
USING 3D VISION FOR THE DIAGNOSIS AND TREATMENT
OF AMBLYOPIA IN YOUNG CHILDREN
∗
Angelo Gargantini
Dip. di Ingegneria Informatica e Metodi Matenatici, Universit
`
a di Bergamo, Viale Marconi 5, Dalmine, Italy
Keywords:
Vision rehabilitation, Computer aided vision therapy, Amblyopia, 3D vision.
Abstract:
The 3D4Amb project aims at developing a system based on the NVIDIA 3D Vision for the diagnosis and
treatment of amblyopia in young children. It exploits the active shutter technology to provide binocular vision,
i.e. to show different images to the amblyotic (or lazy) and the normal eye. It would allow easy diagnosis of
amblyopia and its treatment by means of interactive games or other entertainment activities. It should not
suffer from the compliance problems of the classical treatment, it is suitable to domestic use, and it could at
least partially substitute occlusion or patching of the normal eye.
1 INTRODUCTION
Amblyopia, otherwise known as ‘lazy eye’, is reduced
visual acuity that results in poor or indistinct vision in
an eye that is otherwise physically normal, or out of
proportion to associated structural abnormalities. It
may exist even in the absence of any detectable or-
ganic disease. Typically amblyopia is present in only
one eye and is generally associated with a squint or
unequal lenses in the prescription spectacles. This
low vision is not correctable (or only partially) by
glasses or contact lenses.
There exist several causes of amblyopia. Anything
that interferes with clear vision in either eye during
the critical period (birth to 6 years of age) can re-
sult in amblyopia. The most common causes of am-
blyopia are constant strabismus (constant turn of one
eye), anisometropia (different vision/prescriptions in
each eye), and/or blockage of an eye due to trauma,
lid droop, etc. If one eye sees clearly and the other
sees a blur, the good eye and brain will inhibit the eye
with the blur. The brain, for some reason, does not
fully acknowledge the images seen by the amblyopic
or lazy eye. Thus, amblyopia is a neurologically ac-
tive process. The inhibition process (suppression) can
result in a permanent decrease of the vision in that
eye that can not be corrected with glasses, lenses, or
surgery. This condition affects 2-3% of the popula-
tion, which equates to conservatively around 10 mil-
1
This work is partially supported by NVIDIA corp. un-
der the Professor Partnerships program.
lion people under the age of 8 years worldwide.
Amblyopia is currently treated by wearing an ad-
hesive patch over the non-amblyopic eye for several
hours per day, over a period of several months. This
treatment can require up to 400 hours in total to be
effective (Cleary, 2000). This conventional patch-
ing or occlusion treatment for amblyopia often gives
disappointing results for several reasons: it is un-
popular, prolonged, and it can sometimes make the
squint worse because it disrupts whatever fusion there
is. These issues frequently results in poor or non-
compliance and since the success of patching depends
on compliance, it performs on average very poorly.
The treatment by itself works well, but it is often
abandoned because it is too much trouble to take.
Very often, children are averse to wearing a patch
and parents found occlusion difficult to implement
(Dixon-Woods et al., 2006). For this reason, the or-
thoptists and ophthalmologists are continuously look-
ing for a more acceptable solution to the problem, i.e.
an effective treatment that is also complied with and
so really works (Gregson, 2002).
1.1 Computer based Treatment of
Amblyopia
In the last years, several research groups have ex-
perimented treatment of amblyopia by exploiting and
adapting information technologies. There exist sev-
eral Personal Computer (PC) based software pro-
grams that allow vision training but they still require
472
Gargantini A..
USING 3D VISION FOR THE DIAGNOSIS AND TREATMENT OF AMBLYOPIA IN YOUNG CHILDREN.
DOI: 10.5220/0003127204720476
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 472-476
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Figure 1: The I-BiT
TM
system. Copyright University of
Nottingham, printed with permission.
patching of the good eye. The most original system
which does not require patching, is described in the
following.
The VIRART group at the University of Notting-
ham has developed a novel virtual-reality (VR)-based
display system which avoids occlusion of the nonam-
blyopic eye and facilitates the treatment of amblyopia
with both eyes stimulated simultaneously (Eastgate
et al., 2005). This system is called I-BiT
TM2
. The
I-BiT
TM
system itself consists of a viewer which is
linked to a PC. The PC has a standard monitor for
the clinician while the viewer allows binocular vision.
Several types of viewers were tested, like binocular
headsets and several types of viewers called ”cyber-
scopes” similar to that shown in Figure 1.
This system incorporates adapted VR technol-
ogy and specially written software providing interac-
tive 2D and 3D games and videos to the patient via
a stereo (binocular) display. Treatment consists of
watching video clips and playing interactive games in
the clinic with specifically designed software to allow
streamed binocular image presentation. The children
sit in front of the viewer and play with the software
designed for this kind of treatment.
An Evaluation of I-BiT
TM
. The experiments show
that this type of treatment can be efficiently employed
and it performs better than the classical treatment. In
(Waddingham et al., 2006), the results of the use of
I-BiT
TM
in six children are presented. In the case
study, treatment consisted of watching video clips and
playing simple interactive games with specifically de-
signed software to allow streamed binocular image
presentation via I-BiT
TM
. Improvements in vision
were demonstrable within a short period of time, in
some children after 1h of treatment. However, the
proposed treatment has some limits. The kind of hard-
2
http://hfrg.nottingham.ac.uk/ibit/
ware system used makes the treatment rather costly
and performable only in suitable clinic rooms under
the supervision of a doctor (or at least of an adult).
The cure can be performed only for a limited time
and only with precise time scheduling. For these rea-
sons, we believe that the I-BiT
TM
system suffers from
the same problem of compliance of the patching treat-
ment. The goal of this project is to design a system
which could combine the performance of I-BiT
TM
but
be more accessible and usable.
Other research works present similar approaches
by using binocular head mounted display (HMD) or
similar tools to allow binocular vision. At the best
of our knowledge, no group has experimented the use
of the stereo 3D vision systems for the diagnose and
treatment of the amblyopia. In this paper we present
a project, 3D4AMB which is based on the 3D vision,
for the diagnosis and treatment of amblyopia in young
children.
2 USING THE 3D TECHNOLOGY
FOR BINOCULAR VISION
The main goal of this research project, called
3D4AMB, is to develop a system for the diagnosis
and treatment of amblyopia, based on the binocular
vision but that is accessible. With the term “accessi-
ble” we mean:
Inexpensive. The system needs to be relatively low
in cost, it must be affordable by a family. To be so
cheap, the system may be based on standard off
the shelf technologies, which could be bought in
stores open to the general public.
Friendly to Use. The system needs to be friendly in
its use such that the patients can use it without
requiring a particular education or skill. The sys-
tem may be operated autonomously by the chil-
dren themselves and the intervention of an adult
may be limited to initially set up the system (in-
stallation) and to start the treatment at least.
Suitable for Domestic Use. The system can be used
at home without frequent time-consuming visits
to the hospital. In this way, the timing of the treat-
ment can be decided by the patients. It may use
other domestic appliances like standard personal
computers and televisions.
Easily Extensible. It must be possible to easily de-
velop new applications and programs to be added
to the system. For this reason, standards and open
software libraries may be used for developing the
applications.
USING 3D VISION FOR THE DIAGNOSIS AND TREATMENT OF AMBLYOPIA IN YOUNG CHILDREN
473
We have devised a system which has all the above
characteristics and is based on the 3D technologies,
although the goal is not to provide the patients with
the 3D experience but to allow binocular vision. The
classical use of a 3D system is to provide the two eyes
with two different images of the same scene with a
slightly offset viewing angles which correspond to the
different viewpoints of our left and right eye. This vi-
sion produces an illusion of real depth of the scene
and it is the basis of the virtual reality. We exploit
only the capability of the 3D system to send two dif-
ferent images to the eyes while we do not want to
recreate a virtual reality.
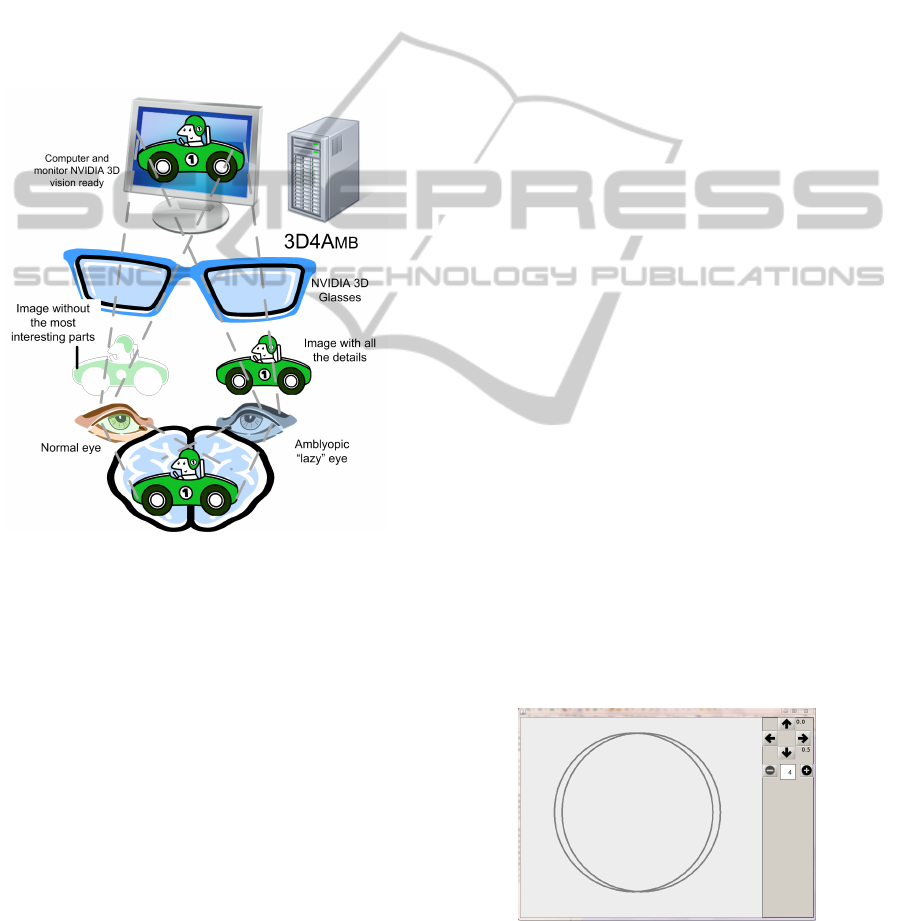
Figure 2: Basic principle of the project.
We have already built a working prototype based
on the NVIDIA
R
3D Vision
TM
technology, although
other 3D technologies may be supported as well in
the future. The NVIDIA 3D vision is based on active
shutter technology which offers full image quality per
eye, wide viewing angle for 3D, excellent 2D Opera-
tion, and acceptable cost.
The system we have developed for 3D4AMB con-
sists in a normal PC desktop connected to a 3D mon-
itor (3D Vision-Ready Display). The PC must be 3D
capable and have all the 3D4AMB software installed
on it. The patient wears the NVIDIA active LCD
shutter glasses that allow viewing a different image
from the left and right eye. The scenario is depicted
in Figure 2.
The basic principle of the system is that the am-
blyopic or ‘lazy’ and the normal eye are shown two
different but related images. This principle can be
used in practice for the treatment of amblyopia, where
the amblyopic eye is shown the more interesting part
of the images of the clip or of the game, while the
non-amblyopic or ‘good’ eye is shown the less inter-
esting part of the image. The content to be shown by
the patient (game or image) is split by 3D4AMB in
two parts, one for the right eye (the amblyopic eye in
the Figure) and one for the left eye (the good eye in
the Figure). The 3D4AMB software will decide what
to send to both eyes depending on the type of treat-
ment suggested by the physician. Note that the lazy
eye of the child is more stimulated to work, but the
non-amblyopic eye is not patched. The patient brain
must join the two images to successfully see the com-
plete image and successfully perform simple tasks in
case of an interactive game. To make sure that the
patient can join the two images there are a significant
number of elements common to both images. Note
that the final image is a bidimensional image because
the goal in not to stimulate the stereo vision of the
patient (at least initially).
2.1 Use Cases of 3D4AMB
We have designed the following use cases that model
the ways we expect 3D4AMB will be used and the
possible interactions with physicians and patients. We
have also developed simple prototype applications to
prove that the designed usage of 3D4AMB is feasible.
Diagnosis. The 3D4AMB system can be used for
the screening and measurement of the amblyopia.
The physician will save the parameters correspond-
ing to the kind of amblyopia and these data will be
reloaded by the 3D4AMB software used by the pa-
tient. In Figure 3 we show a simple application that
permits to measure the squint between the two eyes.
Two circles are shown to the patient, one for each eye.
The two circles are translated until the patient sees
only one circle.
Figure 3: Diagnosis Application.
Passive Image and Movie Viewing. Another use of
3D4AMB is to visualize images and clips. 3D4AMB
HEALTHINF 2011 - International Conference on Health Informatics
474
includes an image and video viewer that is able to
send two different images to both eyes. This activ-
ity, although it is passive, since it does not require any
action by the child, could be performed for prolonged
time and would allow to exercise the lazy eye while
performing activities, like watching movies, likely to
be appealing for children.
Video Games and Exercises. While patching is a
passive method, other treatments which require some
activity on the part of the patients are classified as ac-
tive. Active methods are intended to enhance treat-
ment of amblyopia in a number of ways, including
increased compliance and attention during the treat-
ment periods (due to activities that are interesting for
the patient) and the use of stimuli designed to activate
and to encourage connectivity between certain corti-
cal cell types.
The most advanced and active use of 3D4AMB is
the active playing with interactive games or exercises,
which will stream binocular images. It is well known
that video games can be very useful for visual reha-
bilitation (Achtman et al., 2008). In this settings, the
child plays with a special video game which sends to
the lazy eye all the details while the normal eye will
see only a part of the game scene. To successfully
complete the game the patient must use the informa-
tion shown to the lazy eye (and fuse it with that shown
to the normal eye). In this way, the amblyotic eye
is more stimulated and the fusion encouraged. The
game application can continuously monitor the suc-
cess rate of the game in order to adjust the difficulty
based on the real capability of the player.
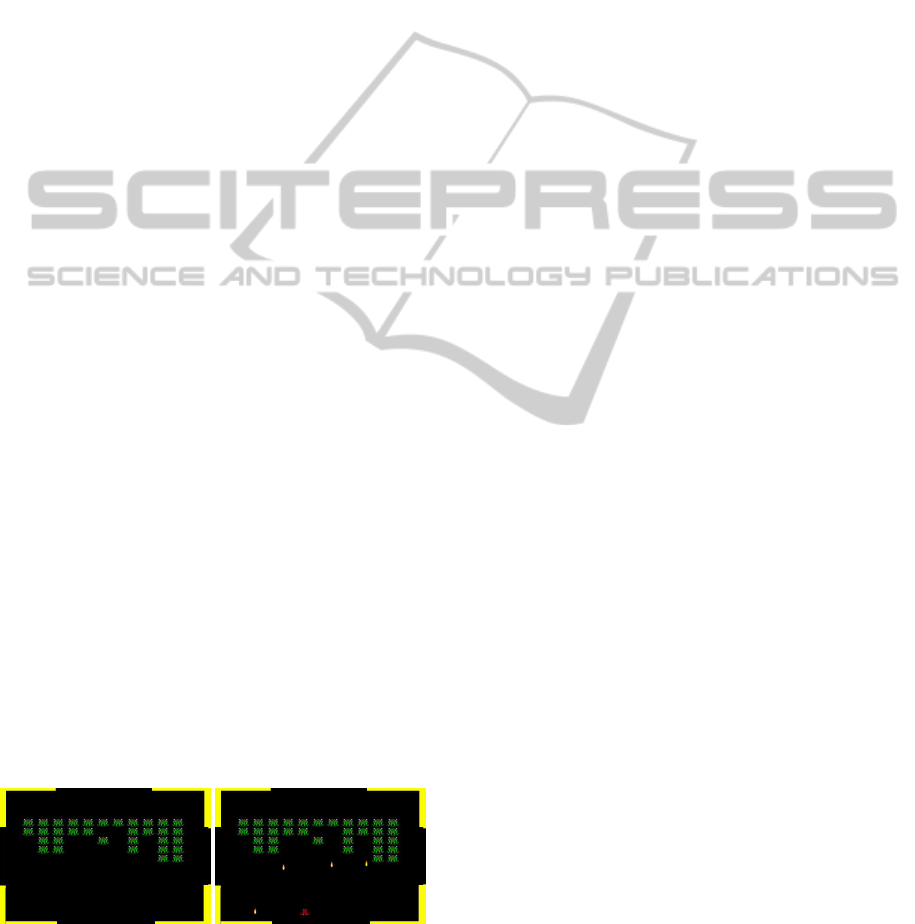
We have developed a small space invaders games
shown in Figure 4 in which the entire scene is pre-
sented to the lazy eye, while the normal eye does
not see the spacecraft (red in the Figure) and the
shots (yellow in the Figure). The player must hit the
invaders (green in the Figure) firing some shots by
pressing the space bar on the keyboard (or a fire but-
ton of a joystick). Some parts of the background (in
yellow in the Figure) are shown to both eyes to facili-
tate fusion.
(a) Normal Eye. (b) Lazy Eye.
Figure 4: Space Invaders Game.
2.2 Software Architecture
The 3D4AMB software is based on several compo-
nents which facilitate the development of new ap-
plications. The system works only (up to now)
on a PC with Microsoft Windows
R
Vista 32/64-bit
or Windows 7 32/64-bit Operative systems with the
NVIDIA 3D Vision drivers and with Sun Microsys-
tems Java Runtime Environment. It is based on the
Java OpenGL (JOGL) which is a wrapper library that
allows OpenGL to be used in the Java programming
language. It is currently an independent open-source
project under the BSD license and on Jadis (Java Ad-
vanced Display Infrastracture for Stereo) which pro-
vides a common interface for displaying Swing GUI
components in stereo.
3 CONCLUSIONS
In this paper we have presented a system, 3D4AMB,
for the diagnosis and treatment of amblyopia in young
children which is based on 3D vision technologies.
The 3D vision is exploited to allow the binocular vi-
sion, i.e. to send different images to the normal and
the lazy eye, in order to exercise and stimulate the lazy
eye and the brain to fuse the images in an unique view.
We have presented several use cases supported by
prototypes we have developed using Java and JOGL
technologies for stereo viewing. The system has been
devised with the goal to improve compliance with
the treatment. It should not suffer from the non-
compliance problems of the classical patching treat-
ment. The children should enjoy the domestic use of
3D4AMB games and exercises, allowing prolonged
therapy and the system promise to be inexpensive
enough to foster its usage.
REFERENCES
Achtman, R., Green, C., and Bavelier, D. (2008). Video
games as a tool to train visual skills. Restorative Neu-
rology and Neuroscience, 26(4-5):435–446.
Cleary, M. (2000). Efficacy of occlusion for strabismic am-
blyopia: can an optimal duration be identified? British
Journal of Ophthalmology, 84(6):572–578.
Dixon-Woods, M., Awan, M., and Gottlob, I. (2006).
Why is compliance with occlusion therapy for ambly-
opia so hard? a qualitative study. Arch Dis Child,
91(6):491494.
Eastgate, R. M., Griffiths, G. D., Waddingham, P. E.,
Moody, A. D., Butler, T. K. H., Cobb, S. V., Comaish,
I. F., Haworth, S. M., Gregson, R. M., Ash, I. M., and
USING 3D VISION FOR THE DIAGNOSIS AND TREATMENT OF AMBLYOPIA IN YOUNG CHILDREN
475

Brown, S. M. (2005). Modified virtual reality technol-
ogy for treatment of amblyopia. Eye, 20(3):370–374.
Gregson, R. (2002). Why are we so bad at treating ambly-
opia? Eye, 16(4):461–462.
Waddingham, P. E., Butler, T. K. H., Cobb, S. V., Moody,
A. D. R., Comaish, I. F., Haworth, S. M., Gregson,
R. M., Ash, I. M., Brown, S. M., Eastgate, R. M.,
and Griffiths, G. D. (2006). Preliminary results from
the use of the novel interactive binocular treatment (I-
BiT[trade]) system, in the treatment of strabismic and
anisometropic amblyopia. Eye, 20(3):375–378.
HEALTHINF 2011 - International Conference on Health Informatics
476
