
A Disciplined Innovation Approach to Health Technology Solutions
Noel Carroll
1
and Ita Richardson
1,2
1
ARCH- Applied Research for Connected Health Technology Centre, University of Limerick, Limerick, Ireland
2
Lero- The Irish Software Reseach Centre, University of Limerick, Limerick, Ireland
Keywords: Connected Health, Innovation, Healthcare Technology, Software Solutions.
Abstract: Despite the potential of innovation-driven healthcare technology services to increase the quality,
accessibility and quality of care, the realization and success of such promise has yet to be achieved. This
prompted us to explore the barriers towards success for healthcare software companies and examine what
frameworks are employed across industry to support their growth in the digital healthcare market. As part of
a three-phase study, this article reports on the first phase – to synthesize the literature on the readiness
factors for healthcare technology companies. The findings of this research will guide our second phase of
this research in surveying industry healthcare software companies. In so doing, we can establish readiness
factors for healthcare software companies with a view to offering a more structured and disciplined
approach to healthcare innovation.
1 INTRODUCTION
We often learn how small and medium-sized
enterprises (SMEs) across the national and
international service sector must consistently and
continuously innovate and adapt to ensure their
survival (Gebauer et al. 2012). It is a matter of
‘survival of the fittest’ to evolve with the dynamic
external environment. To do so successfully largely
depends on the SME’s service innovation capability
and competences to deploy resources and improve
services. This is a challenge particularly in a
healthcare context since technology advancements
continue to rapidly grow while concerns around
healthcare device safety and regulation continue to
surface and challenge innovation (Carroll and
Richardson, 2016). Thus, pertinent questions need to
be asked such as, how can an organization
continuously evolve and offer a new service to meet
healthcare needs? Where does the added capability
and competencies come from to do so? From our
experience, two key factors here are to 1) identify the
unmet healthcare needs and 2) examine how or
where the capabilities will come from to address
those needs.
We often learn about the growing success of
companies breaking new ground in healthcare
innovation and dominating market leadership
(Carroll, 2016). While, this is very much welcome
across the healthcare sector, little is known about
why companies, particularly software companies,
fail to achieve their business objectives in reaching
new markets (Kellermann and Jones, 2013). Thus,
uncovering both why companies fail and what we
can do to reduce such occurrences, drew our
attention towards the concepts of evaluation,
organizational readiness and capability maturity to
establish a more disciplined view of healthcare
technology innovation. Technology has contributed
towards a shift within healthcare practice which
highlights the growing reliance and trust we now
place on software to support healthcare decisions.
However, unlike some sectors, for example business,
failure to correctly align healthcare needs with
software requirements can have devastating
consequences on people’s health – potentially fatal.
2 TOWARDS DISCIPLINED
INNOVATION
In recent years, the concept of ‘Disciplined
Entrepreneurship
1
’ was coined at MIT and offers a
comprehensive step-by-step approach to creating
solutions. It focuses on the iterative process towards
a final solution to meet users’ needs. Aulet (2013)
1
http://disciplinedentrepreneurship.com/
Carroll N. and Richardson I.
A Disciplined Innovation Approach to Health Technology Solutions.
DOI: 10.5220/0006228703890395
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 389-395
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
389

attempts to move away from an abstract view of
entrepreneurship and proposes a toolkit to guide
innovation. This provides a rich insight on
entrepreneurship as a skillset. The toolkit provides
24 steps that is described as disciplined
entrepreneurship and is a practical step-by-step
process to channel the innovation and maximize the
chances of success and ultimate impact. Such a
formal process is considered beneficial to focus the
innovation process. We previously explored how a
similar approach could be achieved in a software
engineering and healthcare innovation context
(Carroll and Richardson, 2016). In this research we
employed Design Thinking with a view to aligning
healthcare innovation and software requirements and
address customer pain points using the Connected
Health Innovation Framework to a) support software
developers in clearly identifying healthcare
requirements and b) extend and enrich traditional
software requirements gathering techniques.
However, we have identified that there is a need to
take this a step further and move towards
establishing measures of innovation in order to
assess risk and the capability to deliver an innovative
solution within a process flow. We describe this as
‘disciplined innovation’.
3 PROBLEM STATEMENT
By services, we often refer to an intangible product,
for example, banking, consultancy, healthcare,
education and software development. Thus, the
service economy is vital across the globe. For the
purposes of this paper, we focus on healthcare and
software development as an exemplar to support
SMEs, i.e. the ‘health-tech’ market. Yet, despite the
significance placed on the service sector, there is a
lack of practical measurement or management tools
for innovation. Such a gap in literature and practice
ensures that the promise of health-tech innovation is
never fully realized across SMEs (Kohler et al.
2013). In an attempt to identify a tool to support
technology companies to guide SMEs to improve
their healthcare innovations, the authors are
continuously faced with the need to restart the
innovation evaluation process for each company.
In this paper, we propose a decision support tool
that will guide organizations to self-assess their
current organizational operations. Such a tool would
support organizational management practice. It
would provides us with a real opportunity to
establish a framework to guide organizations through
the evolutionary dimensions of healthcare
technology innovation.
In a recent article, Christensen et al. (2016)
suggest that, “business model innovation is crowded”
which is driving companies to mount both offensive
and defensive initiatives involving new business
models. Identifying innovation attributes allows us to
have greater control of the innovation flow process
and develop predictable business models to drive
decision-making tasks, measured performance and
accommodate for an efficient innovation process
flow. This becomes the primary motivation to
introduce a ‘disciplined innovation’ model.
4 HEALTHCARE INNOVATION
CAPABILITIES
Healthcare service environments become
increasingly complex when technology is
implemented to execute specific clinical, technical
and business processes to deliver care. This
ultimately adds to the complexity of a service
environment, making it one of the most difficult
environments in which to examine and manage
service capabilities. Capabilities are complex,
structured, and multi-dimensional. They may be
described as fundamental determinants resource
utilization to support and sustain organizational
performance (Teece, 2009). Managing process
maturity has been well documented throughout the
business and IT literature. Little research in this area
is carried out within a health-tech domain.
In IT management, maturity models play an
important and influential role in organizational
change (Becker et al., 2009). The availability of
service and innovation capabilities has motivated us
to review how we conceptualize the health-tech
service environment. The success of innovation often
relies on a number of contributing factors. For
example, according to Birkinshaw et al. (2011, p. 3)
the following “conditions” contribute towards
sustained innovation: (1) shared understanding:
cultural understanding of organizational behaviour;
(2) alignment: aligning systems and processes to
achieve desired performance metrics; (3) tools:
training, concepts, and techniques to innovate; (4)
diversity: optimizing external influences and insights
to offer solutions within a particular domain; (5)
interaction: establishing platforms to exchange ideas
and build networks; and (6) slack: providing
opportunities to access additional resources to
develop ideas. These conditions contribute towards
organizations overall competencies and capabilities.
HEALTHINF 2017 - 10th International Conference on Health Informatics
390

5 CAPABILITY MATURITY
MODELS
The ultimate goal of an organizational capability is
to contribute towards some form of value, e.g.
improved healthcare and increased profits. There are
a very large number of variables that are dependent
on the context and industry which determine the
important role capabilities play in value creation. At
an abstract level we may identify the attributes of a
capability to include (Carroll and Helfert, 2015)
value creation, outcome focused, measurable, and
maturity driven process. Within an innovation
environment, capabilities need to be dynamic.
Dynamic capabilities are considered the source of
competitive advantage. Teece and Pisano (1994)
identify two key aspects in harnessing competitive
advantage through dynamic capabilities that may
apply to a service innovation environment:
(1) The shifting character of the environment, e.g.
healthcare needs;
(2) The importance of strategic management in
agility, adaptability and reconfiguring internal
resources to meet external demands.
Winter (2003, pp. 4-5) suggests, “dynamic
capabilities typically involve long-term commitments
to specialised resources […] [and] […] there must
be an ecological demand for the costs of the
capability and the use that is actually made for it”.
Managing dynamic capabilities requires some form
of structure and models – for example, the capability
maturity model (CMM) (Paulk, 1995). The CMM
assumes progress is made in distinct stages and
capture capability maturity at a given time (moving
through five progressive stages - initial, repeatable,
defined, managed, optimized).
The results of this assessment process supports
the organization to position themselves against
defined best practices while identifying areas of
weakness to drive change (Becker et al., 2009;
Carroll and Helfert, 2015). However, existing
maturity models tend to focus on large organizations
(Blommerde and Lynch, 2016, p.2) and are “too
broad to account for the specificities of service SMEs
and fail to reflect their unique characteristics”. We
set out to address this gap in a health-tech context.
5.1 Health-tech Innovation
Focusing on singular innovation is considered a
thing of the past, i.e. developing one solution and
forever reaping the rewards. Organizations must
continuously innovate and demonstrate their
dynamic capabilities to execute effective innovation
capability (Blommerde and Lynch, 2016).
Blommerde and Lynch (2016, p.2) suggest, “SMEs
are unaware of their service innovation capability or
how to improve their innovative maturity mode”.
Thus, some form of innovation measurement is
required to support SMEs.
Blommerde and Lynch (2016) present the key
dimensions of service innovation capability which
link to all five stages of capability maturity model
using a ‘Service Innovation Capability Maturity
Index’, namely focusing on 1) user involvement; 2)
knowledge management; 3) strategizing and 4)
networking. In addition, and with a view to focusing
on the measurement of innovation, Kohler et al.
(2013) introduce a Service Innovation Model that
comprises of four layers. From their description, they
explain that the top layer (innovation capabilities) is
connected with service innovation capability
indicators, which are captured in the second layer.
Each capability is associated with an indicator that
quantitatively captures the implementation of the
innovation capability in the company.
Performance is a key factor in innovation and
new terms have been introduced over the last decade
such as ‘disruptive innovation’. While the concept of
disruptive innovation stems new terms such as ‘value
network’ which may be described as “the context
within which a firm identifies and responds to
customers’ needs, solves problems, procures input,
reacts to competitors and strives for profit”
(Christensen, 1997; p. 31), we need a systematic
approach to manage the innovation process.
In the Service Innovation Model, the indicators
are a core focus for the assessment and monitoring of
the service innovation capabilities. The indicators are
described by Kohler et al. (2013; p. 1350) as being
quantitative representation of the innovation
capabilities. The indicators are connected to a set of
asset categories within sets of assets and assessed on
a numerical scale. These assets are categorized into
assets, i.e. human, financial, physical, intellectual
property rights, information and information
technology, and relationship assets.
There is also a
similar outlook on the dynamic nature of innovation.
For example, den Hertog et al. (2010) suggests there
are dynamic service innovation capabilities that
successful service innovators outperform their
competitors in some of the following:
1. Signaling user needs and technological
options;
2. Conceptualizing;
3. (Un)bundling;
4. Coproducing and orchestrating;
A Disciplined Innovation Approach to Health Technology Solutions
391

5. Scaling and stretching.
Thus, we have identified that there is a natural
evolutionary process in the innovation process. This
process requires an organization to move between
specific maturity stages of innovation. Maturity
phases are well documented throughout the literature
in CMM but may need to be tailored within an
innovation context and more specifically, within a
health-tech context. For example, Carroll and Helfert
(2015) explain how the traditional view of the
organizational environment raises concerns
regarding the mismatch in the methods used to assess
business value and understanding service process
maturity. They demonstrate this by unpacking the
nature of service capabilities that allows us to
understand the primary components of value co-
creation and their contribution towards service
maturity within an innovation environment to access
organizational readiness. This offers a suitable lens
to view a disciplined approach to innovation that can
be easily adopted by SMEs in health-tech. We also
need to examine how organizational readiness aligns
with innovation capabilities.
5.2 Organizational Readiness
Throughout the literature, organizational readiness is
often associated with organizational change
management (OCM) (Armenakis et al. 1993;
Weiner, 2009). Change is a critical factor for
organizational readiness and is a multi-level, multi-
faceted construct which healthcare technologies
often face to introduce technology innovation. In
most cases, such change refers to organizational
members’ shared resolve to commit towards a
change in practice and a collective ability to improve
organizational performance. Thus, organizational
readiness for change varies as a function of how
much organizational members value the change, e.g.
within a hospital context.
Value of change must be weighted up against the
risk (e.g. cost and investment of resources)
associated with innovation. According to Weiner
(2009) there are three key determinants of change
implementation capability: task demands, resource
availability, and situational factors. We argue that
innovation capabilities are a fourth key determinant
of organizational readiness – which needs to be
calculated to assess the impact of innovation on
organizational readiness. We explain that innovation
is the process of introducing new ideas, devices, or
methods to bring about some change.
We can begin to uncover the key enablers of
innovation by taking a holistic view of change and
integrate this with business activity rather than
isolated processes. This enables us to develop an
innovation model and identify the guiding principles
that are grounded in organizational experience –
documented throughout literature (phase 1 of our
research, as presented in this paper) and captured by
surveying industry experiences (phase 2 of our
research, future work). Weiner (2009) describes how
organizational readiness is “considered a critical
precursor to the successful implementation of
complex changes in healthcare settings”. Weiner
also cautions “most publicly available instruments
for measuring organizational readiness for change
exhibit limited evidence of reliability or validity” –
hence the motivation for this research.
In the case of healthcare software companies,
innovation drives organizational changes to meet
new market demands. To ensure that innovation can
be successful, metrics must be established to drive
such change. Thus, OCM may be described as an
approach to transition an organization from their
current state to a new desired state. This involves the
integration and alignment of people, processes,
culture and strategy to innovate.
Before OCM can be successfully implemented,
managers must clearly evaluate readiness for change.
Armenakis et al. (1993) describes readiness in terms
of the organizational members’ beliefs, attitudes, and
intentions. Thus, there are critical elements of
change agents and social dynamics that influence
organizational readiness process which may
contribute towards the success of healthcare software
innovation. Identifying and measuring these
elements provides a benchmark on the current
organizational state compares with their ideal state to
derisk healthcare software innovation. We capture all
of these factors of CMM and OCM to present our
Disciplined Innovation Model for health-tech SMEs.
6 DISCIPLINED INNOVATION
Migrating from the current state to the future state of
an organization requires a number of key stages to
embrace an innovation culture to drive a specific
strategy and improve their competitiveness. This
enables organizational performance to achieve the
desired business goals. Therefore, innovation is not a
soft or vague construct, but rather, a critical process
to drive organizational performance. Why then is the
process of innovation less defined in terms of
organizational readiness and process flow
measurement? Where are the formal process models
to guide SMEs through the innovation process to
HEALTHINF 2017 - 10th International Conference on Health Informatics
392
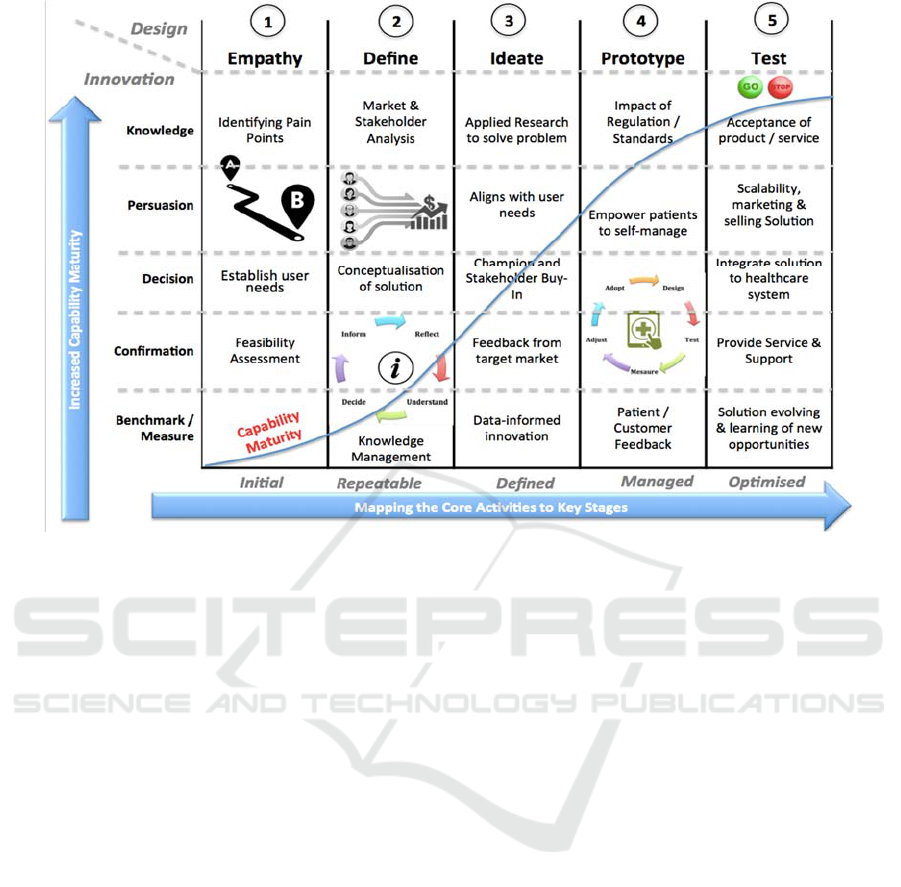
Figure 1: Disciplined Innovation Model.
derisk health-tech initiatives? To begin to address
such questions, we need to ask: Why does a company
need to build a new solution, evolve an existing
solution to maximize performance? How does a
strategy cater for such change? What specific
function(s) of the organization must change to
ensure innovation is successful? Are there any
specific guiding principles to derisk the innovation
process?
Innovation is often linked with creativity and the
ability to design solutions for unmet needs in the
marketplace. However, it remains unclear whether
we can measure innovativeness within organizational
readiness. Some attempts were made to measure
innovation, open innovation and technological
diffusion. For example, Jalles (2010) examines
alternative variables such as technological progress
(using patents and a Intellectual Property Rights
Index) to explain different growth rates of income. In
addition, Narayana (2005) suggests the need to
measures innovation using a CMM to determine a
particular strategic route and whether organizations
need to learn of the innovation management process.
6.1 Disciplined Innovation Model
Figure 1 illustrates the initial Disciplined Innovation
Model. It is influenced by:
1. The key phases of innovation: knowledge,
persuasion, decision, and conformation;
2. Design Thinking stages: empathy, define,
ideate, prototype, and test;
3. CMM stages: initial, repeatable, defined,
managed, and optimized.
We also include the need to benchmark each
phase to measure the capability maturity as a
solution matures through each stage. This captures
the essence of our initial development of the
Disciplined Innovation Model and we have identified
the need to establish specific metrics for each stage
of the model. As the performance demanded by the
customers of a value network increases over time so
does the performance provided within a
technological paradigm. Within a healthcare
technology market, this could include a new set of
performance value attributes that are now more
relevant than the current paradigm to address
healthcare needs.
While there is a strong body of knowledge on
innovation as a method of competitive differentiation
and as a way to create customer value, less attention
has been devoted to developing a measure of
innovation (Dobni, 2008). Dobni (2008) identifies
innovation culture as an important factor to measure
and identifies seven factors: innovation propensity,
organizational constituency, organizational learning,
creativity and empowerment, market orientation,
A Disciplined Innovation Approach to Health Technology Solutions
393

value orientation, and implementation context.
However, more emphasis needs to be placed on the
innovation flow process to support how we can
support the innovation process.
7 DISCUSSION & CONCLUSION
By embedding data analytics into innovation,
organizations can unlock new opportunities if guided
through a disciplined process. In healthcare, this can
build empathy for users and pave the way to
improved experiences to deliver truly user-centered
services and improved connectivity of services. We
identify that despite the potential of innovation-
driven healthcare technology services to increase the
quality, accessibility and quality of care, the
realization and success of such promise has yet to be
achieved.
To address this, we present the initial Disciplined
Innovation Model as a means to establish a self-
assessment toolkit for SMEs to support the
advancement of healthcare technology innovations
and determine whether they are ready for scaling up
their services and targeting innovation opportunities.
We also identify the need to evaluate healthcare
innovation from a healthcare practitioners
perspective (O’Leary et al. 2014) as part of our
future research.
While we introduce the initial version of this
model, as part of our future research we plan to build
on this by identifying specific metrics through
industry collaboration and piloting the model
through an iterative proves across a number of
health-tech SMEs. We anticipate that this model
could be tailored to fit other sectors to support SMEs
though a disciplined innovation process. We will
firstly focus on validating this work with health-tech
SME’s.
ACKNOWLEDGEMENTS
This work was supported, in part, by ARCH -
Applied Research for Connected Health Technology
Centre (www.arch.ie), an initiative jointly funded by
Enterprise Ireland and the IDA and Science
Foundation Ireland (SFI) Industry Fellowship Grant
Number 14/IF/2530.
REFERENCES
Armenakis, A. A., Harris, S. G., & Mossholder, K. W.
(1993). Creating readiness for organizational
change. Human relations, 46(6), 681-703.
Aulet, B. (2013). Disciplined entrepreneurship: 24 steps to
a successful startup. John Wiley & Sons.
Becker, J., Knackstedt, R., & Pöppelbuß, D. W. I. J.
(2009). Developing maturity models for IT
management. Business & Information Systems
Engineering, 1(3), 213-222.
Birkinshaw, J., Bouquet, C. and Barsoux, J.L. (2011), “The
5 myths of innovation”, MIT Sloan Management
Review, Vol. 52 No. 2, pp. 43-50.
Blommerde, T., & Lynch, P. (2016). A Maturity Matrix for
Assessing Service Innovation Capability. In: Irish
Academy of Management Conference 2016, 31 August
- 2 September, UCD, Dublin.
Carroll, N. (2016). Key Success Factors for Smart and
Connected Health Software Solutions, Computer, Vol.
49, No. 11, pp. 32-38.
Carroll, N., & Helfert, M. (2015). Service capabilities
within open innovation: Revisiting the applicability of
capability maturity models. Journal of Enterprise
Information Management, 28(2), 275-303.
Carroll, N., & Richardson, I. (2016). Software-as-a-
Medical Device: Demystifying Connected Health
Regulations. Journal of Systems and Information
Technology, 18(2), pp.186-215.
Christensen, C.M. (1997). The Innovators Dilemma: when
new technologies cause great firms to fail, Harvard
Business School Press, Boston, Massachusetts.
Christensen, C.M., Bartman, T., van Bever, D., Strategy,
D. and Strategy, E., (2016). The Hard Truth About
Business Model Innovation. MIT Sloan: Fall, Research
Feature September 13.
den Hertog, P., van der Aa, W., & de Jong, M. W. (2010).
Capabilities for managing service innovation: towards
a conceptual framework. Journal of Service
Management, 21(4), 490-514.
Dobni, C. B. (2008). Measuring innovation culture in
organizations: The development of a generalized
innovation culture construct using exploratory factor
analysis. European Journal of Innovation Management,
11(4), 539-559.
Gebauer, H., Paiola, M. and Edvardsson, B. (2012) 'A
capability perspective on service business development
in small and medium-sized suppliers', Scandinavian
Journal of Management, Vol. 28, No. 4, pp. 321-339.
Jalles, J. T. (2010). How to measure innovation? New
evidence of the technology–growth linkage. Research
in Economics, 64(2), 81-96.
Kellermann, A. L., & Jones, S. S. (2013). What it will take
to achieve the as-yet-unfulfilled promises of health
information technology. Health Affairs, 32(1), 63-68.
Chicago.
Kohler, M., Feldmann, N., Habryn, F. and Satzger, G.
(2013) 'Service Innovation Analytics: Towards
Assessment and Monitoring of Innovation Capabilities
in Service Firms', 46th International Conference on
HEALTHINF 2017 - 10th International Conference on Health Informatics
394

System Sciences (HICSS), 7-10 January, Hawaii.
O'Leary, P., Carroll, N., & Richardson, I. (2014). The
Practitioner's Perspective on Clinical Pathway Support
Systems. In IEEE International Conference
on Healthcare Informatics (ICHI), (pp. 194-201).
IEEE.
Paulk, M. C. (1995). The capability maturity model:
Guidelines for improving the software process.
Addison-Wesley Professional.
Narayana, M. G. P. L. (2005). A framework approach to
measure innovation maturity. In Proceedings. 2005
IEEE International Engineering Management
Conference, 2005. (Vol. 2, pp. 765-769). IEEE.
Teece, D.J. (2009), Dynamic Capabilities and Strategic
Management: Organizing for Innovation and Growth,
Oxford University Press.
Weiner, B.J., (2009). A theory of organizational readiness
for change. Implementation Science, 4(1), p.1.
Vancouver.
Winter, S.G. (2003), “Understanding dynamic
capabilities”, Strategic Management Journal, Vol. 24
No. 10, pp. 991-995.
A Disciplined Innovation Approach to Health Technology Solutions
395
