
A Model Driven Approach to the Development of Gamified Interactive
Clinical Practice Guidelines
Job N. Nyameino
1,3
, Fazle Rabbi
2
, Ben-Richard Ebbesvik
2
, Martin C. Were
3,4,5
and Yngve Lamo
2
1
Department of Informatics, University of Bergen, Bergen, Norway
2
Department of Computing, Mathematics, and Physics, Western Norway University of Applied Sciences, Bergen, Norway
3
Institute of Biomedical Informatics, Moi University, Eldoret, Kenya
4
Department of Biomedical Informatics, Vanderbilt University Medical Center, Nashville, TN, U.S.A.
5
Vanderbilt Institute for Global Health, Vanderbilt University Medical Center, Nashville, TN, U.S.A
Keywords:
Clinical Practice Guidelines, Model Driven Engineering, Gamification.
Abstract:
Clinical practice guidelines (CPGs) play a fundamental role in modern medical practice since they summarize
the vast medical literature and provide distilled recommendations on care based on the current best evidence.
However, there are barriers to CPG utilization such as lack of awareness and lack of familiarity of the CPGs
by clinicians due to ineffective CPG dissemination and implementation. This calls for research into effective
and scalable CPG dissemination strategies that will improve CPG awareness and familiarity. We describe a
formal model-driven approach to design and implement a gamified e-learning system for clinical guidelines.
We employ gamification to increase user motivation and engagement in the training of guideline content. Our
approach involves the use of models for different aspects of the system, an entity model for the clinical domain,
a workflow model for the clinical processes and a game model to manage the training sessions. A game engine
instantiates a training session by coupling the workflow and entity models to automatically generate questions
based on the data in the model instances. Our proposed approach is flexible and adaptive as it allows for easy
updates of the guidelines, integration with different device interfaces and representation of any guideline.
1 INTRODUCTION
Medical knowledge is increasing at an exponential
rate and it is difficult for clinicians to keep up with
this quantity of knowledge production (Fervers et al.,
2010). The development and use of clinical prac-
tice guidelines (CPGs) is a promising solution to this
problem. CPGs are systematically developed state-
ments that assist practitioners and patients to make
decisions about appropriate health care for specific
circumstances (Lohr et al., 1992). Guidelines are
a comprehensive summary of the available evidence
about medical conditions and provide recommenda-
tions for the management of those conditions (Goud
et al., 2009). A well-developed guideline reduces
variations in care, improves diagnostic accuracy, pro-
motes effective therapy and discourages ineffective
therapies all which contribute to improved quality of
care (Shiffman et al., 2004). The mere availability
of guidelines does not necessarily mean that the rec-
ommendations will be used in actual care. Indeed,
there has been a reported gap between recommended
care according to the evidence base and actual prac-
tice leading to preventable errors in practice (Donald-
son et al., 2000; Baker, 2001). This gap can be at-
tributed to several barriers to guideline dissemination
and implementation which include: internal barriers
(lack of awareness, lack of familiarity, lack of agree-
ment with the guideline content, and the inability to
overcome the inertia of previous practice) and exter-
nal barriers (i.e., patient, environmental, and guide-
line related factors such as ease of use and complexity
of the guideline) (Cabana et al., 1999).
The nature of guideline development means that
published guidelines are well-researched, compre-
hensive documents that can be prohibitively volumi-
nous. For example, the National Heart, Lung, and
Blood Institute (NHLBI) 2007 Guidelines for the Di-
agnosis and Management of Asthma full report is 440
pages long (NHLBI, 2007) while the National Insti-
tute for Health and Care Excellence (NICE) guide-
lines for the diagnosis monitoring and management of
chronic asthma (2017) report is 39 pages long (NICE,
2017). Such large texts are impractical for use at the
Nyameino, J., Rabbi, F., Ebbesvik, B., Were, M. and Lamo, Y.
A Model Driven Approach to the Development of Gamified Interactive Clinical Practice Guidelines.
DOI: 10.5220/0007736401470158
In Proceedings of the 14th International Conference on Evaluation of Novel Approaches to Software Engineering (ENASE 2019), pages 147-158
ISBN: 978-989-758-375-9
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
147

point of care. Additionally, poor guideline presenta-
tion has been identified as a factor in the lack of physi-
cian familiarity as some of the guidelines have been
described as being tedious, repetitive, confusing, and
unclear (Cabana et al., 2000).
To mitigate some of the barriers to knowledge
acquisition of guideline content, new dissemination
strategies aimed at improving awareness and famil-
iarity of guideline content are required. Active guide-
line dissemination strategies have been found to be
more effective than passive strategies at improving
the application of evidence based recommendations
in patient care (Grimshaw et al., 2012). In par-
ticular, educational interventions (e.g. distribution
of printed guidelines, educational meetings and out-
reaches) strengthen the effect of clinical educational
material. Further, the more intensely the information
is provided through these interventions, the greater its
effect on the recipients (Marriott et al., 2000). Re-
search into active strategies for clinical guideline dis-
semination are timely and relevant as they will poten-
tially help to plug the gap between recommended and
actual clinical practice.
One potentially useful active educational inter-
vention is in the distribution of gamified guidelines.
Gamification is the use of game design elements in
non-game contexts (Deterding et al., 2011b; Deter-
ding et al., 2011a). It uses game based mechanics,
aesthetics and thinking to engage people, motivate
action, promote learning and solve problems (Kapp,
2012). The concept of Gamification is relatively new
and has been used to describe the use of game-based
concepts and techniques, with the goal of increasing
the motivation and engagement of the participants and
improving the results.
The implementation of guideline summaries as in-
teractive, gamified flowcharts on a mobile platform
will potentially mitigate the problems of guideline
complexity and presentation that plague the effective
dissemination of guideline content. In this paper we
present a formal model driven approach to gamifica-
tion of clinical practical guidelines. To illustrate the
approach, we present three models, an entity model of
the clinical encounter domain, a workflow model for
the clinical processes and a game model all of which
will be integrated to create our gamified system. We
also describe a prototype mobile-based guideline app
that incorporates these models to present a gamified
interactive guideline training tool.
The rest of the paper is organized as follows: In
section 2 we give an introduction to the Diagram
Predicate Framework (DPF) and show how it can be
used for modelling CPGs workflows and entity mod-
els for the clinical domain. Moreover, we illustrate
how the guideline workflow information is synchro-
nized with the domain information. In section 3 we
introduce our approach to gamification of workflows
and discuss in further detail the use of the different
models in our design. In section 4 we describe the
implementation of our approach in the development
of the prototype system. Finally in section 5 we com-
pare our approach to other works before we conclude
the paper and envision further work in section 6.
2 BACKGROUND
In this work we use a formal diagrammatic approach
to model driven software engineering (MDE), called
Diagram Predicate Framework (DPF). MDE is a sys-
tem development paradigm that promotes the use of
models as the primary artefacts that drives the whole
development process. In MDE models are specified
using a modelling language whose syntax and seman-
tics are defined by a metamodel (Rodrigues da Silva,
2015). This allows for the development of domain-
specific modelling languages (DSLs) using notations
and abstractions that are unique to a given domain.
The use of DSLs allows for the development of more
expressive models and ease of use by domain experts.
In this section we provide an overview of how di-
agrammatic models can be created using DPF. We
chose to use DPF as it can be used to create cus-
tom domain specific modelling languages. Further-
more, we’ll present a metamodel for representing a
CPG workflow, a simple entity model for the medical
domain, a model for the game engine and finally an
integrated multi-metamodel that incorporates the en-
tity and CPG workflow models. UML is another al-
ternative approach for the modeling of various kinds
such as UML entity model, sequence model. How-
ever, DPF allows us to do multilevel metamodeling
and also visualizes constraints in the models.
2.1 Diagram Predicate Framework
(DPF)
DPF formalizes software development activities such
as metamodelling (Rutle et al., 2009) and model
transformations (Rutle et al., 2012) based on category
theory (Barr and Wells, 1990) and graph transforma-
tions (L
¨
owe, 1993). By applying DPF we can formal-
ize clinical guidelines and clinical domain models at
different abstraction levels in form of diagrammatic
specifications. The diagrammatic nature of DPF also
facilitates visual representations of guidelines that can
be presented at different level of abstraction. A model
in DPF is represented by a diagrammatic specification
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
148
Treatment
TreatmentName
treatmentName
Age
Weight
Patient
hasAge
hasWeight
History&Examination
Finding
hasFinding
Diagnosis
DiagnosisName
Severity
hasSeverity
diagnosisName
receives
hasTreatment
hasDiagnosis
conductedOn
PatientName
hasName
Symptom
hasSymptom
Plan
hasPlan
[pre-cond]
Gender
hasGender
Figure 1: A simplified entity model of the clinical encounter domain.
S = (S ,C
S
: Σ) which consists of a graph S and a set
of constraints C
S
specified by a predicate signature
Σ.
The predicate signature is composed of a collec-
tion of predicates, each having a name and an arity
(shape graph). A constraint consists of a predicate
from the signature together with a binding to the sub-
graph of the model’s underlying graph which is af-
fected by the constraint. In order to apply DPF for the
modeling of a game that operates over clinical prac-
tice guideline we need to formalize the concepts of a
guideline using DPF and also model the gamification
concepts with DPF. In the following subsection we
present how DPF can be used to model different as-
pects of guidelines and representing the concepts for
gamification.
2.2 Entity Modelling
We will now present an entity model of the clinical
domain. To do this we use a metamodel contain-
ing Concepts, Attributes and References. An actual
model typed over this metamodel is shown in Fig-
ure 1. We have concepts and corresponding rela-
tions for domain entities such as Patients, Diagnosis,
Treatments etc (see Figure 1). The model consists
of a constraint modeled with a predicate named ‘pre-
condition’ and visualized with symbol [pre − cond].
The constraint specifies that all the treatment in-
stances must have a reference to a diagnosis instance.
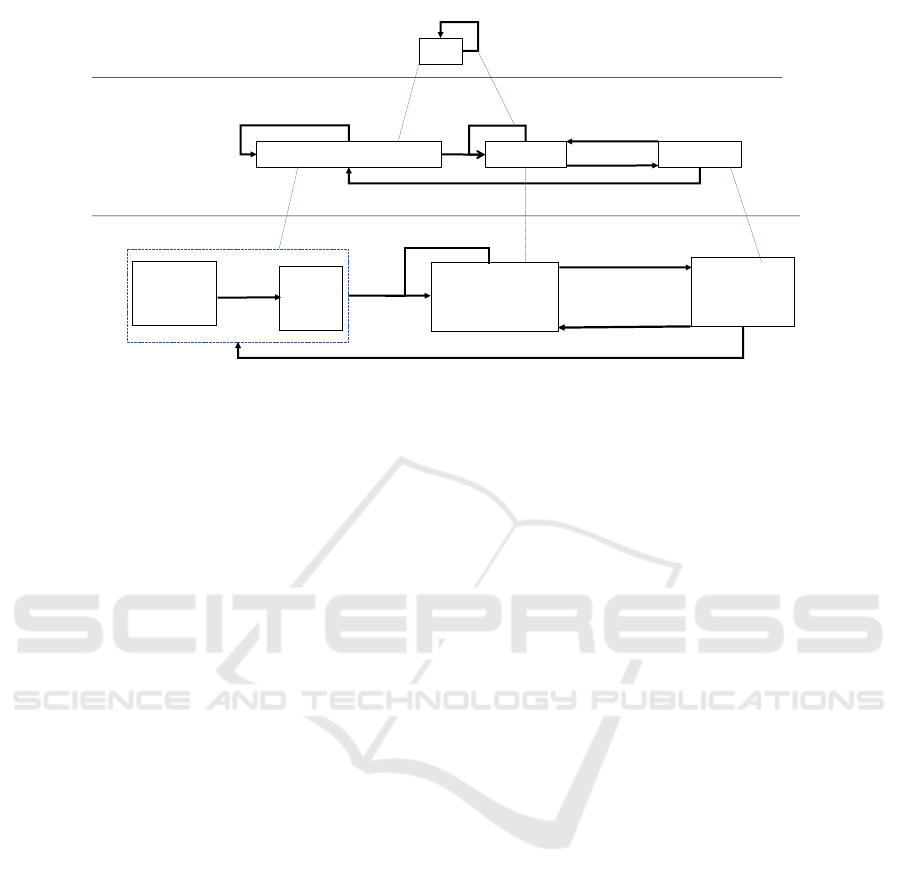
2.3 Workflow Modelling
Clinical practice guidelines often consist of a flow of
information. Workflow models may be used to repre-
sent the flow of a guideline. In Figure 2 below we see
an example metamodel (M
2
) for behavioural models,
where Tasks can be connected by Flow edges. On the
next abstraction level (M
1
) we see a generic treatment
model that is typed by the flow model. The treat-
ment model has three tasks Assessment and Diagno-
sis, Treatment and Evaluation. Finally, at (M
0
) we
see an instance of the treatment workflow of a severe
asthma diagnosis.
2.4 Game Modelling
At their core, games are goal-oriented activities with
reward and progress tracking mechanisms. The de-
sign of gamified e-learning systems should be under-
taken in the view of these core concepts. In our sys-
tem, the training will be done through a series of ques-
tions based on the guideline content. The game en-
gine in our model automatically generates questions
from the entity and workflow models to instantiate a
training module. The questions are categorized ac-
cording to the learner’s skill level (beginner, interme-
diate, advanced) and each question has a reward in the
form of points. A game model should also specify a
learner profile that tracks the learner’s activities.
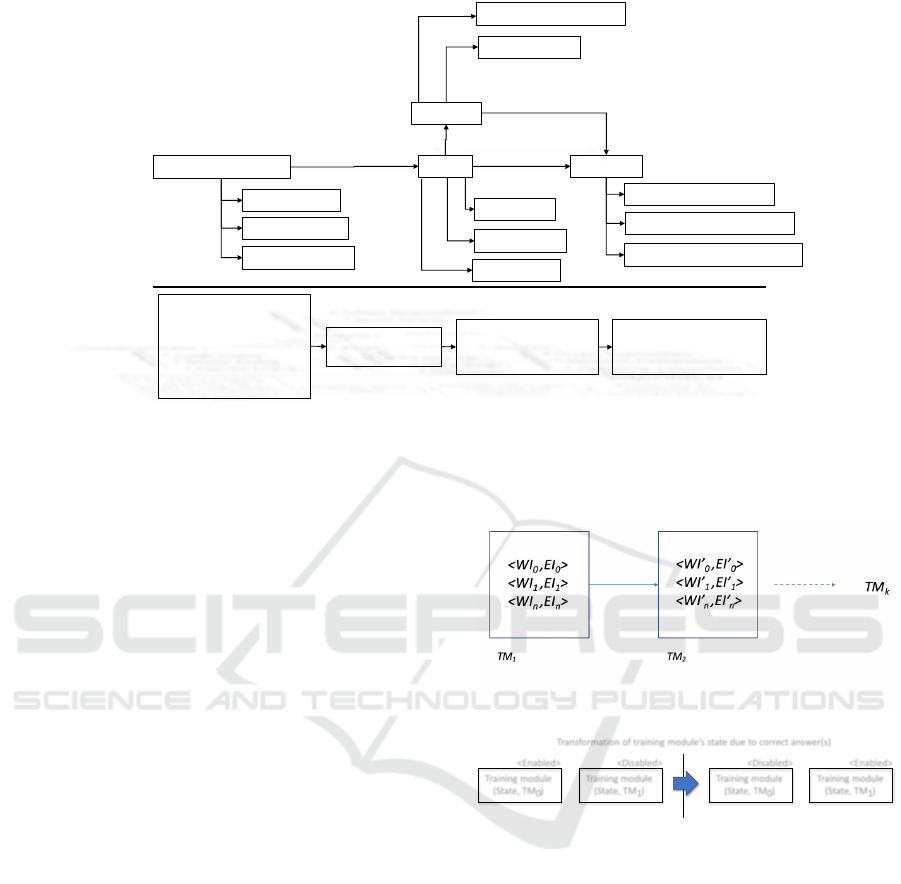
2.5 Integrating Models
The training model is built by the integration of the
entity and workflow models based on the principles
introduced by Rabbi et al (Rabbi et al., 2014a). The
states of the training module T M are defined by a set
of elements that include a pair of workflow instance
W I and an entity instance EI: T M
i
=< EI
i
,W I
i
>
where i is a natural number. This integration of mod-
els is shown in Figure 3 and the concept is discussed
in more details in section 3. In Figure 3, we show a
A Model Driven Approach to the Development of Gamified Interactive Clinical Practice Guidelines
149
Task
flow
Assessment and Diagnosis
Treatment
Evaluation
Severe
Asthma
Re-evaluate
After 20 min
Oxygen
Salbutamol
Prednisolone
Cough +
Wheeze +
Cyanosis
Adjust treatment
Reassess patient to update diagnosis
M
2
M
1
M
0
Re-treat
Figure 2: The workflow model with its metamodel.
section of the entity model with values from a given
scenario where based on the History & Examination
findings, a Diagnosis of Severe Asthma is made and
its Treatment specified. The flow of how this process
should happen is shown in the workflow model.
3 PROPOSED METHOD
3.1 Gamification Elements
The core concepts of games that should inform the
design of gamified e-learning systems are goal ori-
ented activities with reward mechanisms and progress
tracking (Strme
ˇ
cki et al., 2015). In the training of
guideline content, the main goal is for the trainees to
learn how to treat different aspects of a disease as de-
scribed in the guideline. The reward mechanisms and
progress tracking aid in increasing the users engage-
ment and motivation (Bernik et al., 2018).
3.2 CPG Modelling
In our approach, we separate two aspects from a clini-
cal practice guideline (CPG). Medical conditions and
clinical encounters of patients is one aspect which we
model in an entity model; recommended clinical pro-
cesses is another aspect which we model in a work-
flow diagram. A flow in a guideline often consist of
medical conditions such as ‘start giving oxygen if a
child is convulsing for more than 5 minutes’. Typ-
ically a modeling approach specifies all the recom-
mended processes in a workflow diagram. An in-
stance of the diagram would then specify a concrete
scenario representing the care processes executed for
a patient.
In our approach, we skip modeling the general
recommendations in a workflow diagram and directly
specify concrete scenarios. For example, in our ap-
proach we model a scenario where a 2 year old boy
who is convulsing for 7 minutes is admitted to a hos-
pital and we start treatment by giving oxygen. We
follow this approach as it allows us to model concrete
scenario with less effort and we do not need to spend
time on encoding the whole guideline. Since the pur-
pose of modeling the guideline scenario is to generate
questions using our approach, it is sufficient for us
to model the scenario representing the recommended
clinical processes according to the guidelines. To rep-
resent such scenarios we integrate a CPG workflow
model with an entity model which is encoded as a
DPF model. Typically, a CPG consist of a large num-
ber of pages with information from the clinical do-
main. There exists some approaches that allows us to
design a visual model of a CPG.
In (Rabbi et al., 2014a; Rabbi et al., 2014b), the
authors presented an approach where different aspects
of a system were coordinated by means of multiple
metamodels. The approach is based on the foundation
of DPF.
In the multi-metamodeling approach, a workflow
model is integrated with an entity model by means of
metamodel coordination. A workflow metamodel is
used to design the flow of a system and an entity meta-
model used to design the entities and relationship of a
domain. A workflow model can be used to represent
an abstraction of a CPG but we need to incorporate the
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
150
:Treatment
Oxygen: TreatmentName
Salbutamol: TreatmentName
Prednisolone: TreatmentName
treatmentName
4 years: Age
16 Kg: Weight
:Patient
:hasAge
:hasWeight
:History&Examination
Cough: Finding
Wheeze: Finding
Cyanosis: Finding
:hasFinding
:Diagnosis
Asthma: DiagnosisName
Severe: Severity
:hasSeverity
:diagnosisName
:receives
:hasTreatment
:hasDiagnosis
:conductedOn
A 4yr old boy weighting
16 kg presents with a
history of cough, wheeze
and on examination he is
found to have central
Cyanosis
Diagnosis: Severe
ashma
Treatment with oxygen,
Salbutamol and
prednisolone
Reassess after 20
minutes and treat
according to new findings
Workflow Model, WI
Entity Model, EI
Male: Gender
:hasGender
Figure 3: Integrated entity and workflow models.
detailed domain knowledge in our modelling. In this
paper we exploit the use of the multi-metamodeling
approach to represent the domain knowledge of a clin-
ical guideline and the clinical process and apply them
to execute a training session. The idea of using the
CPG workflow model is to control the flow of the
game such that the user is interacting with the right
gaming element at the right time.
In this section we explain a training module which
consist of one or more CPG models and one or
more entity models represented as DPF specifica-
tions. The states of the training module T M are
defined by a set of elements that include a pair of
CPG workflow instance and a DPF entity instance
that represents the entities within a domain and re-
lationships between them. Figure 4 illustrates an
example of two states T M
1
and T M
2
of a training
module. The state T M
1
consists of a set of ele-
ments that include a pair of workflow instances and
DPF instances: {< WI
0
, EI
0
>, < W I
1
, EI
1
>, .. <
W I
n
, EI
n
} where W I
1
,W I
2
, ..W I
n
are workflow in-
stances and EI
0
, EI
1
, ..EI
n
are DPF entity instances.
Figure 4 shows a training session flow which con-
sists of a sequence of states of training module i.e.,
Training
Flow1
:=< T M
1
, T M
2
, ....T M
k
>. Figure 3
shows an instance of a training session. In Figure 3
the game engine instantiates a training session by gen-
erating questions based on the DPF entity model and
CPG workflow model. For example, it could initially
generate a scenario based on the patient details and
history and examination findings and ask what the di-
agnosis is. If answered correctly, it will move on to
the next task and ask about the treatment. A training
session is composed of a sequence of training mod-
ules and is evolved from the initial state of a training
flow and progresses based on the answer provided by
the user.
Figure 4: States of training module.
Training module
(State, TM )
0
<Enabled>
Training module
(State, TM )
1
<Disabled>
Training module
(State, TM )
0
<Disabled>
Training module
(State, TM )
1
<Enabled>
Transformation of training module’s state due to correct answer(s)
Figure 5: Progression of the states of training module.
In our approach a training session is evolved from
the initial state of a training flow and progresses based
on the answer provided by the user. Figure 5 illus-
trates the idea of the progression of the states of train-
ing session. Depending on the answer given by the
user, a game engine consults with the training flow
and evolves the state of the training session. We
use two DPF predicates < Enabled >, < Disabled >
to represent the current status of the training mod-
ules. A training module T M
0
when annotated with
the < Enabled > predicate indicates that the training
module is currently active and is being considered for
training.
The answers are collected from the user in two
different ways. We can ask the user to answer some
questions about the domain ontology i.e., entities and
their relationships; also the question can be based on
A Model Driven Approach to the Development of Gamified Interactive Clinical Practice Guidelines
151
Question
QuestionCategory
Game
requiredMinSkill
numberOfQuestions
passingCondition
Skill
id
title
dependency
Student
skill
PersonalInformation
questionCategory
id
title
questionCategory
questionFormat
Answer (ref to WI/EI)
reward
LearnerProfile
student
learningHistory
id
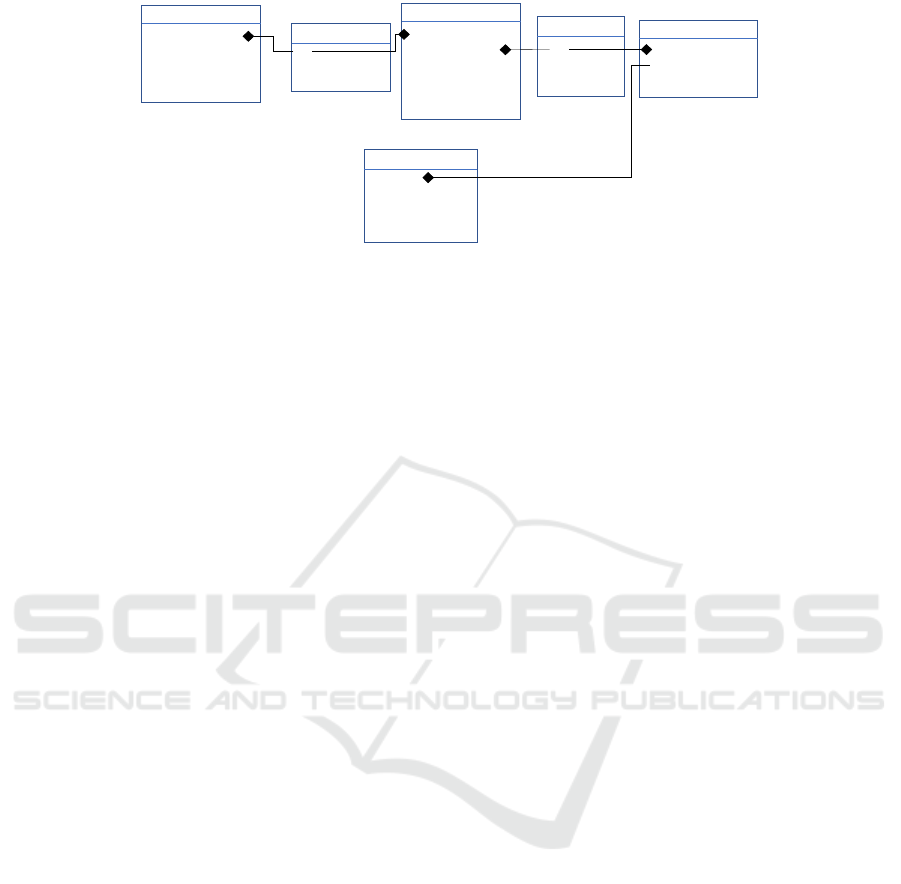
Figure 6: A conceptual model for the game elements.
the workflow instance. We utilize another DPF model
to formulate the questions that can be asked to the
user. Figure 6 shows the DPF model representing the
concepts of an e-learning game. The model represents
the game elements which include information about
how the game engine should control the game. In our
approach a game instance is associated with a train-
ing module. Using this DPF model we can specify
the number of questions to be asked, passing condi-
tion and can include questions under some question
category. We use references to the CPG instances and
entity instances for specifying correct and wrong an-
swers.
A general concern about this approach is the vali-
dation of the training flow. While constructing a train-
ing flow one might make mistake in two ways: (a)
wrong composition of instances of CPG model and
entity model; (b) wrong flow of CPG instances. To
reduce the number of errors we apply inconsistency
checking as described in the next section.
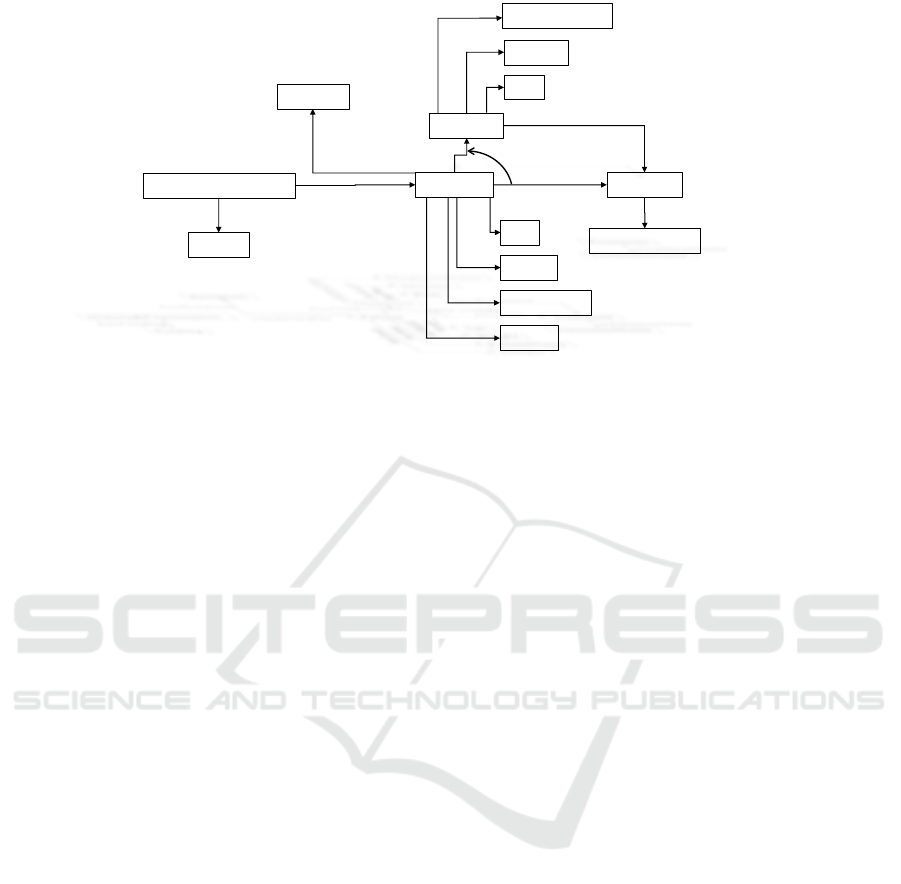
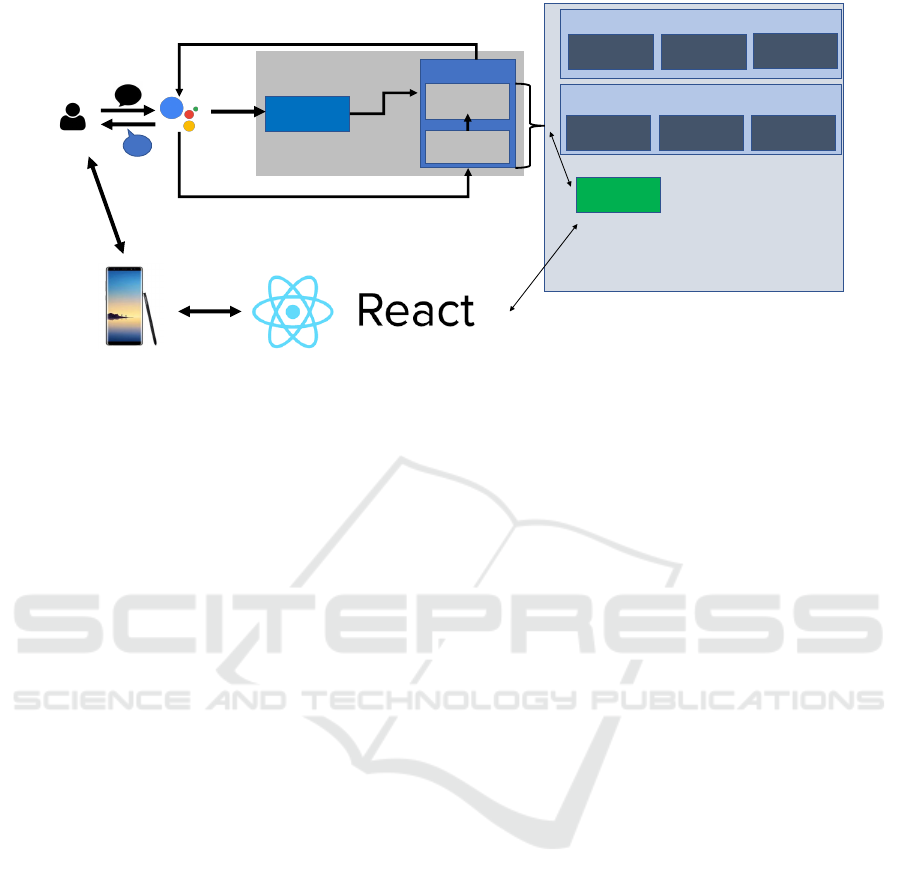
4 SYSTEM DESCRIPTION
We propose to use a generic system based on the
idea of multilevel-metamodeling and their coordina-
tion. Figure 7 shows an overview of the system.
The responsibility of the ‘Game Engine’ is to control
the training flow, maintain the status of the trainee,
produce dialogues or control the visualization of the
screen. The user should be able to interact with the
game engine via ‘Google Assistant’ or ‘Mobile appli-
cation’.
We plan to support different types of devices for
the training to facilitate training considering various
learning style of the trainee.
Question Flow Manager: The question flow man-
ager selects the questions to be asked depending on
the level of difficulty of a training session. It main-
tains the order of questions to be shown to the user.
For example, user-A has skill-1 and chose to go
through the beginning session. While randomly se-
lecting questions that falls under the difficulty of ‘Be-
ginner’, it also looks into the questions that has been
used before for user-A. It puts more emphasize on the
questions that the user has been struggling with.
Conversation Manager: The conversation man-
ager keeps track of the conversation and manages the
context of the conversation. For example, if there are
three questions to be asked that is related to a child
who is 2 years old, then the conversation manager
produces a context for three questions and starts the
conversation saying “A 2 year old child comes to the
emergency department with <some condition>, an-
swer to the following questions:”. Afterwards it asks
the first question, followed by the 2nd and 3rd ques-
tions.
User Management: The user management module
keeps track of the trainees skill, progress and effort.
The user management module is also used to produce
visualization showing the performance of a popula-
tion. If a group of trainee is particularly struggling
with a set of questions or question category then the
user management module will produce a report and
the trainer will be able to monitor it.
4.1 Adaptiveness
There are two ways our system facilitates adaptive-
ness:
• Customizing the gamification process by means
of model-driven-engineering approach.
• Capturing the learning behaviour of trainee and
changing the model accordingly.
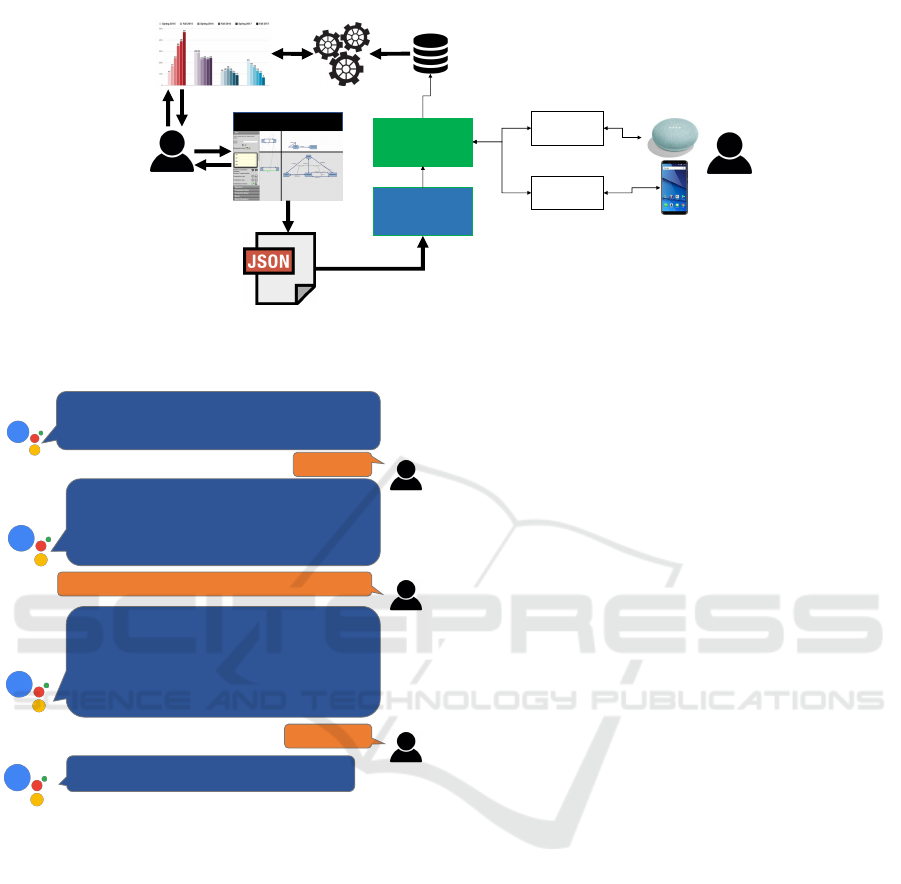
4.2 Methods
Our approach consists of modeling the entity which
represents the concepts related to clinical informa-
tion; the workflow which represents the flow of a
guideline; and the structure of a game. We propose
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
152
Invocation
trigger
Conversation Action
1. invoke
fulfillment
Process
dialog input
2. user requests
Generate
dialog output
3. action responds
Game
Engine
Workflow
Model(s)
Entity
Model(s)
Game
Elements
Conversation
manager
Question
Flow
manager
User
management
DPF Models
Training managmenet
Figure 7: Overview of the proposed system architecture.
to use WebDPF tool for the modeling of these ele-
ments. The multilevel metamodeling supported by
the WebDPF tool allows us to design domain specific
modeling languages. The tool is also facilitated with
a constraint checker which allows us to check if the
models being constructed are valid or not. We per-
sist our models using JSON format. Figure 8 shows
an overview of the proposed system where the game
engine reads the models using a model parser. The
game engine executes the game by asking questions
to the trainee and also stores the answer in a relational
database. We have developed a report engine which
retrieves data from the relational database and visual-
izes learning analytics to the trainer. The trainer can
also interact with the report interface and can visu-
alize the data from different perspective. The trainer
can get an overview of the training modules and can
select individual trainees usage statistics. In our cur-
rent implementation we have not incorporated any
machine learning algorithms. Therefore, adapting a
training module according to the requirement of the
trainee are done manually by the knowledge engineer.
We used this modeling architecture to develop a
proof-of-concept game for the asthma guideline train-
ing. Figure 9 shows a sample conversation from the
asthma guideline training. While the participant is
using google assistant we use the google account for
registering the participant to our system. It is planned
to use OAuth 2.0 protocol for authenticating the user
from the mobile application to the participants Google
account. It will allow the user to switch from one de-
vice to another. While the participant is using the mo-
bile application they get more feature such as brows-
ing the guideline.
4.2.1 Implementation of the Mobile Application
The application is developed using React-Native and
JavaScript. React-Native is based on the React frame-
work, and is used to build mobile applications for An-
droid and iPhone. The motivation for using such a
framework is reuse of code when supporting both mo-
bile platforms as well as the web.
The game consists of a collection of quizzes,
where each quiz contains several questions. These
questions are based around a scenario, where the stu-
dent is presented with answer alternatives. Picking
an answer alternative will give the student points for
how close he was to the right action. The student is
presented with the answer key, an explanation, as well
as pointers to the evidence and the relevant guideline
for further study.
The quiz will conclude with a summary, giv-
ing feedback and statistics on students performance.
The quiz should have a passing condition to unlock
quizzes at a higher difficulty level. This is illustrated
in Figure 10.
4.2.2 Generating the Scenarios
To generate questions, we will write small scenarios
in the form of narrative templates where we use tags
to refer to variables in the entity model. The tag refers
to a path in the entity graph. The application will tra-
verse through the graph and return the value of the
given vertex.
A challenge with this method, is how to present
the data returned by the graph in a text. The value
from a measurement of the pulse-rate is just an in-
teger. An observation that the patient has a breath-
ing condition is a boolean, and an observation of the
patients level of consciousness is an enumerate of
A Model Driven Approach to the Development of Gamified Interactive Clinical Practice Guidelines
153
Model Parser
WebDPF
Persist
models in JSON
UI Flow
Dialog Flow
Game Engine
Training data
Report Engine
Learning analytics
Knowledge
Engineer
Trainee
Figure 8: Proposed method of the system.
Hello, welcome to the asthma guideline training program.
In order to continue, I need your permission to know your
name from google. Is that ok?
Ok
Welcome <<username>>. While the training is going on
you can always choose to go to the main menu or quit.
Please choose from the following options: See Progress;
Start Training; Quit.
What do you wish to do?
I would like to start training
I will ask 5 questions from the diagnosis and assessment
category. The questions have difficulty level ‘Easy’. Lets
start the training. A 2 year old boy comes to the
emergency department with a history of cough and
wheeze. Answer to the following questions.
First question, Central cyanosis would mean a diagnosis
of severe asthma. True or False
True
Correct answer! Second question…..
Figure 9: Sample flow of conversation from the asthma
guideline training.
the AVPU (Alert, Verbal, Pain, Unresponsive) scale.
These values will have to be presented differently to
make a good sentence in the scenario. How we solved
this issue was by letting the vertex hold a string repre-
sentation of its value. This is illustrated in Figure 11.
<%Ben.name%> arrives at the emergency
department.
He <%Ben.hasConsciousness.value.name%>.
translates to
Ben arrives at the emergency
department.
He is not alert and not verbal,
but responds to pain.
5 RELATED WORK
In (Farkash et al., 2013) Farkash et al. presented a
model-driven approach to formalize clinical practice
guideline using natural rule language (NRL). Speci-
fying the constraints of a guideline with English-like
rule language reduces the gap of the representation
and processing of guidelines. The authors presented
a set of software components that support the repre-
sentation, interpretation of CPGs using NRL and also
can be applied directly to a patient’s EHR data for
analysis. Their approach is supported by a proof-of-
concept implementation for a simple essential hyper-
tension guideline directive. Our approach is different
with their approach as we use a graph based modeling
technique and the main contribution of our approach
is to support the training of a guideline by means of
gamification.
In (Kristensen et al., 2009) Kristensen et al.
presented a conceptual model for e-learning where
the learning materials are divided into atomic units
and organized in several graph based models such
as ‘Knowledge map’, ‘Learning map’ and ‘Student
map’. These conceptual models provide a better
structure for representing an e-learning environment
and an easy-to-use navigation interface for exist-
ing learning materials. We borrowed concepts from
this paper and adapted them for representing CPGs
and game elements by means of Diagram Predicate
Framework and multi-metamodelling approach.
A gamification approach was presented in (Akl
et al., 2008) where the authors followed the format
of TV game shows in which two teams of residents
compete in answering questions that are based on the
recommendations of guidelines. However, their ap-
proach is lacking formalization and does not support
model based analysis. In our approach we emphasize
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
154
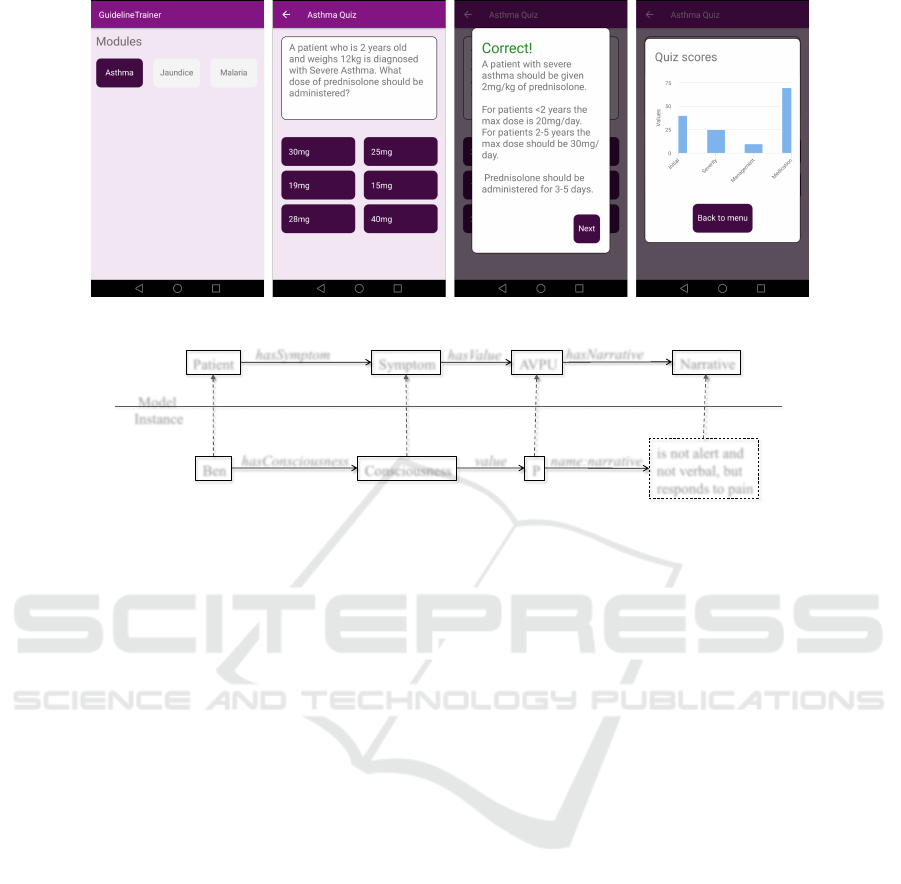
Figure 10: Flow of the mobile application.
Narrative
hasNarrative
Patient Symptom AVPU
hasSymptom
hasValue
Ben Consciousness
hasConsciousness
is not alert and
not verbal, but
responds to pain
Model
Instance
P
value name:narrative
Figure 11: Importing variables from graph into scenario.
on the modeling part and apply model driven engi-
neering technique to interface with various platforms.
In (Del Cura-Gonz
´
alez et al., 2016) the authors
conducted a study to assess the effectiveness of a
teaching strategy for the implementation of CPGs us-
ing educational games. They demonstrated the results
for an e-learning game EDUCAGUIA to improve
knowledge and skills related to clinical decision-
making by residents in family medicine. The game
consists of educational games with hypothetical clin-
ical scenarios in a virtual environment. To iden-
tify the effectiveness of teaching strategies through
e-learning, they proposed an average score compar-
ison of hypothetical scenario questionnaires between
the EDUCAGUIA intervention group and the control
group. Such evaluation is very important and it re-
flects the usefulness of utilizing games in teaching
guidelines. We plan to conduct similar evaluation of
our gamification approach with healthcare profession-
als in future.
(Aouadi et al., 2016) uses Technology-Enhanced
Learning standards to develop serious games which
can be used in technological/professional/academic
fields for learning. Their goal was to make a scenario-
building approach, built upon a model driven archi-
tecture. The game includes a health course with
demonstrative videos and evaluation quizzes with
each course having a passing condition. The game is
also demonstrated as a 3D game in a context of med-
ical training. In their approach Aouadi et al., used a
platform independent model for the development of
game components which was transformed into a plat-
form specific model by means of ATL transformation.
While their approach is very close to our proposed
method, they lack modularization and separation of
concerns. In our approach we do not only apply mul-
tilevel metamodelling but also the integration of dif-
ferent modeling hierarchies which allows us to con-
veniently articulate various aspects of an e-learning
system.
(Wyatt et al., 2013) presents OKWA (Okay with
Asthma) which is a game targeted on children.
They aim at educating children with asthma in self-
management skill. This includes information about
medications, how to avoid triggering the asthma,
monitoring, when and how to get help from others.
The game is an interactive animated movie-style nar-
rative, where the actions the child chooses will have
an effect on how the story develops. Our project dif-
fers from this one as our target group is adult health
care workers. We will also focus more on evalua-
tion of medical knowledge through tasks and quizzes
rather than just story telling.
(Shegog et al., 2006) is similar to the OKWA
project, as it targets self-management skills for chil-
dren with asthma during a role playing game. The
game uses the child’s asthma profile, so the child can
see the responses to his/hers health information in the
game. To complete a scenario, the character in the
game needs to be symptom free.
A Model Driven Approach to the Development of Gamified Interactive Clinical Practice Guidelines
155

(Zolfo et al., 2010) describes an approach where
they use mobile phones as a personal learning envi-
ronment for health care workers in resource limited
environments. They put an emphasize on the impor-
tance of avoiding health care workers being absent
from the health station for training programs. They
use didactic learning material (3d animations, video,
presentations, sound) and evaluates learning through
multiple choice questions. They also use Skype and
Facebook to have clinical case discussions with a
network of experts. The project differs to ours, as
they have an emphasize on didactic distance-learning
while we are learning through actively solving prob-
lems and tasks through gaming elements.
(Bartel et al., 2017) aims for a generic gaming
platform for implementing gamified learning arrange-
ments in engineering education. Their approach to
implementation is based on the concept of domain-
specific modeling, which is descirbed as an instance
of model-driven software design. However both theirs
and our projects are in the field of model driven de-
velopment, Bartels work aims at engineering educa-
tion, while we aim at education of health care work-
ers. Their project is a work in progress, and have lim-
ited results to analyze and compare to.
(Pesare et al., 2016) presents both Edugame and
Simulation of Clinical Cases. Edugame is aimed at
patients and caregivers, to manage the disease and
promote a healthy lifestyle to avoid critical situations
and hospitalization. The game is a role-playing game,
and the users mission is to answer correct on the prob-
lems posed on the character in the game. Simulation
of Clinical Cases is a single player simulation game.
The goal is to save the character in the game, by the
user suggesting the right therapy, action and/or exam-
ination to solve the condition the patient in the game
has. The game adapts to which role the clinician has,
so the game will be different for a nurse and a physi-
cian. The game provides scores according to if the
answer was correct, partially correct or wrong. Our
project has a larger focus on model driven develop-
ment and a data model to easier add new content and
other types of games.
Septris (Evans et al., 2015) is an online training
tool to help emergency clinicians to identify and dif-
ferentiate between the different forms of the sepsis
syndrome. Pick the right diagnostic tests and provide
optimal management of the syndrome. Diagnose and
treatment is a big part of our project as well, but it
will be made general enough to make games for sev-
eral different medical conditions.
6 CONCLUSION
In this work, we have presented a model-driven ap-
proach to the design and development of a gamified
system for learning clinical guideline content. We
also present a prototype mobile e-learning system that
utilized our design approach in its development. In
the near future we aim to test our system with clini-
cians to evaluate its usability, acceptability and effec-
tiveness.
ACKNOWLEDGEMENTS
This work was supported in part by the NORHED
program (Norad: Project QZA-0484). The content
is solely the responsibility of the authors and does not
necessarily represent the official views of the Norwe-
gian Agency for Development Cooperation.
REFERENCES
Akl, E. A., Mustafa, R., Slomka, T., Alawneh, A., Ab-
hishek, V., and Sch
¨
unemann, H. J. (2008). An edu-
cational game for teaching clinical practice guidelines
to internal medicine residents: development, feasibil-
ity and acceptability. BMC Med Education, 8.
Aouadi, N., Pernelle, P., Ben Amar, C., Carron, T., and Tal-
bot, S. (2016). Models and mechanisms for imple-
menting playful scenarios. In 2016 IEEE/ACS 13th In-
ternational Conference of Computer Systems and Ap-
plications (AICCSA), pages 1–8. IEEE.
Baker, A. (2001). Crossing the quality chasm: a new health
system for the 21st century. BMJ: British Medical
Journal, 323(7322):1192.
Barr, M. and Wells, C. (1990). Category theory for comput-
ing science, volume 49. Prentice Hall New York.
Bartel, A., Hagel, G., and Wolff, C. (2017). Work in
progress: Towards a generic platform for implement-
ing gamified learning arrangements in engineering ed-
ucation. In 2017 IEEE Global Engineering Education
Conference (EDUCON), pages 1502–1505. IEEE.
Bernik, A., Buba
ˇ
s, G., and Rado
ˇ
sevi
´
c, D. (2018). Measure-
ment of the effects of e-learning courses gamification
on motivation and satisfaction of students. In 41th In-
ternational Convention-Mipro 2018.
Cabana, M. D., Ebel, B. E., Cooper-Patrick, L., Powe,
N. R., Rubin, H. R., and Rand, C. S. (2000). Barriers
pediatricians face when using asthma practice guide-
lines. Archives of Pediatrics & Adolescent Medicine,
154(7):685–693.
Cabana, M. D., Rand, C. S., Powe, N. R., Wu, A. W.,
Wilson, M. H., Abboud, P.-A. C., and Rubin, H. R.
(1999). Why don’t physicians follow clinical practice
guidelines?: A framework for improvement. Jama,
282(15):1458–1465.
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
156

Del Cura-Gonz
´
alez, I., L
´
opez-Rodr
´
ıguez, J. A., Sanz-
Cuesta, T., Rodr
´
ıguez-Barrientos, R., Mart
´
ın-
Fern
´
andez, J., A.-C. G., Polentinos-Castro, E.,
R.-C. B., Escortell-Mayor, E., Rico-Bl
´
azquez,
M., Hern
´
andez-Santiago, V., Azcoaga-Lorenzo,
A., Ojeda-Ruiz, E., Gonz
´
alez-Gonz
´
alez, A. I.,
´
Avila Tomas, J. F., B.-C. J., Molero-Garc
´
ıa, J. M.,
Ferrer-Pe
˜
na, R.and Tello-Bernab
´
e, M. E., and
Trujillo-Mart
´
ın, M. (2016). Effectiveness of a strat-
egy that uses educational games to implement clinical
practice guidelines among spanish residents of family
and community medicine (e-EDUCAGUIA project):
a clinical trial by clusters. Implementation Sci., 11:71.
Deterding, S., Dixon, D., Khaled, R., and Nacke, L.
(2011a). From game design elements to gamefulness:
defining gamification. In Proceedings of the 15th in-
ternational academic MindTrek conference: Envision-
ing future media environments, pages 9–15. ACM.
Deterding, S., Sicart, M., Nacke, L., O’Hara, K., and Dixon,
D. (2011b). Gamification. using game-design ele-
ments in non-gaming contexts. In CHI’11 extended
abstracts on human factors in computing systems,
pages 2425–2428. ACM.
Donaldson, M. S., Corrigan, J. M., Kohn, L. T., et al.
(2000). To err is human: building a safer health sys-
tem, volume 6. National Academies Press.
Evans, K. H., Daines, W., Tsui, J., Strehlow, M., Maggio, P.,
and Shieh, L. (2015). Septris: a novel, mobile, online,
simulation game that improves sepsis recognition and
management. Academic medicine : journal of the As-
sociation of American Medical Colleges, 90(2):180–4.
Farkash, A., Timm, J. T. E., and Waks, Z. (2013). A model-
driven approach to clinical practice guidelines repre-
sentation and evaluation using standards. Studies in
health technology and informatics, 192:200—204.
Fervers, B., Carretier, J., and Bataillard, A. (2010). Clin-
ical practice guidelines. Journal of visceral surgery,
147(6):e341–e349.
Goud, R., de Keizer, N. F., ter Riet, G., Wyatt, J. C., Has-
man, A., Hellemans, I. M., and Peek, N. (2009). Ef-
fect of guideline based computerised decision support
on decision making of multidisciplinary teams: clus-
ter randomised trial in cardiac rehabilitation. Bmj,
338:b1440.
Grimshaw, J. M., Sch
¨
unemann, H. J., Burgers, J., Cruz,
A. A., Heffner, J., Metersky, M., and Cook, D. (2012).
Disseminating and Implementing Guidelines. Pro-
ceedings of the American Thoracic Society, 9(5):298–
303.
Kapp, K. M. (2012). The gamification of learning and
instruction: game-based methods and strategies for
training and education. John Wiley & Sons.
Kristensen, T., Lamo, Y., Hinna, K. R. C., and Hole, G. O.
(2009). Dynamic content manager - A new concep-
tual model for e-learning. In Liu, W., Luo, X., Wang,
F. L., and Lei, J., editors, Web Information Systems
and Mining, International Conference, WISM 2009,
Shanghai, China, November 7-8, 2009. Proceedings,
volume 5854 of Lecture Notes in Computer Science,
pages 499–507. Springer.
Lohr, K. N., Field, M. J., et al. (1992). Guidelines for
clinical practice: from development to use. National
Academies Press.
L
¨
owe, M. (1993). Algebraic approach to single-pushout
graph transformation. Theoretical Computer Science,
109(1-2):181–224.
Marriott, S., Palmer, C., and Lelliott, P. (2000). Dissem-
inating healthcare information: getting the message
across. BMJ Quality & Safety, 9(1):58–62.
NHLBI (2007). Expert panel report 3: guidelines for the
diagnosis and management of asthma. Number 97.
DIANE Publishing.
NICE (2017). Asthma: diagnosis, monitoring and chronic
asthma management. Nice Guideline 80.
Pesare, E., Roselli, T., Corriero, N., and Rossano, V. (2016).
Game-based learning and Gamification to promote en-
gagement and motivation in medical learning con-
texts. Smart Learning Environments, 3(1):5.
Rabbi, F., Lamo, Y., and MacCaull, W. (2014a). Co-
ordination of multiple metamodels, with application
to healthcare systems. In The 5th International Con-
ference on Emerging Ubiquitous Systems and Perva-
sive Networks (EUSPN-2014)/ The 4th International
Conference on Current and Future Trends of Informa-
tion and Communication Technologies in Healthcare
(ICTH 2014)/ Affiliated Workshops, September 22-25,
2014, Halifax, Nova Scotia, Canada, volume 37 of
Procedia Computer Science, pages 473–480. Elsevier.
Rabbi, F., Lamo, Y., and MacCaull, W. (2014b). A flexible
metamodelling approach for healthcare systems. In
Jaatun, E. A. A., Brooks, E., Berntsen, K. E., Gilstad,
H., and Jaatun, M. G., editors, Proceedings of the 2nd
European Workshop on Practical Aspects of Health
Informatics, Trondheim, Norway, May 19-20 , 2014.,
volume 1251 of CEUR Workshop Proceedings, pages
115–128. CEUR-WS.org.
Rodrigues da Silva, A. (2015). Model-driven engineering.
Comput. Lang. Syst. Struct., 43(C):139–155.
Rutle, A., Rossini, A., Lamo, Y., and Wolter, U. (2009). A
diagrammatic formalisation of mof-based modelling
languages. In Oriol, M. and Meyer, B., editors, Ob-
jects, Components, Models and Patterns, pages 37–
56, Berlin, Heidelberg. Springer Berlin Heidelberg.
Rutle, A., Rossini, A., Lamo, Y., and Wolter, U. (2012). A
formal approach to the specification and transforma-
tion of constraints in mde. The Journal of Logic and
Algebraic Programming, 81(4):422–457.
Shegog, R., Bartholomew, L. K., Gold, R. S., Pierrel, E.,
Parcel, G. S., Sockrider, M. M., Czyzewski, D. I.,
Fernandez, M. E., Berlin, N. J., and Abramson, S.
(2006). Asthma Management Simulation for Chil-
dren: Translating Theory, Methods, and Strategies to
Effect Behavior Change. Simulation in Healthcare:
The Journal of the Society for Simulation in Health-
care, 1(3):151–159.
Shiffman, R. N., Michel, G., Essaihi, A., and Thornquist,
E. (2004). Bridging the Guideline Implementation
Gap: A Systematic, Document-Centered Approach to
Guideline Implementation. J Am Med Inform Assoc,
11(5):418–426.
A Model Driven Approach to the Development of Gamified Interactive Clinical Practice Guidelines
157

Strme
ˇ
cki, D., Bernik, A., and Rado
ˇ
sevi
´
c, D. (2015). Gami-
fication in e-learning: introducing gamified design el-
ements into e-learning systems. Journal of computer
science and technology, 11(12):1108–1117.
Wyatt, T. H., Li, X., Huang, Y., Farmer, R., Reed, D., and
Burkhart, P. V. (2013). Developing an interactive story
for children with asthma. The Nursing clinics of North
America, 48(2):271–85.
Zolfo, M., Iglesias, D., Kiyan, C., Echevarria, J., Fu-
cay, L., Llacsahuanga, E., de Waard, I., Su
`
arez, V.,
Llaque, W., and Lynen, L. (2010). Mobile learning
for HIV/AIDS healthcare worker training in resource-
limited settings. AIDS Research and Therapy, 7(1):35.
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
158
