
Predicting Cases of Ambulatory Care Sensitive Conditions
W. Haque and D. C. Finke
Department of Computer Science, University of Northern British Columbia, Prince George, Canada
Keywords: Predictive Analytics, Ambulatory Care Sensitive Condition, Healthcare, Data Mining.
Abstract: Proper management of ambulatory care sensitive conditions does not only enhance patient care, but also
reduces healthcare costs by minimizing hospitalizations. In order to strategically allocate resources, it is
essential to rely on informed forecasting decisions. Among other factors, the healthcare data is deeply
affected by seasonality, granularity, missing information and the sheer volume. We have used the ten-year
history from a Discharge Abstract Database to build predictive models and perform multi-dimensional
analysis on key metrics such as age, gender, and demographics. The valuable insights suggest that
investments in some areas appear to be working and should continue whereas other areas suggest a need for
reallocation of resources. The results have been confirmed using two distinct time series models. The
forecasted data is integrated with existing data and presented to users through data visualization tools with
capabilities to drill down to reports of finer granularity. It is observed that though some diagnoses appear to
be on an upward trend in prevalence over the next few years, other ACSC-related diagnoses will continue to
occur with either the same or slightly less frequency.
1 INTRODUCTION
Ambulatory care sensitive conditions (ACSC) are
medical conditions such as hypertension, asthma,
diabetes, and COPD which are normally treatable in
an outpatient setting. Identification of
disproportionately high levels of ACSC cases in
specific regions, health service delivery areas
(HSDAs), or public demographics is key to reducing
health care costs and enhancing patient care; most
ACSC cases are preventable (Oster and Bindman,
2003) and do not require hospitalization (Brown et
al., 2001); (Schrieber and Zielinski, 1997). Many
variables affect the distribution of ACSC cases –
such as region, age, socioeconomic conditions and
availability of health services. These variables can
be difficult to identify because of the sheer quantity
of data and the raw format in which it is stored. Data
mining tools can be used to find these data patterns
and to forecast reliably. Examples include the
prediction of the number of cases into several years
in the future, the probability that a person fitting a
demographic set has an ACSC diagnosis, and more.
The external variables (such as new breakthroughs
in disease management or environmental factors
causing more significant disease symptoms) that
influence health care make predicting these metrics
challenging. The data mining algorithms based on
moving averages, linear regressions equations, and
seasonal patterns are designed to reduce the impact
of unknown and undetectable variables. Thus the
algorithms are capable of detecting trends in data
even when it contains a small percentage of outlying
data which could potentially skew the results.
Predictions that show a lack of disease treatment and
management performance (e.g. in a specific
community) will convince health care decision
makers to revisit areas that may have been neglected
but deserve attention.
2 RELATED WORK
It is the nature of ACSC that treatment differs from
normal inpatient care. Additional challenges are
often present such as the frequency of diagnoses
being made, which may be many over a short period
of time (Starfield et al., 1991). Examinations into
demographics and locales that experience higher
rates have been an interesting research in the health
care field. Observations include a higher rate of
ACSC occurrences in younger children and poorer
areas (Parker and Schoendorf, 2000). Research also
shows that non-Caucasian individuals tend to visit
72
Haque W. and Finke D..
Predicting Cases of Ambulatory Care Sensitive Conditions.
DOI: 10.5220/0004479800720079
In Proceedings of the 2nd International Conference on Data Technologies and Applications (DATA-2013), pages 72-79
ISBN: 978-989-8565-67-9
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

physicians for ACSC-related circumstances at a
lesser rate than Caucasian individuals. The
correlation between income and patient’s race
supports the notion that income is related to
accessibility and frequency of ACSC treatment in
potential patients (Lieu et al., 1993). Furthermore,
remote and aboriginal communities were observed
to have increased risk of complications with diabetes
(Booth et al., 2005). It is likely that other ACSC
diagnoses follow a similar pattern. The difference
between areas with a higher overall income and the
poorer areas may show a lack of health care access
for some people (Roos et al., 2005).
Time is a significant component in variations in
ACSC case data. In Ontario, between the years
1994-1999, acute complications of diabetes
decreased by roughly 6% per year (Booth et al.,
2005). In U.S., research into childhood asthma
showed an overall increase in visitations for the
ACSC disease between the years 1980-1998.
However, the data does show a recent stabilization
of the proportion of youth admitted for asthma
(Akinbami and Schoendorf, 2002).
Researching the causes of and situations for
ACSC cases is critical in improving a key health
care performance metric: Primary Health Care
(PHC). It has been identified by professionals that
improving PHC significantly improves the treatment
of ACSC and prevention of ACSC hospitalizations.
By looking for symptoms related to the onset of
ACSC, this pre-emptive care is most effective
(Caminal et al., 2004).
3 METHODOLOGY
The Discharge Abstract Database (DAD), consisting
of approximately one million rows and over seven
hundred sparsely populated columns, formed the
basis of this study. Upon pivoting, this yielded over
twenty-six million rows that were to be analyzed.
Earlier, we had used Business Intelligence (BI) tools
and techniques to efficiently analyze this database
and presented statistically significant trends and
patterns (Haque and Edwards, 2012). We have now
extended this study using advanced analytics for
developing predictive models. There are several
methods which can be deemed viable for predictive
analytics. Our data mining solution focuses
primarily on time-based mining and requires input
sets with equally distributed time slices. Mining
models for the identified metrics have been created
and trained individually for each dimension (or set
of dimensions) in order to attain maximum level of
accuracy. Microsoft SQL Server Analysis Services
(SSAS) tools are used to achieve our solution
(Microsoft Corp, 2013). Furthermore, separate
models are developed using the software R and its
various multivariate linear regression algorithms
(Gentleman et al., 2012).
Other available algorithms include Microsoft
Clustering, Decision Trees, Neural Networks, and
Linear Regression. The Clustering algorithm was
immediately invalidated because it did not support a
continuous type attribute (ACSC data is continuous
as opposed to discrete). While the other algorithms
could be used for our predictions, they would require
a mapping between the id fields in the date
dimension and integer values. Linear Regression
was the most applicable, because the input series for
our data was primarily based on increase and
decrease in number of cases. However, the
Microsoft Time Series algorithm is a special
implementation of a blend of the Linear Regression
algorithm and ARIMA. It is designed to operate with
date key values and simplifies the process of
forecasting over time ranges. As a result, time series
was our choice of data mining technique. This
technique allows use of a combination of the
proprietary Microsoft ARTXP algorithm and
popular ARIMA algorithm (MSDN, 2012).
As Microsoft Time Series does not supply
control over every variable used by ARTXP or
ARIMA algorithms, a comparison of our SSAS
results with those produced by R is used to enhance
our confidence and support the results of our data
mining solution.
3.1 Data Challenges
The data integrity issues encountered ranged from
formatting that prevents straightforward integration
into an existing cube structure to absence of data that
could have been a useful metric for forecasting. An
example of such data is the ethnicity of an individual
identified with ACSC.
3.1.1 Time Series Stationarity
A requirement of the ARIMA time series data
mining algorithm is stationarity of the input time
slices. “Stationarity has three components. First, the
series has a constant mean, which implies that there
is no tendency for the mean of the series to increase
or decrease over time. Second, the variance of the
series is assumed constant over time. Finally, any
autocorrelation pattern is assumed constant
throughout the series.” (Barao, 2008) In general, the
volatility of the health care data causes a lack of
PredictingCasesofAmbulatoryCareSensitiveConditions
73

stationarity. The process of differencing is used to
reduce or eliminate non-stationarity from the input
series. In both manual and automatic differencing
(done by time series implementation examining
autoregressive values) (MSDN, 2012), the
application of the differencing process cannot
resolve the externally influenced changes in input
series mean. Thus, increasing the levels of
differencing in ACSC data cannot redeem ARIMA
as useful for all model applications. As a result, we
are limited to the use of ARTXP time series
algorithm for several predictions.
Due to inherent seasonality in our ACSC data,
creating mining models at a finer granularity
becomes a greater challenge because finding a fitting
historic model curve becomes more difficult.
Trimming the input set of irregular data can help to
improve the generation of historic model.
3.1.2 Input Data Limitations
The input set for time series models should have a
large number of slices in order to create a strong
historic model and reduce the overall impact of
irregularities. In general, using between 32-40 time
slices is the minimum for an acceptable ARTXP
model. The existing set of ACSC data gives us 36
fiscal quarter slices. It is also critical that data is
supplied continuously through all periods – a lack of
data for an input slice means we must either
determine it as zero, or take the mean of previous
time slices, adding error. A similar problem exists
when the series is fully populated but the metric
values lack significant variation. This occurs more
frequently as data granularity becomes finer when
incorporating additional attributes.
Ethnicity has been observed to be a strong
influencer of the frequency and severity of ACSC
occurrences. The DAD, however, does not contain
any aggregations on ethnic demographics. As a
result, we cannot explore or forecast change in
ACSC in varying ethnic groups. We instead choose
to explore how changing gender and age
demographics will affect ACSC prevalence.
3.1.3 Conformed Date Dimension
Time series data mining predictions output their data
as a set of SQL rows split by attributes and future
time slices. An inconsistency exists between the way
SQL creates a date dimension and the way the time
series implementation creates future time slices in
fiscal quarters. The forecasting tool produces data
whose date fields progress in ¼ of a calendar year.
However, the Northern Health (NH) conformed date
dimension uses fiscal quarters aligning along
specific months. As a result, a mapping query is
needed to link the predicted data to the NH
conformed date dimension. The mapping query
prevents the quarter-year output from the mining
prediction from becoming offset from the proper
fiscal quarters.
3.1.4 Storing Forecasted Data
Output from mining model predictions in SSAS is
exported to a SQL table. We have two options when
storing: either update the existing prediction results
table or create a new one for the prediction. When a
large number of unique predictions are done, the
number of tables would become large with the latter
choice. This not only adds complexity to the cube
but additional tables require that SSAS data source
view must be updated for every new table; this
makes calculations more complex, involving
multiple separate relations’ fields as opposed to a
single standard field. Updating existing prediction
tables require distinguishing between sets of rows
using a key column. This solution results in longer
lookup times and increased space complexity, but
this is less of an issue in analytical work than it
would be in a transactional scenario. The cube is
only periodically processed; the lookup on the data
in the database only occurs when the DAD is
updated. As a result, we used a single table whose
rows are differentiated by the key.
4 DATA MINING/PREDICTIONS
The use of data mining functionality in SQL Server
requires creation of a mining structure (with models)
and preparation of two sets of data: a training set,
and a template set. The latter is required for
forecasting in the instance where partial future data
needs to be added to an existing model (such as in
the case of ACSC predictions based on future census
population) and consists of relations with arity and
domain equivalent to the model’s training data.
Training sets are needed for each unique collection
of dimensions used to slice the data.
The SSAS data mining tools support two modes
of creation: the model can be created on top of the
cube, or it can be created based on the corresponding
SQL database. The latter option requires special
formatting of the forecast output data. Though our
ultimate intent is to update the cube, having access
to the SQL database content gives us additional
control over the mining results. With results in SQL
DATA2013-2ndInternationalConferenceonDataManagementTechnologiesandApplications
74

rows, we can easily tie in new data with existing
data as well as split the data by arbitrary conditions.
Therefore, the SQL mode was a preferred choice for
use in our solution.
4.1 Preparation of Training Data
Our training data set consists of numbers of cases
and interventions over a given period of time.
Existing raw data resides in a SQL database from
where we gather appropriate dimensions for the
measures that are being forecast. Preparation of
training data can include any number of dimensions
and conditions. Each row with an ACSC flag in the
diagnosis table represents a unique case. By
aggregating on unique attribute groups, we can
obtain the number of cases belonging to those
groups. As we are working at the SQL level, we
must replicate the calculation for the measure in the
training query. Because each row in the diagnosis
fact table is considered a case, we can select a sum
of the number of rows where one or more of their
dimension parameters match. For example, we could
choose a count of rows where genders match. Thus,
the output set would consist of two columns; one
column specifies the gender, and the other displays
the number of rows/cases corresponding to that
gender. The output is stored in a temporary staging
table.
4.2 Training the Model
SSAS mining structures are used to process data
from the staging tables; the chosen algorithm learns
the patterns in the input data and enables forecasting
based on those patterns. Initially, a univariate
analysis was done. We considered the variations in
either number of ACSC cases or total cases when
divided by various attributes relevant to prescribed
time-based metrics. Eventually, population was
identified as an important predictor for a
multivariate analysis.
In SSAS, the data source view is prepared to
accept newly forecast data for cube processing
without additional configuration. The control
parameters used by the algorithm to learn the trends
in its input series are given in Table 1. The mining
model processes the data based on these values and
exports it as a series of SQL rows. By completing
the query process the raw output data can be
combined with other forecast data as well as DAD
data.
SSAS does not allow control over the algorithm
learning process past these parameters. Instead,
heuristic algorithms assist in determining the values
that compose the prediction algorithm’s equation.
This equation is based on the linear change in input
series as well as some constant variance values. In
case of ARIMA, the additional process of
differencing is used to get the best possible forecast
equation; SSAS deems the equation fitting when
stationarity is maximized. Using the mining model
viewer in SSAS, we examine the short-term results
of the forecast as well as how accurately the
historical model collection matches up with existing
data. Prediction results are exported to the SQL
database once the model is deemed acceptably
accurate.
Table 1: Model parameters.
Parameter
Property
Use
Mthly/Qtrly
value
FORECAST_
METHOD
Controls the algorithm used
by SSAS in forecasting
ARIMA or
ARTXP
HISTORIC_MODEL_
COUNT
Multiplier for historic
models
1
HISTORIC_
MODEL_GAP
Number of time slices each
historic model spans.
12 / 8
MINIMUM_SERIES_
VALUE
Series values cannot be
predicted below this
threshold (case counts
cannot be negative)
0
MISSING_ VALUE_
SUBSTITUION
Value used when points in
the middle of the series are
absent.
0:
values (<10)
MEAN:
values (>10)
PERIODICITY_HINT Seasonality of data 12 / 4
4.3 Integrating Forecasted Data
In order to combine raw forecast data with existing
data in the cube, it needs to be assigned the
appropriate foreign keys for various dimensions.
Output strings are parsed for attribute members
found in dimension tables. A lookup is executed for
finding the key value that corresponds with the
attribute members and finally the data is inserted
into a table for completed predictions. An additional
key is used to identify the unique prediction fields;
for example, a different identifier key is used for a
prediction on the gender attribute than for prediction
on both gender and age group. This identifier
enables us to choose the right data from the cube for
visual reports.
Further examination of the accuracy of the
historical models is conducted by averaging
percentage difference for each time slice. In general,
mining models that generate historical prediction
values of less than 30% difference from the actual
values are accepted for use in deliverable reports.
PredictingCasesofAmbulatoryCareSensitiveConditions
75

ACSC cases
Predictions with few attributes tend to have
differences of less than 5-6%. Data is finally
formatted to be processed by the SSAS cube. New
entries in tables linked to forecasts and forecast-
related dimensions become a part of the cube. Upon
completion, the case count metrics can be split by
the unique prediction identifiers described above.
4.4 Data Visualization
Charts and tables enable users to easily observe
trends in the ACSC metrics; many charts are broken
down by fiscal quarters or fiscal years and show the
change in ACSC over time. Aggregations take place
at levels such as on diagnosis or locale. Data is
aggregated on diagnosis, institution, locale cluster,
HSDA/LHA, and discharge disposition.
4.4.1 Dashboard
The dashboard presents a high-level overview of the
ACSC data. Visualization of data at this level is not
filtered. Common attributes for slicing charts and
tables include diagnosis, age group, and gender. The
users can select up to 5 years into the future. A user
may choose to exclude historical data, forecasted
data, or any combination. Forecast information in
the chosen future period is clearly identified, either
by a description or by an alternate colour. Tooltips
offer additional details on series seen in charts.
Other reports include metrics broken down by
ACSC diagnoses, Discharge Disposition, and ACSC
prevalence by geographic clusters/location.
4.4.2 Other Reports
The drilldown reports provide information about the
core ACSC metrics at a finer granularity. New
information on various charts is displayed in the
same manner as the dashboard, wherever predictions
for the attributes present in those charts produced
results with acceptable accuracy. Users can choose
to filter data by members of the corresponding
attribute, as well as the specified time period. As
explained earlier, forecasting results become
increasingly sparse as more attributes are introduced.
For the sake of space, the dashboard or other
drilldown reports are not included in this paper.
5 ANALYSIS OF RESULTS
In this section, we present some observations from
each of the models developed in SSAS and R,
closeness of results between the two, and significant
trends found from the data forecast by each
corresponding mining model. We have selected the
most representative results from our study.
5.1 Quarterly vs. Monthly Aggregation
The first noticeable result is the quality of forecasts
when using monthly vs. quarterly aggregation of
data. Both SSAS and R models result in higher
quality predictions when using quarterly
aggregation. This is observed by examining R’s
AIC, AICc, and BIC values which determine the
ideal fit from a pool of candidate models. AIC
represents the amount of information suspected to
have been lost by the model. BIC values operate in
the same manner as AIC, but incur a more
significant penalty when additional attributes are
included in the model. This helps to prevent
overfitting to the training data. We use these values
as a confidence measure for R’s models.
The label associated with R models comes in the
form ARIMA(0,0,0)(0,0,1)[12] (Figure 1). It is a
representation of the equation used by ARIMA for
generating the model. The two tuples in parentheses
imply that the model combines two equations. The
first index in a tuple is the number of regressive
terms, the second is the number of deviations in the
series that do not follow a seasonal pattern, and the
last is the lagged forecast error in the equation.
Finally, the label “[12]” implies the model’s
seasonality, which in this case is monthly.
Figure 1: Monthly ACSC count forecasts produced by R.
In Figure 1, values prior to 2010 are data from
DAD. The data beyond 2010 shows predicted metric
values by the ARIMA algorithm and the bands
around this line represent the 85% and 90%
confidence levels. The values of AIC, AICc, and
BIC are 504.96, 505.19, and 513.01, respectively. A
higher value of these metrics implies a lower relative
quality of forecast. Relatively, these values are high
DATA2013-2ndInternationalConferenceonDataManagementTechnologiesandApplications
76
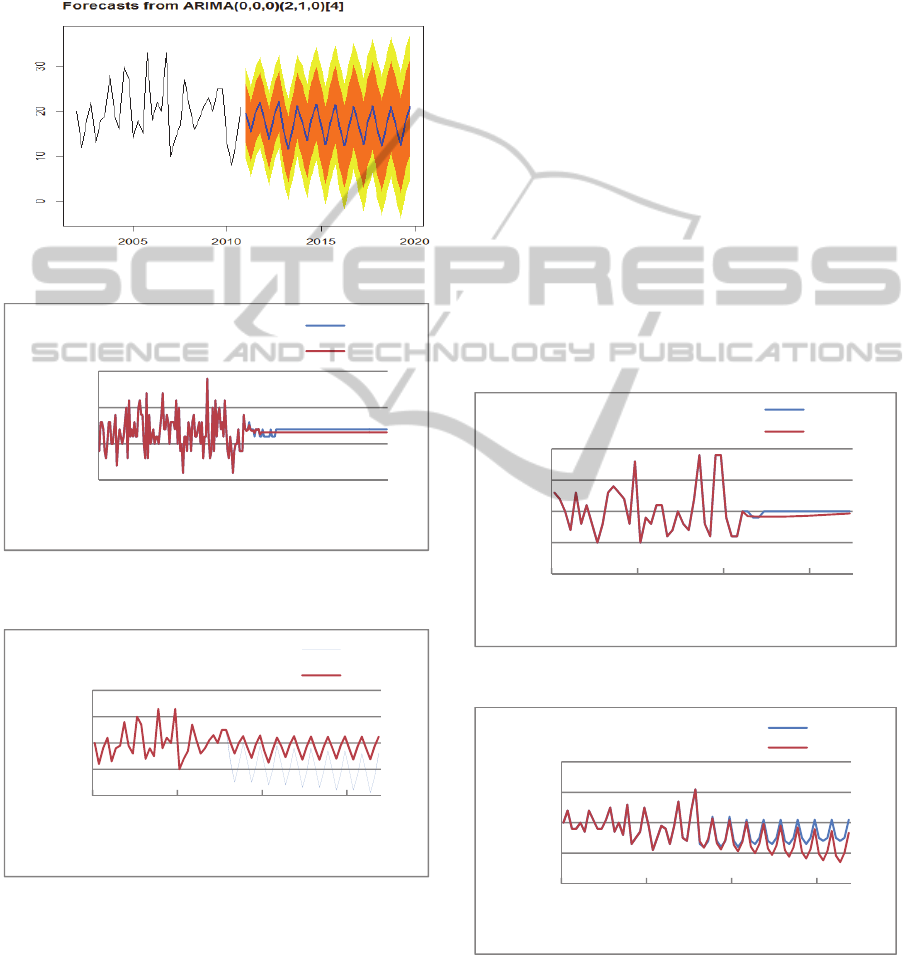
and therefore the level of confidence in this model is
low. An additional observation in this chart is the
absence of any variation in the predicted period.
This commonly occurs when the input series does
not have strong seasonality – as a result, the
algorithm resorts to detecting a mean of the series.
Figure 2: Quarterly ACSC cases forecast produced by R.
Figure 3: Monthly ACSC cases forecast by SSAS and R
models.
Figure 4: ACSC cases forecast by SSAS and R models.
Figure 2 shows the same metrics using quarterly
data due to much more pronounced seasonality. This
results in improved AIC, AICc, and BIC values
(roughly 200 each) and a forecast that retain
seasonal trends; the peak in forecast values is at the
4
th
quarter of each fiscal year. The corresponding
results from our SSAS models are shown in Figure 3
and Figure 4; similar trends were observed.
5.2 Reducing the Number of Attributes
An experiment separating the genders produced
significant variation between the predicted values.
For example, it was observed that the male category
in 30-39 age group showed a poor forecast of
seasonality from both the R and SSAS models
(Figure 5). Though both models were unable to
detect and represent the quarterly seasonal pattern,
the values of AIC, AICc, BIC in the R model were
204.96, 205.32, and 208.13, respectively. These
values, relative to our other successful predictions,
show that the model has a good degree of accuracy.
For this age group, the forecast results were
significantly improved when the male and female
input sets were combined and forecasted on (Figure
6). Both SSAS and R models created forecasts with
strong seasonality and both produced nearly
identical output. AIC, AICc, and BIC values of
approximately 195 show a close fit to DAD data in
the R model.
Figure 5: ACSC cases forecast for 30-39 yr males.
Figure 6: ACSC cases forecast for all 30-39 yr old.
Figure 7 shows the breakdown of ACSC actual
and predicted data (4 year into the future) with only
the gender attribute. This scenario resulted with a
0
5
10
15
2001 2006 2011 2016
ACSCCases
Timebymonth
11‐19yrs
SSAS
R
0
10
20
30
40
2002/03 2007/08 2012/13 2017/18
ACSCCases
FiscalQuarters
11‐19yrs
SSAS
R
0
5
10
15
20
2002/03 2006/07 2010/11 2014/15
ACSCCases
FiscalQuarters
30‐39yrs‐ M
SSAS
R
0
10
20
30
40
2002/03 2007/08 2012/13 2017/18
ACSCCases
FiscalQuarters
30‐39yrs
SSAS
R
ACSC cases
PredictingCasesofAmbulatoryCareSensitiveConditions
77

very acceptable confidence level of 89.5%. This also
demonstrates that predicting on the aggregated case
count produces a more accurate forecast.
Figure 7: Quarterly ACSC cases forecast by gender.
5.3 Some observed Trends
Accurate forecasting of ACSC metrics allows
management to make informed decisions on the
choice of future healthcare strategies instead of
making simple extrapolations from past data.
Sample Observation 1. As an example, Figure 8
identify the 70-75 year old as an age group in which
overall ACSC frequency is on the decline.
Following a spike at around 2007, our models
project a consistent decrease in ACSC occurrence.
Because the forecasting models are heavily
influenced by more recent events, the actual
decrease may not end up being as sharp as the
forecast. However, this does promote the idea that
existing activities designed for improving the ACSC
care of seniors have helped and will continue to help
that group.
Sample Observation 2. In recent years, the number
of ACSC cases in the Region 1 (Figure 9) has stayed
higher than the period around year 2004. Data
predicted by our models suggests that while the
ACSC numbers may stabilize at their current levels
for a couple years, the yearly average trend should
begin to return to previous levels after 2-3 years.
However, though the yearly cases on average will
begin to decline, 4
th
quarter spikes in ACSC will
remain. Region 2 occurrences (Figure 10) will
continue to remain reasonably high after identifying
a recent increase in their prevalence. Earlier time
slices have influenced the model such that the
expected threshold will not be as extreme as the
2008 peak.
Sample Observation 3. The overall number of ACSC
cases in all groups and diagnoses (Figure 11)
appears to remain constant over the forecast period.
In the chart, a diagnosis category with a historical
value approximately twice the forecast value is one
whose ACSC count per year has not changed (the
historical period is twice the forecast period). Within
these counts, COPD and Diabetes appear to be on a
slight increase in prevalence over the next 5 years
and other ACSC-related diagnoses will continue to
occur with either the same or slightly less frequency.
Figure 8: ACSC cases forecast for 70-75 yr females.
Figure 9: Historical and Forecasted Quarterly ACSC cases
in Region 1.
Figure 10: Yearly ACSC prevalence as a percentage of
population in Region 2.
Figure 11: ACSC cases in each diagnosis (2002-2010,
forecast to 2015).
0
100
200
300
400
2002/03 2007/08 2012/13
ACSCCases
FiscalQuarters
Allcases
M
F
0
10
20
30
40
50
2002/03 2006/07 2010/11 2014/15
70‐75yrs‐ F
SSAS
R
ACSCCases
FiscalQuarters
DATA2013-2ndInternationalConferenceonDataManagementTechnologiesandApplications
78

6 CONCLUSIONS
Data mining tools have been applied to ACSC data.
The resulting predictions have identified both, areas
and groups that need attention and those that are
headed in a positive direction. Because of the
inconsistent nature of health-related data, these
trends are more reliable when data is aggregated.
Despite this limitation, improvements to the health
care system can be targeted towards high-impact
locations and critical demographic groups identified
by our predictive models. COPD and Diabetes
diagnosis groupings appear to be on the rise and
require additional health care focus. Conversely,
population such as the 70-75 age group may be
receiving adequate treatment thus decreasing the
morbidity of these cases. Visualizations methods
provide a clear and easy to understand interface for
correctly distinguishing factual existing data and
predicted/forecasted data. The reporting tools offer
drill-down capabilities for further insight into any
desired set of existing and forecasted information
over specified time ranges. The models developed
offer a strong confidence level where stable
forecasting of ACSC-related health data is possible.
The SSAS environment was confirmed as an
effective means of creating forecasting models for
the ACSC data by observing similar results with R.
As a result, SSAS was deemed a beneficial tool for
creating a data mining solution for ACSC as it
simplified the task of designing mining structures
and models without the need for statistics expertise.
The reporting is also more intuitive and interactive.
The tight integration with the existing analytics cube
further centralized the task of data mining and
incorporation of new data into the data warehouse.
ACKNOWLEDGEMENTS
This research was funded by Northern Health, BC
under the Innovation & Development Commons
Program. The authors extend their sincere
appreciation for the support and guidance provided
by Michel Aka and Dr. Bill Clifford of Northern
Health in access/interpretation of data, validation of
results and completion of this research.
REFERENCES
Akinbami, L. J. & Schoendorf, K. C., 2002. Trends in
Childhood Asthma: Prevalence, Health Care
Utilization, and Mortality. Pediatrics, 1 August,
110(2), pp. 315-322.
Barao, S. M. M., 2008. Linear and Non-Linear Time
Series Analysis: Forecasting Financial Markets, s.l.:
Instituto Superior de Ciencias do Trabalho e da
Empresa.
Booth, G. L., Hux, J. E., Fang, J. & Chan, B. T., 2005.
Time Trends and Geographic Disparities in Acute
Complications of Diabetes in Ontario, Canada.
Diabetes Care, May, 28(5), pp. 1045-1050.
Brown, A. et al., 2001. Hospitalization for Ambulatory
Care-Sensitive Conditions: A Method for Comparative
Access and Quality Studies Using Routinely Collected
Statistics. Canadian Journal of Public Health, April,
92(2), pp. 155-159.
Caminal, J. et al., 2004. The role of primary care in
preventing ambulatory care sensitive conditions.
Public Health, 14(3), pp. 246-251.
Gentleman, R., Ihaka, R. & et. al., 2012. The R Project for
Statistical Computing. [Online]
Available at: http://www.r-project.org/
[Accessed 12 November 2012].
Haque, W. & Edwards, J., 2012. Ambulatory Care
Sensitive Conditions: A Business Intelligence
Perspective. York, Canada, s.n., pp. 31-39.
Lieu, T. A., Newacheck, P. W. & McManus, M. A., 1993.
Race, ethnicity, and access to ambulatory care among
US adolescents. American Journal of Public Health,
July, 83(7), pp. 960-965.
Microsoft Corp, 2013. Business Intelligence. [Online]
Available at: http://www.microsoft.com/en-us/bi/
MSDN, 2012. Microsoft Time Series Algorithm Technical
Reference. [Online]
Available at: http://msdn.microsoft.com/en-
us/library/bb677216.aspx
[Accessed 7 September 2012].
Oster, A. & Bindman, A., 2003. Emergency Department
Visits for Ambulatory Care Sensitive Conditions:
Insights into Preventable Hospitalizations. Medical
Care, 41(2), pp. 198-207.
Parker, J. D. & Schoendorf, K. C., 2000. Variation in
Hospital Discharges for Ambulatory Care-Sensitive
Conditions Among Children. Pediatrics, 1 October,
106(3), pp. 942-948.
Roos, L., Walld, R., Uhanova, J. & Bond, R., 2005.
Physician Visits, Hospitalizations, and Socioeconomic
Status: Ambulatory Care Sensitive Conditions in a
Canadian Setting. HSR: Health Services Research,
August, 40(4), pp. 1167-1185.
Schrieber, S. & Zielinski, T., 1997. The Meaning of
Ambulatory Care Sensitive Admissions: Urban and
Rural Perspectives. The Journal of Rural Health,
13(4), pp. 276-284.
Starfield, B., Weiner, J., Mumford, L. & Steinwachs, D.,
1991. Ambulatory care groups: a categorization of
diagnoses for research and management. Health
Services Research, 26(1), pp. 53-74.
PredictingCasesofAmbulatoryCareSensitiveConditions
79
