
RADB database: P
C
R
(X)
Next definition aggregates this information:
Definition 3.3. Let X be a group of data in a docu-
ment D, and C a context, we define the global perti-
nence of X to C as
P
C
G
(X) = (P
R
Dc
(X)⊕P
C
Dc
(X)⊕P
P
Dc
(X)⊕P
C
R
(X))⊗P
T
(D)
(1)
All the pertinences are in [0, 1] and we have cho-
sen the maximum and the minimum as t-conorm and
t-norm because of their simplicity, and therefore, ef-
ficient and fast calculation as well as they are quite
extended.
This way a data group is relevant if the number of
accesses to it is high in comparison to the total num-
ber of accesses allowing, the update of the pertinence
according to the decreasing relevance due to the ag-
ing of the access and to automatically adapt to new
accesses patterns and future needs.
An scheme of the access process in shown in Fig-
ure 3. With this scheme we never loose the access
to the whole EHR, but we get the information in it
according its relevance for the present act. More in-
formation about the interface once logged, the process
to get a concrete data item and a comparison with the
context based access can be found in (Prados-Su´arez
et al., 2012; Prados-Suarez et al., 2012).
The update of the system is performed on each
access by the update of the retrospective pertinence
Figure 4: Scheme for pertinence’s update process.
when the access is logged in the RADB. A scheme
summarizing of the process is shown in Figure 4.
4 CONTEXT-BASED
INTEROPERABILITY
As previously seen proposals made so far lies in fo-
cusing their attention in the interoperability between
system structures, forgetting the real users of the sys-
tem. We change the approach and face it in a more
practical way, giving more importance to the users
and to satisfy their needs of information.
In a real situation, the medical staff does not need
to access the complete EHR of the patient but only
the portion of it related to the act in process. In other
words, in every hospital what a medical doctor needs
is the portion of information pertinent to the context
he/she is involved in. In addition, the contexts in most
of the hospitals are almost the same due to the medical
praxis is very similar in most of the institutions.
Considering these two premises, the main idea is
to apply the context-based access to the communica-
tion between systems such that given two hospital H1
and H2 with a context-based interface (Figure 5):
• A staff member inside a given context in H1 needs
information from H2.
• H1 sends to H2 the identification of the context.
• H2 retrieves the information defined as pertinent
for that context, stores the record of the access
performed and returns it as response to H1.
• H1 shows the received blocks of information to
the staff member in the usual interface of H1.
• If the information required is not in the received
block the communication process is repeated till
the desired data items are retrieved.
Based on the two premises above, in most of the
cases the information needed will be found in the first
blocks. Let us remark that each user works with the
ContextualizedAccesstoElectronicHealthRecords-ApplicationtoHospitalInteroperability
275
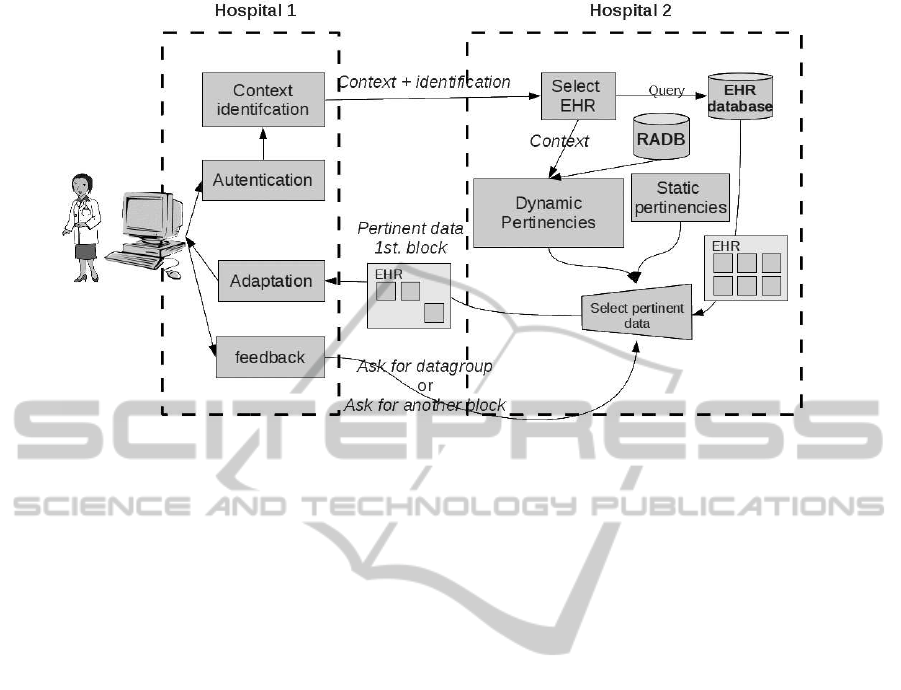
Figure 5: Scheme for an extern access.
usual interface of his/her hospital. Since the commu-
nication is made at the level of archetypes it is only
necessary that both systems support the archetype lan-
guage and that the user interfaces are context-based.
Even if H1 doesn’t have a context-based interface,
H1 could send the information that H2 needs to iden-
tify the context and H2 would perform the context
identification and return the information in any of the
standard formats for medical documents, like DICOM
for images and PDF or XML for textual information.
4.1 Archetype-based Contexts
As mentioned above, the CEN/ISO 13606 only de-
fines a general structure for EHR system interfaces
but not for the internal structure of the system. It is
figured out to establish the interoperability at the level
of archetypes because otherwise it would be neces-
sary to perform the translation of data and structures
between systems. Our proposal here is to define the
contexts as archetypes in such a way that the commu-
nication between institutions will be reduced to send
the identification of the context and get the informa-
tion pertinent to it in the archetype language.
4.1.1 Context Definition
To define the contexts as archetypes we need that their
definition is made as standard as possible. In addition,
the resulting set of contexts must be complete enough
to consider the widest set of possible contexts so all
usual access situations from hospital and institutions
are taken into account. Here we propose to define the
contexts based on the three criteria indicated above
but filling them with standard sources instead of per-
sonalizing them for a concrete hospital. Then the set
of contexts will be obtained from:
• Pathological Process. Each HIS must register all
the diseases defined by the World Health Organi-
zation (WHO) in the ICD, International Statisti-
cal Classification of Diseases and Related Health
Problems, even though they are unusual. Hence
a context for each will be created. The same pro-
cess can also be performed with the ICF (Inter-
national Classification of Functioning, Disability
and Health) and ICHI (International Classification
of Health Interventions).
• Medical Specialty. There are several standards
and correspondencesbetween medical specialities
in different countries, that can be used to create
the contexts. This is the case of the regulation of
the European Union related to the medical spe-
cialities that are automatically recognized in all
the EU plus Norway, Iceland and Liechtenstein or
the American or Australian listings.
• Kind of Assistance. This source has more variety
since it is more related to the internal work-flow
of the sanitary systems, but there are also some at-
tempts of standardization like the one in the Clin-
ical Care Classification (CCC) System or ICF.
In the ICD, ICF and ICHI the WHO has coded the
information (each disease, intervention, etc. has an
unique code), so it isn’t necessary to establish a cor-
respondence. Only in the case of the contexts defined
by medical speciality may be necessary to create a ta-
ble that stores the correspondences between different
sanitary systems. But, as can be seen, this is a very
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
276

simple and small table that, in addition, the system
can automatically complete with the use.
With it the spectrum of contexts covered is wide
enough to ensure a fluent communication and in-
teroperability in most of the usual cases, and only
very special and rare situations might not be covered.
However, even in these cases the access could be per-
formed, it will only require the more queries till the
desired information is found.
4.1.2 Context Identification
The local system at H1, prior to ask for the data, iden-
tifies the context of the access. The system sends it to
the extern hospital H2 when asking for the EHR using
an standard language for medical data like HL7. The
system at H2 looks for that context on its database.
If H2 finds the context, then looks for the pertinent
data groups and sends them back to H1. If the con-
text is not found, the H2 system uses the specialty of
the medical staff member at H1 to send back a list
of contexts related to that specialty. The medical staff
member at H1 selects then the more appropriated con-
text and H1’s system sends the choice to H2’s system.
Then the list of pertinent data groups is created and
sent back to H1. If the person at H1 selects one of
these data groups to see it, then H2 system makes a
correspondence between the required context and the
one selected from the list so in future accesses the sys-
tem can identify it, and send back the pertinent infor-
mation without this previous negotiation.
At this point let us remind that once acceded any
context it is always possible to access the whole his-
tory if necessary, so entering through a wrong context
only would mean that it will be necessary more mouse
clicks to reach the desired information.
4.1.3 Context Adaptation: Extern Pertinence
At this point arise questions like:
• How to obtain information that is pertinent in the
context of the hospital querying, but is not for the
same context of the other hospital.
• How the content of the context can reflect the
changes in the needs of information.
The response in all the cases is the same as in the
local system. To adapt the system to the peculiarities
of the accesses from each hospital or institution, we
introduce an extern pertinence This pertinence will be
learnt with the consecutive accesses in the same way
as explained above for the local system. To calculate
this pertinence the acceded data groups are stored in
a table like the RADB. Then, when a new access is
performed, this new pertinence (P
E
) is introduced in
the calculation of the global pertinence as follows:
P
C
G
(X) =
P
R
Dc
(X) ⊕ P
C
Dc
(X) ⊕ P
P
Dc
(X)
⊕P
C
R
(X) ⊕ P
E
(X)
⊗ P
T
(D)
Hence, as seen in figure 6, in the case of extern ac-
cesses both the local dynamic pertinence and the ex-
tern pertinence are considered. Tanking into account
only the extern pertinence would make the system un-
able to adapt to new needs in the case of few accesses,
due to the lack of information to update the perti-
nence. On the other hand, considering only the local
dynamic pertinence the system would never adapt to
the needs of the extern hospitals requirements, since
the extern accesses would never have enough weight
regarding the local number of accesses.
The first time the EHR is acceded for the extern
hospital, the P
E
is 0 for all the data groups and con-
texts, so the local information determinate the perti-
nent information. This access updates the extern per-
tinence and is stored for future accesses (increasing
the P
E
for some data groups). If the interaction con-
tinues the system will be adapted to the extern hos-
pital needs. This is specially useful, as an example,
when patients are derived from the primary attention
to hospitals with medical specialties, or when a hospi-
tal frequently send patients to a special unit in another
hospital (i.e. emergency or maternity centers).
Regarding implementation issues, the system only
requires to store the pertinence of the acceded data
groups in a table similar to the dynamic pertinence
one, adding the identification of the extern hospital.
4.2 Final Remarks
In this section we indicate the requirements to imple-
ment this proposal, as well as how the problems men-
tioned in the introduction are tackled.
4.2.1 System Requirements
First of all it must be noted that in most of the coun-
tries laws obligate to store the information about the
medical staff accesses to the information in the EHR.
In other words, all the hospitals must have a database
similar to the above mentioned RADB. To implement
this proposal in addition to this RADB are only nec-
essary:
• A context-based user interface.
• Support for an archetype based language or for
any other standard of communication like HL7.
• A table to store the correspondencesbetween con-
texts of different institutions.
• A table to store the extern pertinence.
ContextualizedAccesstoElectronicHealthRecords-ApplicationtoHospitalInteroperability
277
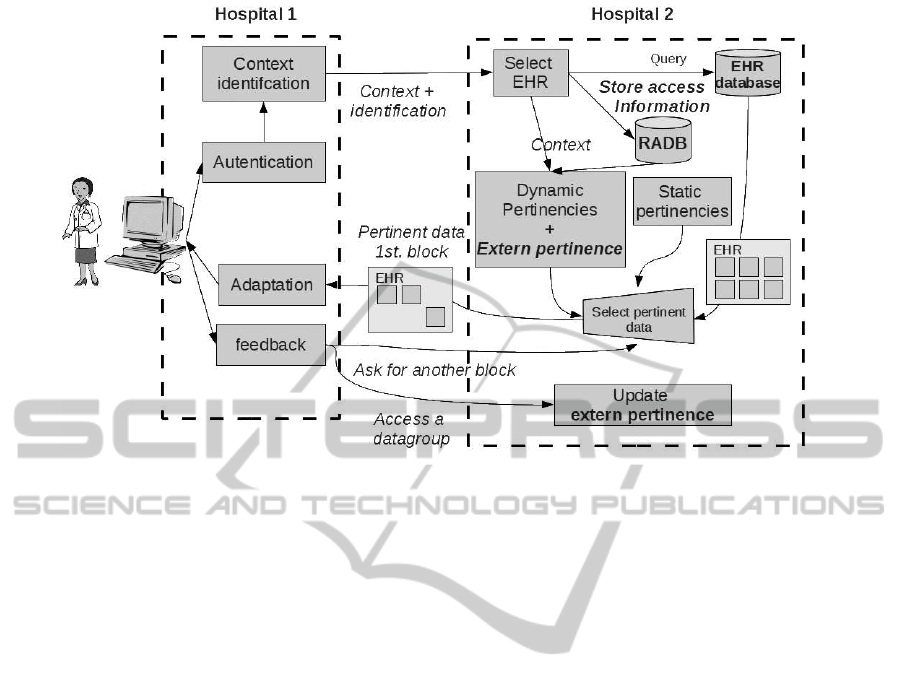
Figure 6: Scheme for an extern access with Extern pertinence and access record.
4.2.2 EHR Defragmentation
The fragmentation of the EHR for a given patient
is also solved in the following way: When an ex-
tern hospital H1 attends a patient and access his/her
EHR, this access is stored in the RADB of the hospital
queried H2 as mentioned above. When that patient re-
turns to his/her usual hospital H2, all the contexts re-
lated to the context from which the extern access was
performed will reflect the extern access. If the med-
ical doctor consider that extern act as relevant, they
can make an extern consultation to H1 to retrieve the
part of the EHR generated in that extern assistance
act. Otherwise, this information will lose relevance
with the time and stop being pertinent, but a record of
it will remain stored in the EHR.
4.2.3 Communication between Systems
The solution to transfer the information depends on
the systems that interact: if both systems support an
archetype language, then the information can be sent
using this language. In other cases, standard formats
for medical documents can be used like DICOM for
images and PDF or XML for textual information.
4.2.4 Security and Authentication
The problems of security and authentication are eas-
ily to solve in this proposal since each hospital and in-
stitution is responsible of authenticating the members
its staff when they access the local system. The au-
thentication problem then is transferred to the authen-
tication between institutions, in such a way that when
a hospital receives a query from another one they are
sure of the identity of each other. This problem in fact
is also solved since most of the institutions use digital
certifies, and if not, any of the available mechanisms
to this purpose can be used.
5 CONCLUSIONS
In this paper we have presented an approach to pro-
vide the HIS with interoperability capabilities by the
use of a context-based interface. In addition our pro-
posal improves the accessibility of the information ,
since the medical staff can reach the desired informa-
tion easier and faster (in less steps), also the mobiliza-
tion of the knowledge since specific contexts for the
mobile devices can be created. Even more the system
is able to adapt to the specific requirements of infor-
mation of each staff member or patient in a hospital,
as well as to the requirements performed from any
other extern institution. Moreover it also adapts to the
changes in the patterns of access over time and it all
is done in an automatic an efficient way.
The problem of the EHR fragmentation is also
solved trough a mechanism to register and localize all
the disperse parts of it, regardless where it is or the
format it is stored in, and avoiding the saturation of
the medical doctors with too much information.
There are no problems of security, since the identi-
fication between institutions is done as usual, and ev-
ery hospital is responsible of the staff identification.
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
278

Finally, this proposal is easy and not costly to im-
plement, and doesn’t require to modify the structure
of the EHR of the hospitals to communicate nor per-
form the translations between these structures. In ad-
dition it is not dependent on the underlying technol-
ogy, and it complies with the ISO 13606 standard but
is also valid for any other protocol of communication
solving the problem of the lack of agreement in the
standard to use.
ACKNOWLEDGEMENTS
The research reported in this paper was partially
supported by the Andalusian Government (Junta
de Andaluc´ıa) under project P07-TIC03175 ”Repre-
sentaci´on y Manipulaci´on de Objetos Imperfectos en
Problemas de Integraci´on de Datos: Una Aplicaci´on
a los Almacenes de Objetos de Aprendizaje”, by the
Spanish Government (Science and Innovation De-
partment) under project TIN2009-08296, and also by
project UJA11/12/56. We would also like to thank
their collaboration to the medical personnel that is
participating in the development of the system.
REFERENCES
Arch-Int, N. and Arch-int, S. (2011). Semantic information
integration for electronic patient records using ontol-
ogy and web services model. In Information Science
and Applications (ICISA), 2011 International Confer-
ence on, pages 1 –7.
Campos, M., Correia, M., and Antunes, L. (2011). Lever-
aging identity management interoperability in ehealth.
In Security Technology (ICCST), 2011 IEEE Interna-
tional Carnahan Conference on, pages 1 –8.
de la Torre-Diez, I., Gonzalez, S., and Lopez-Coronado, M.
(2013). Ehr systems in the spanish public health na-
tional system: The lack of interoperability between
primary and specialty care. Journal of medical sys-
tems, 37(1):9914–9914.
DePalo, P. and Song, Y.-T. (2011). Implementing inter-
operability using an ihe profile for interfacility pa-
tient transport. In Computers, Networks, Systems and
Industrial Engineering (CNSI), 2011 First ACIS/JNU
International Conference on, pages 70 –75.
Halevy, A. (2011). Game-changing interoperability for
healthcare: Bringing semantically harmonized clin-
ical information into provider workflows from dis-
parate health information technologies. In Emerging
Technologies for a Smarter World (CEWIT), 2011 8th
International Conference Expo on, pages 1 –3.
Hu, Y., Jiang, L., Yu, M., and Ye, L. (2011). A peer-to-peer
solution for achieving interoperability among health-
care centers. In Digital Media and Digital Content
Management (DMDCM), 2011 Workshop on, pages
302 –307.
ISO-13606 (2008). Iso 13606: Electronic health record
communication.
Karahoca, A., Bayraktar, E., Tatoglu, E., and Karahoca,
D. (2010). Information system design for a hospital
emergency department: a usability analysis of soft-
ware prototypes. Journal of biomedical informatics,
43(2) , p. 224-32:–.
Liu, Y., Wang, J., Zhao, C., Lu, X., Duan, H., Yao, X., and
Xu, W. (2011). Enhancing interoperability of ecg ma-
chine to support ecg telediagnosis service. In Biomed-
ical Engineering and Informatics (BMEI), 2011 4th
International Conference on, volume 2, pages 1093
–1096.
Martinez-Costa, C., Menrguez-Tortosa, M., and Fernndez-
Breis, J. T. (2010). An approach for the semantic in-
teroperability of iso en 13606 and openehr archetypes.
Journal of biomedical informatics, 43(5):736–746.
Miguel Prados de Reyes, M. Carmen Pe˜na Y´a˜nez, M. A.
V. M. and Su´arez, M. B. P. (2006). Generation and use
of one ontology for intelligent information retrieval
from electronic record histories.
Prados-Suarez, B., Molina, C., Yanez, C., and de Reyes, M.
(2012). Contextualized access to electronical health
records in cardiology. Information Technology in
Biomedicine, IEEE Transactions on, 16(3):401 –412.
Prados-Su´arez, B., Molina, C., Ya˜nez, C. P., and de Reyes,
M. P. (2012). Improving electronic health records re-
trieval using contexts. Expert Systems with Applica-
tions, 39(10):8522 – 8536.
Prados-Su´arez, B., Revuelta, E. G., C. Pe˜na Y´a˜nez, G.
C. M., and Fern´andez, C. M. (2008). Ontology based
semantic representation of the reports and results in
a hospital information system. In Proccedings of the
ICEIS 2008, pages 300–306.
Stan, O., Sauciuc, D., and Miclea, L. (2011). Medical infor-
matics system for romanian healthcare system. In E-
Health and Bioengineering Conference (EHB), 2011,
pages 1 –4.
Sunil Kumar, C., Guru Rao, C., and Govardhan, A. (2010).
A framework for interoperable healthcare information
systems. In Computer Information Systems and In-
dustrial Management Applications (CISIM), 2010 In-
ternational Conference on, pages 604 –608.
Van Gorp, P. and Comuzzi, M. (2012). Myphrmachines:
Lifelong personal health records in the cloud. In
Computer-Based Medical Systems (CBMS), 2012 25th
International Symposium on, pages 1 –6.
Vergari, F., Salmon Cinotti, T., D’Elia, A., Roffia, L., Za-
magni, G., and Lamberti, C. (2011). An integrated
framework to achieve interoperability in person-
centric health management. International journal of
telemedicine and applications, 2011:549282–549282.
ContextualizedAccesstoElectronicHealthRecords-ApplicationtoHospitalInteroperability
279
