
Making Environments Work for People
A Novel Approach towards Personal Lifestyle Management Informatics
Eleni Kaldoudi
School of Medicine, Democritus University of Thrace, Dragana, Alexandroupoli, Greece
Keywords: eHealth, Personal Health Systems, Healthy Behaviour, Lifestyle Related Disease, Self-engagement,
Self-management.
Abstract: This paper introduces a new paradigm for personalized systems used by the citizen for self-management of
health and disease: using smart technologies to exploit the health potential of surrounding environments and
to support the citizen in decisions related to a healthy lifestyle. This approach proposes meshing the
citizen’s specific needs for healthier behaviours with what is available to meet these needs in the
surrounding environment. Rather than focusing on health monitoring alone, the aim should be to create a
healthy digital envelope – a Healthy Place – around the citizen as they move through their everyday lives.
The implementation of this approach needs to integrate existing systems for health assessment and
environmental predictions; collect personal private data from mobile personal sensors and public data on
health content of the environment; design dynamic testable models of behaviour change, that situate the
individual within their environment; develop advanced analytics for context understanding and situational
awareness that will couple the current goals of the person with what his or her environment can offer; and
create personalized decision support services for behaviour change that exploit the current match between a
person’s needs and the opportunities offered by his or her environment.
1 INTRODUCTION
Information and communication technologies have
conventionally been used to support disease
management. A second generation of interventions
addresses personal patient informatics, building the
‘quantified self’ to increase self-knowledge and
autonomy via (large scale) personal data collection.
The current trend is for personal devices and
applications whose primary purpose is less to
enlighten users with information than to urge them
to change (Singer, 2015). However, broadcasting
generic health messages (e.g. ‘do this, don’t do that’)
has relatively modest effects unless the
context/environment makes the advocated changes
very easy to carry out. Technology today cannot
significantly alter physical environments in this
respect, but it can alter something equally or even
more important: the perceived environment.
In this paper, we propose an innovative
approach of meshing the citizen’s specific needs and
goals for healthier behaviours with what is available
to meet these needs in the surrounding environment.
Rather than focusing on health monitoring alone or
individual medical and behaviour change plans, the
proposed approach aims to create a healthy digital
envelope – a Healthy Place – around the citizens as
they move through their everyday lives.
2 BACKGROUND
Lifestyle-related diseases are defined as non-
communicable diseases and are caused by non-
physiological lifestyle factors such as unhealthy diet,
physical inactivity, tobacco use, excessive use of
alcohol and psychosocial factors e.g. chronic stress
and depression, are leading causes of death globally.
Chronic non-communicable diseases such as
cardiovascular disease, cancer, diabetes and chronic
respiratory disease, were responsible for 36 million
deaths (67% of all deaths) in a single year (WHO,
2010). All these diseases are profoundly impacted
by lifestyle options including dietary intake,
exercise, stress, sleep, and use of alcohol.
Lifestyle changes in these patients can prevent
the progress of the disease more successfully than
418
Kaldoudi E.
Making Environments Work for People - A Novel Approach towards Personal Lifestyle Management Informatics.
DOI: 10.5220/0006235904180423
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 418-423
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

any drug treatment (Spruijt-Metz, 2014; Wilson,
2014; Williamson, 2005; Li, 2014)
During the last decade, different forms of health
care delivery have also been considered, based on
the specific needs of patients with chronic diseases,
such as patient empowerment. Environmental
information as provided by smart cities
infrastructure has been proposed to augment
personal health applications and help citizens choose
wisely their whereabouts in the urban environment
(Solanas, 2014). Furthermore, the WHO, among
others, has promoted the idea of preventing disease
through healthy environments (Pruss-Ustun, 2006).
To ensure sustainable healthy behavioural change,
we must foster and promote environments that can
support people in healthier lifestyle habits.
As it is difficult to radically change the
environments of developed societies, we propose to
change how the environment is perceived. This will
be achieved by highlighting, on an individual basis,
those aspects of the environment that are most
conducive to encouraging and maintaining
personalized healthy behaviours. Thus, the aim is to
‘change’ the place around the citizen into a
‘perceived’ Healthy Place. For the rest of this
document, therefore, the term Healthy Place is used
to refer to a place whose health-related aspects have
been highlighted by the proposed technological
framework.
3 HEALTHY PLACES CONCEPT
For any place of everyday life to turn into a
perceived Healthy Place, its objects and concepts
must be semantically described and linked to healthy
habits and values, thus creating an augmented
environment for individuals to manage health,
lifestyle and disease. To be relevant, this needs to
relate to the individual’s every day, real world
context and be coupled to the personal lifestyle and
the medical/behavioural goals of the individual in
question.
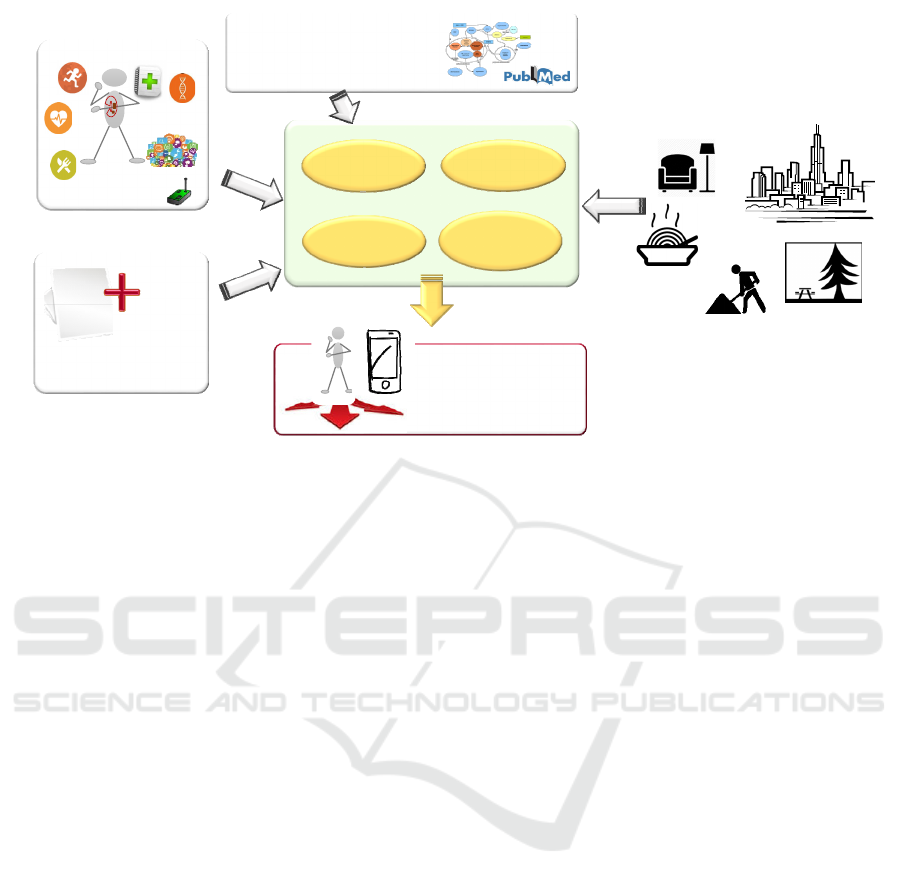
There are three different types of data that
pertain to this approach: private personal data,
public data on the ambient surroundings, and health
related scientific evidence including predictive
models and risk assessment (Figure 1).
Private, individual-level data includes: (a)
personal information on health issues, e.g.
demographics, allergies, risk factors, etc. as
available from a personal health record; (b) real-time
information on physical activity, location, and
dietary choices; (c) lifestyle related information
from the person’s social media presence, including
attitudes, intention and relations to the community;
and (d) via analysis of the above, information on the
motivational and emotional state of the person.
Public data includes data on healthy aspects of
resources and activities of a place, incorporating
commerce, retail, leisure, workplace and community
aspects, or the ambient environment. Aggregating
public data on life contexts can be driven by
stakeholders in commerce, retail, leisure, workplace,
community who will publish key data; it can also
use participatory sensing approaches.
Major lifestyle related contexts include:
Food: the ingredients and calorific content of
food items are an obvious and important source
of data when considering one’s health. This data
can be used in relation to: managing weight,
ensuring an appropriate balance of nutrients is
consumed and coping with food allergies.
Additional information includes meal
preparation processes, e.g. the type of fat used
for frying, whether menu items have been in the
proximity of nuts and other common allergens.
Recreational activities: rich description of
activities in terms of their work load, difficulty,
special requirements, indications and contra-
indications for the healthy person at different
ages and capacities and when suffering from
different health conditions and disease.
Public Transport: with the emergence of ‘Smart
Cities’ and public Open Data there is a growing
tendency for data concerned with transport
routes, stop and station locations, timetables and
vehicle locations to be publicly available. This
data can be used to help with maintaining a
certain level of exercise and energy
consumption.
Ambient environment: temperature,
meteorological conditions, noise level, air
pollution, airborne allergens, etc. pollen counts,
as well as meteorological conditions can affect
health.
Ground medical evidence and health prediction
models can serve as the basis on which the current
environment is analysed for the opportunities it
offers and threats it presents for the individual. The
goal is to dynamically highlight the most suitable
attribute of each environment for the individual and
deter from any threats this environment may hold,
based on the needs of each person. Thus, the same
environment is presented differently according to the
health condition and requirements of each
individual.
Making Environments Work for People - A Novel Approach towards Personal Lifestyle Management Informatics
419
medicalevidence&
healthpredictivemodels
personal
healthdata
healthcontent
oftheenvironment
via
lif econtextdescriptions&
participatorysensing
quantifiedself
mindchange
model
decision
support
analytics
data
interlinking
healthylifestyle
virtualcoach
Figure 1: Data aggregation to realize the concept of a Healthy Place.
The coupling of public and personal data
projected against a behaviour and behaviour change
model to create personalized recommendation
services for the citizen via a personal application.
This can virtually coach individuals by supporting:
(a) advanced behaviour and environment awareness;
(b) self-monitoring, goal setting, and action
planning; and (c) motivational and sustained
behaviour change. Thus, individuals can explore
personal motives, competences, life goals,
preferences, social connections, and other internally-
driven motivational elements around physical
activity, healthy eating and healthy behaviours in
general. These can be coupled with opportunities
offered by the current environment. Social
intelligence tools can also be used to tap into
participants’ sense of volition and ownership (as
opposed to merely external pressure), confidence
and competence (as opposed to self-perceptions of
unpreparedness and even failure), and positive social
support for their activities and goals.
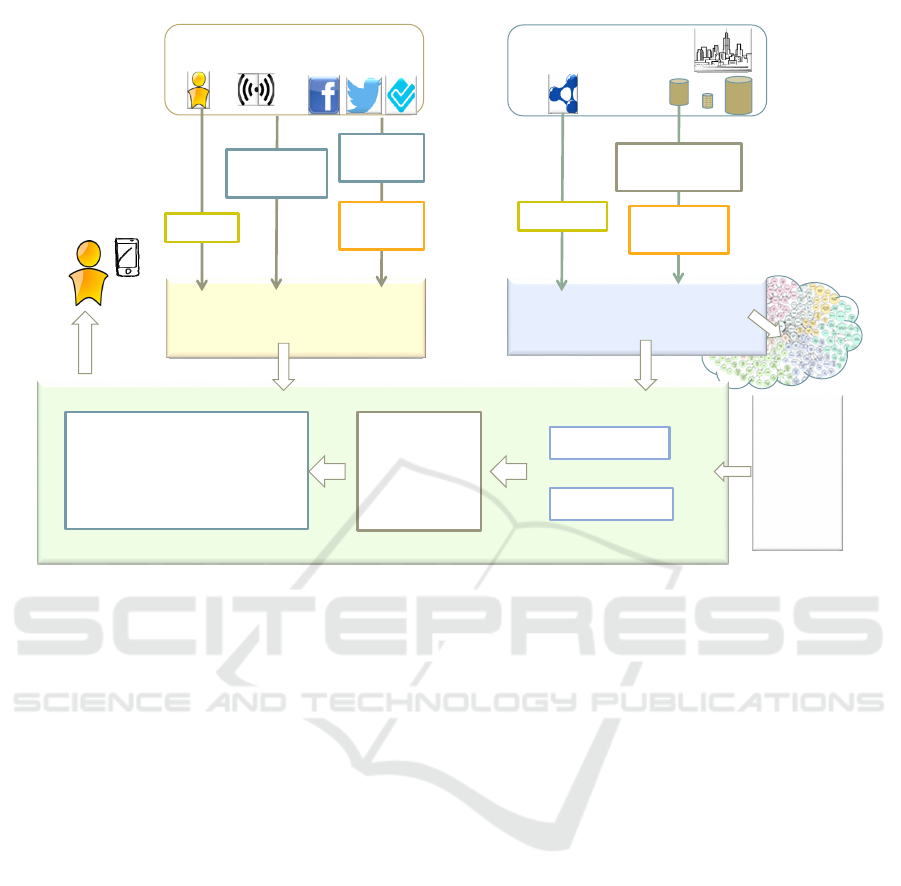
4 OPEN RESEARCH ISSUES
The proposed concept of combining health related
content with personal information to create an
optimum perceived Healthy Place for each
individual can be approached by a modular
architecture as shown in Figure 2.
Starting from top to bottom, data and knowledge
acquisition components acquire personal and public
data. Personal data is nowadays readily available via
a variety of commercially available wearable and
other personal sensors and systems (e.g. personal
health records). However, describing the health
content of the environment may prove challenging.
Participatory sensing can be employed to exploit the
crowds and their mobile devices to harvest and
enrich the information about the environment and
living spaces (e.g. the noise level and the
temperature of a place, photos of food items for
optical nutritional recognition, etc.).
Information a person creates on social networks
may prove to be a significant determinant of
behaviour: We are all individuals who are
interconnected with other individuals by personal,
social, economic and workplace relationships. These
connections facilitate communication, can motivate
us to different behaviours, and have the potential to
support shifts toward healthier lifestyles. Further
research is expected to adapt and develop the
necessary natural language processing, information
retrieval and machine learning methods, combining
data mining with semantic technologies and
expertise in social media sentiment analysis.
Data enriching and interlinking is of outmost
importance to bring up rich data relationships that
would help couple personal health requirements with
the opportunities in the environment. Thus, graph
data repositories (Angles, 2012) are chosen to
establish the middle layers of the proposed
architecture: a public one for the health context of
living spaces and a private for the personal
HEALTHINF 2017 - 10th International Conference on Health Informatics
420
www,LOD
sensors
LinkedOpenData
opendata
social networks
personal,private
LinkedData
repository
LinkedOpenData
repository
dataanalysis
visualization
existing
predictive
models
privatepersonaldata
profiling
users
decisionsupportservices
‒ realbehaviour tracking
‒ goalsetting,actionplanning
‒ motivationalsustained
behaviour change
personal
application
personalized
behaviour &
behaviour
change
model
integratedservicesplatformtorealizeapersonalperceivedhealthylivingspace
dataharvesting
andenrichment
information
extraction
harvesting
sentiment
analysis
data
extraction
sensorsdata
extraction
Figure 2: Overview of an abstract framework to realize personal perceived Healthy Places.
information. Although a lot of work has been put on
releasing semantically rich Open Data,
contemporary solutions often fall short of fully
exploiting the Semantic Web’s potential (d’Aquin,
2008). This shortcoming owes mainly to a) the
shortage of adequate knowledge acquisition
mechanisms, b) the lack of an environment-based,
life and health related semantically integrated
approach and c) the slow progress concerning the
linkage of user data with the Web of Data.
Despite the proliferation of semantic web data,
most published data remains semantically poor (e.g.
XHTML, XML, CSV files). To leverage this wealth,
research should focus on developing solutions that
enable knowledge acquisition, which can be
accommodated using different approaches, such as
data and information extraction, and sentiment
analysis. Applications that are based on traditional
database modelling principles suffer from difficulty
in capturing evolution of the data model, high
software maintenance cost and low reusability. The
semantic web achieves the translation of data across
boundaries that separate different domains and
overcomes these limitations (Feigenbaum, 2007).
Further research is required to define and analyse the
model and corresponding ontology/schema to
describe health context of living spaces. This entails
detailed examination and exploitation of existing
health and life vocabularies and development of the
appropriate Linked Services and service information
(Pedrinaci, 2010).
The emergence of social web has led to the
generation of user interaction and preferences traces
that are often distributed, fragmented and detached
(Rowe, 2009). This limitation not only complicates
efforts to gather relevant user information, but also
weakens the ties between personal data and the web
of data. However, it fails to safeguard privacy, given
the potential for a determined data-gatherer to
integrate diverse data sources to form a detailed
picture of an individual’s actions and preferences.
Concerning the linkage between personal data and
the web of data further research is required to
integrate personal data and web of data through a
single services interface, while ensuring the highest
level of privacy protection for individuals.
Support for analysis and visualization of large
data sets can in principle be done by aggregation
performed in either data space (data reduction) or in
visual space (visual aggregation). Scalability is a key
challenge in visual analytics as it determines the
ability to process large datasets by means of
computational overhead as well as appropriate
rendering techniques. Often, the huge amount of
Making Environments Work for People - A Novel Approach towards Personal Lifestyle Management Informatics
421

data that must be visualized exceeds the limited
number of pixels on a display by several orders of
magnitude. Currently existing techniques typically
focus on a single given data type, e.g., time series or
text data, so further research is required to address
multiple data perspectives simultaneously.
The wealth of available personal health devices
and applications, should be amended by novel
applications tracking real-time personalized lifestyle
to deduce the person’s current real behaviour and
how much this deviates from what is a healthy
behaviour for this person (especially as specified by
the individual in terms of his or her personal
behavioural goals) and to determine mind changing
actions (i.e., behaviour change through cognitive and
emotional determinants). Novel tools are also
required to support individuals to engage with self-
monitoring, goal setting, personal projects and
coping plans. New motivational and sustained
behaviour change decision support applications
should be devised to allow individuals to explore
personal motives, competences, life goals,
preferences, social connections, and other internally-
driven motivational elements around physical
activity, healthy eating and healthy behaviours in
general.
A major enabling factor for realizing the
personal healthy space via messing public and
private health related data lies in the challenge to
preserve privacy (Vayena, 2015). Although
healthcare data are customarily anonymised to
ensure a certain level anonymity (Gkoulalas-
Divanis, 2014), they remain susceptible to threats
caused by data linkage (e.g., with publicly available
data sources) or by background knowledge. Thus,
effective measures for preserving privacy must be
developed (Viceconti, 2015). Also, patient consent
(and its revocation) is recognized as a major
limitation in broadly re-using available healthcare
datasets for novel big data analytics (Barash, 2015).
Additionally, the recent agreement on Commission’s
EU Data Protection Reform (EU Regulation
2016/679) recognizes that practices have to respect
the citizens’ rights to (1) easily access their own
data, (2) transfer data among providers; (3) have
their data deleted when no longer needed; (4) know
when their own data have been hacked. Thus, new
research is required to extend anonymization
algorithms to work on a distributed setting, where
multiple parties hold different parts of the data that
cannot or are not willing to share in raw form.
develop and validate computationally efficient
algorithms for detecting complex events in
healthcare data streams. This research should also be
complemented by novel privacy preserving consent
management mechanisms and cryptography enabled
techniques for anonymous and unlikable feedback
and reward mechanisms to return useful service
output to the citizen (e.g. a health prediction or
personal health status) or reward the citizen for
contributing personal data.
5 DISCUSSION
In a radical departure from traditional eHealth, this
paper introduces a new paradigm for personalized
systems used by the citizen for self-management of
health and disease: smart technologies based on
existing predictive systems are used to exploit the
health potential of the surrounding environment and
support the citizen in his/her decisions related to a
healthy lifestyle. To achieve this, novel research
should address the following:
integrate existing predictive systems from
different domains, namely (a) health risk
assessment models, calculating risks based on
current health condition; (b) health predictive
systems based on environmental factors; (c)
behavioural models; and (d) predictive models
of environmental parameters, e.g. weather
conditions, air pollution and noise levels;
collect personal data from mobile personal
sensors but also collect data on health content of
the environment via citizen participatory
sensing;
design dynamic testable models of behaviour
change, that situate the individual within their
environment and take full account of cognitive,
social and emotional aspects;
develop technology that allows the semantic
description of health-related aspects of an
environment as well as of health-related aspects
of a person’s behaviour;
perform advanced analytics for context
understanding and situational awareness that
will couple the current goals of the person with
what the current environment can offer; and
deploy personalized recommendation services
for behaviour change that, based on
personalized predictions, exploit the current
match between a person’s needs and the
opportunities offered by his or her environment.
The goal is to: (a) help citizens manage actively
health and eventually adopt and maintain a healthy
behaviour, and thus prevent lifestyle related
diseases; and (b) make stakeholders in food,
commerce, retail, leisure, workplace and community
level aware of the healthy (or non-healthy) aspects
of the goods, opportunities and premises they offer
HEALTHINF 2017 - 10th International Conference on Health Informatics
422

to the public and provide them with technology to
promote what is healthier for each citizen.
Health cannot be successfully promoted and
sustained by health care systems alone – these are
naturally focussed on treatment much more than
prevention. At the same time, changing
environments with health-related goals in mind is
extremely difficult – it requires political will and
sometimes costly investments; health is a goal that
needs to be balanced alongside other priorities, such
as prosperity or efficiency.
Changing citizens’ awareness of their everyday
environment, in the light of their own priorities and
goals, creates a new possibility for the prevention of
lifestyle related diseases and, indeed, for the co-
production of health and reduction of potential
chronic, life quality reducing and costly health
conditions and complications.
ACKNOWLEDGEMENTS
The concept presented in this paper was inspired
mainly by work done in the FP7-ICT project
CARRE (No. 611140), funded by the European
Commission
REFERENCES
Angles, R., 2012. A comparison of current graph database
models. In 28th International Conference on Data
Engineering Workshops (ICDEW), IEEE, 171-177.
d’Aquin, M., Motta, E., Sabou, M., Angeletou, S.,
Gridinoc. L., Lopez, V., Guidi, D., 2008. Toward a
new generation of semantic web applications. IEEE
Intelligent Systems, 23(3), 20-28.
Feigenbaum, L., Herman, I., Hongsermeier, T., Neumann,
E., Stephens, S., 2007. The semantic web in action.
Scientific American, 297(6), 90–97.
Gkoulalas-Divanis, A., Loukides, G., Sun, J., 2014.
Publishing data from electronic health records while
preserving privacy: a survey of algorithms. J Biomed
Inf, 50, 4-19.
Li, D., 2014. Effect of the vegetarian diet on non-
communicable diseases. J Sci Food Agric, 94(2), 169-
173.
Pedrinaci, C., Liu, D., Maleshkova, M., Lambert, D.,
Kopecky, J., Domingue, J., 2010. iServe: a linked
services publishing platform. In CEUR workshop
Proceedings, 596, 10.
Prüss-Üstün, A., Wolf, J., Corvalan, C., Bos, R., Neira,
M., 2006. Preventing disease through healthy
environments. World Health Organization WHO,
Geneva.
Rowe, M., 2009. Interlinking distributed social graphs. In
Linked Data on the Web Workshop, WWW2009.
Singer, N., 2015. From knowing yourself, to prodding
yourself, The New York Times, April 19, BU3.
Solanas, A., Patsakis, C., Conti, M., Vlachos, I.S., Ramos,
V., Falcone, F., Postolache, O., Perez-Martinez, P.A.,
Di Pietro, R., Perrea, D.N., Martinz-Balleste, A., 2014.
Smart Health: A Context-Aware Health Paradigm
within Smart Cities. IEEE Comm Mag, 52(8), 74-81.
Spruijt-Metz, D., O’Reilly, G.A., Cook, L., Page, K.A.
Quinn, C., 2014. Behavioral contributions to the
pathogenesis of type 2 diabetes. Curr Diab Rep,
14(4), 475.
Vayena, E., Salathe, M., Madoff, L.C., Brownstain, J.S.,
2015. Ethical challenges of big data in public health.
PLOS Comp Biol, 11(2), e1003904.
Viceconti, M., Hunter, P., Hose, R., 2015. Big data, big
knowledge: big data for personalized healthcare. IEEE
J Biomed Health Inf, 19(4), 1209-1215.
WHO, 2010. Global status report on non-communicable
Diseases.
Williamson, D.A., Stewart, T.M., 2005. Behavior and
lifestyle: approaches to treatment of obesity. J La State
Med Soc, 157(1), S50-S55.
Wilson, D.E., van Vlack, T., Schievink, B.P., Doak, E.B.,
Shane, J.S., Dean, E., 2014. Lifestyle factors in
hypertension drug research: systematic analysis of
articles in a leading Cochrane report. Int J Hypertens,
2014, 835716.
Making Environments Work for People - A Novel Approach towards Personal Lifestyle Management Informatics
423
