
Objective Assessment of Asthenia using Energy and Low-to-High
Spectral Ratio
Farideh Jalalinajafabadi
1
, Chaitaniya Gadepalli
2
, Mohsen Ghasempour
1
, Frances Ascott
2
,
Mikel Luj
´
an
1
, Jarrod Homer
2
and Barry Cheetham
1
1
School of Computer Science, University of Manchester, Oxford Road, Manchester, U.K.
2
Department of Otolaryngology, Manchester Royal Infirmary,
Central Manchester University Hospitals Foundation Trust, Manchester, U.K.
Keywords:
GRBAS, Asthenia, MLR, KNNR.
Abstract:
Vocal cord vibration is the source of voiced phonemes. Voice quality depends on the nature of this vibration.
Vocal cords can be damaged by infection, neck or chest injury, tumours and more serious diseases such as
laryngeal cancer. This kind of physical harm can cause loss of voice quality. Voice quality assessment is
required from Speech and Language Therapists (SLTs). SLTs use a well-known subjective assessment ap-
proach which is called GRBAS. GRBAS is an acronym for a five dimensional scale of measurements of voice
properties which were originally recommended by the Japanese Society of Logopeadics and Phoniatrics and
the European Research for clinical and research use. The properties are ‘Grade’, ‘Roughness’, ‘Breathiness’,
‘Asthenia’ and ‘Strain’. The objective assessment of the G, R, B and S properties has been well researched and
can be carried out by commercial measurement equipment. However, the assessment of Asthenia has been less
extensively researched. This paper concerns the objective assessment of ‘Asthenia’ using features extracted
from 20 ms frames of sustained vowel /a/. We develop two regression prediction models to objectively esti-
mate Asthenia against speech and language therapists (SLTs) scores. These regression models are ‘K nearest
neighbor regression’ (KNNR) and ‘Multiple linear regression’(MLR). These new approaches for prediction
of Asthenia are based on different subsets of features, different sets of data and different prediction models
in comparison with previous approaches in the literature. The performance of the system has been evaluated
using Normalised Root Mean Square Error (NRMSE) for each of 20 trials, taking as a reference the average
score for each subject selected. The subsets of features that generate the lowest NRMSE are determined and
used to evaluate the two regression models. The objective system was compared with the scoring of each
individual SLT and was found to have a NRMSE, averaged over 20 trials, lower than two of them and only
slightly higher than the third.
1 INTRODUCTION
Perceptual and objective assessments of voice qual-
ity are widely used for voice disorder evaluation (Yu
et al., 2006; Wuyts et al., 2000; Jalalinajafabadi et al.,
2013). A single measurement cannot quantify all the
properties of an impaired voice that may be of inter-
est to clinicians. The five dimensional GRBAS scale
has the advantage of being widely understood and rec-
ommended by many professional bodies. The GR-
BAS scale is a 5-dimensional measurement of voice
quality where the dimensions are: ‘Grade’, ‘Rough-
ness’, ‘Breathiness’, ‘Asthenia’ and ‘Strain’(Hirano,
1981). ‘Grade’ represents overall degree of hoarse-
ness or voice abnormality.‘Roughness’ is irregular
fluctuation in amplitude and fundamental frequency
of voicing source, ‘Breathiness’ arises from non-
periodic sound and an auditive impression of turbu-
lent air leakage through an insufficient glottis closure.
‘Asthenia’ is weakness or lack of energy in the voice
and ‘Strain’ is difficulty in initiating and maintaining
voiced speech.
Each dimension is traditionally scored by Speech
and Language Therapists (SLTs) on a scale between
0 and 3; 0 for normal, 1 for mild impairment, 2 for
moderate impairment and 3 for severe impairment
(Hirano, 1981). Subjectivity and reliance on highly
trained personnel are significant limitations of tradi-
tional ways of measuring GRBAS parameters. The
objective assessment of G, R, B and S properties has
76
Jalalinajafabadi F., Gadepalli C., Ghasempour M., Ascott F., Luján M., Homer J. and Cheetham B..
Objective Assessment of Asthenia using Energy and Low-to-High Spectral Ratio.
DOI: 10.5220/0005545000760083
In Proceedings of the 12th International Conference on Signal Processing and Multimedia Applications (SIGMAP-2015), pages 76-83
ISBN: 978-989-758-118-2
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
been well researched and commercial equipment ex-
ists that is capable of doing this (Awan and Roy, 2006;
KayPENTAX, 2008). However, the assessment of
Asthenia has been less extensively researched. It is
one of the most difficult components to score and
there is often more discrepancy between SLTs in As-
thenia scoring, than for the other dimensions. This
research is concerned with the objective assessment
of Asthenia (Hirano, 1981).
Patients with Asthenia might be referred to hospi-
tal for treatment. The weakness can caused by a low
intensity of the glottal source sound and is generally
associated with a lack of higher frequency harmonics
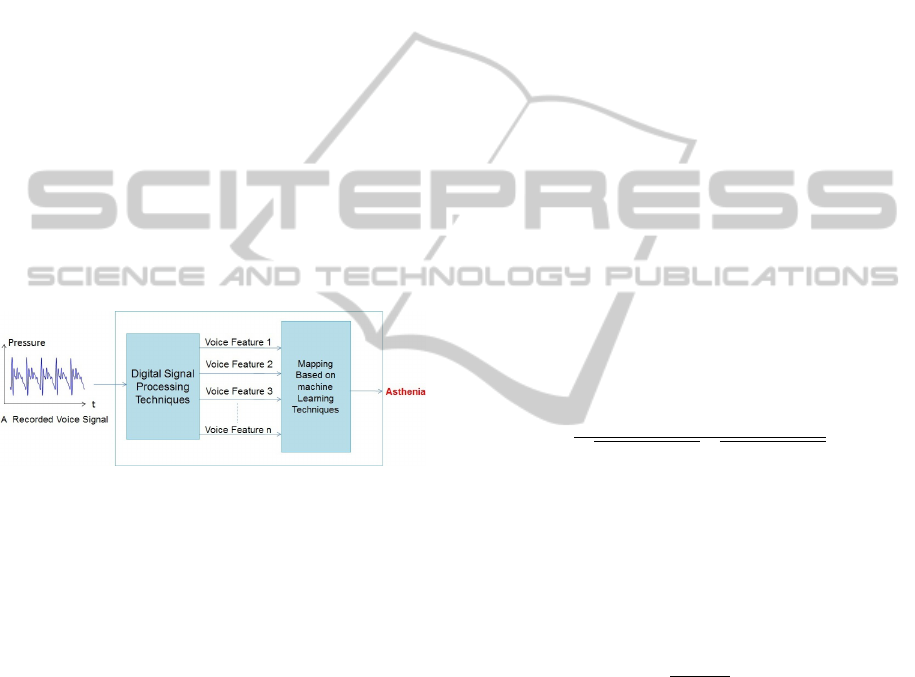
(Hirano, 1981). Figure 1 illustrates the methodology
of the approach. To assess a recorded voice signal
for Asthenia, it will be fed into a digital signal pro-
cessing system for extracting voice features such as
energy, pitch frequency variation, harmonic to noise
ratio and others. This followed by a mapping tech-
nique based on machine learning. The voice features
which reflect the lack of energy and higher frequency
harmonics will be extracted from the voice and used
as features by the mapping techniques.
Figure 1: Methodology of the Approach.
2 DATA COLLECTION AND
ASTHENIA SCORING
Voice data has been collected from a random selection
of 46 patients and 56 controls. Only participants that
can read English fluently were included in this study.
All participants were adults between 18 and 70 years
of age, and they were in different stages of their treat-
ment. Information about the participants was stored in
secure files. The sustained acoustic signals were cap-
tured by a high quality Shure SM48 microphone that
was held a constant distance of 20 cm from the lips
and digitized using the KayPentax 4500 CSL Com-
puterized Speech Laboratory (KayPENTAX, 2008).
Each recording consists of two sustained vowels /a/
and /i/ lasting about 10 seconds, a set of six standard
sentences as specified by CAPE-V (Consensus for au-
ditory perception and evaluation) (Kempster et al.,
2009) and about 15 seconds of free unscripted speech.
To assess the voice quality of each participant sub-
jectively according to the GRBAS scale, the voice
samples were scored by three experienced SLTs using
Sennheiser HD205 head-phones. The samples were
played out in random order with 21 randomly cho-
sen samples repeated as a test for consistency. To
facilitate the scoring process, we developed a ‘GR-
BAS Presentation and Scoring Package’ (GPSP) for
collecting GRBAS scores. The graphical user inter-
face presented by this package is shown in Figure 2.
The software is designed to play out in random order,
with appropriate repetition, the voice samples from a
database of recordings. It enables scores to be entered
by the SLT and stored in the data-base as an excel
spread-sheet easily. The SLTs are given the option of
listening to any samples again, and the software can
be paused at any point, without loss of data. The user
may therefore take breaks to prevent tiredness which
may affect the scoring. The scoring of the 102 voice
samples referred to in this paper was completed by
each SLT in two sessions.
Both Pearson correlation and the Cohen’s Kappa
coefficient were used to measure the level of agree-
ment in scoring Asthenia between each pair of SLTs
(Sheskin, 2003; Cohen, 1968). Equation (1) defines
the Pearson correlation (Sheskin, 2003) between the
two dimensions of a sample {(x
i
,y
i
)} containing n
pairs of random variables (x
i
, y
i
) ; ¯x and ¯y are the
sample means of {x
i
} and {y
i
} respectively.
r =
∑
n
i=1
(x
i
− ¯x)(y
i
− ¯y)
p
∑
n
i=1
(x
i
− ¯x)
2
p
∑
n
i=1
(y
i
− ¯y)
2
(1)
The Cohen Kappa coefficient is defined by Equa-
tion (2) where p
o
is the proportion (between 0 and 1)
of subjects for which the two SLTs agree on the scor-
ing, and p
e
is the probability of agreement ‘by chance’
when there is assumed to be no correlation between
the scoring by each SLT (Streiner, 1995; Viera et al.,
2005).
k =
p
o
− p
e
1 − p
e
(2)
Kappa is widely used for comparing raters or
scorers, and reflects any consistent bias in the aver-
age scores for each scorer (Viera et al., 2005) which
would be disregarded by Pearson’s correlation. A
value less than zero indicates no agreement. Values
in the range 0 to 0.2, 0.2 to 0.4, 0.4 to 0.6, 0.6 to 0.8
and 0.8 to 1 indicate slight, fair, moderate, substan-
tial and almost perfect agreement respectively (Viera
et al., 2005)
Weighted Kappa is often more appropriate when
there are more than two possible scores with a sense
of distance between the scores (Cohen, 1968). With
possible scores 0, 1, 2, 3, Kappa only considers
agreement or disagreement between scores, whereas
ObjectiveAssessmentofAstheniausingEnergyandLow-to-HighSpectralRatio
77
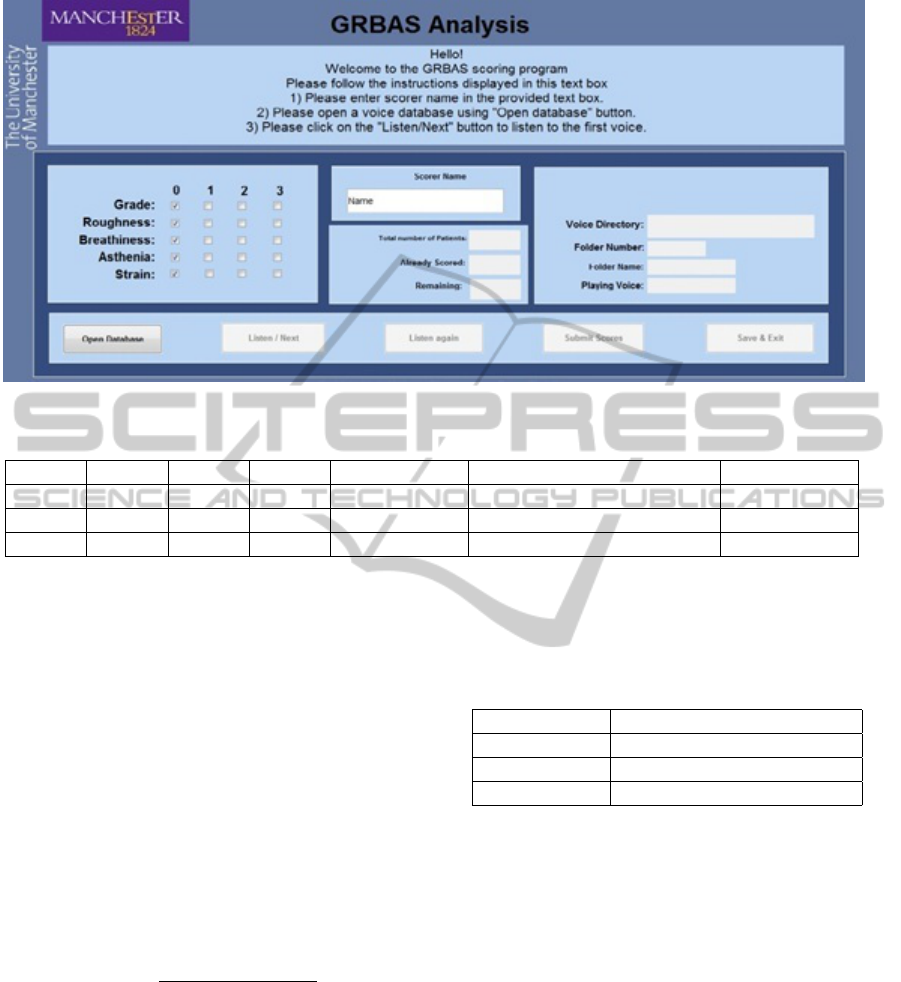
Figure 2: Screen shot of the GPSP.
Table 1: Kappa and Weighted Kappa (k
w
).
SLTs p
o
p
e
Kappa Agreement Weighted Kappa (k
w
) Agreement
1 & 2 0.64 0.48 0.316 Fair 0.311 Fair
2 & 3 0.63 0.50 0.327 Fair 0.317 Fair
1 & 3 0.68 0.38 0.483 Moderate 0.603 Moderate
weighted Kappa takes into account the degree of dis-
agreement. In this application, discrepancy between
scores 0 and 2, for example, is more serious than the
difference between 0 and 1 or between 1 and 2, and
weighted Kappa takes this into account. With lin-
early weighted Kappa (k
w
), the disagreement between
0 and 2 may be weighted twice that between 0 and 1,
1 and 2, or 2 and 3. The discrepancy between 0 and
3 may be weighted three times that between 0 and 1.
Equation (3) is a formula for linearly weighted Kappa
(k
w
), where p
oij
is the proportion of subjects that are
scored i by scorer A and j by scorer B; p
eij
is the prob-
ability of scorer A scoring i while scorer B scores j,
for the observed distribution of scores by each scorer,
but with no correlation between scorers.
kw = 1 −
∑
3
i=0
∑
3
j=0
|i − j|p
oij
∑
3
i=0
∑
3
j=0
|i − j|p
eij
(3)
As results in Table 1 show, there is only fair
agreement between scorer 2 and scorers 3 and 1;
and better agreement between scorers 1 and 3. The
measured agreement between scorer 1 and scorer 3
changes significantly when Kappa is replaced by lin-
early weighted Kappa. To make the Asthenia scores
more reliable, we can take some form of mean of the
three scores. We used the arithmetic mean or average.
If the means for all scorers are the same, Pearson
correlation is a good indicator of absolute agreement.
If the means are not the same, it can be misleading
if incorrectly interpreted. Table 2 shows the mean of
Asthenia scores for each SLT.
Table 2: Mean of Asthenia Scores.
SLT Mean of Asthenia Scores
SLT 1 0.63
SLT 2 0.30
SLT 3 0.76
3 ASTHENIA PREDICTION
3.1 Feature Extraction
The beginning and end of each sustained vowel were
trimmed to remove silence. Each sustained vowel was
divided into a series of non-overlapping 22.676 ms
(1000 sample) frames sampled at 44.1 kHz. For each
frame, the energy was computed. The mean energy
per frame (MEPF), the ratio of minimum to maximum
energy per frame energy (RMMEPF) were computed.
Also the standard deviation of the frame-by-frame en-
ergy (STD EPF) was calculated. The MEPF of each
vowel was normalized by dividing by the average of
the MEPF values obtained for all ‘normal’ voices out
of the 102 examples.
SIGMAP2015-InternationalConferenceonSignalProcessingandMultimediaApplications
78
To extract the ‘low-to-high spectral (L/H) ratio’,
each analysis frame was decimated by factor of 5,
‘zero-padded’, Hamming windowed and applied to a
400 point DFT. The spectral energy below and above
a cut-off frequency of 1.5 kHz was computed for each
frame and hence a low to high spectral ratio (L/H)
was obtained for each frame. This was averaged for
the whole recording to obtain a mean value of L/H
(ML/H). Other features such as the ratio of the max-
imum to minimum value of L/H (RMML/H) and the
standard deviation of L/H (STD L/H) were computed
for each vowel. The cut-off frequency 1.5 kHz was
selected due to most voiced speech energy occurring
below twice this frequency (i.e. about 3kHz). Six fea-
tures were created for predicting an Asthenia score for
each participant. Table 3 represents the six extracted
voice features.
Table 3: Definition of six extracted voice features.
Label Feature Definition
F1 MEPF Mean Energy Per Frame
F2 RMMEPF
Ratio of Minimum to
Maximum Energy Per
Frame
F3 STD EPF
Standard Deviation of
Energy Per Frame
F4 ML/H
Mean of Low to High
Spectral Ratio
F5 RMML/H
Ratio of Minimum to
Maximum Low to High
Spectral Ratio
F6 STD L/H
Standard Deviation of Low
to High Spectral Ratio
3.2 Feature Selection Method
Feature selection methods can determine a subset of
the available features that will give the best accuracy
in predicting Asthenia. They can be used to identify
and remove unnecessary, irrelevant and redundant at-
tributes from data that do not contribute to the accu-
racy of a predictive model or even increase the error
of the prediction. Wrapper methods were used as the
feature selection method in predicting Asthenia (Yuan
et al., 1999; Kohavi and John, 1997; Langley et al.,
1994).
Wrapper methods train a new model for each pos-
sible subset of features. These methods assess subsets
of variables according to their usefulness to a given
predictor. The method conducts a search for a good
subset using the learning algorithm itself as part of
the evaluation function. ‘Wrapper’ methods are com-
putationally intensive, but usually provide the best
performing subset of features (Guyon and Elisseeff,
2003). Greedy Forward Search, Exhaustive Search
are two examples of wrapper methods (Langley et al.,
1994).
In this research, ‘Exhaustive Search’ was used.
This method is looking at every possible combination
of features to find which one gives the best result. It
is only possible to do this with a small number of fea-
tures and so some simplification of this problem must
be done. A straightforward wrapper method was de-
veloped in MATLAB to test all possible subsets of
features. With n features there are 2
n
−1 possible sub-
sets. Therefore, with 6 features, there are 63 different
feature subsets.
3.3 Prediction Models
Linear regression (MLR) and K-nearest-neighbor- re-
gression (KNNR) (Berry and Feldman, 1985; Jiang-
sheng, 2002) were used and compared for the objec-
tive prediction of Asthenia. The average of three SLTs
scores were considered as the true value of the Asthe-
nia scores. Regression was used rather than classifica-
tion in order to take account of the magnitudes of the
differences between the scores, which are significant
with GRBAS scoring.
3.3.1 Feature Scaling
To improve the performance of the prediction mod-
els, features were scaled to make the mean of each
feature equal to zero and the standard deviation equal
to 1. Refer to F
ij
as feature j for participant i. Refer
to feature F
ij
before scaling as F
ij(non-scaled)
and after
scaling as F
ij(scaled)
. Let
¯
F
j
and σ
j
denote the sample-
mean and the sample-standard-deviation respectively
of non-scaled feature j over all n participants. The
scaled version of each feature F
ij
for participant i is
then:
F
ij(scaled)
=
F
ij(non-scaled)
−
¯
F
j
σ
j
(4)
3.3.2 MLR Performance in Asthenia Prediction
To test the capability of the MLR method for Asthe-
nia prediction, and to find out which subset of features
it is the best to use, twenty ‘trials’ were carried out
whereby random selections of 80 recording examples
were used for a cross-validation (training set and vali-
dation set) procedure and the remaining 22 recordings
were used for the testing. The experiment was applied
to the database of 102 recordings. In each trial, 63 dif-
ferent subsets of features selected from the 6 features,
were taken. For each subset, the validation error was
calculated using 10 fold cross validation. The subset
ObjectiveAssessmentofAstheniausingEnergyandLow-to-HighSpectralRatio
79
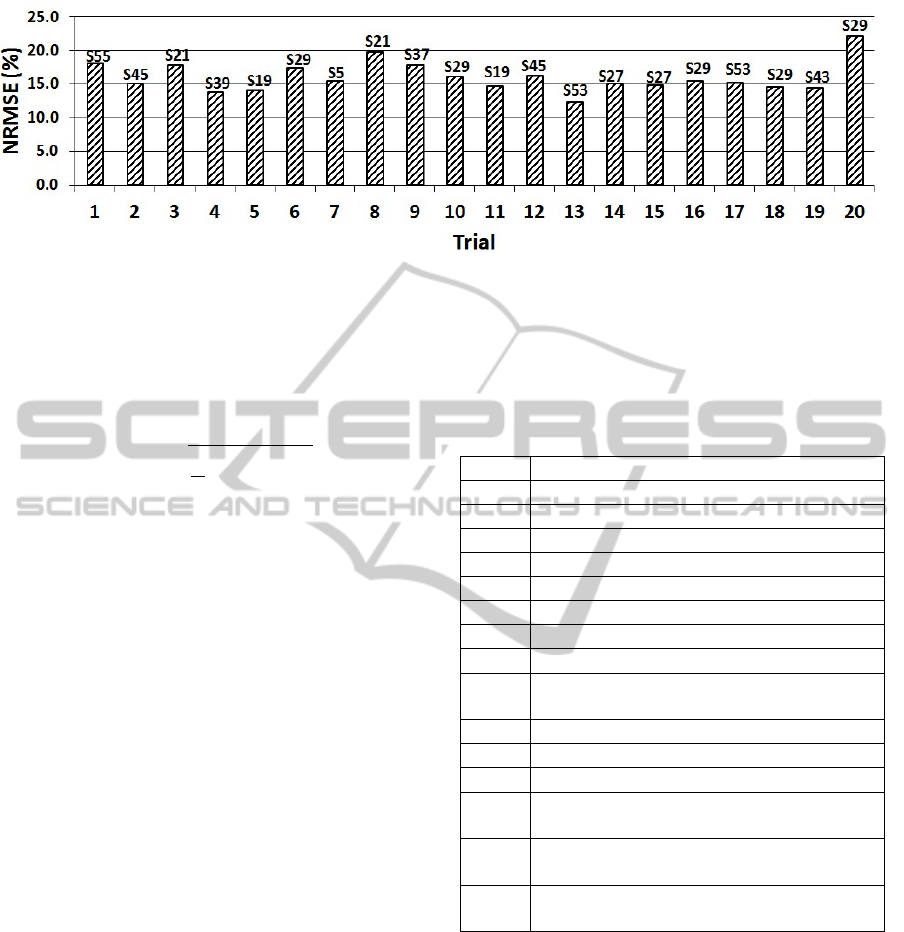
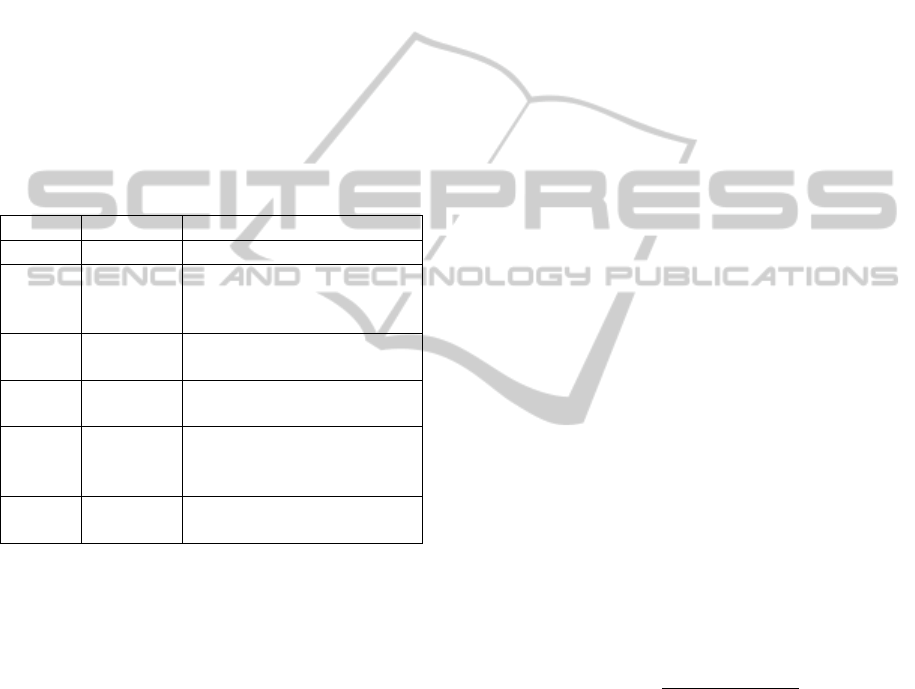
Figure 3: NRMSE for the best subset in each trial (MLR).
which gives the lowest RMSE over the validation set
was used for a training using 80 examples and testing
on 22 examples and the generalisation error was com-
puted. The RMSE between the predicted (
ˆ
Y ) and the
observed value (Y) for 22 (N) recording examples is:
RMSE =
s
1
N
N
∑
i=1
(
ˆ
Y
i
−Y
i
)
2
(5)
Table 4 defines the subset of features that are re-
ferred to in Figure 3. Figure 3 depicts the NRMSE as
generalisation error on 22 examples for the best sub-
set of feature found in each trial. S21 was flagged
as the best subset several times (i.e. five times) with
NRMSE error 17.81%, 17.87%, 14.80%, 15.22% and
22.13% respectively over 20 trials, where NRMSE is:
NRMSE = RMSE/(Asthenia
max
−Asthenia
min
)∗100
(6)
3.3.3 Best Feature Subset Selection and Optimal
K for KNNR
With KNNR, the RMSE of the regression will be af-
fected by the feature subset and value of K, which is
the number of nearest neighbors chosen. We used 10
fold cross-validation (Kohavi et al., 1995) on 80 ran-
dom examples to determine the RMSE on validation
sets for each subset for K in range of 1 to 10. In each
trial, a grid search (Bergstra and Bengio, 2012) was
used to find out the best feature subset and optimal K
with the lowest RMSE amongst 63 different subsets.
To measure the performance of the KNNR model on
unseen examples by generalisation error, the best sub-
set with the optimal K was used on 80 random train-
ing set and 22 random testing examples . This ex-
periment was carried out for 20 different trials and
the generalisation error was computed as NRMSE in
each trial. Figure 5 shows the NRMSE for the best
subset in each trial. Figure 4 illustrates the optimal
K for the best subset in each trial. S15 was flagged
several times (i.e. five times) as the best subsets over
20 trials with 18.12%, 17.95%, 17.28%, 14.91% and
16.90% NRMSE respectively.
Table 4: Definition of feature subsets referred to in Figures
3,4 and 5.
Subset Definition
S3 STD EPF, RMMEPF
S7 MEPF, STD EPF, RMMEPF
S11 RMML/H, STD EPF, RMMEPF
S13 RMML/H, MEPF, RMMEPF
S15 RMML/H, MEPF, STD EPF, RMMEPF
S19 STD L/H, STD EPF, RMMEPF
S21 STD L/H, MEPF, RMMEPF
S23 STD L/H, MEPF, STD EPF , RMMEPF
S27
STD L/H ,RMML/H, STD EPF,
RMMEPF
S35 ML/H, STD EPF, RMMEPF
S37 ML/H, EPF, RMMEPF
S39 ML/H, MEPF, STD EPF, RMMEPF
S43
ML/H, RMMML/H, STD EPF,
RMMEPF
S47
ML/H, RMML/H, MEPF, STD EPF,
RMMEPF
S61
ML/H, STD L/H, RMML/H, MEPF,
RMMEPF
4 COMPARISON BETWEEN MLR
AND KNNR
The performance of the MLR and KNN techniques
were compared for predicting Asthenia objectively.
The standard deviation of the error may be investi-
gated to estimate the stability of the models. For
MLR, the mean and standard deviation of error for the
best subsets over 20 trials are about 16.06% and 2.25
respectively with 95% confidence limits at 15.1% and
17% over 20 trials. KNN makes this mean and stan-
SIGMAP2015-InternationalConferenceonSignalProcessingandMultimediaApplications
80
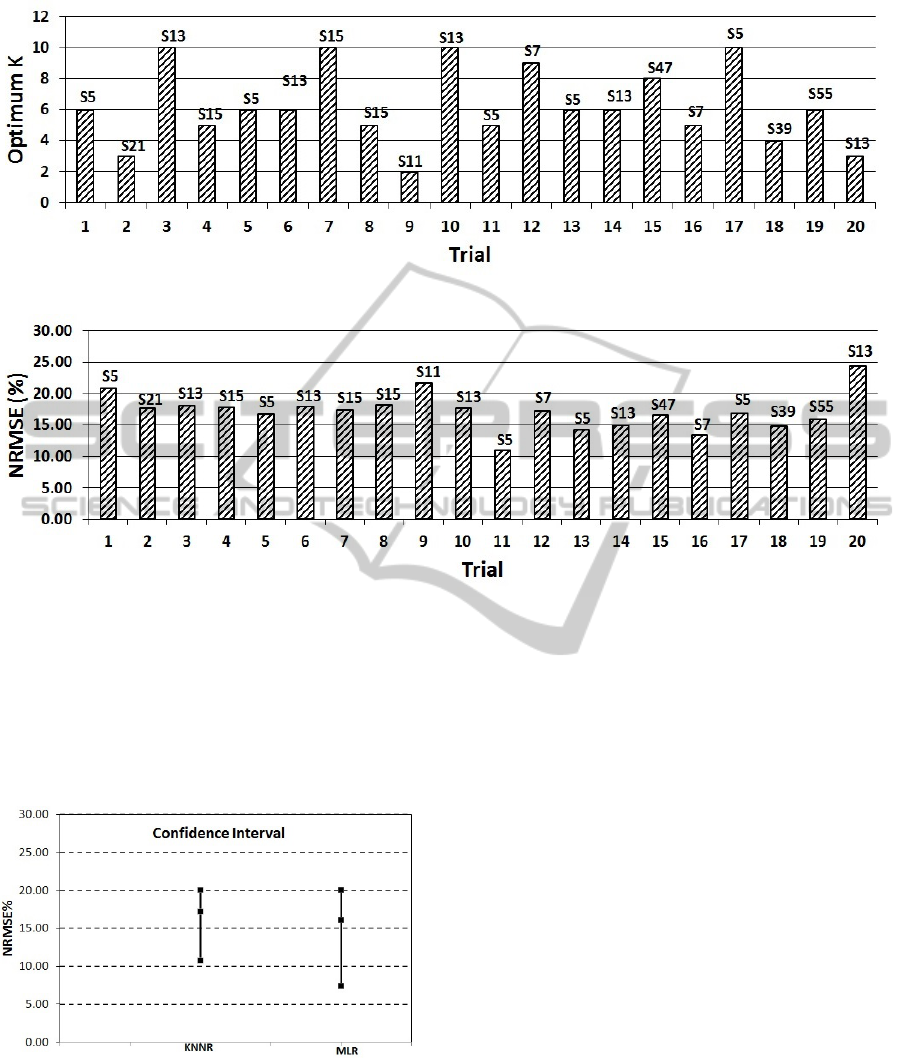
Figure 4: Best K for the best selected feature subset in each trial.
Figure 5: NRMSE for the best selected feature subset in each trial (KNNR).
dard deviation of the error 17.20% and 2.92 respec-
tively with 95% confidence limits at 15.9% and 18.5%
over 20 trials. Figure 6 displays no statistically sig-
nificant difference between the models because of the
overlap in the confidence interval of both models but
KNNR has lower standard deviation in error and the
error is more closely clustered around mean.
Figure 6: Confidence Interval.
5 OBJECTIVE SYSTEM VS
PERCEPTUAL SCORING
The objective system over 20 trials, using the best
subset of features, has an average of NRMSE around
16.06% and 17.20% by MLR and KNN respectively.
For each of these prediction models NRMSE was
computed over 22 examples. To evaluate the objec-
tive system and each scorer against the average of
three SLTs, the NRMSE was computed for the objec-
tive system and each individual SLTs who are rated
the same number of patients (22 examples) in the 20
trials. Figure 7 shows the NRMSE between the three
SLTs, the KNNR model and the MLR where average
of the 3 scorers taken as the reference. On average,
for both objective prediction models, the NRMSE
is lower than that obtained for SLT2 and SLT1 and
higher than that obtained for SLT3.
6 RELATED WORK
Objective assessment of voice has been studied ex-
tensively (Villa-Canas et al., 2013; Bhuta et al., 2004;
Yu et al., 2006; Wuyts et al., 2000). Considering the
GRBAS dimensions, Asthenia has not been as widely
covered as the others. A recent paper (Villa-Canas
et al., 2013) uses a K Nearest Neighbor classifier to
predict all parameters using spectral energy measure-
ments, cepstral coefficients, a glottal-to-noise excita-
tion ratio and other parameters. The objective scores
ObjectiveAssessmentofAstheniausingEnergyandLow-to-HighSpectralRatio
81
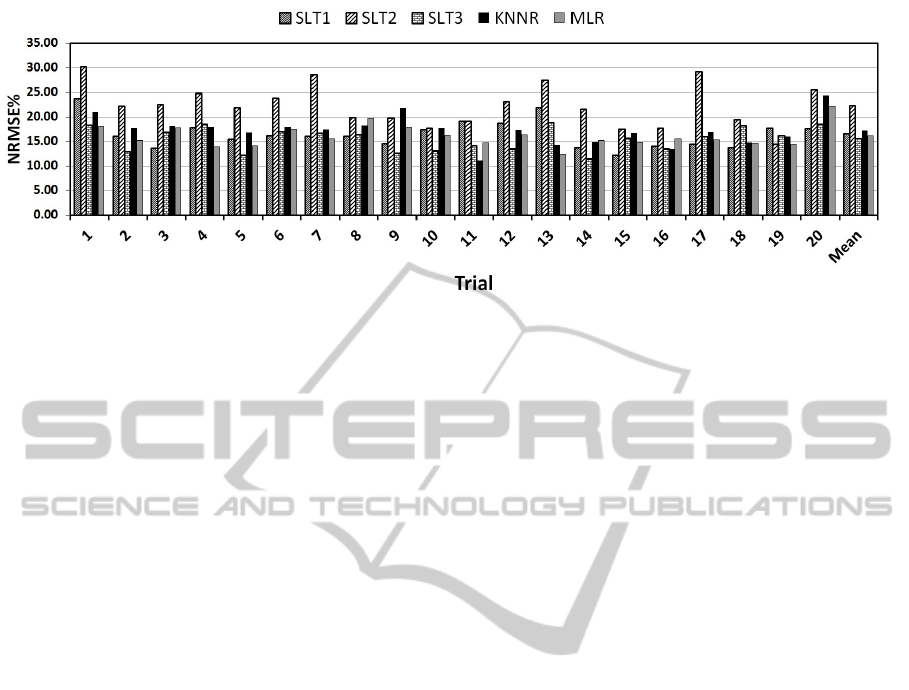
Figure 7: Comparison between NRMSE for three SLTs and objective system (KNNR and MLR).
were compared with perceptual evaluations by a sin-
gle expert at the University Poletecnica of Madrid.
Good correspondence were obtained, the best effi-
ciency, 89.3%, being obtained for Asthenia (Villa-
Canas et al., 2013) . Our work uses a different data-
base, three experienced SLT scorers and a different
feature set. Also we use regression models rather than
classification, and compare two regression models.
Regression is sensitive to the degree of disagreement
between scores where classification is concerned only
with agreement or disagreement.
7 CONCLUSIONS AND FUTURE
WORK
The proposed schemes are intended to be used for
the objective assessment of Asthenia according to the
GRBAS scale. The average of the three Asthenia
scores obtained by SLTs 1, 2 and 3 was assumed to be
the best possible estimate of the true Asthenia score
for each subject in this experiment.
The objective measurement of Asthenia was ob-
tained using multiple linear regression and K-nearest
neighbor regression by combinations of energy and
low to high spectral measurement for sustained vowel.
The use of low to high spectral ratio and energy per-
mits estimation of Asthenia without the limitations as-
sociated with traditional time-based dysphonia mea-
sures such as jitter and shimmer.
For both prediction models the best feature subset
was selected based on the lowest validation error in
each trial. Moreover, MEPF, RMMEPF, RMML/H
and the STD L/H features were found to be the
strongest contributors.
The average of generalisation error (NRMSE)
over 20 trials was measured for KNNR and MLR
which is less than 17.20% in both models.
It is now necessary to apply the approach in this
paper to the data-base used by Villa et al. (Villa-Canas
et al., 2013) to compare the values of Asthenia ob-
tained. Different methods can be proposed for the de-
cision about the true Asthenia scores which may give
different results from averaging in prediction. The
use of connected speech as well as sustained vowels
should also be introduced since this is used by SLTs.
Future studies with larger samples of voice disorder
types and severities are then needed.
ACKNOWLEDGEMENTS
This work is partly supported by EPSRC grant
AnyScale Apps EP/L000725/1. Mikel Luj
´
an is
funded by a Royal Society University Research Fel-
lowship.
REFERENCES
Awan, S. N. and Roy, N. (2006). Toward the development
of an objective index of dysphonia severity: a four-
factor acoustic model. Clinical linguistics & phonet-
ics, 20(1):35–49.
Bergstra, J. and Bengio, Y. (2012). Random search for
hyper-parameter optimization. The Journal of Ma-
chine Learning Research, 13(1):281–305.
Berry, W. D. and Feldman, S. (1985). Multiple regression
in practice. Number 50. Sage.
Bhuta, T., Patrick, L., and Garnett, J. D. (2004). Percep-
tual evaluation of voice quality and its correlation with
acoustic measurements. Journal of Voice, 18(3):299–
304.
Cohen, J. (1968). Weighted kappa: Nominal scale agree-
ment provision for scaled disagreement or partial
credit. Psychological bulletin, 70(4):213.
Guyon, I. and Elisseeff, A. (2003). An introduction to vari-
SIGMAP2015-InternationalConferenceonSignalProcessingandMultimediaApplications
82

able and feature selection. The Journal of Machine
Learning Research, 3:1157–1182.
Hirano, M. (1981). Clinical examination of voice, volume 5.
Springer New York.
Jalalinajafabadi, F., Gadepalli, C., Ascott, F., Homer, J.,
Luj
´
an, M., and Cheetham, B. (2013). Perceptual eval-
uation of voice quality and its correlation with acous-
tic measurement. In Modelling Symposium (EMS),
2013 European, pages 283–286. IEEE.
Jiangsheng, Y. (2002). Method of k-nearest neighbors. In-
stitute of Computational Linguistics, Peking Univer-
sity, China, 100871.
KayPENTAX (2008). A Division of PENTAX medical
Company. http://www.kaypentax.com. [Accessed 19-
March-2015].
Kempster, G. B., Gerratt, B. R., Abbott, K. V., Barkmeier-
Kraemer, J., and Hillman, R. E. (2009). Consensus
auditory-perceptual evaluation of voice: development
of a standardized clinical protocol. American Journal
of Speech-Language Pathology, 18(2):124–132.
Kohavi, R. et al. (1995). A study of cross-validation and
bootstrap for accuracy estimation and model selection.
In IJCAI, volume 14, pages 1137–1145.
Kohavi, R. and John, G. H. (1997). Wrappers for feature
subset selection. Artificial intelligence, 97(1):273–
324.
Langley, P. et al. (1994). Selection of relevant features
in machine learning. Defense Technical Information
Center.
Sheskin, D. J. (2003). Handbook of parametric and non-
parametric statistical procedures. crc Press.
Streiner, D. L. (1995). Learning how to differ: agreement
and reliability statistics in psychiatry. The Canadian
Journal of Psychiatry/La Revue canadienne de psychi-
atrie.
Viera, A. J., Garrett, J. M., et al. (2005). Understanding in-
terobserver agreement: the kappa statistic. Fam Med,
37(5):360–363.
Villa-Canas, T., Orozco-Arroyave, J., Arias-Londono, J.,
Vargas-Bonilla, J., and Godino-Llorente, J. (2013).
Automatic assessment of voice signals according to
the grbas scale using modulation spectra, mel fre-
quency cepstral coefficients and noise parameters.
In Image, Signal Processing, and Artificial Vision
(STSIVA), 2013 XVIII Symposium of, pages 1–5.
IEEE.
Wuyts, F. L., De Bodt, M. S., Molenberghs, G., Remacle,
M., Heylen, L., Millet, B., Van Lierde, K., Raes,
J., and Van de Heyning, P. H. (2000). The dyspho-
nia severity indexan objective measure of vocal qual-
ity based on a multiparameter approach. Journal of
Speech, Language, and Hearing Research, 43(3):796–
809.
Yu, P., Garrel, R., Nicollas, R., Ouaknine, M., and Gio-
vanni, A. (2006). Objective voice analysis in dyspho-
nic patients: new data including nonlinear measure-
ments. Folia Phoniatrica et Logopaedica, 59(1):20–
30.
Yuan, H., Tseng, S.-S., Gangshan, W., and Fuyan, Z.
(1999). A two-phase feature selection method using
both filter and wrapper. In Systems, Man, and Cyber-
netics, 1999. IEEE SMC’99 Conference Proceedings.
1999 IEEE International Conference on, volume 2,
pages 132–136. IEEE.
ObjectiveAssessmentofAstheniausingEnergyandLow-to-HighSpectralRatio
83
