
Integrating Users Logic Into Requirements Engineering for Connected
Healthcare co-Design
Sofia Ouhbi
1
, Maria Karampela
2
and Minna Isomursu
2
1
Computer Science & Software Engineering Department, CIT, UAE University, U.A.E.
2
IT University of Copenhagen, Copenhagen, Denmark
Keywords:
Requirements Engineering, Service-dominant Logic, Connected Health, Value co-Creation.
Abstract:
The ongoing transformation in healthcare requires the creation of agile systems to meet the growing needs of
patients. An approach to develop such systems requires the elicitation of end-users’ perspectives to software
development life circle. The current requirements development process does not emphasis on the importance
of end-users’ participation in the requirements elicitation phase. The present study proposes an approach uti-
lizing Service-Dominant (S-D) logic framework to contribute to the co-design of connected health services.
Value co-creation practices when combined with requirements engineering best practices can contribute to-
wards the development of usable software for connected healthcare systems.
1 INTRODUCTION
Population age distribution is shifting towards an in-
crease of the elderly. World Health Organization
(WHO) has announced that between 2015 and 2050
the population aged over 60 years will surpass the
children younger than 5 years (Organization, 2015).
The increasingly aging population worldwide arises
various challenges to healthcare systems, among oth-
ers pertinent to support costs and service provision
(Chouvarda et al., 2015). Future healthcare systems
will have to deliver services to a larger number of pa-
tients with chronic conditions and multimorbidities.
Therefore, they have to accommodate the needs of a
population with interrelated and complex health con-
ditions from different backgrounds, while sustaining
cost effective services (Ouhbi et al., 2017).
These challenges have sparked innovation in
healthcare management models shifting traditional
management approaches towards more agile solu-
tions. Connected health model revolves around pa-
tients’ needs, utilizing the latest technological ad-
vancements to facilitate efficient management of dis-
eases (Ouhbi et al., 2018). Patients and health data
are in the spotlight of the healthcare model, that uses
information technology to enable active participation
of all actors (citizens, patients, healthcare profession-
als, and policy makers) to decision-making (Caulfield
and Donnelly, 2013; Karampela et al., 2019). Effec-
tive utilization of health data means that “the correct
information” is available “to the correct person at the
correct time” (Chouvarda et al., 2015). Connected
health paradigm encompasses a range of technologies
such as e-Health, m-Health and remote patient moni-
toring solutions (Caulfield and Donnelly, 2013).
User involvement in the healthcare management
paradigm is only an aspect of users’ participation in
healthcare provision. Propositions of active involve-
ment of users’ on the design of health devices sup-
ports further the argument that users’ contribution can
improve not only services but also products (Harte
et al., 2014; Hardyman et al., 2015). But what is the
difference between services and products? According
to Vargo and Lusch services and products have more
similarities or commonalities than differences (Vargo
and Lusch, 2004b). They argue that “goods are dis-
tribution mechanisms for service provision” and that
“economic exchange is fundamentally about service
provision” (Vargo and Lusch, 2004b), p.326. In the
same vein, Gummesson suggested that “customers do
not buy goods or services: they buy offerings, which
render services, which create value” (Gummesson,
1993).
Service-Dominant (S-D) logic, proposed by Vargo
and Lurch, places service as the core value of both
services and products. Value co-creation has been
the centre of the S-D logic literature. According to
Vargo et al. (2008) “The customer is always a co-
creator of value”, while the value has been defined
as the value-in-use (Vargo et al., 2008), p.148. In
480
Ouhbi, S., Karampela, M. and Isomursu, M.
Integrating Users Logic Into Requirements Engineering for Connected Healthcare co-Design.
DOI: 10.5220/0007754504800485
In Proceedings of the 14th International Conference on Evaluation of Novel Approaches to Software Engineering (ENASE 2019), pages 480-485
ISBN: 978-989-758-375-9
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
this context customers are co-creators of value (Vargo
and Lusch, 2004a; Vargo and Lusch, 2017), while
companies “cannot deliver value, but only offer value
propositions” (Vargo et al., 2008), p.148. Reflect-
ing upon this, companies can co-create value through
users’ involvement (Vargo and Lusch, 2004a; Vargo
and Lusch, 2017; Lusch et al., 2008).
Requirements engineering (RE) is the first step of
the software lifecycle and plays a critical role towards
delivering quality and reliable software. This paper
relies on the requirements development process pre-
sented in RE body of knowledge (REBOK) (Nilsson,
2013) and software engineering body of knowledge
(SWEBOK) (Bourque et al., 2014) which are widely
accepted and established work in the field of software
engineering (Ambreen et al., 2018).
Previous literature focusing on users’ involvement
into the system development cycle, points out that
their inclusion can have a positive impact on the cre-
ation of more effective services (Kujala, 2003; Ku-
jala et al., 2005; Wagner and Piccoli, 2007; Pekkola
et al., 2006; Bano and Zowghi, 2013). Nevertheless,
standardisation of users participation to the phases of
the requirements development process has been seen
as a challenge that can have an impact on the sys-
tem design process (Damodaran, 1996). According
to a recent systematic mapping study about personal
health data (Karampela et al., 2018), the majority of
the proposed solutions in healthcare services are de-
veloped without any empirical validation on patients’
data. The aim of the present study is to employ the
S-D logic framework to propose an approach to in-
crease the understanding of the value co-creation in
connected health by considering end-users’ involve-
ment in the requirements development process.
The following section will introduce the require-
ments development process, the core ideas of S-D
logic and two examples of challenges related to users
exclusion from the design process. Section 3 will dis-
cuss the approach of integrating S-D logic into RE.
Finally, the conclusion section presents future direc-
tions outlining S-D logic contribution to RE.
2 BACKGROUND
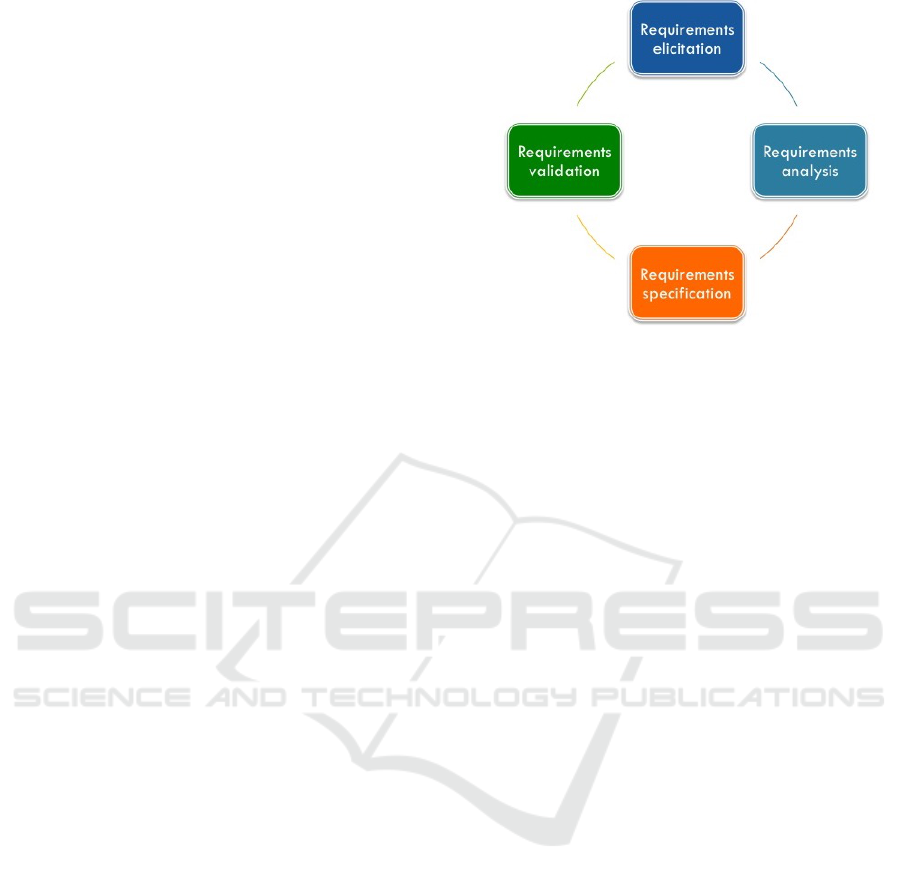
2.1 Requirements Development Process
The requirements development process includes the
four following phases: requirements elicitation, re-
quirements analysis, requirements specification, and
requirements validation. Fig. 1 presents an overview
of the requirements development process.
Figure 1: Requirements development process.
Requirements Elicitation is a complex problem
formulation phase in which business requirements,
needs and information are gathered and identified.
In the Requirements Analysis phase, the identi-
fied customers’ needs are translated and transformed
into requirements that are traceable, so that can be
measured and tested, and will be the core elements
of the design process.
Requirements Specification results in the speci-
fication of the users and system requirements which
can establish the system requirements specification
(SyRS) document and the software requirements
specification (SRS) document (IEE, 2011).
Requirements Validation is the last phase of the
requirements development process and it is crucial as
mirrors the elicitation of requirements phase. This
phase validates whether the requirements of the cus-
tomers have been met or not, so that it gives a re-
ply to the question “did we create the right product?”
(Bourque et al., 2014).
This study focuses on the four aforementioned
phases proposing an approach to incorporate the S-D
logic into the requirements development process.
2.2 S-D Logic
S-D logic is a dynamic framework that continues
evolving as economic and social factors change over
time. The core idea of this framework relies upon the
notion that services are exchange of competences be-
tween actors underlined by common interests. Ser-
vices considered to be not just associations of individ-
uals to products, but dynamic relations (“service-for-
service exchange”) underpinned by commonalities.
Services include not only business and customers, but
a service ecosystem. This ecosystem of interactions
includes all the possible interrelated economic and so-
Integrating Users Logic Into Requirements Engineering for Connected Healthcare co-Design
481
cial actors of an exchange network. Service design
networks are complex and built up in three levels:
macro, meso and micro. Zooming in or out in these
levels one can examine ecosystems of services from
different perspectives, including thus various levels of
interactions. So, service ecosystems enable services
representations as networks of “holistic experiences”.
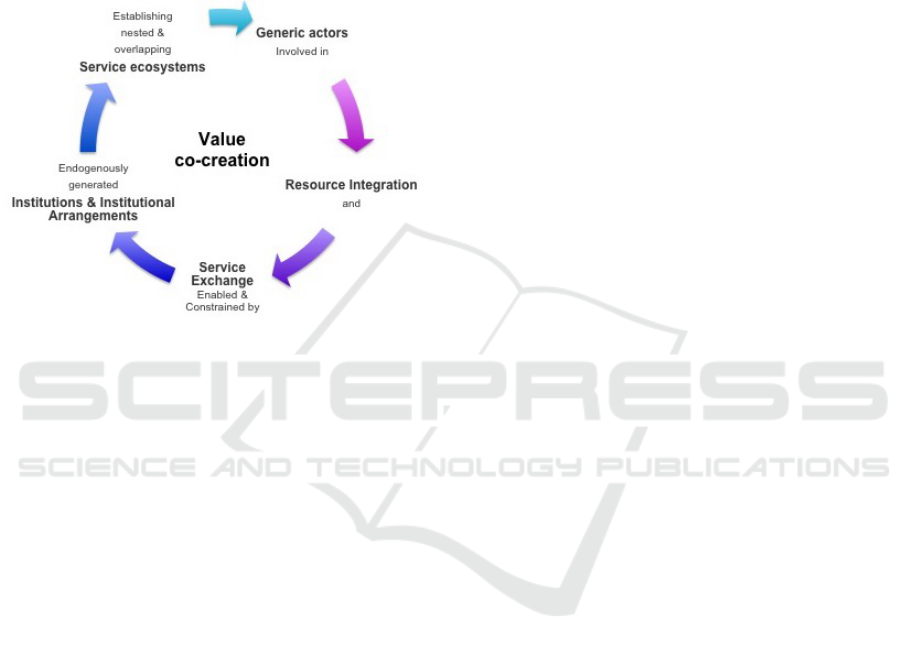
Fig 2 presents the core narrative and processes of the
S-D logic.
Figure 2: The core narrative and processes of S-D logic.
The essence of core values of the S-D logic frame-
work has been formulated into axioms. Table 1
presents the eleven foundational premises (FPs). Five
of these FPs have been considered to be the core ax-
ioms from which the other FPs can be derived. The
five axioms of the S-D logic are presented below.
Axiom1/Service is the Fundamental Basis of
Exchange. Services are exchange of resources. Re-
sources are applications of knowledge and skills,
which are the core for every exchange.
Axiom2/Value is co-Created by Multiple Ac-
tors, Always Including the Beneficiary. The value
is created when the beneficiaries use the end-product.
So, “the value-in-use” is co-created by producers and
consumers in an interactive manner through exchange
of resources (knowledge and skills).
Axiom3/All Social and Economic Actors are
Resource Integrators. All the actors of a service
have common objectives. Traditionally the term “pro-
ducer” was used for the actors who created value
and the term “customers” for the ones who destroyed
value. This notion had restricted interaction between
businesses and customers assuming that they had dif-
ferent goals. Nevertheless, all actors (businesses,
customers. etc.) that are involved in a service,
as a product of economic exchange, are “resource-
integrating, service providing enterprises” and have
a common objective to (co)-create value (Vargo and
Lusch, 2017), (p.48). What joints this network of ac-
tors is the “collective wellbeing”, in an individual and
common level as an act for achieving or maintaining
well-being.
Axiom4/Value is always Uniquely and Phe-
nomenologically Determined by the Beneficiary.
The value is determined by beneficiaries when they
use the end-services. But the value is subjective, is
based on the experiences and is dependent on the con-
text of services. The perceived value of services is
unique and related on the direct experiences of benefi-
ciaries (Kujala and V
¨
a
¨
an
¨
anen-Vainio-Mattila, 2009).
Axiom5/Value co-Creation is Coordinated
through Actor-generated Institutions and Institu-
tional Arrangements. In S-D logic framework the
terms institutions does not concern organizations, but
“are the humanly devised rules, norms, and beliefs
that enable and constrain action and make social
life at least somewhat predictable and meaningful”
(Vargo and Lusch, 2017), (p.49).
The S-D logic framework has been applied to var-
ious disciplines such as branding, logistics and sup-
ply chain management (Ballantyne and Aitken, 2007;
Flint and Mentzer, 2006; Tokman and Beitelspacher,
2011), consumer culture theory (Arnould, 2007), pub-
lic management (Osborne et al., 2013) and informa-
tion systems (Alter, 2010). Studies have also been
discussing applications of S-D logic to healthcare in-
formation systems (Hardyman et al., 2015; Rehman
et al., 2012).
2.3 Examples of Design Challenges Due
to Poor Requirements
The Chaos Report series conducted by the Standish
Group demonstrated that the major software project
impaired factors are incomplete requirements and
lack of user involvement (Sta, 2009).
A typical example of software failure due to exclu-
sion of users to the requirements development process
is the HealthCare.gov health insurance exchange web
service. It launched on October 2013, failed to serve
users needs due to various issues such as inaccurate
forecasting of user population which resulted to ac-
cessibility issues. Various system and software design
failures were related to poor user evaluation (BBC-
News, 2013). The failure to test scalability and in-
clude end-users to the design process resulted among
others to user dissatisfaction, delays in the project im-
plementation and growth of expenditures.
A second example concerns the National Pro-
gramme for IT in the NHS (NPfIT) in the United
Kingdom. The NPfIT web service was an effort to of-
fer a centralized electronic health record (EHR) that
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
482
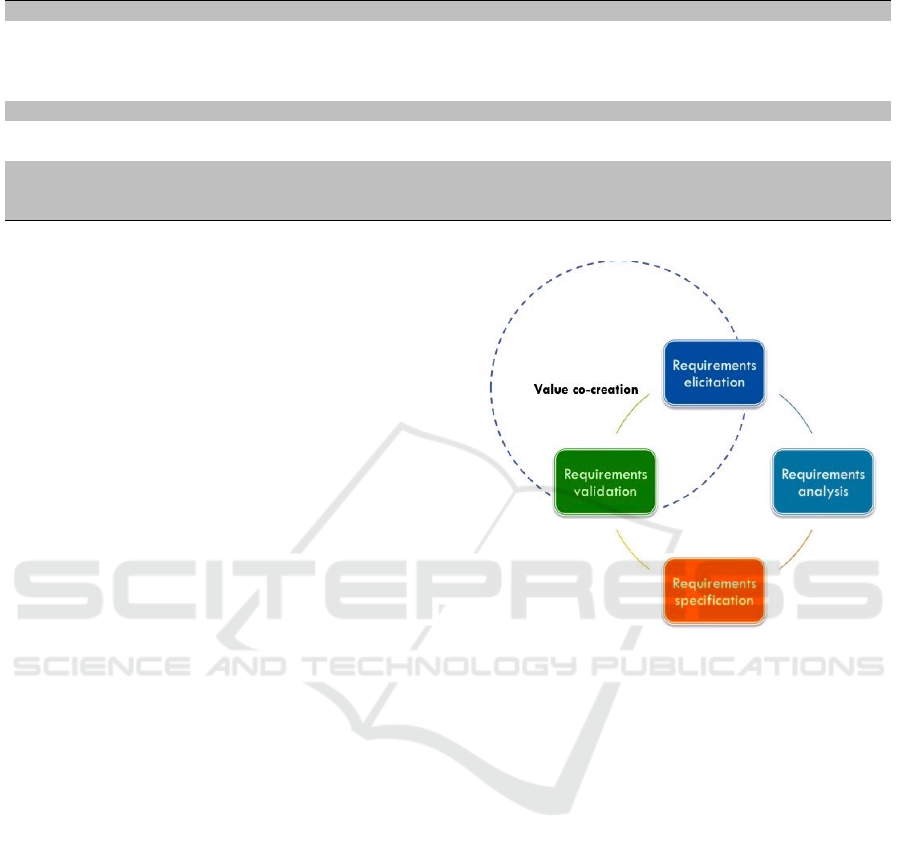
Table 1: Axioms and Foundational Premises (FPs) of S-D Logic (Vargo and Lusch, 2016).
Axiom1 FP1 Service is the fundamental basis of exchange.
FP2 Indirect exchange masks the fundamental basis of exchange.
FP3 Goods are a distribution mechanism for service provision.
FP4 Operant resources are the fundamental source of strategic benefit.
FP5 All economies are service economies.
Axiom2 FP6 Value is co-created by multiple actors,always including the beneficiary.
FP7 Actors cannot deliver value but can participate in the creation and offering of value propositions.
FP8 A service-centered view is inherently beneficiary oriented and relational.
Axiom3 FP9 All social and economic actors are resource integrators.
Axiom4 FP10 Value is always uniquely and phenomenologically determined by the beneficiary.
Axiom5 FP11 Value co-creation is coordinated through actor-generated institutions and institutional arrangements.
would be accessible by patients and also would con-
nect general practitioners and hospitals’ records. Af-
ter its implementation the software was scrapped due
to several failures such as poor functionality con-
nected to exclusion of end-users and stakeholders in
the design process (Justinia, 2017).
3 INTEGRATING THE USERS
LOGIC INTO RE
Healthcare transformation underpinned by connected
health aims to empower patients by creating services
that will “connect” all the stakeholders’ needs in an
effective manner (Caulfield and Donnelly, 2013). The
challenge for requirements development process is
that it should respond to these needs by enabling
stakeholders participation to the life cycle of software
development.
Fig. 3 presents where value co-creation can be
generated in the requirements development process.
Drawing from S-D logic paradigm software can be
seen as a “service”. This means that software en-
gineers hold the responsibility to design complex
healthcare services encapsulating social and relational
norms and interactions into services. However, trans-
forming knowledge, business and users’ needs into
software components is a challenge by itself. Our pro-
posed framework based on S-D logic can contribute
on that in different ways.
Considering software in the lens of service means
that the focus of the requirements development pro-
cess should be shifted to the design of exchange of
resources, so to the design of knowledge and skills
(Axiom1, FP1) (Vargo and Lusch, 2017). In case of
healthcare services it is essential to involve patients
into the design process as their needs are often com-
plex and unique, requiring thus solutions that are sen-
sitive on that (Axiom4, FP10).
The idea of value-in-use is a notion that require-
ments development process can benefit from. Ac-
Figure 3: Value co-creation in requirements development
process.
cording to this notion, value is created by the bene-
ficiaries of a service while using the services. More-
over, the value is co-created by multiple actors includ-
ing always the end-users (Axiom2, FP6). Based on
that, a suggestion would be to involve beneficiaries,
patients in this case, along the requirements develop-
ment process. Their knowledge in each step of the
requirements development process could lead to the
creation of more agile and effective solutions that will
be aligned with their needs.
The idea of a common objective for “collective
wellbeing” amplifies the argument that stakeholders
involvement in the requirements development process
can have positive impact (Axiom 3, FP9). The contri-
bution of this axiom is the notion that service ecosys-
tems are environments that connect actors under a
common goal. So, more attention should be given to
the commonalities of the stakeholders of a services
than to the differences (Axiom5, FP11).
The relation of actors in a service ecology envi-
ronment is complex and develops in different levels.
One can argue that the complexity of such networks
can pose a challenge to engineers, designers or busi-
Integrating Users Logic Into Requirements Engineering for Connected Healthcare co-Design
483

ness analysts. The S-D logic suggests a frame to clus-
ter these relations into different levels (micro, meso,
macro). On this way software engineers could gain
a better understanding of this complex network of
actors focusing on different perspectives within the
same network. Mapping the actions and stakehold-
ers could contribute to better understanding of service
ecology leading to the development of more agile so-
lutions.
Although the S-D logic framework could con-
tribute towards better understanding of service ecol-
ogy and network of users, the education of the future
software engineers can also facilitate them to better
understand and reflect upon citizens’ needs. Design-
ing multidisciplinary education programs that will fo-
cus not only on the technical perspectives, but also
on the self-reflection of students has been suggested
as an innovation that can make a difference (Graham,
2018).
Another suggestion has been to reconsider the ed-
ucation of engineers (Ouhbi et al., 2015), drawing
lines towards societal and environmental challenges
that the world is facing. In addition, project-based
education and internships have been seen as a way
to shift the focus of engineers from the laboratories
to real-world challenges leading thus to better under-
standing of human nature (Graham, 2018). Software
engineers hold an essential role and an ethical respon-
sibility to serve society by contributing towards the
creation of welfare services.
4 CONCLUSION AND FUTURE
WORK
This paper presents a preliminary discussion of S-D
logic integration into the requirements development
process. It has discussed how the five core axioms
of the S-D logic, the service ecology and reformation
on education of engineers could contribute on the re-
design of the requirements development process.
Our future work will focus on the refinement
of the proposed approach and the development of
a model to support software engineers to improve
the requirements development process for connected
health systems. We intend also to conduct empirical
evaluation to validate our proposed approach.
REFERENCES
(2009). Standish-Group, CHAOS summary 2009.
(2011). IEEE Std 29148-2011, ISO/IEC/IEEE International
standard - systems and software engineering – life cy-
cle processes – requirements engineering.
Alter, S. (2010). Viewing systems as services: a fresh ap-
proach in the IS field. Communications of the associ-
ation for information systems, 26(1):11.
Ambreen, T., Ikram, N., Usman, M., and Niazi, M.
(2018). Empirical research in requirements engineer-
ing: trends and opportunities. Requirements Engi-
neering, 23(1):63–95.
Arnould, E. J. (2007). Service-dominant logic and con-
sumer culture theory: Natural allies in an emerging
paradigm. In Consumer culture theory, pages 57–76.
Emerald Group Publishing Limited.
Ballantyne, D. and Aitken, R. (2007). Branding in B2B
markets: insights from the service-dominant logic of
marketing. Journal of Business & Industrial Market-
ing, 22(6):363–371.
Bano, M. and Zowghi, D. (2013). User involvement in soft-
ware development and system success: a systematic
literature review. In Proceedings of the 17th Interna-
tional Conference on Evaluation and Assessment in
Software Engineering, pages 125–130. ACM.
BBCNews (2013). Obama addresses healthcare website
glitches.
Bourque, P., Fairley, R. E., et al. (2014). Guide to the
Software Engineering Body of Knowledge (SWEBOK
(R)): Version 3.0. IEEE Computer Society Press.
Caulfield, B. and Donnelly, S. (2013). What is connected
health and why will it change your practice? QJM: An
International Journal of Medicine, 106(8):703–707.
Chouvarda, I. G., Goulis, D. G., Lambrinoudaki, I., and
Maglaveras, N. (2015). Connected health and inte-
grated care: Toward new models for chronic disease
management. Maturitas, 82(1):22–27.
Damodaran, L. (1996). User involvement in the systems
design process-a practical guide for users. Behaviour
& information technology, 15(6):363–377.
Flint, D. J. and Mentzer, J. T. (2006). Striving for integrated
value chain management given a service-dominant.
The service-dominant logic of marketing: dialog, de-
bate, and directions, 139.
Graham, R. (2018). The global state of the art in engineer-
ing education. Technical report, Massachusetts Insti-
tute of Technology (MIT), Massachusetts, USA2018.
Gummesson, E. (1993). Quality management in service or-
ganizations. ISQA, New York, NY, 487.
Hardyman, W., Daunt, K. L., and Kitchener, M. (2015).
Value co-creation through patient engagement in
health care: a micro-level approach and research
agenda. Public Management Review, 17(1):90–107.
Harte, R. P., Glynn, L. G., Broderick, B. J., Rodriguez-
Molinero, A., Baker, P., McGuiness, B., O’Sullivan,
L., Diaz, M., Quinlan, L. R., and
´
OLaighin, G. (2014).
Human centred design considerations for connected
health devices for the older adult. Journal of person-
alized medicine, 4(2):245–281.
Justinia, T. (2017). The UK’s national programme for IT:
Why was it dismantled? Health services management
research, 30(1):2–9.
ENASE 2019 - 14th International Conference on Evaluation of Novel Approaches to Software Engineering
484

Karampela, M., Ouhbi, S., and Isomursu, M. (2018). Per-
sonal health data: A systematic mapping study. Inter-
national journal of medical informatics, 118:86–98.
Karampela, M., Ouhbi, S., and Isomursu, M. (2019). Ac-
cessing and sharing electronic personal health data. In
12th International Conference on Health Informatics,
HealthInf, page in Press.
Kujala, S. (2003). User involvement: a review of the bene-
fits and challenges. Behaviour & information technol-
ogy, 22(1):1–16.
Kujala, S., Kauppinen, M., Lehtola, L., and Kojo, T. (2005).
The role of user involvement in requirements quality
and project success. In Proceedings. 13th IEEE In-
ternational Conference on Requirements Engineering,
pages 75–84. IEEE.
Kujala, S. and V
¨
a
¨
an
¨
anen-Vainio-Mattila, K. (2009). Value
of information systems and products: Understanding
the users’ perspective and values. Journal of Infor-
mation Technology Theory and Application (JITTA),
9(4):4.
Lusch, R. F., Vargo, S. L., and Wessels, G. (2008). Toward a
conceptual foundation for service science: Contribu-
tions from service-dominant logic. IBM systems jour-
nal, 47(1):5–14.
Nilsson, F. (2013). Introduction to requirements engineer-
ing REBOK requirements engineering body of knowl-
edge. REQB
R
Certified Professional for Require-
ments Engineering, 1:59.
Organization, W. H. (2015). World report on ageing and
health. World Health Organization.
Osborne, S. P., Radnor, Z., and Nasi, G. (2013). A new the-
ory for public service management? toward a (public)
service-dominant approach. The American Review of
Public Administration, 43(2):135–158.
Ouhbi, S., Fern
´
andez-Alem
´
an, J. L., Carrillo-de Gea, J. M.,
Toval, A., and Idri, A. (2017). E-health internation-
alization requirements for audit purposes. Computer
Methods and Programs in Biomedicine, 144:49–60.
Ouhbi, S., Fern
´
andez-Alem
´
an, J. L., Toval, A., Rivera Pozo,
J., and Idri, A. (2018). Sustainability requirements for
connected health applications. Journal of Software:
Evolution and Process, 30(7):e1922.
Ouhbi, S., Idri, A., Fern
´
andez-Alem
´
an, J. L., and Toval, A.
(2015). Requirements engineering education: a sys-
tematic mapping study. Requirements Engineering,
20(2):119–138.
Pekkola, S., Kaarilahti, N., and Pohjola, P. (2006). To-
wards formalised end-user participation in informa-
tion systems development process: bridging the gap
between participatory design and ISD methodologies.
In Proceedings of the ninth conference on Participa-
tory design: Expanding boundaries in design, vol-
ume 1, pages 21–30. ACM.
Rehman, M., Dean, A. M., and Pires, G. D. (2012). A re-
search framework for examining customer participa-
tion in value co-creation: Applying the service dom-
inant logic to the provision of living support services
to oncology day-care patients. International Journal
of Behavioural and Healthcare Research, 3(3-4):226–
243.
Tokman, M. and Beitelspacher, L. S. (2011). Supply chain
networks and service-dominant logic: suggestions for
future research. International Journal of Physical Dis-
tribution & Logistics Management, 41(7):717–726.
Vargo, S. L. and Lusch, R. F. (2004a). Evolving to a new
dominant logic for marketing. Journal of marketing,
68(1):1–17.
Vargo, S. L. and Lusch, R. F. (2004b). The four service mar-
keting myths: remnants of a goods-based, manufac-
turing model. Journal of service research, 6(4):324–
335.
Vargo, S. L. and Lusch, R. F. (2016). Institutions and ax-
ioms: an extension and update of service-dominant
logic. Journal of the Academy of Marketing Science,
44(1):5–23.
Vargo, S. L. and Lusch, R. F. (2017). Service-dominant
logic 2025. International Journal of Research in Mar-
keting, 34(1):46–67.
Vargo, S. L., Maglio, P. P., and Akaka, M. A. (2008).
On value and value co-creation: A service systems
and service logic perspective. European management
journal, 26(3):145–152.
Wagner, E. L. and Piccoli, G. (2007). Moving beyond user
participation to achieve successful IS design. Commu-
nications of the ACM, 50(12):51–55.
Integrating Users Logic Into Requirements Engineering for Connected Healthcare co-Design
485
