
SeGTE: A Serious Game to Train and Evaluate Basic Life Support
Claudia Ribeiro
1
, Joana Tiago
1
, Micaela Monteiro
2
and Jo
˜
ao Pereira
1
1
INESC-ID, Lisbon, Portugal
Instituto Superior T
´
ecnico, Universidade T
´
ecnica de Lisboa, Lisbon, Portugal
2
Servic¸o de Urg
ˆ
encia Geral Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal
Keywords:
Basic Life Support, Cardiopulmonary Resuscitation, Serious Games, Finite State Machines.
Abstract:
Basic life support (BLS) is the level of medical care which is used for victims of life-threatening illnesses or
injuries until they can be given full medical care at a hospital. It can be provided by trained medical personnel,
including emergency medical technicians, paramedics, and by laypersons who have received BLS training.
BLS is generally used in the pre-hospital setting, and can be provided without medical equipment. The ability
to respond to an emergency situation can be the difference between life and death. Acknowledging this fact has
made decision-makers, governments and Non Government Organizations (NGO) to make a priority to spread
this knowledge and skills to the general population. Currently, BLS is taught in a standard course provided by
the Red Course or certified entities, where the pedagogical content given to the students is a mix of theoretical
and practical training where life-size mannequin are used. In this paper we argue that serious games could
help spread this knowledge through the general population and it could also be used to refresh the knowledge
of people that have been certified in BLS in the past. In order to test this hypothesis we have developed the
SeGTE game and performed an evaluation of its effectiveness on conveying such pedagogical content.
1 INTRODUCTION
In this new millennium, the prevalence of road acci-
dents is so frequent and fatal it is an issue uppermost
in the minds of individuals, decision-makers, govern-
ments and Non Government Organisations (NGOs)
worldwide (Fiander, 2009).
The Statistics of Road Traffic Accidents in Eu-
rope and North America contains the basic statistics
provided by the Governments States members of the
United Nations Economic Commission for Europe
(UNECE). In this report is stated that for the ECE re-
gion in the decade 1999-2008 there were on average
150 000 persons killed and about 5.5 million persons
injured annually in more that 3.8 million road acci-
dents (UNECE, 2011). In the attempt of improving
both the consequences and well and the causes for this
statistics the International Federation of Red Cross
(IFRC) and Red Crescent Societies have issue sev-
eral reports where recommendations are proposed on
how to deal with this critical situation. Namely, one
of the central recommendations is to develop greater
first aid knowledge amongst the general population
be they drivers, car-users or pedestrians involved in,
or bystanders to, road accidents (IFRC, 2009; IFRC,
2010).
Although first aid is not a replacement for a emer-
gency services’ intervention, it is a vital initial step in
intervention that provides an effective and rapid con-
tribution. This both reduces the severity of injuries
and improves the chances of survival. In this manner,
the IFRC believes that everyone has the potential to
save lives. First aid is not just about techniques. It is
an act of humanity and therefore is a key responsibil-
ity of global citizenship (IFRC, 2009; IFRC, 2010).
The IFRC points out that the solution is not just
about making training compulsory. There is also a
need to improve the existing training practices and
quality. This is why people are called to attend first
aid refresher classes. All skills must be practised
and upgraded. Refresher classes will bring the per-
formance of most interveners to a higher level than
that recorded after initial training (IFRC, 2009; IFRC,
2010). Continuing first aid education is essential to
maintain providers’ knowledge and skills particularly
when they do not use their skills frequently.
An area where training can be improved is by in-
creasing the level of a course’s realism. It is one thing
to be in a training session but quite another to ap-
ply that classroom learning in a real situation. First
aid is not just about providing life-saving skills to a
438
Ribeiro C., Tiago J., Monteiro M. and Pereira J..
SeGTE: A Serious Game to Train and Evaluate Basic Life Support.
DOI: 10.5220/0004661504380444
In Proceedings of the 9th International Conference on Computer Graphics Theory and Applications (GRAPP-2014), pages 438-444
ISBN: 978-989-758-002-4
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

manikin; the real situation means dealing with fac-
tors that can prevent the provision of efficient first aid,
such as coping with the terrifying presence of blood or
a person’s pale and sweaty appearance when having a
cardiac arrest. The person providing first aid can also
be influenced by a crowd gathering around an acci-
dent. All these are important reasons for preparing all
first aid providers for the stress that they will face. Im-
proving this aspect of training will avoid what should
never be seen: people trained in first aid running away
from an accident scene simply because they are afraid
of blood or of the level of exposure.
In this paper we present SeGTE, a serious game
designed to train and evaluate Basic Life Support,
with the aim to teach the procedures described by the
European Resuscitation Council (ERC, 2012). This
game exploits video game technology to link in a
framework computer-based case with e-learning func-
tionalities. Some computer graphics techniques are
used to reproduce different situations where basic life
support is required and also the procedures that have
to be applied. SEGTE includes two game modes,
training mode and evaluation mode. In training mode,
the user can train the different medical procedures
provided in the ERC’s protocol (ERC, 2012). In the
evaluation mode the users can assess their knowledge.
The remaining sections of this paper are com-
posed as follows: Section II present the state of the
art of serious games for teaching and training of Basic
Life Support. Section III presents SeGTE architec-
ture and the main characteristics. Section IV presents
Evaluation, how the solution was validated with real
users. Section V presents the conclusions and future
work.
2 BACKGROUND
Basic life support (BLS) is a sequence of attitudes and
procedures aimed at recognizing a patient in cardiac
arrest, calling specialized help and meanwhile estab-
lishing blood circulation and oxygen supply in order
to keep the victim alive. In 2010 The European Resus-
citation Council (ERC, 2012) published new guide-
lines that precisely redefined the algorithm of proce-
dures for BLS. Every citizen should ideally be trained
in BLS as most cardiac arrests happen with layper-
sons as first helpers and brain death usually occurs
within 5 minutes of cardiac arrest if no help is pro-
vided. Traditionally BLS is taught and trained with
dummies in special courses of several hours.
Recently simulation software programmes have
been developed where the BLS algorithm can be
trained. ”Staying Alive” by iLumens
1
creates a 3D
environment where the user has to assist a collapsed
victim by following the BLS rules. ”AedChallange”
by Insight Instructional Media
2
is a video game for
refreshing already acquired skill. It presents several
clinical cases where the player can train BLS. The
player scores when he/she proceeds according to the
BLS algorithm. At the end there is a debriefing and
errors are explained.
3 SeGTE: A SERIOUS GAME TO
TRAIN AND EVALUATE BASIC
LIFE SUPPORT
SeGTE is a serious game, designed in collaboration
with healthcare professionals, to train and evaluate the
general public (lay persons) in basic life support. The
main objective of the game is to teach the procedures
described in the ERC’s protocol (ERC, 2012).
The sequence of procedures is determined by the
current condition of the patient. Specifically, if a pa-
tient is responsive it will not be necessary to execute
the procedure that corresponds to preform 2 rescue
breaths and 30 compressions. Actually, it would be
dangerous to perform such a procedure in a respon-
sive patient. In order to achieve this flexibility both in
specifying game cases as well as in game mechanics,
we used a finite state machine to guide the simulation
underlying the game logic. This finite state machine
was defined interactively with the help of healthcare
professionals. It was necessary to guaranty that every
path through the finite state machine was a valid one
and also that the feedback given during game play was
correct both in terms of content as well as the simu-
lation execution step. In the next subsections it will
be further elaborated how the finite state machine was
defined, as well as the game play, clinical cases defi-
nition and implementation details.
3.1 SeGTE Finite State Machine
The use of finite state machines in video games is pro-
moted by many developers due to their robust nature
as they are easy to test and modify. They are typically
used to model the behaviour of computer-controlled
game characters, also called no-player characters
(NPC), to make NPCs react to game events seem as
intelligent and natural as possible, (Hu et al., 2011;
Saini et al., 2011).
1
http://ilumens.fr/numerique/serious-games/
2
http://aedchallenge.com/
SeGTE:ASeriousGametoTrainandEvaluateBasicLifeSupport
439
A finite state machine is a system with a set of
states and a collection of transitions, which represent
some kind of actions for each state. It has a initial
state, and one or more final states. In practice, it’s a
description of how an object can change its state over
time in response to the environment and events that
occur. Each state represents a behaviour, resulting in
the behaviour changing as states change from one to
another, (Saini et al., 2011).
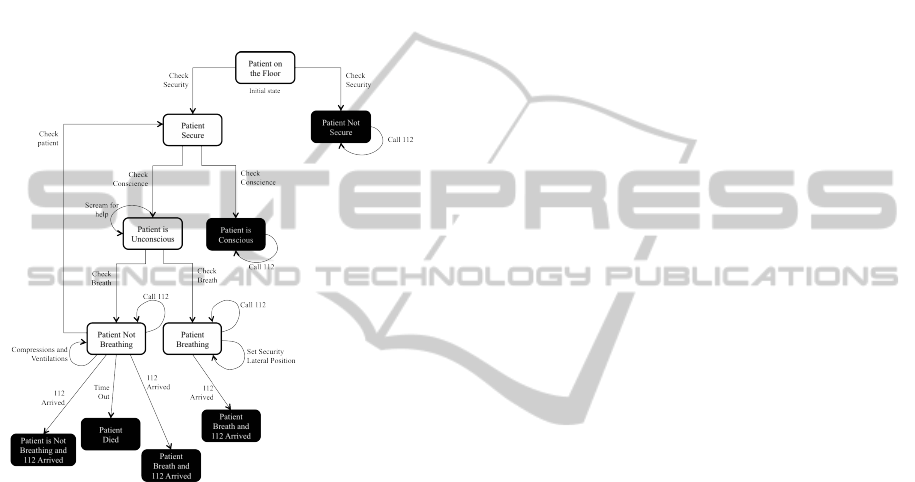
In Figure 1, is depicted the Finite State Machine
of our serious game.
Figure 1: The Finite State Machine representing the proce-
dures of ERC’s protocol.
To create this finite state machine, we transform
the basic life support algorithm, presented by the Eu-
ropean Resuscitation Council 2012 (ERC, 2012), to
a set of states and actions, and define how they are
connected. The process starts with the transformation
of each medical action in a element of the finite state
machine. For this purpose, it was necessary to under-
stand what is an action, a state or a transition.
Each state of the finite state machine corresponds
to the current state of the patient during a game
play. In each state the player can decide which action
she/he should take but only the valid transitions of the
finite state machine are considered correct. Therefore,
every action taken which is outside the set of actions
permitted or considered correct will have a negative
feedback. Depending on its level of severity, the game
can either end, resulting in the death of the patient or
a warning is issued to the player. More details about
the game play and different elements that make-up
the game SeGTE are described in the following sub-
sections.
3.2 SeGTE Game Play
The game play starts with a briefing screen where the
player is introduced to the pedagogical goals of the
game. Also, in this screen the player can access in-
formation concerning the basic life support algorithm
and how the user interface works. In this phase a facil-
itator that has background knowledge of the game and
the basic life support algorithm, provides extra infor-
mation and clarifies any necessary doubts that might
be posed by the player.
Once this phase is terminated, the player can
choose either to play in training mode or in evalua-
tion mode. In training mode, the player can train the
different game cases. If the player chooses the wrong
procedure a warning appears. This warning con-
tains information about what procedure should have
be done. After this, the player can correct her/his er-
ror and continue the game. Furthermore, some in-
formation is given on how to make certain actions
(e.g. compressions and ventilations). In evaluation
mode, the players can assess their knowledge, there-
fore no type of information or help is provided during
the game. If she/he makes a mistake, the patient’s life
is at risk and some decisions can lead to prematurely
ending the game resulting in the patient death.
Independent of the game mode, after each game
case the player is presented with the debriefing screen.
On this screen the player is given an explanation of
what were her/his mistakes and how they can be cor-
rected. This phase of the game play is critical for
knowledge retention. By reflecting on the game af-
ter playing it, debriefing helps the player make mean-
ingful connections between the game experience and
the ”real world” (Crookall, 1990; Crookall, 1992),
thereby likely enhancing transfer of knowledge and
skills. Debriefing can promote active learning by de-
constructing the experience, exploring alternatives re-
sponses, and linking observations and experiences in
the virtual world to those in the real world (Gaba
et al., 2001). It is still not clear how debriefing
can be most effectively incorporated in serious games
(Thompson et al., 2010). Therefore, during the evalu-
ation of different releases of the game informal inter-
views were made to users in order to better understand
if our choices were both aligned with the expectations
of the users and, as well as the pedagogical goals of
the game.
3.3 Clinical Cases
In SeGTE several game cases were set up in order to
allow the player to have the opportunity of exploring
the application of the algorithm in patients with differ-
GRAPP2014-InternationalConferenceonComputerGraphicsTheoryandApplications
440

ent health conditions. Therefore, each game case cor-
responds to what we have denominate a clinical case.
Basically, a clinical case is a description of several at-
tributes that make up the patient’s current condition
and the environment were he is currently in. Such at-
tributes are for example, if the patient is secure or if
the patient is breathing.
Currently the game cases are configured inside the
game application, but extending this solution to sup-
port adding new clinical cases is trivial and is one of
the top priorities of the next release of the SeGTE
game. Structuring this information in an XML file
would not just facilitate the process of adding new
game cases, it would also admit to translate the game
into different languages. Apart from this and most
important it would allow healthcare professionals to
add this information without the intervention of a pro-
grammer. This is very relevant, both because it would
ideally motivate the use of this game by healthcare
professionals but it would also make this game less
fragile to new updates of the basic life support algo-
rithm.
3.4 User Interface
The interface was create with the goal of making the
player’s interaction as simple and efficient as possible.
With this purpose we have use a navigation based on
point-and-click. This greatly facilitates the navigation
inside the virtual world for players that are not used
to play games or to navigate inside 3D environments.
For the reminder of the user interface, the standard
style of interaction such as buttons, boxes and win-
dows were used.
The environment is outside of a hospital. Most
of this cases deal with the basic life support, i.e. the
primary skills in cardiopulmonary resuscitation and
include basic mouth-to-mouth resuscitation and chest
compressions to circulate blood. No medical equip-
ment is required and there are no invasive procedures.
The player interface simulates the unexpected
emergency incident and allows the player to rescue
the victim.
The scene starts with the emergency situation,
when a victim falls in the street. The player plays
the role of the helper that tries to save the victim. Af-
ter finishing the clinical case the debriefing menu is
shown and the player can assess her/his performance.
Figure 2 shows the sequence of procedures for a
cardiopulmonary resuscitation situation from (a) ini-
tial state with the patient on the floor; (b) Check is
Secure; (c) Check conscience; (d) Check is breathing;
(e) Initiate Compressions and Ventilations. Helper
choose mouth-to-mouth or mask; (f) Helper starts
compressions and Ventilations.
Figure 2: Sequence of Procedures in SeGTE.
Some of the animations and actions lack realism
as avatar performance is limited. However, for this
first prototype the main objective is that the player
learns the order of each procedure.
In the future work, we can improve some of these
animations and procedures. The possibility of player
collaboration with other characters (e.g. a person for
help in compressions and ventilations)will also be in-
cluded.
3.5 Implementation Details
SeGTE architecture is divided into two main com-
ponents, the serious game component and the Finite
State Machine component. The serious game com-
ponent is generically responsible for managing the
game logic, graphic assets, interfaces and players in-
teractions. It’s based on Unity3D
3
game engine and
follows a script based architecture, that encapsulates
functionality as C# scripts.
In the serious game component there are four main
modules, the HUD manager, the Camera Manager,
the FiniteStateMachine Manager and the Game Man-
ager. The HUD manager is responsible for manag-
ing all the interfaces of the game, namely all the
menus, feedback information messages and briefing
screen menu. The Camera manager is responsible
for managing the navigation inside the game. This
is accomplished by methods and routines that dy-
namically change the camera position in order to al-
low the player to explore the 3D virtual environment.
The FiniteStateMachine manager is responsible for
instantiating the finite state machine with the current
clinic case and also managing its execution with the
3
http://unity3d.com/
SeGTE:ASeriousGametoTrainandEvaluateBasicLifeSupport
441

Finite State Machine component. The game man-
ager is responsible for managing all the game me-
chanics, interfaces and player interactions. Finally,
the Unity3D kernel is responsible for managing the
graphical pipeline, graphic asset and scene graph.
4 EVALUATION
One important differentiating factor between serious
games and entertainment games is the importance
of assessment. Measuring, discussing and reasoning
about the game play effectiveness is very important in
this domain. This can lead to reflection and there-
fore improved learning (Lopes and Bidarra, 2011).
Chen and Michael have identified some of the main
challenges that assessment in serious games is facing,
namely effecting and improving player experience.
The authors suggest that log information and teach-
ers/instructors knowledge should be fully explored
and, in some way, incorporated back in the game, to
guide its course (Chen and Michael, 2005).
Pamela Kato (Kato, 2012) has also argued that the
few research studies published on the validity and ef-
ficacy of health games are often poorly designed and
that their conclusions cannot be considered valid evi-
dence to support or refute efficacy. In this respect, she
has suggested a set of guidelines for conducting high
quality efficacy studies on games for health. These
guidelines include grounding the game design in well
defined theories, conducting randomized trials that in-
cluded adequate control groups and number of partic-
ipants, and also incorporating standardized measures
to facilitate comparisons across studies.
The authors agree with the recommendations pro-
vided by the previous cited authors and they have
been considered both during the development of the
game as well as when designing and planning the
evaluation of game play effectiveness. During game
design, both experts and lay people were involved in
defined check-points to validate that both the peda-
gogical goals as well as the user interactions were ac-
cording to the expectations of the end-users. Also,
the inclusion of pedagogical content in the game
had into account previous studies of similar games
and approaches such as design patterns (Bj
¨
ork and
Holopainen, 2005) and finite state machine diagrams.
It was then important to evaluate if the game actu-
ally taught what it had been designed to. This was the
hypothesis of our study. In order to confirm or dis-
card this hypothesis, we designed a qualitative study
based on pre-experimental design research method
(Creswell, 2008), which includes three specific mo-
ments: briefing, where the player is introduced to the
pedagogical goals of the game; a pre-test, where the
user responds to the questionnaire; game experience,
where the user plays the different game modes (train-
ing mode and evaluation mode); and, a pos-test where
the player responds to the questionnaire. The pre-test
and pos-test questionnaire are one and the same, and
consist of a set of questions related to the ERC’s pro-
tocol and some demographic information related to
the player. In the reminder of this section, we detail
how the study was conducted and the achieved results.
4.1 Pre-test and Pos-test
Before each game experience each player was asked
to answer the questionnaire in order to have feed-
back about their knowledge of basic life support. The
main goal of the pre-test was to evaluate the previous
knowledge the user had about the different procedures
provided in ERC’s protocol.
The questionnaire was composed by ten ques-
tions. The first three questions concern demographic
information about the player. According to this infor-
mation, the participants are between 20-30 years; 23
are male and 8 are female, in a total of 31 participants,
without any specific previous knowledge about Basic
Life Support.
The remaining questions, were related to the ERC’s
protocol and they were validated by healthcare pro-
fessionals.
After playing, each player was asked to answer
the questionnaire again in order to evaluate the knowl-
edge the player had acquired during the game session.
The pos-test was exactly like the pre-test except for
the first three questions concerning demographic in-
formation. The main goal of this pos-test was to eval-
uate if the game teaches the sequence of procedures
described in the ERC’s protocol. In other words, vali-
dated the evolution of the user’s knowledge after play-
ing the serious game SeGTE.
After all the participants were evaluated, the data
collected were analysed and the results of the pre and
pos-test were compared.
5 DISCUSSION
Comparing the results of the pre-test with the pos-test,
we obtain better results in all of the questions in the
pos-test. This positive trend may show that the seri-
ous game has some impact in the user’s knowledge,
as presented in Figure 3.
These results are very positive which give us a certain
confidence that the game fulfils its educational goals.
Furthermore, the participants in general demonstrated
GRAPP2014-InternationalConferenceonComputerGraphicsTheoryandApplications
442

Figure 3: Comparison between Pre-test and Pos-test.
to have enjoyed playing the game and they considered
it very interesting. Some participants also got a lit-
tle sad when the victim died. This is an interesting
point, because it demonstrates her/his emotional in-
volvement in the game and their motivation to save
the victim.
Nevertheless, there are also some limitations that
should be mentioned. Namely, although the game was
designed to teach the ERC’s protocol procedures it
can’t be neglected that certain aspects of these pro-
cedures can’t be entirely simulated in a virtual envi-
ronment. For example, in a real-world situation per-
forming compressions requires strength and a certain
level of physical condition to sustain until assistance
arrives. This is why Basic Life Support should ideally
be performed by two helpers instead of just one.
Therefore, it is not intended that this game substi-
tutes training with a life-sized doll with replicated air-
ways and anatomy, used in CPR training to simulate
the performance of rescue breathing and cardiac com-
pressions. Instead, this game should be used as a com-
plement of this training, as it has proven to help mem-
orize the Basic Life Support procedures and some of
its specificities. Also, it can be used as a tool to re-
fresh the knowledge previously acquired in a proper
Basic Life Support Course.
6 CONCLUSIONS
In this paper the serious game SeGTE has been de-
scribed. This game was design to teach the ERC’s
protocol to laypeople, specifically focusing on the
specificities of each procedure and also how it should
be applied according to the current condition of an
adult victim. SeGTE has been developed in collabo-
ration with healthcare professionals, that participated
both in validating the pedagogical content of the game
and the correct simulation of the ERC’s protocol. To
simulate the ERC’s protocol we have used Finite State
Machines, were the states represent the current state
of the patient and the possible actions of the player
are the transitions between states. This representation
also allowed us to set up different clinical cases by in-
stantiating accordingly different finite state machines.
A study based on pre-experimental design was also
conducted in order to assess if SeGTE fulfil its ped-
agogical goals. For that purpose a questionnaire was
devised in collaboration with healthcare profession-
als. This questionnaire was used to evaluate both the
previous and prior knowledge regarding the basic life
support. In between answering the questionnaire the
participant played each clinical case once in training
mode and once evaluation mode. This study involved
31 participants and the analysis and comparison of the
results was presented in section 4. The number of cor-
rect answers increased after the participants played
the game which provided us with some confidence
that the game could be used as a tools to teach or
refresh the procedures of the ERC’s protocol. Nev-
ertheless, as future work this study needs to be ex-
tended to a bigger and more diverse audience in order
to assess its statistical significance. Also, further de-
velopments are being included in the current version
of the game with the goal of integrating it as a learn-
ing tool in the Portuguese Red Cross courses, which
have already shown an interest in SeGTE.
ACKNOWLEDGEMENTS
This work was supported by FCT (INESC-ID
multiannual funding) under the project PEst-
OE/EEI/LA0021/2013. The authors also would
like to acknowledge to the European funded Project
Games and Learning Alliance (FP7 258169) the
Network of Excellence (NoE) on Serious Games.
REFERENCES
Bj
¨
ork, S. and Holopainen, J. (2005). Patterns in Game De-
sign. Charles River Media.
Chen, S. and Michael, D. (2005). Proof of learning: assess-
ment in serious games.
Creswell, W. J. (2008). Research Design: Qualitative,
Quantitative, and Mixed Methods Approaches. Sage
Publications, Inc.
Crookall, D. (1990). Editorial: Future perfect? Simulation
& Gaming: An International Journal, pages 3–11.
Crookall, D. (1992). Editorial: Debriefing. Simulation &
Gaming: An International Journal, pages 141–142.
ERC (2012, acessed 29 October 2012). European resusci-
tation council guidelines 2010.
Fiander, S. (2009). Anyone can save a life: Road
accidents and first aid. (accessed Novembro
SeGTE:ASeriousGametoTrainandEvaluateBasicLifeSupport
443

2012) http://www.medyouthportal.org/Uploads/docs/
RoadAccidents&FirstAids.pdf.
Gaba, D. M., Howard, S. K., Fish, K. J., Smith, B. E.,
and Sowb, Y. A. (2001). Simulation-based train-
ing in anesthesia crisis resource management (acrm):
a decade of experience. Simulation & Gaming,
32(2):175–193.
Hu, W., Zhang, Q., and Mao, Y. (2011). Component-based
hierarchical state machine - a reusable and flexible
game ai technology. In in Information Technology
and Artificial Intelligence Conference (ITAIC), 2011
6th IEEE Joint International, volume 2, pages 319–
324.
IFRC (2009). First aid for a safer future: Fo-
cus on europe. (accessed Novembro 2012)
http://www.ifrc.org/PageFiles/53459/First%20aid
%20for%20a%20safer%20future%20Focus%20on
%20Europe%20%20Advocacy
%20report%202009.pdf.
IFRC (2010). First aid for a safer future: Focus on europe.
(accessed Novembro 2012) http://www.ifrc.org/
PageFiles/53459/First%20aid%20for%20a%20safer
%20future%20Updated%20global%20edition%20
%20Advocacy%20report%202010%20(2).pdf.
Kato, M. P. (2012). Evaluating efficacy and validating
health games. Games for Health Journal, 1(1):74–76.
Lopes, R. and Bidarra, R. (2011). Adaptivity challenges in
games and simulations: a survey. Computer Intelli-
gence and AI in Games, IEEE Transactions on, pages
85–99.
Saini, S., Chung, P., and C.W.Dawson (2011). Mimicking
human strategies in fighting games using a data driver
finite state machine. In in Information Technology and
Artificial Intelligence Conference (ITAIC), 2011 6th
IEEE Joint International, volume 2, pages 389–393.
Thompson, D., Baranowski, T., Buday, R., Baranowski, J.,
Thompson, V., Jago, R., and Griffith, M. J. (2010).
Serious video games for health: How behavioral sci-
ence guided the development of a serious video game.
Simulation & Gaming, 41(4):587–606.
UNECE (2011). Statistics of road traffic accidents in europe
and north america. (accessed Novembro 2012) http:
//www.unece.org/fileadmin/DAM/trans/main/wp6/
pdfdocs/RAS 2011 Final Version.pdf.
GRAPP2014-InternationalConferenceonComputerGraphicsTheoryandApplications
444
