
Aphasia Types and Language Modality Disorder by Ischemic Stroke
Patient
Willyana Willyana, Syihabuddin Syihabuddin and Dadang Sudana
Sekolah Pascasarjana, Universitas Pendidikan Indonesia, Bandung, Indonesia
willyanaramlan25@gmail.com, syihabuddin@upi.edu, dsudana2013@yahoo.com
Keywords: Aphasia, Ischemic Stroke, Modality, Language.
Abstract: This study focuses on analysing the types of aphasia caused by an ischemic stroke and their modality
language disorder. The classification of aphasia syndromes employed in this research is based on Benson
(1979). The subjects of the study were one male patient and two female patients with ischemic stroke in
RSUD Subang. The data for this case study were collected and analyzed by using the TADIR test by
Dharmaperwira-Prins (2000). Based on the analysis, it is concluded that there are two types of aphasia
caused by the ischemic stroke, namely transcortical motor aphasia and broca’s aphasia. The participants
with broca’s aphasia and transcortical motor aphasia had a disorder in spontaneous speech on personal
information, such as listing, words and sentence naming, and not only verbally, but also in writing
comprehension. The participant with broca aphasia had verbal paraphasia; however, the participant with
transcortical motor aphasia only had literal paraphasia. Patients with broca’s Aphasia and transcortical
motor aphasia produced fewer than 76 words per minute, which indicated that they suffered from a non-
fluent type of aphasia. Disorder with reading aloud and repetition in broca’s aphasia were more severe than
in those with a transcortical motor aphasia. The male transcortical motor participant was able to write,
although suffering from literal paragraphia. On the contrary, the female participants were unable to write
because they had the weakness on the right side of the body.
1 INTRODUCTION
The nature of communication is an interaction
process between people, which is expressed in the
form of one’s thoughts or feelings to another using
language as the medium. Effendi (1993) argues that
communication means the act of delivering a
message from the sender to the receiver. The
message delivery in a communication process must
be able to create a shared meaning between the
sender and the receiver, so that a good message relay
can occur. However, the message delivery is often
hindered by several disturbances, Gamble (1986) in
Nurudin (2007) reveals that communication
disturbances are factors that affect the pace of a
message or interfere with the ability of sending or
receiving a message.
Generally, communication disturbances are
either static ones (constant and always present), or
dynamic ones (continuously changing). For instance,
the static disturbances of climate and weather
disturbances are wind, rain, and the obstacles from
the surrounding physical environment. Meanwhile,
the dynamic disturbances be resolved despite their
constant state of change, such as an engine failure on
message transmission machines (telephone and the
like), psychological disturbance (low self-esteem,
anxiety, phobia), physical disturbance, and semantic
disturbance and semantic disturbance. Semantic
disturbance which causes a hindered communication
process can occur because of a brain tumor, brain
infection (meningitis), traumatic brain injury (TBI),
dementia, alzheimer, cerebral palsy and stroke.
A Stroke is one of the brain disorder sources
which occurs at the peak of a productive age and is
considered to be a second cause of death after the
heart attack in most countries. In the United States
of America, stroke is the third death cause for adults.
Every year, the mortality rate is solely caused by a
stroke which accounts for more than 200,000. Stroke
incidents on the national scale are approximately
750,000 each year. The incidence number of
African-Americans is 60% higher than in
Caucasians (Sacco, et.al., 2013). Some suffer a
stroke at all ages, but two-thirds of stroke incidence,
impact people of age above 65. In Asia, stroke
434
Willyana, W., Syihabuddin, S. and Sudana, D.
Aphasia Types and Language Modality Disorder by Ischemic Stroke Patient.
DOI: 10.5220/0007168704340440
In Proceedings of the Tenth Conference on Applied Linguistics and the Second English Language Teaching and Technology Conference in collaboration with the First International Conference
on Language, Literature, Culture, and Education (CONAPLIN and ICOLLITE 2017) - Literacy, Culture, and Technology in Language Pedagogy and Use, pages 434-440
ISBN: 978-989-758-332-2
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

incidence accounts for more than two-thirds of the
global incidence of stroke (Suwanwela and
Poungvarin, 2016). According to the Ministry of
Health data, in Indonesia, stroke is also considered
to be the leading cause of death, with a stroke
prevalence of 12.1/1000 recorded in 2013. Thus, it
can be assumed that 4 out of 1000 Indonesians are at
risk of aphasia. Unfortunately, Neuro-rehabilitation
in Indonesia does not always include speech therapy.
This is true especially in smaller hospitals or more
remote areas where stroke is treated only with the
primary care of physicians. Often, stroke patients
may receive neither aphasia assessment nor
intervention.
The limited attention being paid by linguists to
clinical linguistics, especially language disorders of
stroke patients (especially in Indonesia) are the main
reason this research was conducted. Besides,
according to previous research, it was found that
there are language disorders suffered by people with
aphasia. However, there is no specific note about the
type of aphasia observed, and the linguistic disorders
discussed are still in general aspects. Therefore, the
objectives of the research are to analyse the types of
aphasia caused by ischemic stroke and their
modality language disorders.
2 APHASIA
Aphasian said can be defined as the loss or
impairment of language caused by brain damage. In
more depth, Goodglass and Kaplan (1972) define
aphasia as disturbance of any or all of the skills,
association and habits of spoken or written language,
produced by injury to certain brain areas which are
specialized for this function. Aphasia is labelled as
aphasic, namely a variety of limited disorder such as
“selective disorders of auditory comprehension,
object-naming, articulation, reading or repetition...”,
and these experts classify alexia with or without
agraphia among the aphasias. Schuell, Jenkins, and
Jumenez-Pabon (1964) require that aphasia be
reserved for language disorder crossing all
modalities – reading, writing, listening, speaking,
and gesturing.
Sinanović, et. al. (2011) states that there are
different definitions of aphasias, but the most widely
accepted neurologic and/or neuropsychological
definition is that aphasia is a loss or impairment of
verbal communication, which occurs as a
consequence of brain dysfunction. It manifests in
impairment of almost all verbal abilities, i.e.
abnormal verbal expression, difficulties in
understanding spoken or written language,
repetition, naming, reading and writing.
2.1 Types and Characteristics of
Aphasia
Apart from the broca’s and wernicke’s type of
aphasia, Ardila (2014) proposed diverse aphasia
classifications since Broca’s first description of a
language disorder associated with brain pathology
(Broca, 1863). There are, however, two most
influential aphasia classifications, that have
significantly guided the area during the last decades:
the Boston Group classification; and Luria’s aphasia
interpretation. The first one has been particularly
influential in the US and western European
countries; the second one has been mostly used in
eastern European countries and Latin America.
Boston Group classification represents a further
development of Wernicke’s ideas about brain
organization of language, and includes two basic
distinctions: (1) aphasias can be fluent or non-fluent;
and (2) aphasias can be cortical, subcortical, or
transcortical (e.g., Benson, 1979; Goodglass and
Kaplan, 1972). Nevertheless, this research uses the
classification stated by Benson (1979) that classifies
aphasia more in detail, into global aphasia, broca’s
aphasia, wernicke’s aphasia, anomic aphasia,
conduction aphasia, transcortical motor aphasia,
transcortical sensory aphasia, and mixed
transcortical aphasia.
Examination, diagnosis, and treatment on
aphasia patients resulted in the classification of
aphasia. Some systems use neurology criteria, in
which the location of brain injury becomes the
condition to classify aphasia. Other systems classify
aphasia based on the linguistic ability of the
disorder, namely The National Aphasia Association
in the United States of America classifies aphasia
into fluent and non-fluent. In fluent aphasia, also
called as Wernicke’s/posterior/sensory/receptive
aphasia, the language comprehension is very poor,
but fluent in their language. Fluent aphasia results in
long and unorganized utterances, good articulation
with the melody and supra-segmental characteristics
just like in normal utterances (these characteristics
may give the impression to the audience that fluent
aphasia possesses a good linguistic ability).
Non-fluent aphasia is also called as
broca’s/anterior/motor/expressive aphasia. People
with non-fluent aphasia may have difficulty in word
production, even though the comprehension is
relatively intact. In non-fluent aphasia, patients
challenge themselves to express utterances, unlike
Aphasia Types and Language Modality Disorder by Ischemic Stroke Patient
435
the ones with fluent aphasia. They realize that they
are poor and frustrated and have great difficulty
forming complete sentences. The articulation and the
characteristics of supra-segmental utterances form
are severely disturbed. The intonation unit is really
short and affects the grammatical ability, the deficit
of sentences structure's ability, and producing
incomplete sentences. Non-fluent aphasia patients
are also known as suffering from agrammatic
speech, in which their speaking quality is like
telegrammatic speech. For instance, if they want to
say, “I will take the dog for a walk”, they will only
say, “walk dog”. The occurrence of lexical-
semantical disorder, in which the patients make
mistakes in using dictions, for example, using ‘front’
when they mean ‘back’. This is called semantic
paraphasia, while phonemic paraphasia occurs when
the intention is saying ‘snowman’, but ‘stowcan’
comes out instead.
3 STROKE
3.1 Definition of Stroke
Stroke is defined as cerebrovascular disease that is
incorporated into a sudden neurologic disorder
caused by a blockage of blood flow to the brain
through the artery supply system. In line with Wolf
(2004) in Talvitie, et.al. (2010), stroke is the most
common, life-threatening neurologic disease with an
annual incidence of approximately six cases in 1000
persons. The older term often used is
Cerebrovascular Accident (CVA). According to
Delaney and Potter (1993) in Teasell, Hussein and
Norhayati (2013), stroke is a cerebrovascular
disorder which represents the third leading cause of
mortality and the second major cause of long-term
disability in North America.
3.2 Types of Strokes
The types of stroke as mentioned by Ardila (2014)
are the two major types of strokes distinguished:
hemorrhagic and ischemic.
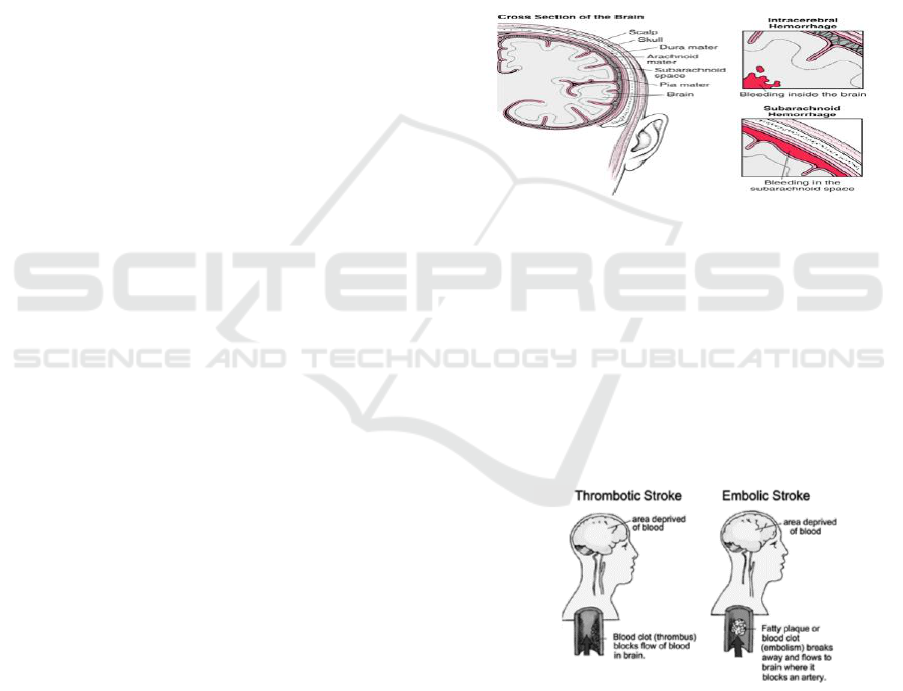
Haemorrhagic stroke (see figure 1) is another
type of stroke. It is caused by an artery in the brain
bursting and causing localized bleeding in the
surrounding tissues. Two major types of brain
hemorrhage are distinguished, as figure 1 shows.
a. Subarachnoid hemorrhage: There can be
bleeding into the subarachnoid, the space
between the arachnoid and the pia mater, the
innermost membrane surrounding the central
nervous system. Most frequently, it is caused by
bleeding from a cerebral aneurysm, but also can
be due to bleeding from an arteriovenous
malformation or head injury; Injury-related
subarachnoid hemorrhage is often seen in the
elderly who have fallen and hit their head.
Among the young, the most common injury
leading to subarachnoid hemorrhage is motor
vehicle crashes;
b. Intracerebral hemorrhage: is a type of stroke
caused by bleeding within the brain tissue itself.
It is most commonly caused by hypertension,
arteriovenous malformations, or head trauma.
Figure 1: Haemorrhagic stroke.
Ischemic stroke (as figure 2 shows) two different
conditions can be found relative to ischemic stroke:
a. Embolism: it is the occlusion of a vessel by
material floating in the arterial system. The
emboli are usually formed from blood clots, but
are occasionally comprised of air, fat, or tumour
tissue;
b. Thrombosis: is the formation of a blood clot
(thrombus) inside a blood vessel, obstructing the
flow of blood through the circulatory system.
Figure 2: Ischemic stroke.
On the other hand, stroke can be classified based
on anatomical pathology and the causes (Misbach,
2011), namely ischemic and hemorrhagic stroke.
The incidence of ischemic stroke accounts for 70-80
% of the total incidences. Meanwhile, hemorrhagic
stroke cases are low in number. The types of
ischemic stroke, according to the pathology and its
causes are transient ischemic attack (TIA), cerebral
CONAPLIN and ICOLLITE 2017 - Tenth Conference on Applied Linguistics and the Second English Language Teaching and Technology
Conference in collaboration with the First International Conference on Language, Literature, Culture, and Education
436

thrombosis and cerebral embolism. Ischemic stroke
is the major cause of the damage on left brain or left
hemisphere. The damage on the left hemisphere of
the brain causes communication disorder called as
aphasia (dysphasia).
4 RESEARCH METHODS
This study was conducted to reveal the types of
aphasia caused by ischemic stroke. In particular, this
research attempts to obtain a clear description of
their modality language disorder. This study was
conducted at RSUD Subang, West Java, Indonesia.
The site selection was based on several reasons.
First, this hospital was very welcoming to the
researcher who would like to undertake a research.
Second, participants were cooperative and the
researcher had little difficulties in collecting data
from them. Also, with the patients’ relatives who
were in charge, they were really helpful. The
participants of the study were 1 male and 2 female
patients with ischemic stroke in RSUD Subang. This
study was also assisted by a neurologist from RSUD
Subang who diagnosed the disease suffered by the
patients.
This study uses the case study as a research
method. By using a case study, the data obtained are
expected to fulfil criteria strictly in accordance with
the research to be conducted. As Merriam (1988)
suggests that a case study is a bounded system or a
defined individual or entity (like a student, program,
school, institution) that the researcher wishes to
explore. However, Stake (1995) points out that what
forms the boundaries and the context is not
immediately apparent. Yin (2003) agrees, defining a
case study as an empirical inquiry that investigates a
contemporary phenomenon within its real-life
context, especially when the boundaries and the
contexts are not clearly evident.
The data for this case study were collected and
analysed by using the TADIR by Dharmaperwira-
Prins (2000). According to The TADIR (Tes Afasia
untuk Diagnosis, Informasi, dan Rehabilitasi) or
Aphasia Test for Diagnosis, Information, and
Rehabilitation has four aims that are fulfilled by a
combination of the subtests (Dharmaperwira-prins,
2000); (1) to diagnose individuals with or without
aphasia, (2) to diagnose which aphasia syndrome is
being suffered, (3) to provide information to
patients, and their environment, (4) to provide a
basis for therapy and rehabilitation. The partisipants
tasks are (1) spontaneous speech in personal
information, (2) listing some animals names in one
minute (3) naming in word and sentence level (4)
spontaneous speech, elicited by a set of questions (5)
reading aloud (6) word and sentence repetition (7)
verbal language comprehension in word and
sentence level (8) written language comprehension
in word and sentence level (9) writing personal
information (10) dictation word level (11) filling-in
own personal information, (12) writing in word and
sentence level.
The duration for administering the TADIR was
set to be one hour, and the manual recommends the
testing to be split into two separate sessions of thirty
minutes. All the participants with ischemic stroke in
this study were tested with the TADIR.
5 FINDINGS AND DISCUSSION
The test results showed that there were two types of
aphasia caused by ischemic stroke, namely motor
transcortical and broca’s aphasia, as table 1 shows in
Appendix. The detailed explanation is stated below.
P1, male, achieved a normative score from the
listing subtest (4) and word-level naming (4),
therefore P1 got a score of 1-4 of both subtests,
which meant P1 suffered aphasia. Next, from the
verbal fluency score achieved from spontaneous
speech subtest, P1 got 36 words per minute (below
76 words per minute), thus it was found that P1
suffered non-fluent aphasia. In order to disclose the
types of non-fluent aphasia suffered by P1, it can be
decided from verbal comprehension (word and
sentence level) and sentence repetition. Normative
score from verbal comprehension of P1 was 3, and
the sentence repetition score was 5, thus it was
certain that P1 suffered transcortical motor aphasia.
P2, female, achieved a normative score from
listing (4) and word-level naming (4), therefore P2
got a score of 1-4 of both subtests, which meant P2
suffered aphasia. Then, from fluency score achieved
from spontaneous speech subtest, P2 got 25 words
per minute (under 76 words per minute), thus it was
found out that P2 suffered non-fluent aphasia. To
decide what type of non-fluent aphasia suffered by
P2, it can be decided from verbal comprehension
(word and sentence level) and sentence repetition.
Normative score from verbal comprehension of P2
was 3, and the sentence repetition score was 3, thus
it was certain that P2 suffered broca’s aphasia.
P3, female, achieved a normative score from the
listing subtest (4) and word-level naming (4),
therefore P3 achieved scores of 1-4 of both subtests,
which meant P3 suffered aphasia. Then, verbal
fluency score achieved from spontaneous speech
Aphasia Types and Language Modality Disorder by Ischemic Stroke Patient
437

subtest, P3 got 13 words per minute (under 76 words
per minute), thus it was found that P3 suffered non-
fluent aphasia. In order to determine the type of non-
fluent aphasia suffered by P3, it can be decided from
verbal comprehension (word and sentence level) and
sentence repetition. Normative score from verbal
comprehension of P3 was 4, and the sentence
repetition score was 4, thus it was certain that P3
suffered motor transcortical aphasia.
P1 obtained a normative score 3 for spontaneous
speech with personal information, 4 for listing, 4 for
word level naming, and 3 for sentence level naming.
P2 achieved normative score 4 for spontaneous
speech in personal information, 4 for listing, 4 for
word level naming, and 3 for sentence level naming.
While, P3 achieved a normative score 4 for
spontaneous speech in personal information, 4 for
listing, 4 for word level naming, and 3 for sentence
level naming. Therefore, it can be concluded that the
participants with broca’s aphasia and motor
transcortical aphasia had a disorder in spontaneous
speech in personal information, listing, word and
sentence naming, and not only in verbal, but also in
writing comprehension.
P2 with broca’s aphasia had verbal paraphasia,
P2 called “segitiga” (triangle) on card 1 with
“persegi” (square). Literal paraphasia also occurred
in P3, female motor transcortical aphasia patient, in
this case P3 changed the syllables of ‘gelas’ (glass)
into ‘beras’ (rice).
Reading aloud and repetition disorder in broca’s
aphasia was more severe than in motor transcortical.
The patient with broca’s aphasia gained a normative
score 1 (reading aloud) and 3 (repetition), which
meant the participant with broca’s aphasia was
having great difficulty in reading aloud and
disturbed in repeating.
On the other hand, the male participant with
motor transcortical obtained a normative score 3
(reading aloud) and 5 (repetition), which meant the
male participant with motor transcortical suffered
difficulty in reading aloud but was able to repeat
normally. A better score was achieved by the female
participant with motor transcortical who got a
normative score 4 (reading aloud) and 4 (repetition),
which meant either in reading aloud and repetition,
the participant with motor transcortical had only a
little difficulty. In writing ability, the male
participant with motor transcortical was able to
write, although suffering from paragraphia literal, as
figure 3 shows.
Figure 3: Paragraphia literal in P1.
Conversely, the female participants were unable
to write because they had weaknesses on the right
side of the body, as figure 4 and 5 show.
Figure 4: Handwriting P2.
Figure 5: Handwriting P3.
6 CONCLUSIONS
The objectives of the research are to analyze the
types of aphasia caused by ischemic stroke and their
modality language disorder. Benson (1979)
mentioned eight types of aphasia i.e. global aphasia,
broca aphasia, aphasia wernickhe, anomic aphasia,
aphasia conduction, aphasia motor transcortical,
sensory transcortical aphasia and mixed transcortical
aphasia. However, the type of aphasia found in 3
patients suffering from ischemic stroke is only broca
aphasia and motor transcortical aphasia. To
answering the second research question about the
partisipants modality language disorder, the
participants with aphasia broca and motor
transcortical had a disorder in spontaneous speech in
personal information, listing, word and sentence
naming, and not only in verbal, but also in written
comprehension. The participants with aphasia broca
had verbal paraphasia, and literal paraphasia also
occurred to female transcortical motor. Aphasia
broca and transcortical motor uttered fewer than 76
words per minute (P1-36, P2-25, dan P3-13). It
showed that they suffered from non-fluent aphasia.
Reading aloud and repetition disorder in aphasia
broca was more severe than in motor transcortical.
The male motor transcortical participant was able to
write although suffering from paragraphia literal.
Conversely, the female participants were unable to
write because they had a weakness on the right side
of the body.
CONAPLIN and ICOLLITE 2017 - Tenth Conference on Applied Linguistics and the Second English Language Teaching and Technology
Conference in collaboration with the First International Conference on Language, Literature, Culture, and Education
438

ACKNOWLEDGEMENTS
I am very gratefully acknowledge the help of dr. Edi
Prasetyo, Sp.S. In addition, I would like to thank
Walim, Umas, and Siti Khodijah for their immense
help in various ways. I am very grateful to Farida
Hidayati, M. Pd for correcting my English.
REFERENCES
Ardila, A., 2014. Aphasia Handbook. University Miami:
Florida, USA.
Benson. D. F., 1979. Aphasia, Alexia, and Agraphia. New
York: Churchill Livingstone
Broca, P., 1863. Localisation des functions cerebrales.
Siege de la faculte du langage articule. Bull Soc
Anthropol, 4, pp.200-208.
Sacco, R. L., Kasner, S.E., Broderick, J.P., Caplan, L.R.,
Culebras, A., Elkind, M.S., George, M.G., Hamdan,
A.D., Higashida, R.T., Hoh, B.L. and Janis, L.S., 2013.
An updated definition of stroke for the 21st century: a
statement for healthcare professionals from the
American Heart Association/American Stroke
Association. Stroke, 44(7), pp.2064-2089.
Dharmaperwira-Prins, R. I. I., 2000. Tes Afasia untuk
Diagnosis Informasi Rehabilitasi. Jakarta: Balai
Penerbit FK UI.
Effendy, O. U., 1993. Ilmu, Teori & Filsafat Komunikasi.
Bandung: PT. Citra Aditya Bakti
Goodglass, H., and Kaplan, E., 1972. The assessment of
aphasia and related disorders. Philadelphia: Lea &
Febiger.
Merriam S. B., 1988. Case Study Research in Education.
San Francisco: Jossey-Bass
Misbach, J., 2011. Stroke. Jakarta: Kelompok Study Club
Stroke Perhimpunan Dokter Spesialis Syaraf Indonesia.
Nurudin, 2007. Pengantar Komunikasi Massa. Jakarta: PT.
Raja Grafindo Persada.
Schuell, H., Jenkins, J. J., Jimenez-Pabon, E., 1964.
Aphasia in Adults: Diagnosis, Prognosis, and
treatment. Newyork: Harper and Row.
Sinanović, O., Mrkonjić, Z., Zukić, S., Vidović, M., and
Imamović, K., 2011. Post-Stroke Language Disorders.
Acta Clin Croat, 50, pp.79-94.
Stake, R. R. E., 1995. The Art of Case Study Research.
Thousand Oaks, CA: Sage Publications
Suwanwela, N.C. and Poungvarin, N., 2016. Stroke burden
and stroke care system in Asia. Neurology India, 64(7),
p.46.
Talvitie, S.S., Matilainen, L.E., Pekkonen, E., Alku, P.,
May, P.J. and Tiitinen, H., 2010. The effects of cortical
ischemic stroke on auditory processing in humans as
indexed by transient brain responses. Clinical
Neurophysiology, 121(6), pp.912-920.
Teasell, R., Hussein, N., and Norhayati, 2013.
Consequences of Stroke. MBBS Clinical.
Yin, R. K., 2003. Case Study Research: Design and
Methods. Thousand Oaks, CA: Sage Publications.
Aphasia Types and Language Modality Disorder by Ischemic Stroke Patient
439

APPENDIX
Table 1: Analysis of aphasia types and language modality disorder of ischemic stroke patient.
Type of
Aphasia
Language Impairment
Comprehension
Production
Listening
Reading
Speaking
Writing
Word and
Sentence
Level
Word and
Sentence
Level
Personal
Information
Personal
Information
Listing
Naming
Word
Level
Naming
Sentence
Level
Spontaneous
Speech
Reading
Aloud
Repetition
Personal
Information
Dictation
Word
Level
Sentence
Level
Broca
(Female)
3
3
4
4
4
4
3
Average 25
words/minute
(non-fluent)
1
3
1
1
1
1
Transcortical
Motoric
(female)
4
4
3
4
4
4
3
Average 13
words/minute
(non-fluent)
4
4
2
1
1
1
Transcortical
Motoric
(male)
3
3
3
3
4
4
3
Average 36
words/minute
(non-fluent)
1
5
2
4
3
3
CONAPLIN and ICOLLITE 2017 - Tenth Conference on Applied Linguistics and the Second English Language Teaching and Technology
Conference in collaboration with the First International Conference on Language, Literature, Culture, and Education
440
