Overview: The Sustainability of District Health Account in
Contributing to the Strengthening Health System in Sampang
Nensi Kristin Ningsih
Public Health Faculty, Universitas Airlangga, Mulyorejo, Surabaya, Indonesia
nensi.kristin37@gmail.com
Keywords: DHA, Strengthening health system, Sustainability.
Abstract: In 2000, the flow of national funds in Indonesia became increasingly complex, and so the nation needed to
develop a tool (account) to make the measurements of the health expenditures easier. However, DHA
development is often unsustainable, because there’s no government decision or term from government to
make a team consisting of a cross-sector of disciplines. In Sampang, the referral system team was formed
together with a DHA team and HR team in 2013. The problem that Sampang faced was about the culture of
the community where self-referrals were high at 30%. The objective of this paper is to identify the
sustainability of DHA implementation in Sampang. The data collection techniques in this paper have used
secondary data. This paper give results, that Sampang already had DHA team, various data from
SKPD/vertical institutions, and there is interaction between policy makers and DHA team. DHA has
provided benefits for district, such as advocacy when additional health funding is needed, and better health
financing allocations, which will contribute to strengthening the health system in Sampang according to the
specific needs there. The expected result is a recommendation for the government of Sampang to help them
make DHA in Sampang sustainable.
1 INTRODUCTION
In 2000, the flow of national funds became
increasingly complex, so the nation needed to
develop a tool (account) to make the measurements
of the health expenditures easier. As was already
mentioned on the AIPHSS webpage, the need for a
Health Account increased when Sistem Jaminan
Sosial Nasional (SJSN) was enacted in 2014
(AIPHSS, 2013). Health Account is a new way of
health expenditure planning based on evidence. The
needs of health in the future can be analysed and
planned based on the evidence from a given calendar
year (AIPHSS, 2013). Health Account includes a
comprehensive, consistent, and systematic way of
monitoring the utilisation of financing in a given
health system.
Indonesia has already applied Health Account,
referring to the International Standard System, as
agreed by the WHO. AIPHSS mentioned that health
expenditure in Indonesia still amounts to 3% from
Produk Domestik Bruto (PDB), even though the
recommendation from the WHO amount closer to
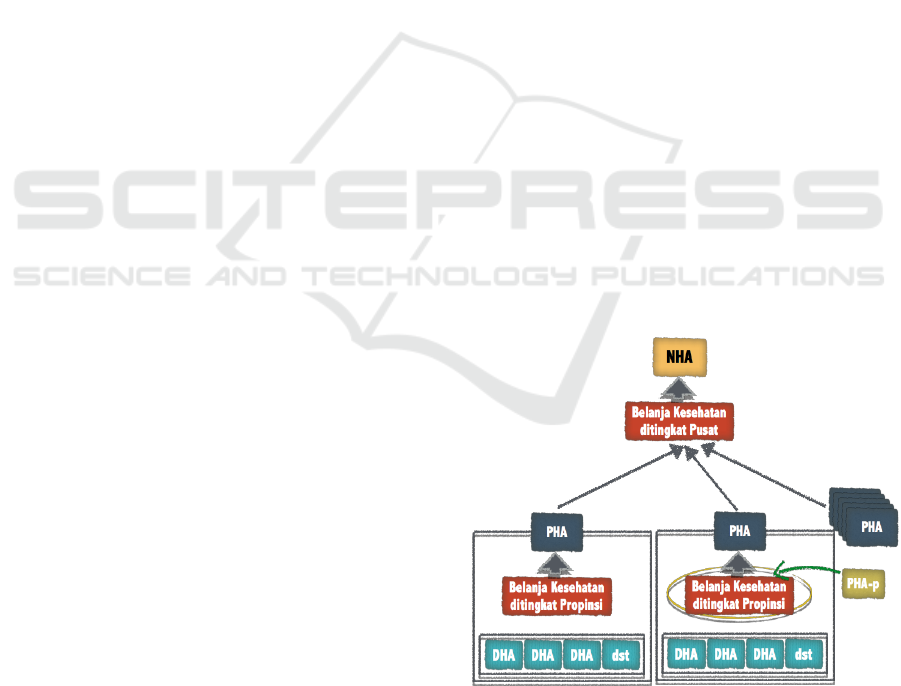
5% from PDB (AIPHSS, 2013). Health Account in
Indonesia is as in the below figure:
Source: Ernawaty, 2017
Figure 1 : Health Account in Indonesia
Different from other countries, Health Account
applied elsewhere is only the National Health
+
+
+
+
+
Ningsih, N.
Overview: The Sustainability of District Health Account in Contributing to the Strengthening Health System in Sampang.
In Proceedings of the 4th Annual Meeting of the Indonesian Health Economics Association (INAHEA 2017), pages 29-32
ISBN: 978-989-758-335-3
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
29

Account (NHA), but Indonesia can’t apply just
NHA. This is because the government system is
based on a system of decentralisation, and the
reports of health expenditure from all sources at the
regional level can’t be done completely collated
(Bappeda of West Java, 2016). Therefore, Indonesia
also applied the Provincial Health Account (PHA)
and District Health Account (DHA).
One of the districts in Indonesia which has
already applied DHA is Sampang
(AIPHSS, 2015).
Sampang already had a team in place for the referral
system in 2013 that consisted of a DHA team and a
Human Resources team (AIPHSS, 2015). Therefore
the question is, how good is the sustainability of
DHA in contributing to the strengthening health
system in Sampang?
In 2014, Sampang had 21 community health
clinics, and one hospital. The Ministry of Health
standard of Indonesia said that the ratio between
community health clinics and the total population is
1:30.000. However, the reality in Sampang is that
there are 929,918 people (data from 2014), so that
one community health clinic can serve 39,870
person. Therefore, for the proportion of community
health clinics in Sampang to be correct, there needs
to be 28 community health clinics (Health Office,
2014).
The health funding of Sampang itself comes
from APBN Ministry of Health, APBN Ministry of
Social, provincial APBD (PAD), district/municipal
APBD (DBH, DAU, DAK and PAD), donors,
grants, household health expenditures and social
institutions/foundations. The total health cost of
Sampang in 2014 based on the multiple sources of
its financing was Rp 339,749,065,932.00 (DHA
Team, 2014). The other data mentioned that the
APBN funds in 2014 amounted to Rp
23,652,717,00.00 which was allocated accordingly.
The JKN funds amounted to Rp 21,693,567,000.00,
overseas grants from AIPHSS amounted to Rp
1,878,083,000,00, and BOK amounted to Rp
1,959,150,000,00 (Health Office, 2014) .
Sampang also faces problems to do with the
culture of the community where self-referrals are
high at 30% (AIPHSS, 2015). The implementation
of DHA of Sampang needs sustainability to
strengthen the health system. The aim of this paper
is to identify the sustainability of DHA
implementation in Sampang.
2 METHOD
This paper was prepared using secondary data
collected from existing data sources. The data
sources were PowerPoint presentations, papers,
documents, regional governments, the Department
of Health and overseas coordination boards. The
appropriate references have been attached.
After all of the data was collected, the
information was compiled into a series of sentences
forming a comprehensive paragraph. The author’s
opinions were also added, and the data collected was
used to reinforce the author's opinion.
3 RESULTS
The implementation of DHA in Sampang can be
seen of as sustainable if it meets four criteria such as
the DHA team having the task to manage data
related to district health expenditure from various
cross sectors, various data coming from SKPD or
vertical institutions/centres, commitment from
policy makers/the government, and the interaction
between policy makers and the DHA technical team.
From the results of the DHA implementation in
Sampang, it already had a DHA team in 2012. The
below are the members of the DHA team in
Sampang (DHA Team, 2014):
1. Anas Muslim, ST. M.AP (Bappeda)
2. Yupita Widyaningsih, S.KM (Dinkes)
3. Daqiqus Syafatain, W. S. ST (Dinkes)
4. Taufiqurrahman, S.KM. MM (RSUD)
5. Ahmad Anang M. S.ST (BPS)
The second results of DHA implementation
related to the data source for the analysis of health
financing of Sampang were derived from the
realisation of the 2013 budget in Satuan Kerja
Perangkat Daerah (SKPD) as well as vertical
institutions/centres in Sampang, like the Department
of Health, RSUD, BPS (Susenas), the Office of the
Secretariat of the Regional People's Legislative
Assembly, the General Section of the Regional
Secretariat, Bappeda, BKD, the Department of
Education, the Department of Social, Bapemas,
BPPKB, Food Security, PNPM, PT. Askes, PKH,
PMI and Jampersal For Private Practice Midwives
(DHA Team, 2013).
The third criterion is about the interaction
between the policy makers and the DHA technical
team. This interaction is shown by the existence of
health expenditure arrangements based on the
funding manager of Sampang in 2014, as follows:
INAHEA 2017 - 4th Annual Meeting of the Indonesian Health Economics Association
30
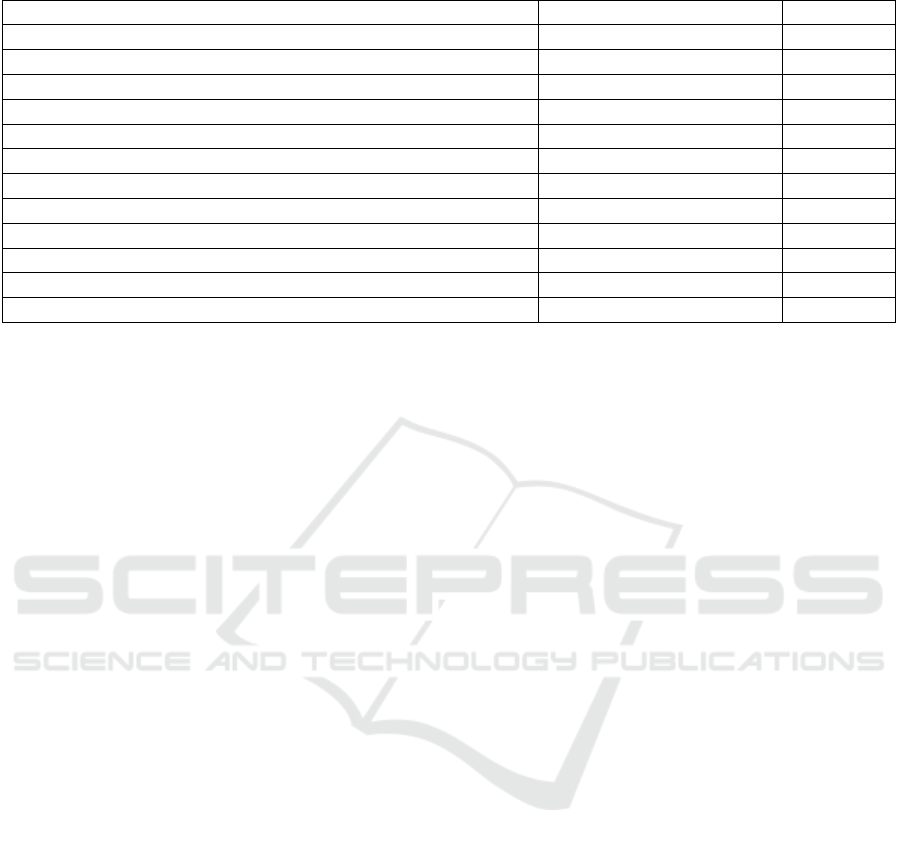
Table 1: Health Care Allocation Based on Financial Manager in Sampang District 2014
Financing Manager
Amount of Expenditures
%
Public Sector
198,895,545,944
59%
HF 1.1.1.2.3 Ministry of Social : Family Hope Program
17,425,593,500
9%
HF 1.1.2.1 Deconcentration Fund
88,750,000
0%
HF 1.1.3.1 District Governments : Health Office
122,407,746,915
62%
HF 1.1.3.12 Other District/City Government
1,482,711,600
1%
HF 1.1.3.3 District General Hospital
56,789,188,429
29%
HF 1.1.3.9 Women’s Empowerment and Family Planning Office
701,555,500
0%
Non Public Sector
140,853,519,988
41%
HF 2.3.1 Household : OOP beyond cost sharing
138,028,079,988
97.994%
HF 2.4.1 NGO / Social Institution / National Foundation
1,525,200,000
1.105%
HF 2.4.2 NGO/ Social Institution / Foreign Foundation
1,300,240,000
0.923%
Grand Total
339,749,065,932
100%
4 DISCUSSION
The results of the secondary data have not shown
two of the criteria that must exist to find out the
sustainability of DHA implementation in Sampang,
such as the commitment from policy makers/the
government, and the interaction between policy
makers and the DHA technical team. The
sustainability of DHA implementation in Sampang
can be seen from the criterion that already
mentioned in the results.
DHA team consisting of a cross-sector, the
secondary data results indicate that the DHA team
has been formed and whose members consist of a
cross-sector. However, there are two people in the
team who come from the same sector of health.
These DHA team members should be more equally
distributed from every sector. There is no other
supporting data stating the reason why, in a DHA
team, there are two people from the same sector, but
for the beginning of DHA implementation in
Sampang, this effort is good enough because there is
an effort from the government to implement DHA to
monitor district health expenditure which is more
systematic than what existed previously. The DHA
team from across multiple sectors is indispensable
for an institution to work well, producing accurate
data which is correct, and beneficial for the DHA
(District Pasaman Government, 2011).
The data sourced from SKPD and vertical/
central agencies, Sampang’s DHA team gets health
expenditure data from SKPD and related
vertical/centre agencies. This is appropriate for the
sustainability of DHA implementation in Sampang.
A variety of data from SKPD sources and vertical
agencies/centres increases the support of active
participation from each SKPD, which means that the
DHA activities in Sampang can be a success
(District Pasaman Government, 2011).
The commitments of policy maker/
government, this criterion is important in
guaranteeing the sustainability of DHA
implementation in Sampang. The commitment of the
policy makers is long-term. There is no secondary
data related to the commitment of the policy makers,
but the actual commitment of the policy
makers/government making can be manifested in the
form of DHA team institutionalisation through
regulation (AIPHSS, 2016). Therefore, the
implementation of DHA in Sampang has been
working.
The interaction between policy makers and
the DHA technical team, this criterion has been
demonstrated by the existence of the health spending
arrangements made by the DHA team. This
interaction is needed to enable the team to respond
to specific policy needs through deeper sub-sector
analysis work as needed (AIPHSS, 2016). The
results are not explained in-depth for the needs of
each sub-sector; the data only shows the health
needs of each sector more generally.
The sustainability of the implementation of DHA
can bring benefits to districts such as a tool for
monitoring and evaluating district-level health
financing ranging from the adequacy of health costs,
allocations to health policies, and effectiveness and
efficiency of health financing; serving as the basis
for financing reforms, the development of the health
insurance system, and the development of social
insurance systems; and the basis for performance-
based planning and budgeting [8]. Therefore, from
the existing data analysis related to the DHA
Overview: The Sustainability of District Health Account in Contributing to the Strengthening Health System in Sampang
31

implementation of Sampang, it is certain that the
District Health Account of Sampang will contribute
to strengthening the health system in Sampang
according to the specific needs of the location.
5 CONCLUSIONS
The implementation of DHA in Sampang has
taken place both due to the seriousness of the
government in the establishment of the DHA team to
the interaction between policy makers and the DHA
technical team from the 2012 data obtained. The first
obstacle came from the preparation of this paper
describing the sustainability of DHA in Sampang in
relation to its contribution to strengthening the
health system such as the lack of data sources of the
latest year discussing about the DHA in Sampang. It
is therefore not known whether DHA in Sampang is
still going on now or not. Another obstacle in the
preparation of this paper was the difficulty of
accessing the secondary data related to DHA in
Sampang. This should be easy in the DHA era
because the community should also participate,
monitor and access it.
The policy makers/government should be able to
remedy the shortcomings of the DHA system in
Sampang, so that in the future, the Sampang District
health expenditure is more open and the community
can also monitor any source of financing for health.
Therefore, a good DHA system can help the
government of Sampang do better advocacy, as well
as the community also becoming more aware about
the details of health expenditure in the District.
REFERENCES
AIPHSS. Health Account: Bukti untuk Perencanaan
Pembiayaan Kesehatan [serial online] July 2013.
Available from URL: http://aiphss.org/id/health-
account-evidence-for-health-financing-planning/.
Accessed September 3, 2017
AIPHSS. National Health Account (NHA) Referensi Bagi
Pembelanjaan Kesehatan [serial online] June 2013.
Available from URL: http://aiphss.org/id/national-
health-accounts-nha-reference-for-health-financing/.
Accessed September 3, 2017.
AIPHSS. DHA: Mendukung Penguatan Sistem Kesehatan
dengan Informasi yang Lebih Baik tentang
Pengeluaran Kesehatan [serial online] September
2015. Available from URL: http://aiphss.org/id/dha-
supporting-health-systems-strengthening-with-better-
information-on-health-expenditure/. Accessed
September 3, 2017.
AIPHSS. Provincial Health Account (PHA) dan District
Health Account (DHA): Melacak Biaya Kesehatan
Daerah [serial online] June 2016. Available from
URL: http://aiphss.org/id/id-provincial-health-
account-pha-dan-district-health-account-dha-melacak-
biaya-kesehatan-daerah/. Accessed September 5, 2017.
Bappeda of West Java. Provincial Health Account
(PHA) untuk Analisis Belanja Kegiatan Kesehatan
Provinsi [serial online] August 2016. Available from
URL: http://bappeda.jabarprov.go.id/7299-2/.
Accessed September 3, 2017.
DHA Team. District Health Account (DHA) Kabupaten
Sampang Tahun 2014 [excel]; 2014.
DHA Team. Protret Pembangunan Kesehatan Berdasarkan
Pembiayaan Kesehatan di Kabupaten Sampang Tahun
Anggaran 2013 [powerpoint presentation]; 2014.
DHA Team. Dokumen DHA Tahun 2013 [document];
2013.
Ernawaty. Health Account [powerpoint presentation];
2017.
Health Office. Profil Kesehatan Kabupaten Sampang
[serial online] 2014. Available from
URL:http://www.depkes.go.id/resources/download/pro
fil/PROFIL_KAB_KOTA_2014/3527_Jatim_Kab_Sa
mpang_2014.pdf. Accessed September 3, 2017.
Pasaman District Government. Dinas Kesehatan
Kabupaten Pasaman Laksanakan Lokakarya DHA
[serial online] December 2011. Available from URL:
http://www.pasamankab.go.id/article-dinas-kesehatan-
kabupaten-pasaman-laksanakan-lokakarya-dha.html.
Accessed September 5, 2017.
INAHEA 2017 - 4th Annual Meeting of the Indonesian Health Economics Association
32
