
Correlation between Spirituality and Coping Strategy in Patients with
Type 2 Diabetes Mellitus
Nur Widayati, Nuhita Siti Rohmin, Retno Purwandari
Faculty of Nursing, University of Jember, Jember, East Java, Indonesia
Keywords: Type 2 Diabetes Mellitus, Spirituality, Coping strategy.
Abstract: Patients with type 2 Diabetes Mellitus (DM) experience changes related to self-care management. This
condition can lead to a negative psychological reaction such as stress. People deal with stress depending on
their coping strategy. One of the factors affecting coping strategy is spirituality. This study aimed to analyse
the correlation between spirituality and coping strategy in type 2 DM patients. This research applied an
observational analytic design with cross-sectional approach. A total of 84 respondents were enrolled in this
study by using consecutive sampling technique. Data collection was conducted by administering
questionnaires of Daily Spiritual Experience Scale (DSES) and Cope Inventory. Data were analysed by
using Spearman correlation test with significance level of 0.05. The result showed that the mean value of
spirituality was 70.25 and coping strategy was 75.88. There was a significant positive correlation between
spirituality and coping strategy (p-value: 0.001; r: 0.616). The correlation is strong and positive which
means the higher the level of spirituality the better the coping strategy. This study suggests the importance
of assessing the aspect of spirituality to optimize coping strategy in patients with type 2 DM.
1 INTRODUCTION
Diabetes Mellitus (DM) is one of the world's health
problems with an increasing prevalence every year.
The global prevalence of DM was 8.8% in 2015 and
it is predicted to increase to 10.4% in 2040. Adult
people with diabetes will rise from 405 million
people in 2015 to 642 million people by 2040. In
2015 Indonesia ranked seventh of the top ten
countries with the highest number of adults with
diabetes in the world. The number of adult people
with DM in Indonesia was 10 million people by 2015
and it is estimated to reach 16.2 million by 2040
(International Diabetes Federation, 2015). The
prevalence of DM increased from 1.1% in 2007 to
2.1% in 2013 (Indonesia Ministry of Health, 2013).
Diabetes causes lifestyle changes and
complications that negatively affect the health and
social life of the patients (Young and Unachukwu,
2012). DM also results in a negative psychological
response or emotional disorders such as stress,
anxiety, and depression (Chew, Ghazali and
Fernandez, 2014). When a person is diagnosed with
DM, they should adopt an adaptive coping strategy
immediately in order to perform proper therapeutic
management. However in reality, not all of DM
patients have an adaptive coping strategy (Saputra et
al., 2017). A study of 201 patients with type 2
diabetes showed a maladaptive coping strategy that
focused on emotions (17.9%) and avoidance (72.1%)
(Moasheri et al., 2017).
Coping skill is important in the management of
diabetes because effective coping improves self-
management, better blood sugar control, and
decreases complications (Grey, 2000). One of the
factors that influence coping is spirituality belief
(Stuart, 2013). Spirituality is mentioned as a process
of discovering the meaning and purpose of one's life
by relying on God, the relationship to the universe,
and peace (Graham et al., 2001). Research of
spirituality in 200 persons with DM resulted in 86
people (43%) had moderate spirituality and 114
people (57%) had high spirituality (Zareipour et al.,
2016).
Spirituality is used as a source of emotional
support, a positive influence on health and a role in
life satisfaction (Samuelhodge et al., 2000).
Spirituality becomes a source for better problem
solving and self-adaptation. Faith and religion are
used to accept the reality of the disease, to manage
conditions patiently and tolerantly, to hope calmly,
and to be confident for a good future (Shahrbabaki et
al., 2017). The practice and belief of spirituality
458
Widayati, N., Rohmin, N. and Purwandari, R.
Correlation between Spirituality and Coping Strategy in Patients with Type 2 Diabetes Mellitus.
DOI: 10.5220/0008326804580465
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 458-465
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

become a coping mechanism that can relieve
physiological and psychological stress such as pain
and helplessness (Harvey and Silverman, 2013). The
more important the spirituality for an individual the
greater the individual's coping ability towards the
problem (Graham et al., 2001). Spirituality plays an
important role in one's central life in facing
challenges by prioritizing strength and hope (Gupta
and Anandarajah, 2013). Spiritual factor contributes
positive activity to behavioural changes and
individual motivations that impact on lifestyle
changes in achieving blood glucose control
(Wibisono, 2012).
Public Health Center (PHC) of Jenggawah
ranked sixth in terms of the highest number of DM
patient visit in 2016 of all PHC in Jember Regency.
Preliminary study on 10 patients with type 2 diabetes
in the area of PHC of Jenggawah showed an average
value of spirituality of 59.7 from the maximum value
of 90. The average value of coping strategy was 60.8
from the maximum value of 112. Three people who
had spirituality in high category said that they did not
feel worried and they did not obedient in doing a
healthy lifestyle such as diet. The reason they did not
follow the recommended diet because they think the
fate has been determined by God and healthy or
illness is destiny from God. Seven people who had
spirituality in moderate category said that even
though they had performed worship activities but
sometimes they feel worried and afraid of the illness.
They said that the illness is the result of their own
mistakes for not taking care of their health in the
past, however, they said they are living with the
spirit and they do not forget to pray. Based on this
background, this research was conducted to analyse
the correlation between spirituality and coping
strategy in type 2 DM patients.
2 METHODS
This study was a quantitative, observational analytic
study with cross-sectional approach. The
independent variable was spirituality and the
dependent variable was coping strategy. The
population of this study was all of type 2 DM
patients recorded in PHC of Jenggawah Jember from
January 2016 until September 2017; that was 295
people. The sample was determined by G* Power 3
-
error probability): 0.80, effect size: 0.30) and
obtained a sample of 84. Consecutive sampling
technique was applied in this study. The sample was
determined based on the order of names of type 2
diabetes patients recorded at PHC of Jenggawah
from January until September 2017. The inclusion
criteria included patients who have been diagnosed
with type 2 DM for at least 3 months, able to
communicate well, and willing to participate. The
exclusion criteria were patients who have severe
physical disorders or conditions that are not possible
to participate in the research, have physical
limitations such as blindness or deafness, have
severe mental disorders such as Alzheimer's or
dementia assessed by Mini-Mental State
Examination (MMSE).
Spirituality was assessed by using Daily Spiritual
Experience Scale (DSES) questionnaire
((Underwood, 2006); (Underwood and Teresi,
2002)). Face validity test of Indonesian translation of
DSES in 20 DM patients showed that all of the
respondents could easily and did not have difficulties
when filling DSES questionnaire
Wijayanti, 2015). The value of Cronbach's Alpha of
Indonesian translated DSES was 0.79 (Karomah,
2015). The minimum score of spirituality is 15 and
the maximum score is 90. The minimum value for
each indicator is 1 and the maximum value is 6.
Coping strategy was measured using Cope Inventory
questionnaire ((Carver, Scheier and Weintraub,
1989); (Rahmaturrizqi, 2012)). Indonesian translated
questionnaire has been tested for its validity and
reliability and it showed a value of 0.791
(Rahmaturrizqi, 2012). The minimum score of
coping strategy is 28 and the maximum score is 112.
The minimum score for each indicator is 1 and the
maximum score is 4.
Data collection was conducted in December
2017. The researcher visited each respondent's house
based on the name and address of patients recorded
at PHC of Jenggawah. Respondents who agreed to
participate in this study were asked to sign the
consent. This research was conducted after obtaining
approval from Research Institute of University of
Jember (No: 7003/UN25.3.1/LT/2017), Department
of Political Unity for the Protection of the Public
(No: 072/4530415/2017), and the District National
Health Department (No: 440/54136/311/2017).
Univariate analysis was performed to describe the
respondent characteristic, spirituality, and coping
strategy. Spirituality was categorized as follows: low
(score 15-40), moderate (score 41-65), and high
(score 66-90). Before conducting bivariate analysis,
Kolmogorov Smirnov was used to test the normality
of the data. Based on the result of normality test, data
were analyzed by Spearman correlation test with
significance level of 0.05.
Correlation between Spirituality and Coping Strategy in Patients with Type 2 Diabetes Mellitus
459
3 RESULTS
3.1 Characteristics of Respondents
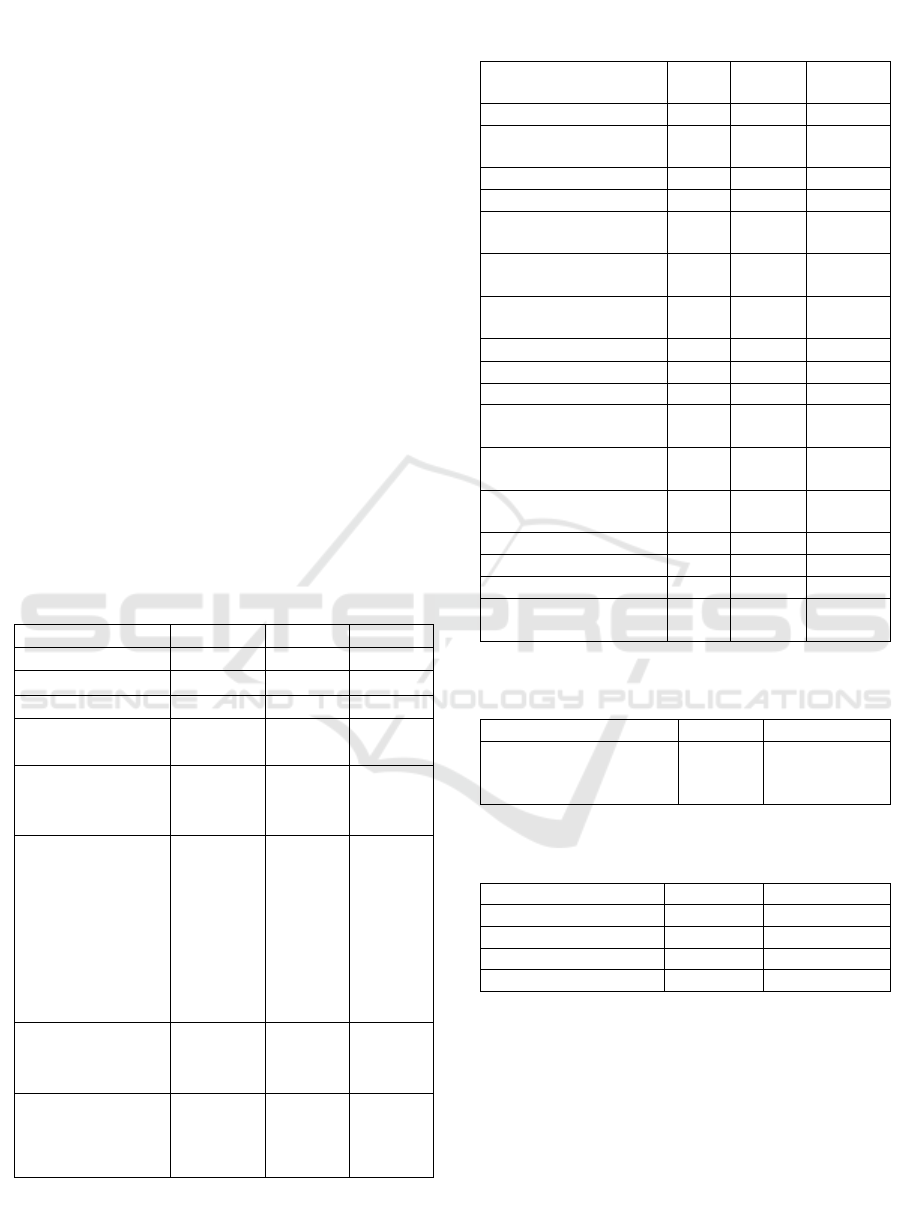
Table 1 reveals that the average age of respondents
was 54.38 years old. The mean of diabetes duration
was 3.92 years. All of the respondents were Moslem.
The number of female (63.1%) was more than male
(36.9%). The last education level of most
respondents was an elementary school (35.7%). All
of respondents were married. Most of the
respondents were still working (88.1%).
3.2 Spirituality
Table 2 indicates that the average value of
spirituality was 70.25. The minimum value was 61
and the maximum value was 81. The indicator of
spirituality that had the highest value was the
presence of God and indicator with the lowest value
was accepting others. Table 3 shows that majority of
respondents had spirituality in high category
(83.3%). Table 4 described that nearly three-quarters
of respondents stated that they felt very close to God.
3.3 Coping Strategy
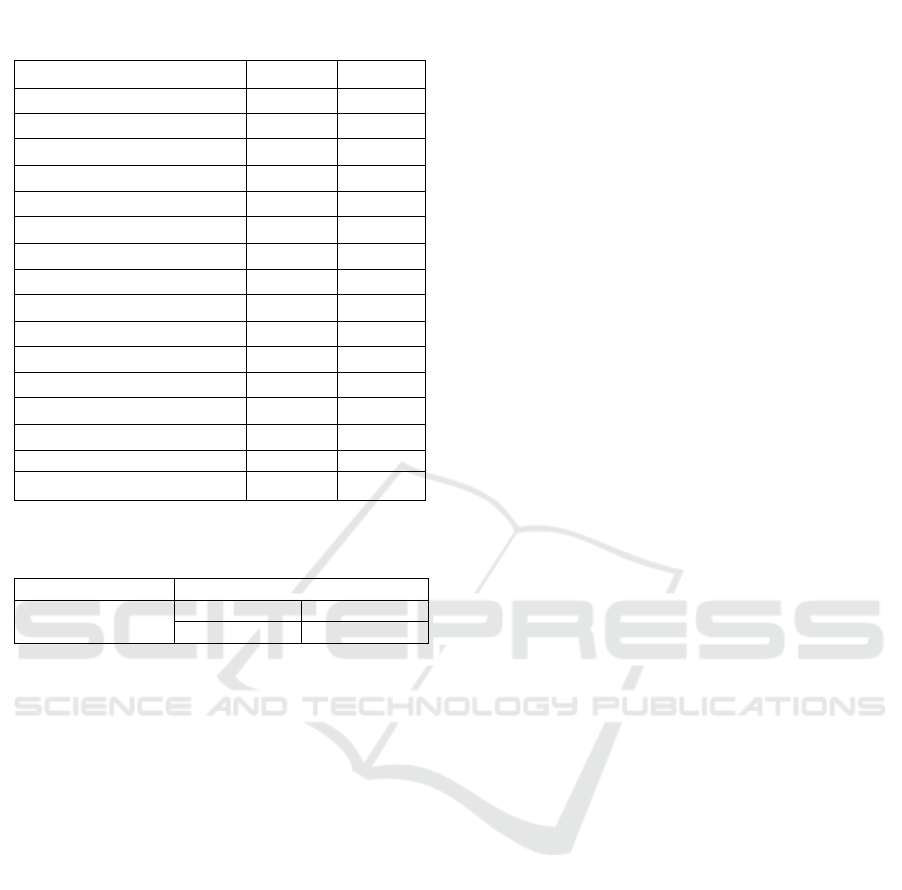
Table 5 shows the average value of coping strategy
was 75.88 with a standard deviation of 6.19. The
indicator of coping strategy that had the highest
value was religious coping and indicator with the
lowest value was the use of emotional support.
Table 1: Characteristic of type 2 DM patients (n: 84).
Characteristic
Mean
SD
Age
54.38
7.24
Diabetes Duration
3.92
2.32
n
%
Religion
Moslem
84
100
Gender
Male
Female
31
53
36.9
63.1
Education Level
None
Elementary
School
Junior High
School
Senior High
School
University
8
30
22
21
3
9.5
35.7
26.2
25
3.6
Marital status
Single
Married
0
84
0
100
Employment
status
Employed
Unemployed
74
10
88.1
11.9
Table 2: Mean value of spirituality in type 2 DM
patients (n: 84).
Variable
Mean
Median
Min-
max
Spirituality
70.25
71
61-81
Indicator of
Spirituality
5.33
5
3-6
Connection to all life
4.62
5
3-6
Joy connecting with
God
4.87
5
3-6
Strenght in
religion/spirituaity
4.71
5
3-6
Comfort in
religion/spirituaity
4.70
5
3-6
Deep inner peace
4.67
5
4-6
A
4.67
5
3-6
Guided by God
4.74
5
3-6
F
directly
4.58
5
3-6
F
through others
4.58
5
3-6
Touched by the beauty
4.46
5
3-6
thankful for blessings
4.56
5
3-6
Selfless caring
4.30
4
3-6
Aaccept others
4.20
4
3-6
Desire to be closer or
in union with God
4.80
5
3-6
Table 3: Distribution of Spirituality Levels in Type 2
DM patients (n: 84).
Spirituality level
n
%
Low
Moderate
High
0
14
70
0
16,7
83,3
Table 4: Feeling of Closeness to God in type 2 DM
patients( n: 84).
Closeness to God
n
%
Not close at all
0
0
Somewhat close
15
17.9
Very close
61
72.6
As close as possible
8
9.5
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
460
3.4 Correlation between Spirituality
and Coping Strategy in Type 2 DM
Patents
Table 6 shows that Spearman rank correlation test
obtained a p-value of 0.001 and r-value of 0.616. It
indicates a significant positive correlation between
spirituality and coping strategy which means the
higher the spirituality the better the coping strategy.
4 DISCUSSION
4.1 Spirituality
The result shows that the average value of
spirituality was 70.25 and majority of respondents
had spirituality in high category (83.3%). Along with
the stage of individual development, it will be
followed by the development of spirituality that
begins from infants to the elderly (Carson and
Koenig, 2008). The stage of development has a close
relationship with physical growth and individual
spirituality. When entering the age of an adult,
individuals will experience spiritual maturity
(Jalaluddin, 2015). The average age of respondents
in this study was 54.38 years. This age included in
the age of adulthood so that the spirituality develops
better along with the increasing age.
Another factor that can affect spirituality is
cultural background. In general, individuals will
follow the spiritual and religious traditions
performed by each family. Traditions can include
prayer or other activities related to religion (Hamid,
2008). The results showed the value of spirituality in
this study was high, it can be related with traditions
to perform obligations in Islamic religious culture
such as praying and following other religious
activities.
Another factor affecting spirituality is crisis and
change (Hamid, 2008). Diabetes is one of the chronic
diseases that affect the changes in a person.
Spirituality affects the way patients deal with the
complications of illness as a mediating factor when
adapting to overcome the challenge of change (Baby
and Khan, 2015). When an individual faced with
death they will have spiritual beliefs as well as a
desire in worship and more praying (Hamid, 2008).
This factor allows diabetic patients in this study to
experience spiritual improvement.
This study shows the indicator of spirituality that
has the highest value is the presence of God. This is
these conditions, respondents feel the presence of
God and assert that they are not alone (Underwood,
2006). In addition, the result also indicates that
almost three-quarters of respondents stated that they
felt very close to God. Spending time with God and
awareness of the presence of God will be able to
change the perspective of the individual in facing a
challenge and consider the difficulty as a trial
(Girardot, 2010). The presence of God is a spiritual
experience that is used as a lesson to promote a more
conducive awareness (Pretorius, 2008).
The indicator of spirituality with the lowest value
was accepting others. Accepting others is a feeling of
mercy and acceptance of others even when making
mistakes (Underwood, 2006). This is shown by the
statement "I accept others even when they do things
that I think are wrong". Research in diabetes patients
revealed a lower value of the dimensions of
relationship with others than the religious dimension
(Baby and Khan, 2015). Relationships between
others can arise from the desire of appreciation and
respect for others, the desire to do good things, the
need for justice, and the fear of feeling lonely
(Ningrum, 2014).
Table 5 : Mean value of coping strategy in type 2 DM
patients (n: 84).
Variable
Mean
SD
Coping strategy
75.88
6.19
Indicator of Coping
Self-diversion
2.68
0.53
Active coping
3.01
0.37
Use of help
2.60
0,43
Planning
3.10
0.39
Acceptance
2.68
0.41
Religious coping
3.11
0.40
Humor
2.70
0.65
Positive reinterpretation
2.95
0.34
Denial
2.63
0.43
Substance use
2.85
0.42
Use of emotional support
2,14
0.40
Helplessness
2.51
0.67
Disengagement
2.43
0.75
Self-blame
2.25
0.70
Table 6: Correlation between spirituality and coping
strategy in type 2 DM patients (n=84) .
Variable
Coping strategy
Spirituality
r
0.616
p value
0.001
Correlation between Spirituality and Coping Strategy in Patients with Type 2 Diabetes Mellitus
461

4.2 Coping Strategy
The results showed that the average value of coping
strategy is 75.88. In general, a person's experience
will be able to increase his role in solving problems
and become more capable in overcoming
encountered difficulties. As getting older, someone
will be faced with many problems. Through this
process, an individual can understand the type of
coping strategies that are less effective or effective
and can achieve its goals in various situations
(Aldwin, 1991). A study mentioned that DM patients
with the age group of 50 to 69 years are more
actively motivated to overcome the problem so that
the ability to cope will be better (Hara et al., 2014).
The average age of respondents in this study was
54.38 years which included in the group of age that
have an active motivation to overcome problems.
There were more women than men in this study.
Gender has an influence on a person in overcoming
illness, stress, and the use of coping in solving health
problems (Yeh et al., 2009). Women reported using
more adaptive coping than men (Gentry et al., 2007).
Women have more adaptive coping than men
because women connect more with belief as the
control in dealing with stress (Kelly et al., 2007).
Another factor that may affect the coping of
respondents is the marital status in which all the
respondents in this study are married. DM patients
who have good family support will have better
coping (Saltzman and Holahan, 2002).
The indicator of coping strategy that has the
highest score in this research is religious coping.
This value was obtained from the respondent's
answer in the statement "after I was diagnosed with
diabetes mellitus, I am getting closer to God" and "I
do not forget to pray for my recovery". Individuals
use religious coping when they are under pressure
for various reasons. In this context, religion works as
a source of emotional support, media of
reinterpretation, and active coping with stressors
(Carver, Scheier and Weintraub, 1989). Religious
coping is manifested by individual efforts to find
spiritual or religious beliefs such as meditation and
prayer (Carver, 1997).
Religious beliefs and practices play a role in
giving a better sense of control, hope, and adaptation.
Common practices such as prayer are the most
common forms of coping strategies used in religion
(Malhotra and Thapa, 2015). Type 2 diabetes
patients use religious coping to manage and
understand the disease. This is significantly related
to their level of involvement in glucose control
activities (Fincham, Seibert and May, 2017).
The indicator of coping strategy that has the
lowest score in this research is the use of emotional
support. This score was obtained from the answer to
the statement "when I was diagnosed with diabetes
mellitus I received support from my family" and
"although I have diabetes mellitus I gain comfort and
acceptance in my family". Similar results also
suggest that DM patients in Turkey use lower
emotional support (Tuncay, Musabak and Kutlu,
2018). The use of emotional support is manifested by
activities such as talking to others about feelings,
trying to gain support from friends or relatives,
discussing feelings with others, and gaining the
sympathy and understanding of others (Carver,
Scheier and Weintraub, 1989). Support from family
affects the health of DM patients. Unsupportive
behavior is associated with poor treatment, one of
which is characterized by poor glucose control.
Diabetic patients need emotional support as a support
system in order to develop an adaptive coping. DM
patients who do not get support from family
members will have an impact on the patient's non-
compliance with DM treatment (Mayberry and
Osborn, 2012).
4.3 Correlation between Spirituality and
Coping Strategy
The result reveals a significant positive correlation
between spirituality and coping strategy in patients
with type 2 DM. This indicates that the higher the
spirituality of patients the better the coping strategy.
Patients with type 2 diabetes look for meaning in
their diagnosis. They assume that illness is a trial
from God that is similar to the other problems they
face during life. They think that they should be
patient and tolerant of this God-given test.
Spirituality gives meaning to disease and increases
coping in overcoming stress caused by the diagnosis
of DM. Patients with type 2 DM become more
oriented to spirituality after diagnosis of the disease.
They consider spirituality as a powerful source to
overcome the illness. Spirituality can make patients
more focused, strong, dynamic and help them in
overcoming the problem of the disease
(Aghamohammadi, 2017). Spirituality can help
humans in searching for meaning and purpose in life
to gain hope, love, inner peace, comfort and support
(Saad and Medeiros, 2012).
Coping strategy can be done through practice and
belief as part of spirituality. Spirituality is also
integrated into reasoning and problem-solving
techniques through an approach that serves as a
coping strategy for managing disease and reducing
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
462

potential stress such as pain and helplessness
(Harvey, 2008). Spiritual needs are assessed in the
context of health such as finding meaning and
purpose in life and recognizing the importance of
good relationships with others, transcendent strength
and the natural environment (Greenstreet, 2006).
Spiritual factors contribute positive activity to
behavioral changes and individual motivations that
impact on lifestyle changes in achieving blood
glucose control (Wibisono, 2012). Controlled blood
glucose levels will prevent further complications of
DM (Kurniawan, 2010).
Awareness of the positive meaning gained from
every situation and the awareness of God's power
indicates that the individual has good spiritual
integrity. This awareness makes a stable emotional
state and a symbol of positive behavior. Good
emotional state has a negative correlation with
depression, anxiety, and other psychological distress
due to health problems (Newlin et al., 2003).
DM patients mentioned that they ultimately
decided to make efforts to improve behavior due to
consciousness from a religious point of view.
Patients stated that the motivation of worship made
them aware and tried to improve their lifestyle
(Wibisono, 2012). DM patients who were desperate
and did not care about their diet changed after
reading the warning from the holy book (Salehi,
Ghodousi and Ojaghloo, 2012). There is a negative
relationship between belief in God, religious
guidance and the power of prayer with the incidence
of depression. This indicates that spiritual influence
changes in motivation and behavior of patients
(Doolittle and Farrell, 2004).
The belief systems and religious beliefs play an
important role in spiritual development. Patients with
type 2 diabetes believe that sickness and health are
God's will. Based on religious tradition, God loves
His creation, therefore, people must be patient when
facing the problem including the disease. Spiritual
belief can affect mental and physical balance in DM
patients (Aghamohammadi, 2017). Spiritual
practices such as prayer and visiting places of
worship can provide coping support in self-
management (Polzer and Miles, 2005). Patients who
are obedient to faith have good welfare and show
more positive coping strategy (Dehning et al., no
date). Adaptive coping can improve glucose control
and prevent complications (Turan et al., 2002).
5 CONCLUSIONS
There is a significant positive correlation
between spirituality and coping strategy in patients
with type 2 DM. The higher the spirituality of
patients the better the coping strategy. Assessing
spiritual aspect of patients and adding spiritual
approach in caring DM patients is required to
optimize the coping strategy of type 2 DM patients.
REFERENCES
Journal of Research Development in Nursing &
Midwifer, 14(2), pp. 3444. Available at:
https://www.researchgate.net/publication/320196552_
Spiritual_Growth_in_Patients_with_Type_II_Diabetes
_Mellitus_A_Qualitative_Study.
Coping Process? Implications of Age Differences in
J Gerontol, 46(4), pp. 174180.
Available at:
https://www.ncbi.nlm.nih.gov/pubmed/2071843.
-Being
International Journal of
Indian Psychology, 3(4), pp. 6571. Available at:
http://www.ijip.in/Archive/v3i4/18.01.141.20160304.p
df.
Carson, V. B. and Koenig, H. G. (2008) Spiritual
Dimensions of Nursing Practice (Templeton Science &
Religion). West Conshohocken: Templeton Foundation
Press.
International Journal of Behavioral Medicine, 41(2),
pp. 92100. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/16250744
Carver, C. S., Scheier, M. F. and Weintraub, J. K. (1989)
ally Based
Journal of Personality and Social
Psychology, 56(2), pp. 267283. Available at:
http://psycnet.apa.org/record/1989-17570-001.
Chew, B. H., Ghazali, S. S. and Fernandez, A. (2014)
behavioral change in patients. World Journal of
World Journal of Diabetes, 5(6). doi:
10.4239/wjd.v5.i6.796.
Dehning, D. O. et al. (no date) Does Religious Adherence
Help Diabetic Patients’ Well-Being?, 2013. Available
at: http://stage.teleiosresearch.com/wp-
content/uploads/2017/07/CV-408-Religion-and-
diabetes-JCN-2013.pdf.
between Spirituality and Depression in an Urban
Prim Care Companion J Clinic Psychiatry,
6(3), pp. 114118. Available at:
Correlation between Spirituality and Coping Strategy in Patients with Type 2 Diabetes Mellitus
463

https://www.ncbi.nlm.nih.gov/pmc/articles/PMC47473
4/pdf/i1523-5998-6-3-114.pdf.
Fincham, F. D., Seibert, G. S. and May, R. W. (2017)
Journal of marital and family
therapy, pp. 112. Available at:
http://www.fincham.info/papers/2017-jmft12241.pdf.
Gentry, L. A. et al.
Californian Journal of Health Promotion, 5(2), pp. 89
102. Available at:
http://www.cjhp.org/Volume5_2007/Issue2/089-102-
gentry.pdf.
fe and Music
National Association of Pastoral Musicians, pp. 18.
Available at: http://npm.org/wp-
content/uploads/2017/07/SpiritualLifeGirardot.pdf.
Graham, S. et al.
copiCounseling and Values, 46, pp. 2
13. Available at: http://onlinelibrary.wiley.com.
British
Journal of Nursing, 15(17), pp. 938942. Available at:
https://www.magonlinelibrary.com/doi/abs/10.12968/b
jon.2006.15.17.21909?journalCode=bjon.
Journal of
diabetes spectrum, 13(3), p. 167. Available at:
http://journal.diabetes.org/diabetesspectrum/00v13n3/p
g167.htm.
G
Spirituality in Diabetes Self-Management in an Urban,
Underserved Population: A Qualitative Exploratory
Rhode Island medical journal, 97(3), pp. 31
35. Available at:
http://www.rimed.org/rimedicaljournal/.
Hamid, A. Y. (2008) Bunga Rampai Asuhan Keperawatan
Kesehatan Jiwa (Nursing Care of Mental Health).
Jakarta: EGC.
Hara, Y. et al.
Support, and Treatment on Perceived Stress and
Coping of Patients with Type 2
BioPsychoSocial Medicine, 8(16), pp. 111. doi:
10.1186/1751-0759-8-16.
Perspectives, pp. 112129. Available at:
http://www.rcgd.isr.umich.edu/prba/perspectives/sprin
g 2008/Harvey.pdf.
Spirituality in the Self-management of Chronic Illness
J Cross Cult
Gerontology, 22(2), pp. 205220. Available at:
https://www.ncbi.nlm.nih.gov.
Indonesia Ministry of Health (2013) Basic Health
Research. Available at:
http://www.depkes.go.id/resources/download/general/
Hasil Riskesdas 2013.pdf.
International Diabetes Federation (2015) Diabetes Atlas -
7th Edition. Available at:
http://www.diabetesatlas.org/resources/previous-
editions.html.
Spirituality and Its Underlying Factor at Majelis
Intizar,
21(2), pp. 165183. Available at:
http://download.portalgaruda.org/.
Karomah, N. N. (2015) Correlation between the Spiritual
Level and the Anxiety of Death in Elderly with Chronic
Illness. Diponegoro University. Available at:
http://eprints.undip.ac.id.
Kelly, M. A. R. et al. ship between
beliefs about depression and coping strategies: Gender
British Journal of Clinical Psychology,
46, pp. 315332. doi: 10.1348/014466506X173070.
Usia [Type 2 Diabetes Mellit Majalah
Kedokteran Indonesia, 60(12), pp. 576584. Available
at:
https://silver0zero.files.wordpress.com/2013/04/511-
570-1-pb.pdf.
International Journal of
Multidisciplinary and Current Research, 3, pp. 613
619. Available at: http://ijmcr.com/wp-
content/uploads/2015/07/Paper36613-619.pdf.
Support, Medication Adherence, and Glycemic Control
Diabetes Care,
35(6), pp. 12391245. doi: 10.2337/dc11-2103.
Moasheri, B. et al.
Styles in Type 2 Diabetic Patients and their
Health
Education & Health Promotion, 5(4), pp. 5563.
Available at: http://hehp-
old.modares.ac.ir/article_18195.html.
Kualitas Hidup Penderita Diabetes Mellitus
[Spirituality and Quality of Life of Diabetes Mellitus
Prosiding Seminar Nasional
Keperawatan Komunitas, pp. 289294. Available at:
http://eprints.undip.ac.id/47394/.
Newlin, K. et al.
and Health Outcomes in Black Women with Type 2
Ethicity & Disease, 13(2), pp. 6168.
Available at:
https://www.ncbi.nlm.nih.gov/pubmed/1272301
Ningrum, A. W. (2014) The Spirituality Level of Patients
with Diabetes Mellitus at Puskesmas Kampung Baru
Medan. Universitas Sumatra Utara. Available at:
http://repository.usu.ac.id.
-
Journal of Holistic Nursing, 23(2), pp. 230250.
Available at:
http://journals.sagepub.com/doi/abs/10.1177/08980101
05276179?journalCode=jhna.
Acta Theologica
Supplementum, 28(11), pp. 147165. doi:
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
464

10.4314/actat.v28i2.105667.
Rahmaturrizqi (2012) The Effect of Coping Strategies on
the Level of Depression in Patients with Diabetes
Mellitus in the Working Area Lhoksukon Heal. UIN
Maulana Malik Ibrahim Malang. Available at:
http://etheses.uin-malang.ac.id/2172/.
-Religious
Coping
Complementary Therapies for the
Contemporary Healthcare. Intech, pp. 127144. doi:
10.5772/50445.
Salehi, S.,
Spiritual Experiences of Patients with Diabetes- related
Iran Journal Nurse and Midwifery
Research, 17(3), pp. 225228. Available at:
https://www.researchgate.net/publication/247153497_
The_spiritual_experiences_of_patients_with_diabetes-
_related_limb_amputation.
Support, Self-Efficacy, and Depressive Symptoms: An
Journal of Social and Clinical
Psychology, 21(3), pp. 309322. Available at:
https://guilfordjournals.com/doi/abs/10.1521/jscp.21.3.
309.22531.
Samuelhodge, C. D. et al. -to-
Day Self-Management of Type 2 Diabetes Among
African-American Women: Spirituality, the multi-
caregiver role, and other social
Diabetes care, 23(7), pp. 928933. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/1089584
Saputra, O. et al.
Jurnal Agromedicine, 4(1), pp. 713. Available at:
http://juke.kedokteran.unila.ac.id/index.php/agro/articl
e/view/1542.
Shahrbabaki, P. M. et al.
International
Journal of Community Based Nursing and Midwifery,
5(1), p
.
Stuart, G. W. (2013) Principles and Practice of
Psyachiatric. 10th edn. Louis Missouri: Elsevier
Mosby. Available at: https://books.google.co.id.
Relationship between Anxiety, Coping Strategies and
Health and
Quality of Life Outcomes, 6(79), pp. 19. Available at:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC25725
93/pdf/1477-7525-6-79.pdf.
Turan, B. et al.
in Adherence to Treatment Regimen and Disease
Control in Type 1 and Insulin Treated Type 2 Diabetes
Diabetes & Metabolism, 28(3), pp.
186193. Available at: http://www.em-
consulte.com/en/article/80104.
Qualitative Research, Interpretive Guidelines, and
Population Distribution for the Daily Spiritual
Archive for the Psychology of
Religion/ Archivfür Religions psychologie, 28(1), pp.
181218. Available at:
http://www.dsescale.org/OrdSpirExp.pdf.
Spiritual Experience Scale: Development, Theoretical
Description, Reliability, Exploratory Factor Analysis,
and Preliminary Construct Validity Using Health-
Annals of Behavioral Medicine, 24(1),
pp. 2223. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/1200879
Wibisono, A. H. (2012) Experience of Client with Type 2
Diabetes Mellitus. Universitas Indonesia. Available at:
http://lib.ui.ac.id/file?file=digital/20317905-T31564-
Pengalaman klien.pdf.
Yeh, S. J. et al.
Sex
Roles, 60, pp. 4456. Available at:
https://link.springer.com/article/10.1007/s11199-008-
9515-2.
African Journal of
Diabetes Medicine, 20(1), pp. 57. Available at:
www.africanjournalofdiabetesmedicine.com.
Zareipour, M. et al.
Spiritual Health and Blood Sugar Control in Elderly
Elderly Health
Journal, 2(2), pp. 6772. Available at:
http://ehj.ssu.ac.ir/article-1-66-en.pdf.
Correlation between Spirituality and Coping Strategy in Patients with Type 2 Diabetes Mellitus
465
