
Preliminary Study on the Design of a Low-cost Movement
Analysis System
Reliability Measurement of Timed Up and Go Test
Asma Hassani
1
, Alexandre Kubicki
2
, Vincent Brost
1
and Fan Yang
1
1
LE2I CNRS 6306 Laboratory, University of Burgundy, Dijon, France
2
INSERM U1093 Laboratory, University of Burgundy, Dijon, France
Keywords:
Geriatric Health, TUG Test, Autonomy Assessment, Kinect, Spatio-temporal Movement Parameter Extrac-
tion, 3D Real-time Video Processing.
Abstract:
In this paper, we present experiments on the design of a novel movement analysis system for real-time balance
assessment in the frail elderly. Using the Microsoft Kinect sensors, we capture TUG (Timed Up and Go) tests
and mainly analyze the transfer from sitting-to-standing and back-to-sitting which represent two of the most
commonly executed human movements. Nine spatio-temporal parameters were extracted from recorded joint
positions by 3D skeletal sequence processing. In order to validate and evaluate the developed system, practical
test experiences have been performed on ten healthy young subjects, who were asked to realize the TUG in
three different conditions: normal, cognitive and motor. Obtained results showed good measurement reliability
and reproducibility with important precision. In addition, we observed that even for young healthy subjects,
there is a significant difference of movement parameter between normal condition and cognitive condition,
which represents a stimulating result in the dual task paradigm field. This preliminary study opens a new
research and development way for geriatric health which implies multiple aspects: user-friendly, hygiene,
low-cost, home-based environment, and automatic autonomy assessment.
1 INTRODUCTION
Geriatric rehabilitation has become a major public
health issue. The balance assessment in the frail el-
derly consists to assess functional capacity and fall
risk, and help determine the underlying reasons for
balance disorders. Also, it can allow to objectify
progress or deterioration and measuring the patient’s
autonomy. Thus, many strategies of balance assess-
ment are developed. Most of these strategies involve
complex operations to perform in clinical environ-
ment and require the presence of a health professional
to determine the score for each person.
Clinical balance assessment can be classified into
three broad categories: system assessments, quanti-
tative assessments and functional assessments. The
system assessments are helpful to determine the un-
derlying causes of the balance deficit. However, all
balance rating scales are relatively course measures
of complex motor behaviour and all subjective assess-
ments can easily suffer from tester bias (Mancini and
Horak, 2010). Regarding quantitative assessments,
several systems are being exposed to the market, but
they are not scientifically validated before being of-
fered to therapists, except some systems such as the
static or dynamic posturography platforms. In gen-
eral, functional balance tests assess performance on a
set of motor tasks on a 3 to 5 point scale or use a stop
as watching to time how long the subject can keep up
balance in a specific posture. Several clinical tests ex-
ist such as Tinetti and TUG. This functional approach
is usually used to detect balance problem existence.
However, clinical balance assessments give subjective
results that are usually not responsive enough to rate
low progress or deterioration in a subject’s ability to
balance (Mancini and Horak, 2010). Indeed, clinical
human evaluation is limited in terms of the parame-
ters evaluated.
In elderly autonomy and independence maintain-
ing context, it is very interesting to realize functional
balance assessments automatically in home-based en-
vironment using artificial vision technology. If an in-
novative device associated with video processing is
capable to assess the motor abilities of the frail el-
derly, health professionals could be alerted in case
of deterioration. The earlier balance problem detec-
tion and the precocity of rehabilitation could allow,
through a primary or secondary prevention, prolong-
662
Hassani A., Kubicki A., Brost V. and Yang F..
Preliminary Study on the Design of a Low-cost Movement Analysis System - Reliability Measurement of Timed Up and Go Test.
DOI: 10.5220/0004747806620667
In Proceedings of the 9th International Conference on Computer Vision Theory and Applications (VISAPP-2014), pages 662-667
ISBN: 978-989-758-004-8
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

ing autonomy and independence of elderly. In addi-
tion, we can increase the number of studied parame-
ters with fairly accurate measurement, by balance as-
sessment automation.
This paper is organized as follows: in section 2
some related works of human motion analysis for re-
habilitation by computer vision are cited. Section 3
presents the proposed real-time system from data ac-
quisition to feature parameter extraction after a brief
description of the TUG test. Section 4 illustrates ex-
periment tests and obtained analysis results with ten
healthy young subjects. Finally, we discuss and con-
clude this preliminary study in section 5.
2 RELATED WORK
Several methods have been developed for human mo-
tion analysis and applied to rehabilitation research.
For example, marker-based systems (MBS) usually
use infrared cameras to detect markers placed on the
patients’ bodies. These systems are accurate and
yield highly robust measurements of a person’s mo-
tion. However, MBS involve frequently the use of
expensive specialized equipment and are impractical
to move. Furthermore, passive or active markers must
be correctly placed on the body before each capture
session which makes such systems obtrusive and in-
appropriate for home-based rehabilitation.
In (Hagler et al., 2010), the authors propose a sys-
tem for continuous and unobtrusive in-home assess-
ment of gait velocity which is based on estimating
walking speed from noisy time and location data col-
lected by a ”sensor line” of restricted view passive in-
frared motion detectors. Indeed, sensor suites provide
information upon the daily activity levels of moni-
tored subjects, and arrays of such sensors allow ob-
taining velocity measurements on a continuous basis
in home settings. However, such systems do not yield
measurements of the detail necessary for assessment
of fall risk, particularly, spatial and temporal gait pa-
rameters (other than walking speed), TUG duration
and sit-to-stand time.
Recent pervasive/ubiquitous healthcare and wire-
less sensor networks incorporate multimodal sensing
and computer vision. The pervasive and ubiquitous
computing aim to integrate information and comput-
ing into the everyday physical world, so that this tech-
nology is available to everyone in any context. Wire-
less sensor network nodes increasingly include iner-
tial sensors such as accelerometers and gyroscopes
which have been used for activity detection and ges-
tural recognition.
Several studies identify the Kinect’s potential for
use in rehabilitation. Indeed, Kinect is an inexpen-
sive and portable sensor that includes a RGB cam-
era, a depth sensor and a multi-array microphone. It
provides full-body 3D motion capture, facial and ges-
ture recognition. Although the accuracy of Kinect is
limited, it still provides a good tradeoff between cost
and portability and could be used at home for reha-
bilitation exercises (Bonnech
`
ere et al., 2012). Re-
cently, Kinect has been shown to be able to create
a 3D human model with similar accuracy to expen-
sive and complex 3D body scanning systems (Weiss
et al., 2011). Moreover, it allows to evaluate gait
velocity (Stone and Skubic, 2011), hand and elbow
movements and anatomical landmark displacement
and trunk angle during commonly performed clini-
cal tests of postural control that represent favorable
results when compared to some existing 3D motion
analysis systems. In (Gabel et al., 2012), a method
for full body gait analysis using Kinect is presented. It
consists in applying a supervised learning approach to
automatically and accurately extract a set of gait pa-
rameters, using the 3D virtual skeleton as the input to
the learned model. Likewise, Kinect is able to obtain
some kinematic and anatomical mapping data with
a similar degree of accuracy to more expensive 3D
motion analysis and scanning systems (Clark et al.,
2012).
In this paper, we propose a low-cost, robust and
home-based system for real-time balance assessment
in the frail elderly. Our system can accurately mea-
sure several parameters that have been shown rele-
vant for balance assessment using the Kinect sensor
and Software Development Kit. It automatically and
accurately extracts shoulder kinematics and TUG du-
ration by the use of the 3D skeleton, with robustness
to environmental changes and variations in the place-
ment of the Kinect sensor. We demonstrate how a
rich set of parameters can be extracted. Furthermore,
we suggest that the proposed method is not cumber-
some since in a typical use-case a Kinect sensor can
be placed in a fixed position at home. In addition, our
system requires no human intervention and no mark-
ers or wearable sensors will be attached to the body.
3 FUNCTIONAL BALANCE
ASSESSMENT SYSTEM
DESIGN PRESENTATION
3.1 Timed Up and Go Test Description
The Timed Up and Go test is a clinical measure of
balance and mobility in the elderly and in neurolog-
PreliminaryStudyontheDesignofaLow-costMovementAnalysisSystem-ReliabilityMeasurementofTimedUpandGo
Test
663

ical populations. The TUG is relatively simple, re-
quires no special equipment or training and is easily
included as part of the routine medical examination.
It consists of a sequence of sit-to-stand (STS), walk-
ing a distance of 3 m, turning and back-to-sit (BTS).
The total time taken to complete the TUG test allows
predicting the risk of falling. A score of 12 s is con-
sidered as the upper limit of normal mobility. Abnor-
mal mobility was defined as having a TUG score of
>= 20 s. The TUG has been modified to add a sec-
ondary task that could be cognitive or motor. In the
TUG-cognitive, subjects were asked to complete the
test while naming some names that begin with a cer-
tain letter and the TUG-motor consists of completing
the TUG while carrying a cup of water. A score of 15
s on the TUG-cognitive and 14,5 s on the TUG-motor
is associated with increased risk of falls (Mancini and
Horak, 2010).
In general, the TUG rests upon one time measure
to evaluate the overall performance of a sequence of
tasks. However, it can provide specific information
on components of each task that could disclose more
specific mobility problems. The TUG includes two
actions that are commonly executed throughout the
different stages of the human lifetime: STS and BTS.
For both STS and BTS, the shoulder was the first to
move and the last to stop, and it moved in the sagittal
plane with a forward-upward (STS) and downward-
backward (BTS) displacement. These movements al-
low estimating some parameters that were identified
in the literature as relevant for balance assessment
(Manckoundia et al., 2006). These parameters are the
following: a) movement duration, b) shoulder path
curvature, c) trunk angle, and d) ratio which matches
the vertical phase duration divided by the horizontal
phase duration.
3.2 Experimental Setup and Data
Acquisition
We use image processing technology with Kinect
to detect patients’ TUG movements. The proposed
system automatically produces virtual skeleton cor-
responding to the patient’s joint position, and this
skeleton information allows determining in real-time
spatio−temporal parameters which are relevant for
the balance assessment.
To extract parameters for balance assessment,
we captured Kinect skeleton recordings of the TUG
movement realized by the subject with time synchro-
nized (see Figure 1). Therefore, we used the data ac-
quired to compute the parameters set. The Kinect sen-
sor was placed to capture the image of the subject at
an approximate distance of 2−2,5 m to the chair, at a
height of 50−60 cm above the floor. The subject di-
rectly faced the Kinect sensor. The Kinect sensor and
its SDK produce a 3D virtual skeleton to establish the
positions of 20 skeleton joints on a human form. For
example, skeleton tracking determines where a user’s
head, hands, knees, and center of mass are. For each
of these skeleton joints, X, Y, and Z values are re-
ported. Kinect provides approximately 30 skeleton
frames per second.
Figure 1: Overview of the proposed system with Kinect sen-
sor.
3.3 Kinematic Parameter Extraction
Process
To begin the calculation of parameters, it is first nec-
essary to determine whether the subject is sitting or
not. The posture and position of a subject’s body
joints define a pose; more specifically, it is the rela-
tionship of each joint to another. A pose is detectable
by either intersection or position of joints or the angle
between joints, using one or more plane. The distance
between two points for 2D and 3D points is respec-
tively given by:
d
2
=
q
(x
1
−x
2
)
2
+ (y
1
−y
2
)
2
(1)
and:
d
3
=
q
(x
1
−x
2
)
2
+ (y
1
−y
2
)
2
+ (z
1
−z
2
)
2
(2)
Regarding the joint angles, we can draw a triangle us-
ing any two joint points. The third point of the trian-
gle is derived from the other two points. The Law of
Cosines formula defined as:
c
2
= a
2
+ b
2
−2abcosC (3)
where C is the angle opposite side c, gives us the value
of any desired angle. Transforming the formulas to
solve for the unknown angle C yields:
C = arccos(
a
2
+ b
2
−c
2
2ab
) (4)
Extracted features correspond to the kinematics
of shoulder displacement during STS and BTS and
VISAPP2014-InternationalConferenceonComputerVisionTheoryandApplications
664
the TUG duration. STS is composed of two main
phases: the first phase is the forward flexion and the
second, the extension phase, started on lift-off of the
buttocks from the seat and ended when maximum
hip, trunk and knee extension and maximum head
flexion velocity were reached. BTS is characterized
by a movement in the opposite direction than STS:
downward and backward.
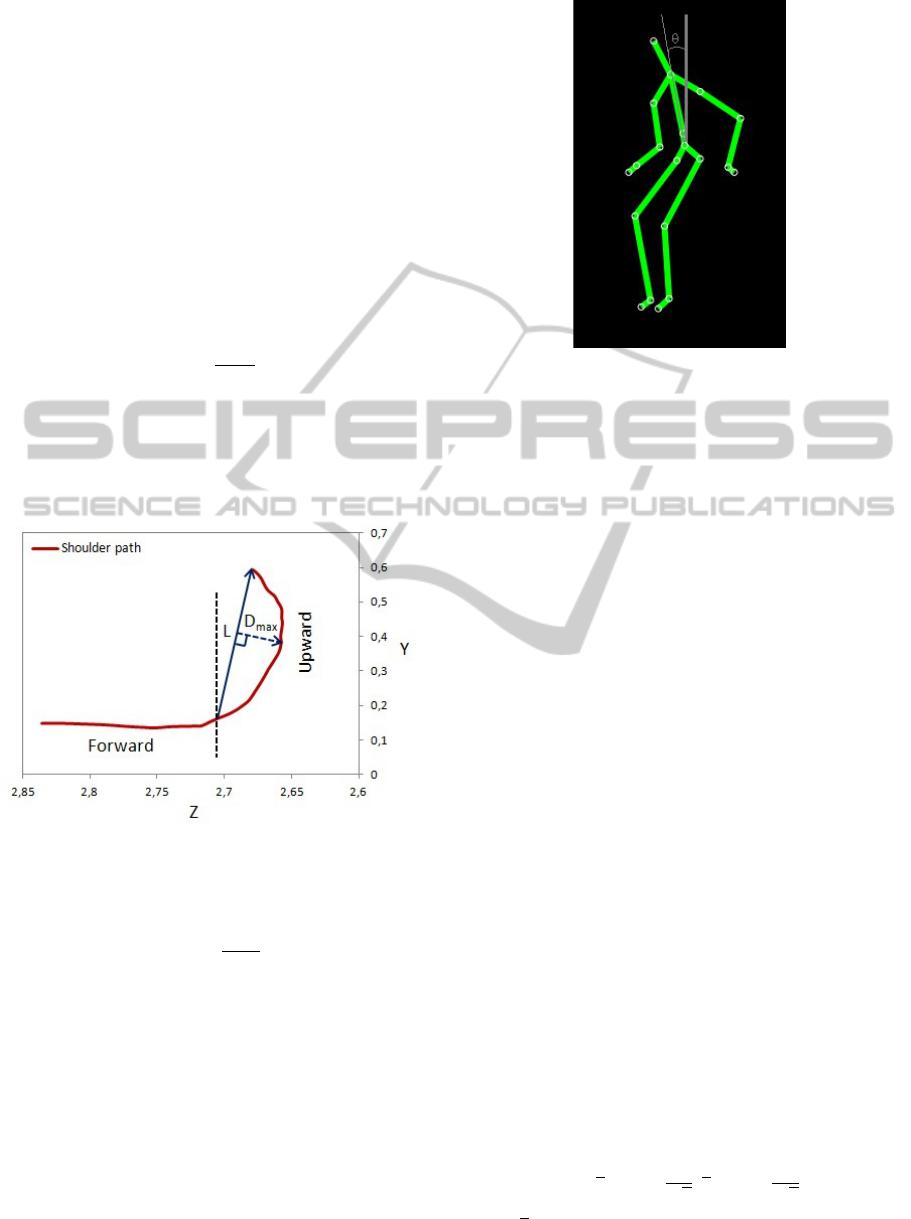
Shoulder Path Curvature. Shoulder paths during
forward and backward displacements were similar
and almost straight, therefore the curvature of path
for upward and downward displacements were only
calculeted (Manckoundia et al., 2006). Curvature is
defined as:
cur =
D
max
L
(5)
where L corresponds to a straight line passing be-
tween the initial and the final position of shoulder
displacement and D
max
means the maximal perpen-
dicular distance measured from the actual path to the
straight line.
Figure 2: Shoulder path during STS transfer. Curvature of
paths is given by the ratio Dmax/L.
Ratio. The ratio is computed using the following re-
lationship:
ratio =
D
vph
D
hph
(6)
where D
vph
and D
hph
they represent, respectively, the
vertical and the horizontal movement duration.
Trunk Angle. It refers to the angle θ between the
trunk and the vertical plane passing through the
center of mass of the body (see Figure 3).
Movement Duration. The total movement duration
of shoulder motion, during STS, corresponds to the
time interval between the moment when the shoul-
der depth component exceeded 8, 5% of its initial
position, and the moment when the head vertical
Figure 3: Trunk angle calculation.
component reaches or exceeds 94% of the size of
the person which was calculated. The thresholds are
experimentally determined. In BTS, it is defined
as the time interval between the moment when the
shoulder vertical component dropped its peak value,
and the moment when the vertical components of the
hips reach their minimum values and the trunk angle
reaches its limit.
TUG Duration. TUG duration, measured in seconds,
means the total time taken to perform all TUG tasks.
It corresponded to the time interval between the mo-
ment when the forward phase starts and the moment
when the backward phase ends.
4 EXPERIMENT RESULTS
4.1 Experimental Protocol
Ten healthy young subjects participated in the present
study. Subjects were asked to complete three tri-
als for each of three TUG conditions: the TUG
alone (TUG−normal), the TUG−cognitive and the
TUG−motor. Subjects were given verbal instructions
to rise from a chair, walk 3 m, cross a mark on the
floor, turn around, walk back, and sit down again.
4.2 Result Analysis
Figure 4 shows STS parameter histograms for
TUG−normal. In this section, the confidence inter-
val (CI) is defined as:
I
c
= [x −1, 96
s
√
n
;x + 1, 96
s
√
n
] (7)
where x, s and n represent, respectively, the mean, the
standard deviation and the size of the sample. The
PreliminaryStudyontheDesignofaLow-costMovementAnalysisSystem-ReliabilityMeasurementofTimedUpandGo
Test
665
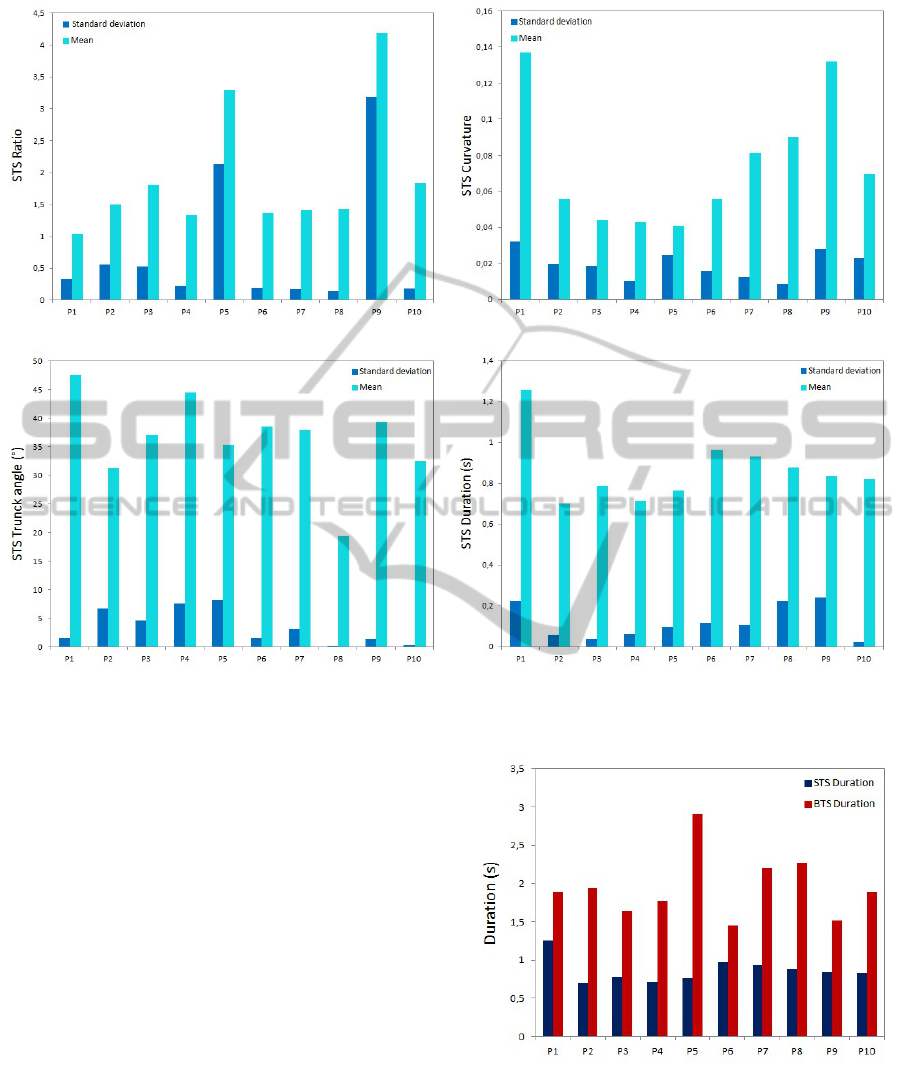
(a) Histogram of STS ratio parameter. (b) Histogram of STS curvature parameter.
(c) Histogram of STS trunck angle parameter. (d) Histogram of STS duration parameter.
Figure 4: Histogram of STS ratio, curvature, trunck angle and duration parameters of 10 young healthy subjects (P1-P10).
CI of the ratio, the curvature, the trunck angle and
the duration during STS for the TUG-normal are, re-
spectively, [1,038; 2,798], [0,051; 0,098], [31,162;
41,548], and [0,744; 0,987]. For the ten subjects, 70%
of the mean values of ratio, trunck angle and duration
are contained in their CI. This indicates that the vari-
ability of parameter measurement is reduced between
the different subjects for these three parameters and
we suggest that our system processes good measure-
ment reliability. Regarding the curvature, only 50%
of the mean values are in the CI. Indeed, the calcu-
lation is based on the outbreak of the vertical phase
which takes into account the size differences between
subjects. Therefore, the variability of curvature values
between subjects is not related to a miscalculation of
our system, but rather to inter-individual differences.
In figure 5, duration of STS was shorter than dura-
tion of BTS which was proved in the work of Mourey
(Manckoundia et al., 2006).
Concerning dual TUG task, in TUG-Normal,
mean values of the TUG duration are between 8,21
Figure 5: Comparison between STS duration and BTS du-
ration.
s and 11,89 s, in TUG-motor, they are between 8,18 s
and 12,65 s and in TUG-cognitive, they are between
8,21 s. and 14,84 s. These values refer to healthy
subjects as the limit score of each test is not exceeded
(see Section 3.1). These results are compatible with
VISAPP2014-InternationalConferenceonComputerVisionTheoryandApplications
666
previous studies. During STS, mean value of trunck
angle is between 18, 30
◦
and 49, 62
◦
, and in BTS, it is
between −3, 53
◦
and 54, 68
◦
.
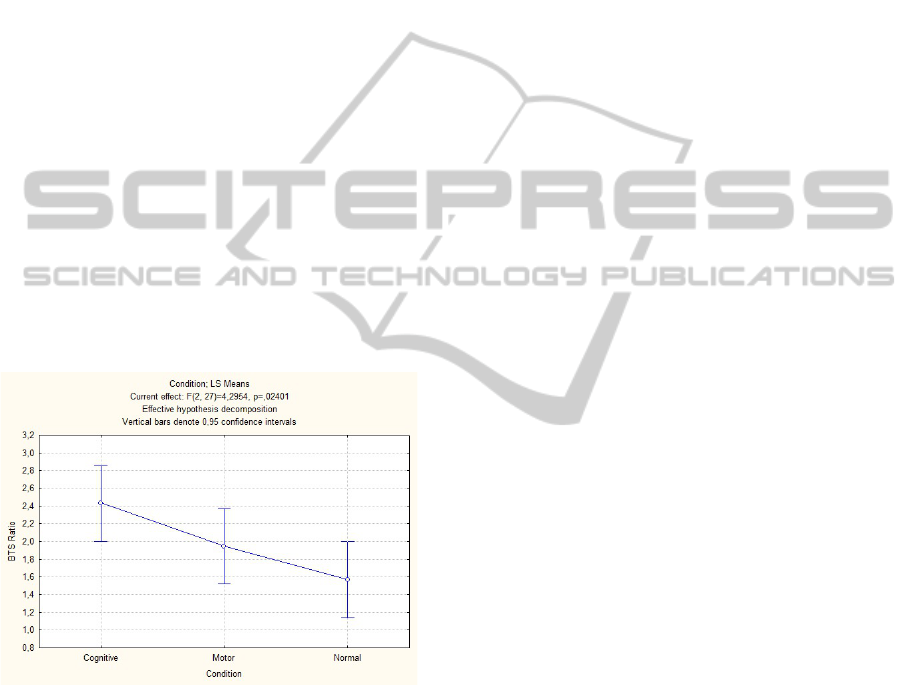
The only parameter showing a main effect of the
factor ”condition” is the ratio in BTS transfer. For this
parameter, Kolmogorov-smirnov and Shapiro-Wilk
tests showed that the distribution follows a NORMAL
law (see Figure 6). Results from the one-way analy-
sis of variance (one-way ANOVA), whose factor is
condition, showed that there was a high variability in
the BTS ratio between normal condition and cognitive
condition (F(2, 27)= 4,2954, p= ,02401). A post hoc
within condition analysis was performed and showed
that there is a significant difference between normal
condition and cognitive condition, this last result is
very stimulating regarding the literature about dual
task paradigm field. In aging, the automatic motric-
ity seems less efficient and some functional activities,
as the TUG, need a cognitive involvement (Teasdale
and Simoneau, 2001). Some authors proposed that
the BTS motion could be an interesting tool to assess
posturo-motor abilities (Manckoundia et al., 2006) in
aged adults. Here we showed that a simple BTS anal-
ysis can reveal an impairment involved by the dual
task condition even in a population of young adults.
Figure 6: Result of one-way ANOVA analysis.
5 CONCLUSIONS
In this work, we have presented a novel movement
analysis system for real-time balance assessment in
the frail elderly. It captured and recorded the TUG
test movement using a Kinect sensor and nine spatio-
temporal parameters were automatically extracted for
sit-to-stand and back-to-sit transfers by 3D real-time
video processing. Obtained experiment results with
ten healthy young subjects showed good measure-
ment reliability and reproducibility with important
precision. In addition, we showed that even in young
healthy subjects, some modifications of motor pat-
terns can be seen in dual task condition. Moreover,
our system allows detecting some very fine changes
in posturo-motors abilities.
Our future works consist to perform TUG test for
real-time balance assessment in the frail elderly to
validate the proposed system in real world condition.
This study will open a new research and development
way for geriatric health which implies multiple as-
pects: user-friendly, hygiene, low-cost, home-based
environment, and automatic autonomy assessment.
REFERENCES
Bonnech
`
ere, B., Jansen, B., Salvia, P., Bouzahouene, H.,
Omelina, L., Cornelis, J., Rooze, M., and VAN
SINT JAN, S. (2012). What are the current limits of
the kinect sensor? Proc. 9th Intl Conf. Disability, Vir-
tual Reality & Associated Technologies (ICDVRAT),
pages 287–294.
Clark, R. A., Pua, Y.-H., Fortin, K., Ritchie, C., Webster,
K. E., Denehy, L., and Bryant, A. L. (2012). Valid-
ity of the microsoft kinect for assessment of postural
control. Gait & Posture, 36(3):372–377.
Gabel, M., Gilad-Bachrach, R., Renshaw, E., and Schuster,
A. (2012). Full body gait analysis with kinect. In 2012
Annual International Conference of the IEEE Engi-
neering in Medicine and Biology Society (EMBC),
pages 1964–1967.
Hagler, S., Austin, D., Hayes, T. L., Kaye, J., and Pavel, M.
(2010). Unobtrusive and ubiquitous in-home monitor-
ing: A methodology for continuous assessment of gait
velocity in elders. IEEE transactions on bio-medical
engineering, 57(4):813–820.
Mancini, M. and Horak, F. B. (2010). The relevance of clin-
ical balance assessment tools to differentiate balance
deficits. European journal of physical and rehabilita-
tion medicine, 46(2):239–248.
Manckoundia, P., Mourey, F., Pfitzenmeyer, P., and Pa-
paxanthis, C. (2006). Comparison of motor strate-
gies in sit-to-stand and back-to-sit motions between
healthy and alzheimer’s disease elderly subjects. Neu-
roscience, 137(2):385–392.
Stone, E. and Skubic, M. (2011). Evaluation of an inexpen-
sive depth camera for passive in-home fall risk assess-
ment. In 2011 5th International Conference on Perva-
sive Computing Technologies for Healthcare (Perva-
siveHealth), pages 71 –77.
Teasdale, N. and Simoneau, M. (2001). Attentional de-
mands for postural control: the effects of aging and
sensory reintegration. Gait & posture, 14(3):203–210.
Weiss, A., Hirshberg, D., and Black, M. (2011). Home 3D
body scans from noisy image and range data. In 2011
IEEE International Conference on Computer Vision
(ICCV), pages 1951–1958.
PreliminaryStudyontheDesignofaLow-costMovementAnalysisSystem-ReliabilityMeasurementofTimedUpandGo
Test
667
