
Moving Medical Semeiotics to the Digital Realm
SEMEOTICONS Approach to Face Signs of Cardiometabolic Risk
Giuseppe Coppini
1
, Riccardo Favilla
1
,
Amalia Gastaldelli
1
, Sara Colantonio
2
and Paolo Marraccini
1
1
CNR Institute of Clinical Physiology, Pisa, Italy
2
CNR Institute of Information Science and Technology, Pisa, Italy
Keywords: Face Semeiotics, Cardiovascular Diseases, Cardio-metabolic Risk Factors, Cardio-Metabolic Risk Signs,
Personalized Prevention, Self-monitoring, Virtual Individual Model, Well-being Index.
Abstract: In modern medicine signs derivable from face observation remain an important part of the physical
examination that, together with the anamnesis, constitutes the basis for a rational decision-making.
Therefore, face semiotics may be considered as a potential source of information for obtaining markers of
obesity, metabolomics, cardiovascular homeostasis and psychophysical status. Once properly mapped to
computational descriptors, their systematic exploitation is expected allowing the building of effective self-
monitoring systems. In this perspective, in the frame of the FP7 project SEMEOTICONS, the most relevant
face signs of cardio-metabolic risk are reviewed and analysed so as to drive their detection, quantification
and integration into a virtual individual model useful for cardio-metabolic risk prevention.
1 INTRODUCTION
Human face has been always considered to be a
mirror of emotions, mood and health status. Face
signs have been studied since the time of Aristotle.
Hippocrates already described aspects of
pathological conditions related to face, becoming
common heritage to associate face traits with
character, psychological dispositions and health
status.
In present days, medical semeiotics deems the
face as an important revelaer of precious information
about the healthy or unhealthy status of individuals,
produced by the combination of biophysical signs
and expressive features. Experienced medical
doctors acquire a personal and typical ability in
reading and interpreting the complex and composite
signs of patients’ face. These signs usually suggest
how to steer the medical examination and may
contribute to suggest which diagnostic investigations
are to be prescribed. So far, although its striking
importance, semeiotic evaluation has not raised a
systematic scientific interest. Despite the face
represent a naturally pre-eminent mean for
communication among human beings and
modulating inter-personal interaction, the valuable
pieces of information conveyed by human face have
not been comprehensively investigated with the aim
to assist medical professional and individuals with
computational tools.
Nowadays, results from clinical and
epidemiological studies strongly stimulate the
development of personalized health care systems.
This is also in view of new and more efficient
strategies for disease prevention, which is a strategic
objective for modern health systems. On the other
hand, personalized systems working at individual
home offer a significant way to contain health care
costs with improved effectiveness and efficiency.
Proficient self-monitoring coupled to individual
education and coaching is key point to build systems
capable to help people staying healthy. The FP7
project SEMEOTICONS (SEMEiotic Oriented
Technology for Individual’s CardiOmetabolic risk
self-assessmeNt and Self-monitoring) has as a major
technological objective the building of a
multisensory system having the appearance of a
conventional mirror, called the Wize Mirror, to be
hosted in everyday life environments (including
individuals’ home, pharmacies, fitness centres and
schools). The Wize Mirror will exploit face
semeiotics to instantiate a Virtual Individual Model
(Honka et al., 2011) from which a Well-Being Index
(WBI) will be obtained. Starting form an initially
defined state, tracking WBI temporal evolution will
enable individual to self-monitor life-style related
606
Coppini G., Favilla R., gastaldelli A., Colantonio S. and Marraccini P..
Moving Medical Semeiotics to the Digital Realm - SEMEOTICONS Approach to Face Signs of Cardiometabolic Risk.
DOI: 10.5220/0004939106060613
In Proceedings of the International Conference on Health Informatics (SUPERHEAL-2014), pages 606-613
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

risks for cardio-metabolic diseases and implement
personalized prevention actions.
In the following, we will review and analyse
some basic aspects of face semeiotics so as to define
the traits of a related computational model.
2 MEDICAL SEMEIOTICS
The face is a fine descriptor of a person’s well-being
state and, people, not only doctors, commonly derive
from the observation of the face significant clues
about psychophysical condition. Evidence on the
state of nutrition, fitness, and mental state can be
obtained. In addition, conditions affecting the colour
or the appearance of the skin can be also revealed.
The appearance and features of the face allow the
distinction among ethnicity, gender, age and
emotions (such as happiness, sadness, fear, anxiety,
and pain). Face changes can be due to alterations of
skeletal and/or muscular structure, subcutaneous
tissue, colour of the skin and eyeballs appearance.
For examples, chronic endocrinological diseases
(achondroplasia, acromegaly) and congenital anemia
(thalassemia) may produce characteristic alterations
of bone structures. Diseases of the nervous system
(Parkinson, myasthenia, tetanus) may cause typical
variations of the muscular structures. Other local and
systemic illness may induce modifications of the
superficial tissues due to changes of water content,
growth of adipose tissue, and deposition of
mucoproteins such as in the case of myxoedema
(hypothyroidism). Haemoglobin concentration,
oxygen saturation, vasodilation or vasoconstriction
affects the colour of facial skin (pallor, redness, and
cyanosis); moreover the deposit of other substances
may be responsible of pathologic appearance of the
skin, as bilirubin in jaundice. Local accumulation of
cholesterol may become evident with the appearance
of xanthelasmas in the eyelid and arcus cornealis, a
white ring in front of the periphery of the iris.
Moreover some clusters of characteristic features of
the face are considered pathognomonic of specific
medical conditions such as mitral face (mitral
stenosis), Hippocratic face (sepsis), lunaris face
(Cushing's syndrome, obesity) and other well-known
semeiotic facies.
From this brief summary, it is evident that
building a comprehensive model of face semeiotics
able to capture all the available pieces of
information is an extremely complex task.
Therefore, focusing on a specific application helps
to make the problem tractable. Moreover, working
with a “real world” setting is expected offer a
significantly general framework for further
utilization.
That led us to focus on cardiovascular diseases
(CVD) and cardio-metabolic risk for which the need
of personalized prevention strategies has gained a
universal acceptance.
3 CARDIOMETABOLIC RISK
Atherosclerotic cardiovascular diseases (CVDs),
including heart disease and stroke, are the leading
causes of mortality worldwide (World Health
Organization, 2008). The atherosclerotic illness
develops insidiously, and clinical manifestations
often become evident in its advanced stages.
Altogether, frequently, the major events, such as
serious health complications, disability and death
occur between 40 and 60 years of age. Moreover, the
majority of patients who survive a myocardial
infarction do not fully recover the ventricular
function, and many stroke survivors have physical
limitation in the daily activities. This explains why
CVDs represent one of the major challenges to the
health systems and considerable efforts are profuse
to treat clinical manifestations of CVDs. These
efforts have granted significant advances with actual
improvements in patients’ outcome, quod ad vitam
and valitudinem (Ford et al., 2007).
Despite the success of the pharmacological,
interventional, and surgical treatment of the CVDs,
it is obvious that all these therapies cannot modify
the epidemiological impact of the disease.
Moreover, the cost of health systems grows
exponentially with the widespread use of complex,
and often inappropriate, diagnostic procedures, as
well as with population aging. At present, the
strategy of prevention, which attempts to modify
some pathophysiological factors related to the
genesis of the disease, seems to be the only way to
limit the epidemic growth of CVDs (Graham et al.,
2007). In a recent paper (Pandya et al., 2013) on
forecasting cardiovascular disease in the USA
through the year 2030, an inversion of the
epidemiologic trend was found, which predicts an
increase in the overall incidence of cardiovascular
disease. This trend is related to two independent
factors: the aging of the population and the
incidence of obesity and diabetes.
Cardio-metabolic risk is a cluster of risk factors
indicative of a patient's overall risk for CVD and
type-2 diabetes. These risk factors include: incorrect
dietary habits, physical inactivity, smoke, alcohol
abuse, abnormal lipid metabolism, hyper-glycaemia,
and arterial hypertension (Grundy et al., 2005,
National Cholesterol Education Program, 2002,
MovingMedicalSemeioticstotheDigitalRealm-SEMEOTICONSApproachtoFaceSignsofCardiometabolicRisk
607

Kahn, 2005). In particular, the metabolic syndrome
is characterized by groups of clinical and metabolic
features that include high triglycerides, low HDL
cholesterol, high blood pressure, high fasting
glucose, visceral adiposity (Alberti et al., 2006,
Lorenzo et al., 2007). Epidemiological studies have
shown that persons with metabolic syndrome have
morbidity and mortality for cardiovascular disease
3-4 times increased as compared to control
population (Isomaa et al., 2011).
The importance of primary prevention for the
decrease of cardiovascular epidemic is well
documented by epidemiological studies (Tunstall-
Pedoe, 2003) Moreover the impact on mortality of
prevention is judged higher in comparison with the
effects of evidence-based therapies such as medical
and interventional treatments (Ford, 2007; Di Chiara
et al., 2009). According to this observation some
clinical trials and observational studies have shown a
rapid decline in the risk for cardiovascular disease
mortality after individual or population-wide
changes in diet and/or smoking and in general
following a healthy life-style (Capewell et al., 2011).
In addition, the favourable impact of prevention on
human wellbeing and economics has been estimated
by committees of several countries (Capewell et al.,
2011, National Institute for Health and Clinical
Excellence 2010). Unfortunately, the adherence to
the recommended lifestyles and the proportions at
goal for blood pressure, lipids, and blood glucose in
patients at high risk resulted less than 50% in
European surveys (Kotseva et al., 2009; 2010).
Educational programs and lifestyle interventions
represent effective tools for reducing cardio-
metabolic risk profile and incidence of CVDs
(Laaksonen, 2002, Tuomilehto et al., 2001, Vale et
al., 2005). However, maintaining a healthy lifestyle
frequently needs the counselling and supervision of
various health professionals such as dieticians,
physical trainers, psychologists and behaviourists.
Such a prevention strategy is individually tuned and
requires an expensive organization of the health
systems.
This evidence suggests the need for new strategies
aiming to directly involve people and families in this
important task (Aktas, 2004). Self-monitoring is an
effective tool to stimulate individual awareness of
physical cues and/or behaviours and to identify the
barriers to changing behaviour. It may allow the
recognition of goals and may provide direct
feedbacks guarantying discretion and confidentiality.
At the same time, people may choose to activate
external communication with prompts such as
personal digital assistant or health care professionals
(Appel et al., 2003, Wing, 1999). Ward et al., (2010)
analysed clinical trials that used self-monitoring in
the area of cardiovascular risk management. They
indicated 4 major interventions obtainable with self-
monitoring strategies: a) education b) self-
measurement c) adjustment of (or adherence to)
behaviour d) contact with health professionals
(Figure 1).
Figure 1: Basic self-monitoring strategy.
As a matter of fact, a rationale alternative to the
intensive use of conventional individual coaching is
the exploitation of properly developed systems for
self-learning and self-monitoring. These systems are
expected to help people to change and maintain their
lifestyle providing tailored suggestions about
nutrition, weight, physical activity, fatigue, and
stress according to daily surveys. Moreover, data
collected by such coaching systems could be
analysed and interpreted by health care professionals
so as to support decision-making targeted to the
specific individual conditions. This approach has the
potential to result highly cost-effective and might
foster the diffusion of self-coaching systems with
favourable impact on social, physiological, and
environmental factors that, at present, remain
barriers for the success of large-scale preventive
intervention on CVD and diabetes.
4 CARDIO-METABOLIC RISK
AND FACE SIGNS
In Table 1 we list a set good indicators of patient’s
overall risk for CVD and type-2 diabetes. These risk
factors are classified in two groups: modifiable and
non-modifiable. The majority of them belong to the
modifiable category.
In SEMEOTICONS, we propose the adoption of
self‐
measuremen
t
coach
adjust
HEALTHINF2014-InternationalConferenceonHealthInformatics
608

a digital semeiotics of the face, that is the
computational evaluation of facial signs, focused on
those signs that relate to some widely recognized
risk factors of CVDs. Consequently, a semeiotic
model of the face can be defined taking into account
signs concerning: obesity, diabetes, hyper-
cholesterolemia, endothelial dysfunction, and
psychological status.
Other general semeiotic signs can be considered
to gain more general information about the overall
individual’s condition.
Each of the above-mentioned risk factors has
several observable manifestations on an individual’s
face.
Table 1: Main cardio-metabolic risk factors.
Modifiable factors
Non-modifiable
factors
Overweight/Obesity
High LDL
cholesterol
Low HDL
cholesterol
High triglycerides
hyper-coagulation
High blood glucose
Hypertension
Inflammation
Smoking
Unhealthy
eating
Health
disparities
Physical
inactivity
Psychosocial
issues
Age
Race/Ethnicity
Gender
Family history
Obesity: The general appearance and several
features of the face are relevant indicators of
overweight and obesity. The reconstruction of face
shape from images and videos and its
characterization through a detailed morphometric
analysis can, then, serve to localize and evaluate a
fatty physiognomy.
Diabetes: The metabolic alterations due to diabetes
favour the glycation of proteins and the
accumulation of Advanced Glycation End-products
(AGE) in the skin (Singh et al., 2001). According to
recent results in AGE detection and measurements,
autofluorescence stimulated by UV light is a viable
solution to detect AGE in sub-cutaneous layer.
Diagnostic instrument working in contact with
forearm skin are commercially available for clinical
use (Meerwaldt et al., 2004). Contact-less
measurement of AGEs looks a challenging task.
Using hyperspectral-imaging methods is expected to
provide a meaningful solution to the problem.
Hyper-cholesterolemia: High level of blood
cholesterol could result in some typical signs that
have been often related to hypercholesterolemia. In
particular, this may be the case of xanthelasmas in
the periocular region, as well as the arcus cornealis
in the iris border. Both these signs are detectable and
reasonably quantifiable in the images of the face
with proper morphological/structural analysis
methods. Furthermore, one expects that visible -
near infrared (VIS-NIR) spectroscopy and imaging
may be used to assess the accumulation of
cholesterol in the skin of the face and in the iris
(Ikawa et al., 2009). As in the case of AGEs, contact
measurement of skin cholesterol is described in
literature using different approaches (Zawydiwski et
al., 2001; Mancini et al., 2002), while contactless
measurements are still open to scientific
investigation. It must be also pointed out that a
deepened knowledge about skin cholesterol
accumulation processes and their relation to cardio-
metabolic risk would be an important achievement.
Endothelial Dysfunction: Endothelial dysfunction is
a major physio-pathological mechanism that leads
towards coronary artery disease. Broadly speaking,
the endothelium function can be seen as the
capability of the endothelium to balance between
vasodilating and vasoconstricting substances
produced by (or acting on) the endothelium.
Endothelial dysfunction can result from and/or
contribute to several disease processes (e.g.
hypertension, hypercholesterolemia, and diabetes)
and it can also result from environmental factors
(e.g. smoking tobacco, exposure to air pollution).
Endothelial dysfunction is therefore highly
informative about individuals’ health status. Non-
invasive assessment of endothelial dysfunction may
be obtained by per cent Flow Mediated Dilation
(FMD) measured by brachial artery ultrasound
imaging (Peretz et al., 2007). Another simple non-
invasive evaluation of endothelium function adopted
in clinical practice is based on peripheral artery
tonometry (PAT) (Kuvin et al., 2007), which works
by measuring Reactive Hyperaemia Index and has
been tested in several clinical trials at multiple
centres (including major cohort studies such as the
Framingham Heart Study, the Heart SCORE study,
and the Gutenberg Health Study). A simple
alternative to these methods is based on studying
microcirculatory blood flow after local heating
(Joyner et al., 2001). The key point in the latter
approach is that variations in blood supply to sub-
cutaneous districts result in variations of skin optical
properties (“colour”). Consequently, an accurate
analysis of temporal sequences of face images in the
visible and a near-infrared band is a practicable way
to evaluate elementary hemodynamic parameters.
These can relate to heart rate, oxygen saturation,
MovingMedicalSemeioticstotheDigitalRealm-SEMEOTICONSApproachtoFaceSignsofCardiometabolicRisk
609
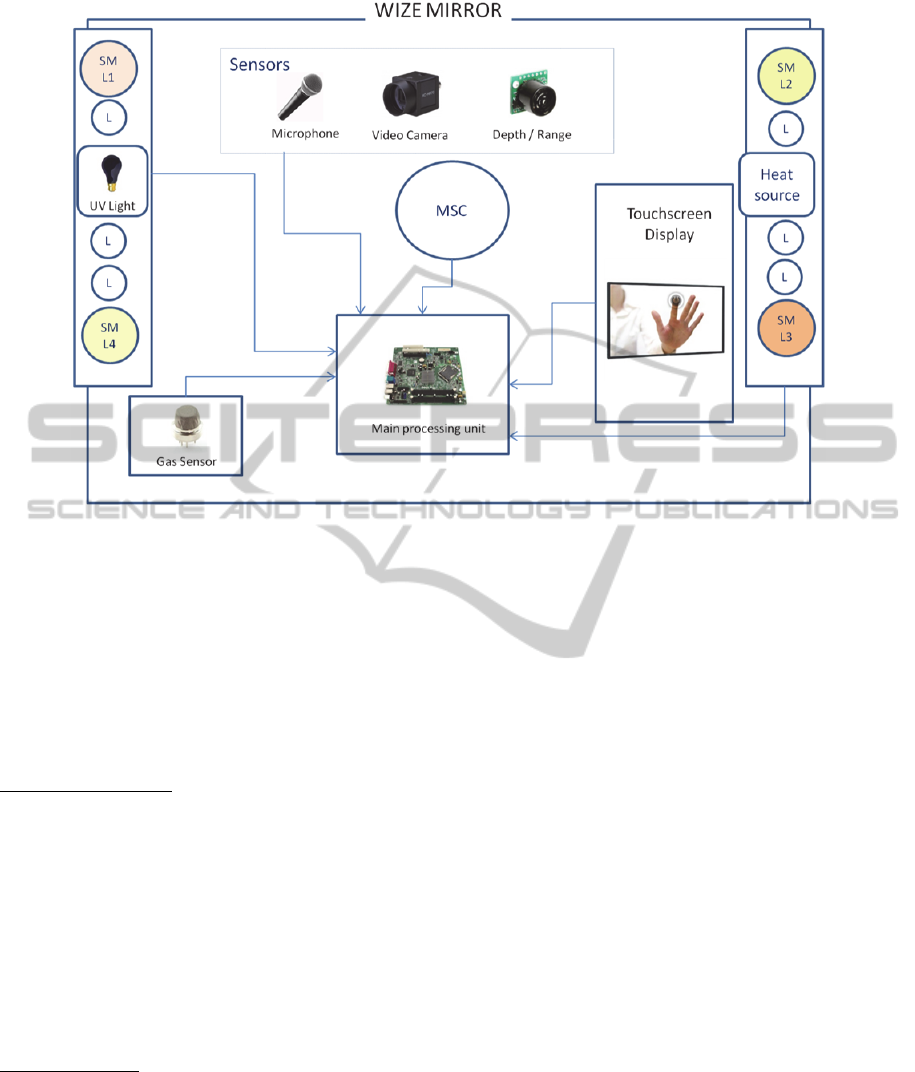
Figure 2: Wize Mirror hardware scheme, including Multi Spectral Camera (MSC), standard lights (L) and multicolour lights
(SMLi, i=1, ...,4).
peripheral resistances and also endothelial function.
Actually, after providing a controlled thermal
stimulus to trigger a vasodilatation, the evaluation of
such hemodynamic response gives a measure that
can be correlated to the endothelial function.
Moreover, the analysis of heart rate variability can
serve to the characterization of the autonomous
nervous system.
Psychological Status: The morphological appearance
of human face can reveal useful information about
an individual’s mood, anxiety, and status of fatigue
(Pantic and Bartlett, 2007). Facial expression
recognition and facial biometrics in 3D space are
expected to serve this scope. Integration of these
descriptors with other well-established cardio
metabolic risk signs into self-monitoring systems is
worth of investigation. Correlation of facial
descriptors of psychological status with
questionnaires can help to better understand their
role to assess an individual’s wellness status.
Other Semeiotics: Among the other signs that can be
related to well being status and may potentially
relate to different individual conditions going from
fatigue/tiredness and stress to specific diseases, the
following are worth of consideration:
– Face colorimetric features, e.g. pallor, jaundice,
redness.
– Regional skin surface temperature in the face.
– Respiratory rate.
5 SEMEOTICONS APPROACH
A main technological objective in SEMEOTICONS
is the development and design of a multisensory
system hosted into a hardware platform having the
exterior aspect of a conventional mirror (Wize
Mirror). A conceptual drawing of the Wize mirror is
shown in Figure 2.
It will include cameras and depth sensors to
enable 3D reconstruction of the user face. This will
be used for morphological analysis (overweight and
obesity description, feature recognition for
psychological status evaluation) as well as to drive
other acquisitions phases (normalization of face
position and orientation). Properly designed
multispectral cameras will allow obtaining data on
the cardio-respiratory system (heart rate, blood-
oxygen saturation, endothelial function, respiratory
rate), on the presence of products of glucose and
lipid metabolism in the skin. The inclusion of other
sensors is also planned. In particular, the Wize
Sniffer, i.e. a gas sensor able to analyse exhaled
gases, will help to monitor lifestyle habits (smoking
and alcohol consumption). The Wize mirror will
include a lighting system for image acquisition, UV
light to stimulate fluorescence mechanisms and
HEALTHINF2014-InternationalConferenceonHealthInformatics
610

Figure 3: Wize Mirror Virtual Individual Model.
thermal lamps for heat testing of endothelial
function. User interaction will occur by an integrated
touch screen.
According to section 4, images and signals have
to be mapped into a set of descriptors, each of them
being related to some aspects of cardio-metabolic
risk. Afterwards, to obtain indication about the
individual’s health status and discover noxious
lifestyles, the computed descriptors, which are
intrinsically disaggregated entities, need to be
integrated into a high-level representation able to
capture the individual as a whole. For that aim, one
has to take into account individual’s peculiarities,
including both family and personal history. The
Virtual Individual Model (VIM) implemented in the
mirror will carry out the integration task. The major
requirement on VIM is the ability to detect and
signal significant changes of face semeiotics to assist
user behavioural change. Therefore, an absolute
assessment of individual wellness is not mandatory.
The model instantiation process shall include a
preliminary user-profiling phase to be accomplished
at the beginning of any self-monitoring activity. This
phase aims at defining the psychophysical
characteristics of the individual at baseline. These
should be derived on the ground of previous medical
examinations, personal history, and interactive
psychological questionnaires.
Therefore, the user profile will serve to define
the initial status of the VIM and may also provide
important constraints on the user-interface
preferences. According to this approach, the
temporal evolution of the model will describe the
changes of the user’s psychophysical status starting
form a known initial condition. In general, past VIM
history would enter the computation of the current
status and is expected to contain useful indications
for user advising and coaching. For these reasons, a
track of the VIM evolution will be retained in the
Individual Diary.
The internal VIM representations and the related
adaption rules are designed to operate at the level of
input data and would be, in general, unsuitable for
user communication and interaction. For this aim
the system would compute the WBI, which
represents a synthetic description of VIM state. The
WBI will be a multidimensional entity whose
components should measure the different aspects of
individual lifestyle appropriateness (e.g. food,
physical activity, psychological status, noxious
habits). According to the profiling phase, WBI
components would be properly presented to the user
along with educational and coaching messages.
To summarize, detection and integration of signs
derived from the semeiotics of the face should lead
to build sensitive equipment to self-monitor the
Initial
Status
VirtualIndividual’s
Model
UserInterface
Well‐BeingIndex
Face
Morphology
Breath
Analysis
Face
Expression
Multispectral
analysis
Iris
Analysis
Individual
Diary
MovingMedicalSemeioticstotheDigitalRealm-SEMEOTICONSApproachtoFaceSignsofCardiometabolicRisk
611

psychophysical state and, possibly, elaborate
suggestions useful for optimizing the personal life
style and to trap the major cardio-metabolic risk
factors.
In this perspective, SEMEOTICONS aims at
building an innovative virtual individual’s model,
which is based on a set of objective signs, closely
related to cardio-metabolic risk profile and derived
from external physical examination of the face. The
model should serve to evaluate a subject well-being
status over time and allow early detection of
improper lifestyles as well as potentially dangerous
conditions mainly related to cardio- metabolic risk.
6 CONCLUSIONS
Medical semeiotics, in the era of magnetic
resonance, computed tomography and molecular
biology, is still a valuable resource that may be
useful in every condition and location independently
of other structural facilities. The development of
advanced imaging and biological diagnostic
techniques has probably attenuated the interest for
developing technological tools based on data
obtained from simple semeiotics. Nevertheless, the
role recently acquired by self-monitoring and self-
training has opened new, significant perspectives to
this well-established branch of classical Medicine.
Semeiotics offers a sound methodological frame
to build new computational tools also exploiting
innovative multi-sensing devices. The adoption of a
digital-semeiotics approach is expected to ease the
implementation of virtual individual models able to
effectively assist people in keeping a healthy life-
style.
In this view, SEMEOTICONS Wize Mirror will
be a new kind of self-monitoring system. Its
architecture will be absolutely non-obtrusive and
will be able to use personal data for coaching and
learner-adaptive messaging.
ACKNOWLEDGEMENTS
This work was partly supported by the EU FP7
Project SEMEOTICONS - SEMEiotic Oriented
Technology for Individual’s CardiOmetabolic risk
self-assessmeNt and Self-monitoring (Grant
agreement no: 611516)
REFERENCES
Aktas MK, Ozduran V, Pothier CE, Lang R, Lauer MS.
2004, Global risk scores and exercise testing for
predicting all-cause mortality in a preventive medicine
program. JAMA, 292:1462 – 1468.
Alberti KG, Zimmet P, Shaw J. Metabolic syndrome—a
new world-wide definition. A Consensus Statement
from the International Diabetes Federation. Diabet
Med (2006) 23: 469–480.
Appel LJ, Champagne CM, Harsha DW, Cooper LS,
Obarzanek E, Elmer PJ, Stevens VJ, Vollmer WM,
Lin PH, Svetkey LP, Stedman SW, Young DR;,
2013.Writing Group of the PREMIER Collaborative
Research Group. Effects of comprehensive lifestyle
modification on blood pressure control: main results of
the PREMIER clinical trial. JAMA, 289:2083–2093.
Capewell S, O’Flaherty M, 2011. Rapid mortality falls
after risk-factor changes in populations. Lancet,
378:752–753.
Di Chiara A, Vanuzzo D. 2009. Does surveillance impact
on cardiovascular prevention? Eur Heart J, 30:1027–
1029.
Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR,
Kottke TE, Giles WH, Capewell S. 2007. Explaining
the decrease in U.S. deaths from coronary disease,
1980 – 2000. N Engl J Med, 356:2388 – 2398.
Graham I, Atar D, Borch-Johnsen K, et al. 2007. European
guidelines on cardiovascular disease prevention in
clinical practice: full text. Fourth Joint Task Force of
the European Society of Cardiology and other
societies on cardiovascular disease prevention in
clinical practice (constituted by representatives of nine
societies and by invited experts). Eur J Cardiovasc
Prev Rehabil, 14 Suppl 2:1–113.
Grundy SM et al. 2005. Diagnosis and management of the
metabolic syndrome. An American Heart
Association/National Heart, Lung, and Blood Institute
Scientific Statement. Executive Summary.
Circulation, 112:2735-2752.
Honka A, Kaipainen K, Hietala H, Saranummi N, 2011.
Rethinking Health: ICT-Enabled Services to Empower
People to Manage Their Health. IEEE Reviews in
Biomedical Engineering, 4:119-139.
Ikawa T, Ishii K, Awazu K, 2009. Hyperspectral imaging
of lipids using near-infrared super continuum light.
WC 2009, IFMBE Proceedings 25/II: 630-632.
Isomaa B, Almgren P, Tuomi T, Forsén B, Lahti K,
Nissén M, Taskinen MR, Groop L. 2001.
Cardiovascular morbidity and mortality associated
with the metabolic syndrome. Diabetes Care, 24:683-
689.
Joyner MJ et al, 2001. Nitric oxide and neurally mediated
regulation of skin blood flow during local heating. J
Appl Physiol, 91:1619-1626.
Kahn R, Buse J, Ferrannin E, Stern M, 2005. The
metabolic syndrome: Time for a critical appraisal.
Diabetes Care, 28:2289-2304.
Kotseva K, Wood D, De Backer G, De Bacquer D,
Pyorala K, Keil U. , 2009. EUROASPIRE III: a survey
HEALTHINF2014-InternationalConferenceonHealthInformatics
612

on the lifestyle, risk factors and use of cardioprotective
drug therapies in coronary patients from 22 European
countries. Eur J Cardiovasc Prev Rehabil 16:121 –
137.
Kotseva K, Wood D, De Backer G, De Bacquer D,
Pyorala K, Reiner Z, Keil U. 2010. EUROASPIRE III.
Management of cardiovascular risk factors in
asymptomatic high-risk patients in general practice:
cross-sectional survey in 12 European countries. Eur J
Cardiovasc Prev Rehabil, 17:530 – 540.
Kuvin JT, Mammen A, Mooney P, Alsheikh-Ali AA,
Karas RH, 2007. Assessment of peripheral vascular
endothelial function in the ambulatory setting. Vasc
Med. 12:13-6.
Laaksonen DE, Lakka H-M, Salonen JT, Niskanen LK,
Rauramaa R, Lakka TA, 2002. Low Levels of Leisure-
Time Physical Activity and Cardiorespiratory Fitness
Predict Development of the Metabolic Syndrome.
Diabetes Care, 25(9): 1612-1618.
Lorenzo CL, Williams K, Hunt KJ, Haffner SM, 2007.
National Cholesterol Education Program - Adult
Treatment Panel III, International Diabetes Federation,
and WHO Definitions of the Metabolic Syndrome as
Predictors of Cardiovascular Disease and Diabetes.
Diabetes Care, 1:8-13.
Mancini GJ, Chan S, Frohlich J, Kuramoto L, Sulzer M,
Abbott D. 2002. Association of skin cholesterol
content, measure by a novel non-invasive method,
with markers of inflammation and Framingham risk
prediction. Am J Cardiol, 89:1313–6.
Meerwaldt R, Graaff R, Oomen PH, Links TP, Jager JJ,
Alderson NL, Thorpe SR, Baynes JW, Gans RO, Smit
AJ. 2004. Simple non-invasive assessment of
advanced glycation endproducts accumulation.
Diabetologia. 47:1324-30.
National Cholesterol Education Program, 2002. Third
report of the National Cholesterol Education Program
(NCEP) Expert Panel on Detection, Evaluation, and
Treatment of High Blood Cholesterol in Adults (Adult
Treatment Panel III). Final report. Circulation,
106:3143-3421.
National Institute for Health and Clinical Excellence, 2010
Prevention of Cardiovascular Disease: Costing
Report. 2010. Nice Public Health Guidance 25.
Pandya A, Gaziano TA, Weinstein MC, Cutler D, 2013.
More Americans Living Longer With Cardiovascular
Disease Will Increase Costs While Lowering Quality
Of Life. Health Aff, 32:1706-1714.
Peretz A, Leotta DF, Sullivan JH, Trenga CA, Sands FN,
Aulet MR, Paun M, Gill EA, Kaufman JD, 2007.
Flow mediated dilation of the brachial artery: an
investigation of methods requiring further
standardization. BMC Cardiovascular Disorders,
7:11.
Singh R, Barden A, Mori T, Beilin L, 2001. Advanced
glycation end-products: a review. Diabetologia, 44:
129-146.
Tunstall-Pedoe H (World Health Organization). MONICA
Monograph and Multimedia Sourcebook. 2003.
Pantic, M, Bartlett M, 2007. Machine Analysis of Facial
Expressions, Face Recognition. In: I-Tech Education
and Publishing, Vienna, Austria, pp. 377-416.
Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT,
Hamalainen H, Ilanne-Parikka P, Keinanen-
Kiukaanniemi S, Laakso M, Louheranta A, Rastas M,
et al., 2001: Prevention of Type 2 Diabetes Mellitus by
Changes in Lifestyle among Subjects with Impaired
Glucose Tolerance. N Engl J Med, 344(18):1343-
1350.
Vale M, Jelinek M, Best J, 2005. Impact of coaching
patients on coro- nary risk factors – Lessons from the
COACH Program. Disease Management & Health
Outcomes 13(4):225-244.
Ward LM, Carl Heneghan C, Perera R, Dan Lasserson D,
Nunan D, Mant D, Glasziou P, 2010. What are the
basic self-monitoring components for cardiovascular
risk management? BMC Medical Research, 10:105.
Wing RR, Jeffery RW, 1999. Benefits of recruiting
participants with friends and increasing social support
for weight loss and maintenance. J Consult Clin
Psychol; 67:132–138.
World Health Organization, 2008. The Global Burden of
Disease: 2004 Update, Geneva, Switzerland: World
Health Organization.
Zawydiwski R, Sprecher DL, Evelegh MJ, Horse- wood P,
Carte C, Patterson M. 2001. A novel test for the
measurement of skin cholesterol. Clin Chem, 47:
1302–1304.
MovingMedicalSemeioticstotheDigitalRealm-SEMEOTICONSApproachtoFaceSignsofCardiometabolicRisk
613
