
Process Improvement in an Oncology Day Hospital: Design of a
Traceability and Indicator System
Eduardo Cañada
1
, Enrique Casado
1
and Ana M. Bernardos
2
1
Hospital Universitario Infanta Sofía, San Sebastián de los Reyes, Madrid, Spain
2
Universidad Politécnica de Madrid, Madrid, Spain
Keywords: Process Improvement, Traceability, Oncology Day Hospital, Information System.
Abstract: Day hospitals (DH) are organizational structures that enable the supervision of patients who must go through
diagnosis methods or treatments taking several hours, but not requiring inpatient hospitalization. Oncology
Day Hospitals (ODH) are a particularly complex subset of DH, due to the variety and type of pathologies that
are treated in them, the characteristics of cytostatic drugs, the involvement of different hospital units and
professional profiles, the number of stages of the care procedure and the cost. In this paper, we describe the
design of a traceability and indicator system for ODH, which aims at improving the performance and quality
of service, providing three-folded benefits for patients, practitioners and hospital managers. The system is
currently being tested in a public hospital in the Autonomous Community of Madrid. Their users perceive
that they have access to a much more accurate fingerprint of everyday workflow, thus facilitating the design
of improvement actions.
1 INTRODUCTION
Since their introduction in the 70s, Oncology Day
Hospitals (ODH) have played a key role in the
treatment of cancer: it is in this organizational
structure where the oncology patients receive their
chemotherapy treatment, with specifically tailored
drugs. ODH are target of continuous improvement
measurements: the disease impact in patients’ quality
of life, the nature of cytostatic drugs, the usually long
visit protocols, the number of professionals involved
in the treatment workflow and the cost of the attention
require that ODH operations are revisited and
optimized to guarantee safety, efficiency and quality
of service. For example, in the last years, a particular
effort has been done to deploy traceability systems for
cytostatic drugs over all the clinical workflow, to
provide maximum protection in drug administration.
The works of Queralt et al. (2015), Kergosien et al.
(2011) or Sini et al. (2011) focus on this issue, while
the preparation and manipulation of the drugs
themselves is also a matter of interest (Masini et al.,
2014). From a more holistic approach, some other
experiences, such as the one described by Galligioni
et al. (2009), examine the hindrances and benefits of
the use of specific tools to manage electronic
oncological patient records.
This paper describes the process improvement
analysis that has been carried out to have an accurate
fingerprint of the activity and performance of the
ODH at Hospital Universitario Infanta Sofía. Hospital
Universitario Infanta Sofía is a public hospital in the
Autonomous Community of Madrid (Spain), active
from 2008. In 2015, 35515 care sessions where
handled in its Day Hospital (SIAE, 2015); 7085 of
those were oncology sessions (approximately 20%).
As a result of the procedural analysis, a
Traceability and Indicators System (TIS) for the ODH
has been designed; it is composed by a real-time
visualization interface and a business intelligence tool
(dashboard). On one hand, the visualization interface
retrieves real-time timestamps at the different stages
of the ODH operation workflow, so it can provide
real-time data and alerts for health workers and
managers, at the same time that facilitates the
integration of information services for patients. On
the other hand, the business intelligence tool enables
the retrieval of a complete set of activity,
performance, quality of care and procedure indicators
that aims at providing information to design
continuous improvement strategies.
CaÃ
´
sada E., Casado E. and Bernardos A.
Process Improvement in an Oncology Day Hospital: Design of a Traceability and Indicator System.
DOI: 10.5220/0006278506010608
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
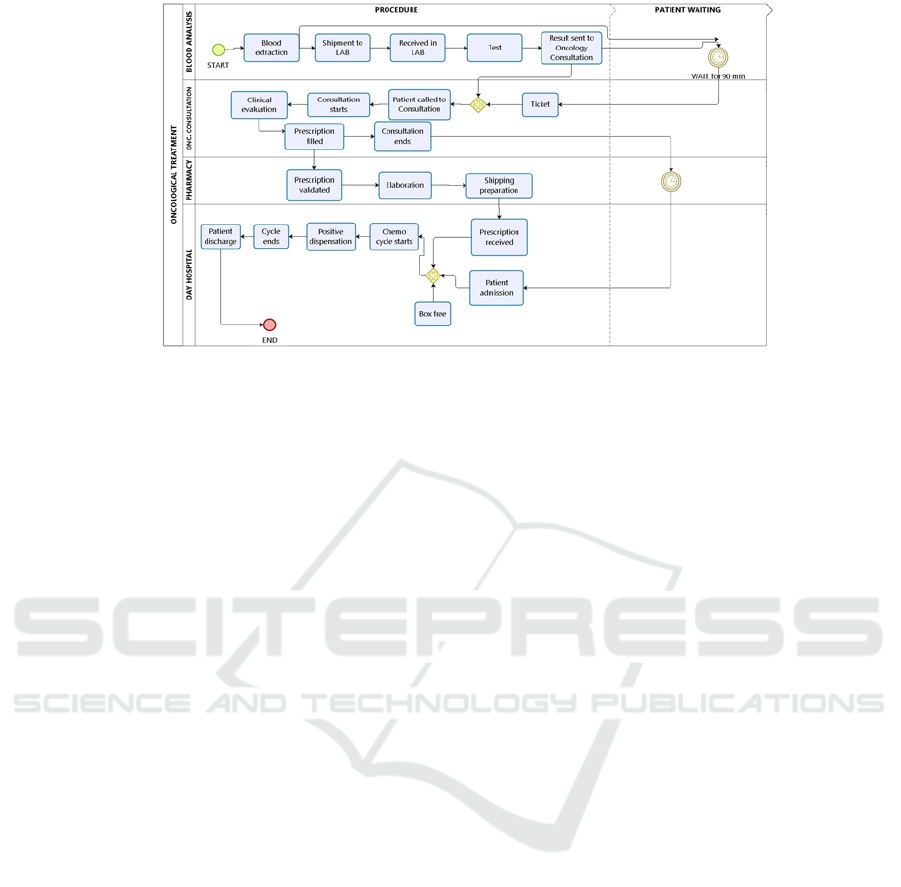
Figure 1: ODH workflow for a patient.
The TIS has been built on already available
information that was not being retrieved in an easy-
to-visualize way. The system aims at delivering three-
folded benefits: for the patient, to reduce and lighten
the time at the ODH; for the clinician, to facilitate the
retrieval of real-time information about the workload
and improved agenda management thanks to the
existence of accurate and reliable indicators; for the
manager, to facilitate the design of actions to raise of
the perceived quality of service and to handle
bottlenecks and process problems, so the impact of
the investments agenda can be better evaluated.
In this context, the paper is structured as follows.
Section II describes the operation workflow at the
ODH and the subsequent TIS’ functional and non-
functional requirements. Section III describes the
deployed architecture and the customized real-time
visualization interface. Section IV describes the
indicators. Finally, Section V concludes the work,
stating the impressions gathered about the system and
defining further steps.
2 OPERATIONAL CONTEXT
2.1 Workflow Analysis
A standard visit of a patient to the ODH is as follows:
on arrival, the patient goes directly to take the 1)
preliminary blood tests. After that, they head to the 2)
medical consultation, where the practitioner
examines the overall situation and prescribes the
cytostatic drugs. The cytostatic drugs are then 3)
prepared at the Pharmacy Service and sent to the
ODH for dispensation. When the cytostatic drugs are
prepared and delivered at ODH and the needed
resources (seat, bed, pump, etc.) are ready, the 4)
patient is admitted to the ODH for the 5) drug
administration. When the treatment is over, the
administrative staff in charge proceeds to the 6)
patient discharge, who leaves the hospital. Figure 1
summarizes the full workflow.
In practice, during all the process, it is needed to
do a follow up of the patients, personnel, resources
and drugs. This tracking involves four Hospital Units:
ODH, Laboratory, External Consultations and
Pharmacy. The professional profiles participating in
the workflow are oncologist (FAC), pharmacologists
(PHAR), health staff (NUR), administrative staff
(ADM) and ancillaries (ANC).
As our objective is to build a traceability and
indicators system (TIS) that may report a real-time
picture of the ODH operation and a full view of the
service performance, it is important to analyze which
milestones may be automatically retrieved through
the APIs provided by the commercial information
systems that are already deployed in the Hospital. In
the particular case of Hospital Universitario Infanta
Sofía, these systems include the Hospital Information
System (Selene from Siemens), the Pharmacy
Information System (FarmaTools from Dominion)
and the Laboratory Information System (LIS-
ServoLab from Siemens). Apart from those, an
Appointment and Queue Tracking System for
consulting rooms (AQ-Quenda from Plexus
Technologies) is also in use.
Table 1 summarizes all the events in the operation
workflow. As the reader will notice, there are events
that are not being registered (e.g. when the patient
enters the hospital or the NUR takes blood), and some
others that are still being registered in manual way,
thus their timestamps cannot be directly integrated
into the TIS.

2.2 System Requirements
On this workflow analysis, the functional
requirements for the TIS have been defined (i.e. what
the system has to do in practice):
Show the status (situation in the encounter
workflow and particularities) of all the
scheduled patients, both for regular visits and
ODH.
Include the non-scheduled patients that may
appear during the day.
Execute the automatic capture of information
from all the hospital IS that provide
information about the patient whereabouts and
health records.
Facilitate the input of relevant information in
manual mode, in case it is not recorded at the
HIS.
Provide user management, so managers,
clinicians, administrative staff may access to
the information that is useful for them.
Define specific rules for alerts and generate
visual feedback when these rules are not
satisfied.
Generate alert messages for patients and
clinicians to manage specific situations, both
manually and automatically.
Provide a dashboard of indicators that may
provide an overview of the activity and
resources occupancy.
Generate and submit a daily report.
Table 1: Events in the ODH workflow.
Unit Event Info. Sys.
ODH PAT enters the hospital -
ODH PAT goes to ODH services for blood
extraction.
-
ODH NUR prints tags. HIS
ODH NUR takes blood. -
ODH NUR puts blood sample in the
pneumatic tube.
-
LAB LAB receives blood sample. * HIS
LAB LAB does blood analysis. -
LAB LAB provides the report. * LIS+HIS
EXC PAT takes the turn ticket. * AQ
EXC FAC calls PAT when LAB report
ready. *
AQ+HIS
EXC FAC provides subsequent
appointments and lab requests. *
HIS
EXC FAC fills in pharmacy prescription. * PhIS
EXC FAC fills in a form at HIS, updates
the PAT record and copies the report
in an unassigned note. The note is
always assigned to protocols (colon,
pulmonary, tumor committee). *
HIS
EXC FAC finalizes consultation. * HIS
PHAR PHAR checks the prescriptions
through the IS, following a stage-gate
predefined process. *
PhIS
PHAR The treatment is verified. * PhIS
PHAR PHAR prints the Report of
Preparation to Administer. This report
is signed by NUR and PHAR and it is
taken to the clean room.
Manual
PHAR Once the drug is ready, an ANC is
called.
Manual
PHAR ANC collects preparation at FAR. Manual
ODH ODH receives preparation. Manual
ODH ADM registers the patient and prints
the identification bracelet.
HIS
ODH PAT is admitted in ODH. * HIS
ODH NUR assigns a seat. HIS
ODH The administering process starts,
guided by the pharmacy system for
secure administration. *
HIS
ODH PAT discharge. * HIS
Events with asterisk are those that can be automatically retrieved
from IS. PAT: patient. LAB: laboratory. EXC: External
Consultation. ADM: Admissions. In the very specific case of ODH,
patients go straight to the blood draw service without going through
the reception desk.
Regarding the non-functional requirements (how
the system has to be), the TIS must perform
satisfactorily with respect to:
Availability: it must be accessible and easy to
configure from any connected workplace at the
hospital, not needing any specific additional
software.
Concurrency: its performance must to be not
penalized by the simultaneous use from
different workplaces.
Security: the system must manage and control
every access and keep trace of them.
Performance: the system response must be real-
time (not above 3 seconds).
Usability: the system must be easy and
comfortable for the users. Not more than 10
minutes training should be necessary for the
users to work with the system.
2.3 Design Methodology
The methodology utilized to design the system
follows an iterative approach, in which iterations are
composed by analysis, development and testing
phases. In this case, the main users of the systems are
practitioners and managers, so their permanent
contribution on three prototyping stages that have
been necessary to come out with a first stable version
has been crucial.

3 SYSTEM ARCHITECTURE
The core of all the hospital information systems is the
HIS (Selene from Siemens), which is used in
Emergency Care, Hospitalization, External
Consultations and Day Hospital. Through it, any
patient appointment or request is managed
(diagnostic tests, subsequent consultations, inter-
consultations, follow-up notes, etc.). The HIS
facilitates the elaboration of forms, the generation of
reports and the visualization of the patient’s
Electronic Health Record.
Figure 2: System architecture.
Departmental applications are deployed to cover
the specific needs of a given Department or Service.
For example, FarmaTools is the departmental tool for
Pharmacy (drugs purchase, store distribution, and in
this case, cytostatic drug prescription, verification
and management). The appointment system (Quenda)
avoids voice calls and guarantees privacy overall the
hospital consultations. It enables to put in order the
waiting rooms and provides indicators for
consultation management (arrival time to the hospital,
consultation call time, finalization time). The
traceability and indicator system for ODH connects to
the APIs provided by these three tools to
automatically retrieve the data of interest.
Figure 2 shows the TIS architecture, which is in
practice deployed over Linux in a virtual machine.
The traceability and indicator system is composed by
several modules developed in PHP and HTML; these
modules retrieve real time information from the
mentioned systems. For integration with HIS Selene,
HL7 messaging is used, through a channel in the
integration engine MirthConnect. For Quenda,
FarmaTools and Selene’s mirror DB, direct access to
the databases is implemented (SQL Server and Oracle
DB in the last two cases). The TIS is composed by
four main elements: 1) a MySQL database, 2) a main
module in PHP/HTML that shows the current state of
the ODH patients, 3) eleven processes that update the
information in the MySQL database through cron
programmed jobs (Table 2) and 4) the indicators
module.
Table 2: Description of cron jobs.
Job Description Provider
TICKET
Patient takes the turn ticket on
arrival the hospital.
Quenda DB
LAB-
SENT
Patient goes to ODH for blood
test. Blood draw is notified.
HL7
ORU^R01,
HIS Selene
LAB-
RES
Lab result is received. HL7
EXC-
START
Timestamp when the oncologist
calls the patient for consultation.
Quenda DB
PHAR-
CONF
Timestamp for confirmation of
the drugs for the day, enabled by
the oncologist. When PHAR is
notified with the treatment
confirmation, the pharmacologist
in charge verifies the order and
submits it to the technicians, who
start working on the preparation.
FarmaTools
Oracle DB
EXC-
END
Timestamp when the oncologist
finishes the consultation.
Quenda DB
ODH-
ADM
After leaving the consultation, the
patient goes to the ODH and
admission verifies the
appointment and provides the
identification wristband.
HL7
ADT01
PROTOC
OL
The drug protocol is obtained
from the PHAR database,
together with the number of
components to administer to the
patient.
FarmaTools
Oracle DB
PD
When the administration of a
component is completed, it is
registered in the positive
dispensation module.
FarmaTools
Oracle DB
ODH-
DIS
When the administration is
completed, the patient is
discharged.
HL7
ADT^03
ALERTS
It checks if the alerts’ conditions
are fulfilled and generate the
defined alerts if so.
MySQL
DB

Figure 3: a) Main dashboard for traceability. From the fourth column on, it is possible to find the timestamps for the 10 jobs
in Table 2. The 11th job generates the alerts, marked as blocks in orange. In the top right corner of the Figure, a shortcut to
filter the available agendas is provided.
Everyday at 7:00 am, a cron job initiates the
patients’ registry for the day, by using the agendas of
the ODH and the monographic agendas (related to the
oncology specialties) or nominative ones (related to
specific practitioners). Cron jobs are executed each 5-
10 minutes (configurable time), updating the data for
real-time visualization and feeding the indicators’
database.
Access and interface personalization is carried out
through IP control. ODH or Consultation users can
access the ODH TIS through any browser in an
authorized computer. The main interface, in Figure 3,
is daily initialized and dynamically completed
throughout the day, it starts “growing” when the ODH
activity begins. The interface provides visual alerts
(in orange) indicating when issues occur in the
workflow. These alerts are informative up to now,
being generated e.g. when “the laboratory results are
taking too long” or “the patient is not in the next step
of the workflow”. In the future, it is desired that these
alerts may trigger automatic or supervised responses,
such as “recall results from the laboratory” or “send a
notification to the patient”.
In the right side of the real-time interface, there
are several options that enable to parametrize the TIS,
showing information from a) all the agendas, only
from the ODH agendas or the Oncologists
Consultations agendas, b) detailed information about
the patient and c) day indicators.
4 REPORTING
Apart from the visualization interface, the TIS
provides a business intelligence tool that summarizes
a set of relevant key indicators, which can be
classified into four different groups: a) activity, b)
performance, c) procedural and d) quality of care
indicators.
Activity indicators reflect the day dynamics at the
Oncology Service (both at ODH and consultations).
These six indicators are directly accessible from
the interface in Figure 3 and include aspects such as
snapshot of number of active patients in ODH and
patient distribution per agenda (in ODH and
consultations), protocol, visit type and treatment type.
Table 3 shows an example of a protocol indicator, in
particular the one in which each chemotherapy
protocol for a given cancer type is retrieved (an
example of protocol is FOLFOX – oxaliplatin,
fluorouracil, folinic acid - for gastric cancer).
Table 3: Activity indicator example.
Activit
y
indicator no. 4
Scope
ODH, Oncology Consultations
and Pharmacy.
Definition Patient distribution per protocol.
Info. source Selene Replica, FarmaTools
Formula
Query that retrieves the total
number of patients in the agendas
of a) ODH (non-scheduled
patients included) and b)
Oncology Consultations,
classified by protocol.
Goal
To be defined by the evaluator /
manager.

Table 3: Activity indicator example (Cont.).
Activit
y
indicator no. 4
Responsible
Exploitation: Hospital
Management.
Evaluation: Oncology Service
Head
Visualization
The rest of indicators are retrievable from a
specific interface. There are nine performance
indicators, which aims at providing a view of the
service efficiency. This group of indicators include
e.g. the average number of admissions per hour, the
appointments’ status (cancellations, completed, not
registered), the number of non-scheduled patients, the
resource use or the real duration of the treatment. The
information available about an example of
performance indicator, the average duration of the
patient’s stay at ODH, is showed in Table 4.
There are six quality of care indicators that are
focused on compiling information about how the
patient’s perception may be. These indicators include
issues such as the delay of the patient with respect to
the appointment for blood extraction, the delay at the
oncology consultation, the time between the patient’s
appointment and the call time in the oncology
consultation or the delay in the start of the treatment,
etc. An example is available in Table 5.
Finally, there are some specific procedural
indicators that are focused on measuring the
evolution of procedure errors (e.g. admissions
without discharge time, number of never ended
consultations, number of non-called patients, etc.).
Table 4: Performance indicator example.
Performance indicator no. 8
Scope ODH
Definition Avera
g
e sta
y
duration at ODH.
Info. source Selene Replica, MySQL indicators
database
Formula Query, average duration of
admitted patients in ODH.
Goal To be defined by the evaluator /
mana
g
er.
Responsible Exploitation: Hospital Managmnt.
Evaluation: Oncology Service
Hea
d
Statistics Mean: 3.85 h.; Standard
deviation:0.17; Min: 3.51; Max:
4.21.
Visualization
Table 5: Example of Quality of care indicator.
Qualit
y
of care indicator no. 4.
Scope ODH
Definition Delay between the patient’s
scheduled appointment time and the
call time to consultation.
Info.
source
Selene Replica, Oncology
Consultation A
g
endas.
Formula Query, mean delay between the
scheduled time and the real call time
to consultation, filtered for days,
months or years.
Goal 0 minutes.
Responsible
Exploitation: Hospital Managmnt.
Evaluation: Oncolo
gy
Service Hea
d
Statistics Mean: 22.97 m.; Standard deviation:
4.77; Min: 14.21; Max: 31.25.
Visualization
Figure 4 shows the components for the extract,
transform and load (ETL) process necessary to
generate the indicators. All these data are stored in the
MySQL database and queried from a PHP service that
uses Google Chart libraries to generate the final
interface. Everyday, a cron job captures the main
dashboard screen of the traceability system and
emails it to the designated receivers (e.g. Director of
the Oncology Service).
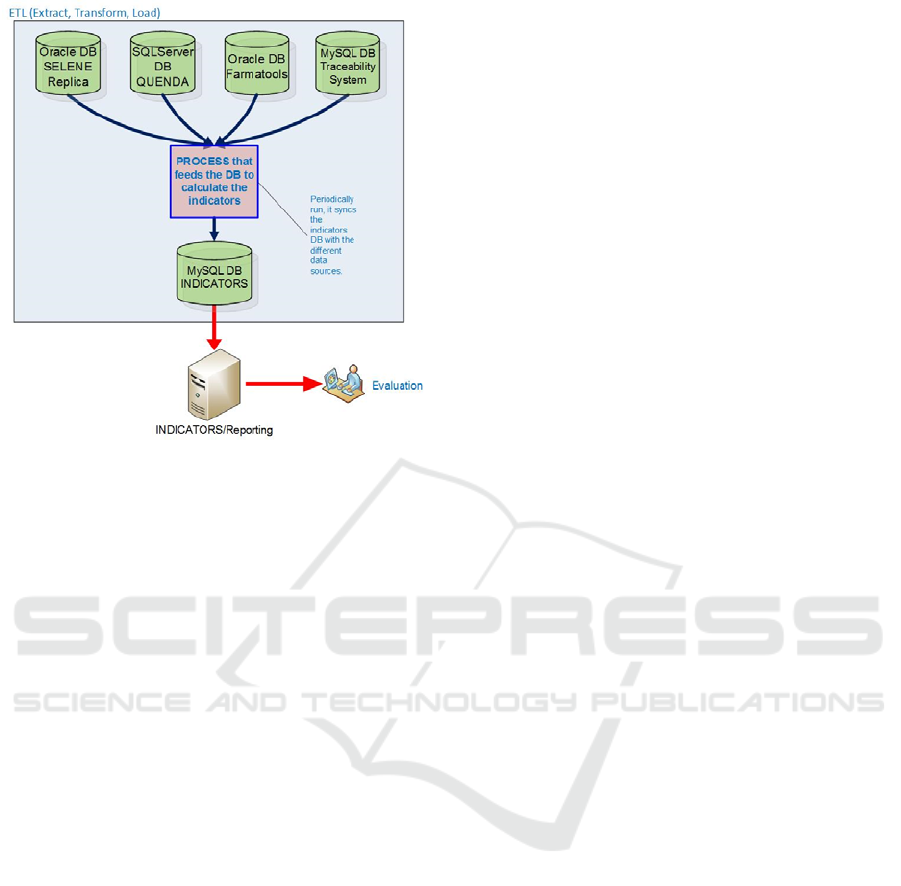
Figure 4: Extract, Transform, Load process for indicators.
DB stands for database.
5 CONCLUSIONS
The Traceability and Indicators System described in
this paper facilitates the retrieval of significant
information in an ODH, with the purpose of
improving daily operation and patient satisfaction.
Traditionally, part of the information retrieved by the
TIS has been manually recorded and processed to
obtain indicators, and only significant deviations,
detected. The TIS has been designed upon request of
the Oncology Service Management to have a better
view of the ODH workflow, so specific
organizational and technical actions can be designed
on a solid informational input.
The TIS has been designed in tight collaboration
with practitioners and administrative staff, with the
objective that it can fulfil the real requirements of
day-to-day operation in the Oncology Service of a
hospital, providing added value and avoiding
problems in the organizational change that the
availability of this tool may suppose.
The TIS relies on information that can be
automatically retrieved from the existing systems in
the hospital. This entails that the deployment does not
require complex technology or significant
investments, while providing relevant information of
the workings of the oncology day hospital. The design
process has been useful to identify information gaps
(e.g. part of the processes that are not automatized,
still done in manual ways), so their improvement can
be added to the strategic agenda of investments.
The system has been technically evaluated against
the design requirements in Section 2.2. Although it
fulfils them reasonably well, there are several aspects
that need to be improved. For example, the
management of both alerts and notifications still need
to be better implemented, and the set of indicators,
polished. Additionally, although the available
presentation interfaces have been incrementally
improved with the help of the users, different
presentation formats should be benchmarked. This
can also be applied to indicators; it is also necessary
to systematically analyse the causes of the detected
deviations to feed the TIS.
Up to now, practitioners and nurses have partly
tried the system in oncology consultations, ODH and
Service Head offices, but their experience with the
TIS is still brief to extract conclusive comments. In
any case, from their feedback it is possible to say that:
The system gathers real-time information in a
reliable way, although it is still necessary to
make some procedural changes to better
contextualize some data. For example, due to
specific instructions given to ODH patients, the
time when these patients take the turn ticket for
consultation is stored, but the entry time at the
hospital is not (ODH patients are told to go
directly for blood draw service).
It is necessary to provide better traceability at
resource level (seat or bed), with the purpose of
optimizing its occupation. This traceability is
manually done and may not be accurate enough
due to human errors. A technical solution
involving RFID or barcodes is currently being
designed to address this issue, and it will be
integrated at the TIS when ready.
Alerts in the real-time visualization interface
need to include specific management options,
to track if the alert has been handled. Up to
now, they are merely informative and no action
is triggered from them.
One of the possibilities to manage alerts is to
make them trigger SMS both to patients or care
professionals, as there is a corporate existing
platform for this purpose. Other options, such
as instant messaging, involve technology and
organizational changes and may delay the
integration with the service. In any case, it is
necessary to study to which extent these SMS
may be effective and useful for their recipients
(misleading or spam effects). In particular, it is
necessary that involved users express their

opinion about the best means and configuration
of alerts.
An important issue is related to human factors: to
assure the full exploitation of the visualization tool
for real time patient-flow management purposes wide
acceptance within the health team is needed. All
health staff members need to understand the ultimate
instrumental goal, focused on improving delivery of
quality of care and not staff monitoring. Specific
communication initiatives are needed to guarantee
that this fact is correctly understood. In this sense, the
involvement of navigator nurses in key steps control
has been shown of great help. In the next months, it is
expected that the tool is integrated in the daily activity
of the ODH and improved following the users
suggestions.
Taking into consideration this TIS, another tool is
currently being designed to monitor the workflow in
the 200 hospital consultations, so delay times and
bottlenecks can be identified.
ACKNOWLEDGMENT
Authors want to acknowledge the Hospital
Universitario Infanta Sofía Management for the
support to this initiative.
REFERENCES
Queralt M., Frías M.C., de Pedro, V., Ramírez, J., Mesalles,
M. 2015. Sistema de trazabilidad integral de
administración de citotóxicos. Boletín de Prevención de
Errores de Medicación de Cataluña, Vol. 12, no.4.
Kergosien, Y., Tournamille, J.F., Laurence, B. and Billaut,
J.C., 2011. Planning and tracking chemotherapy
production for cancer treatment: A performing and
integrated solution. International journal of medical
informatics, 80(9), pp.655-662.
SIAE (2015). Información estadística de hospitales.
Estadística de Centros Sanitarios de Atención
Especializada (National statistic information about
hospitals). Available at: https://www.msssi.gob.es/
estadEstudios/estadisticas/estHospiInternado/inforAn
ual/homeESCRI.htm.
Sini, E., Torresani, M., Locatelli, P., Restifo, N. and
Facchini, R., 2011. Information and communication
technologies enable a comprehensive governance of
patient safety in chemotherapy. An Italian framework
project. In 24th International Symposium on Computer-
Based Medical Systems (CBMS) (pp. 1-7). IEEE.
Masini, C., Nanni, O., Antaridi, S., Gallegati, D., Marri, M.,
Paolucci, D., Minguzzi, M. and Altini, M., 2014.
Automated preparation of chemotherapy: quality
improvement and economic sustainability. Am J Health
Syst Pharm, 71(7), pp.579-85.
Galligioni, E., Berloffa, F., Caffo, O., Tonazzolli, G.,
Ambrosini, G., Valduga, F., Eccher, C., Ferro, A. and
Forti, S., 2009. Development and daily use of an
electronic oncological patient record for the total
management of cancer patients: 7 years' experience.
Annals of Oncology, 20(2), pp. 349-352.
