
QUALITY ASSESSMENT IN COLONOSCOPY
New Challenges Through Computer Vision-based Systems
Fernando Vilari˜no
Computer Vision Center and Computer Science Dep. Universitat Aut`onoma de Barcelona, Spain
Gerard Lacey
Graphics, Vision and Visualisation Group (GV2), School of Computer Science and Statistics, Trinity College Dublin, Ireland
Keywords:
Colonoscopy, Quality assessment, Eye-tracker, Computer vision, Polyps, Colon cancer.
Abstract:
The assessment of the quality of the colonoscopic interventions arises as a most relevant issue once the number
and the availability of these clinical procedures are increased day by day. The use of the latest computer vision-
based techniques can provide the physician with both qualitative and, most important, objectively verifiable
quantitative indicators of performance. In this paper we present a study in which we propose the automatic
analysis of colonoscopy video for the quality assessment of the intervention from different points of view:
1) We propose the characterization of the different parts of the colon in order to obtain metrics of the time
used for navigation, portion of gut analyzed, etc. 2) We analyze the image contents in order to automatically
characterize the presence of polyps. 3) We use the information obtained by and eye-tracker in order to assess
the physician’s skills.
1 COLON CANCER AND
INTESTINAL SCREENING
1.1 Colon Cancer in Numbers
The main lesions associated to the intestine are:
bleeding, lump, ulcer, Crohn disease, and cancer.
During the last 20 years, colon cancer has been
the second leading cause of cancer deaths in the
United States, behind lung cancer, with approxi-
mately 60, 000 deaths per year as shown in O’Brien’s
report (O’Brien et al., 1990), and also analyzed in
other studies (U.S. Department of Health and Human
Services, 2003). America Cancer Society’s 2007 re-
port (American Cancer Society, 2007) provides an ex-
tended summary of facts and statistics about colon
cancer prevalence and impact in the population. Col-
orectal cancer is the second leading cause of cancer-
related deaths in Singapore and Europe (Ministry of
Health Singapore, 1990). Although colon screening
has become the main alternative for prevention of col-
orectal cancer, recent data suggest that there is a sig-
nificant miss-rate for the detection of even relatively
large polyps and cancer (Pabby et al., 2005). For this
reason, special efforts havebeen focused on the devel-
opment of computer-aided systems for the detection
of this type of pathologies. Nowadays, novel lines
of research are oriented to widen this perspective by
means of the implementation of objective indicators
for the assessment of the procedures used in colon
screening, since the miss rate of polyps is highly cor-
related to elements such as the quality of the prepa-
ration, the time consumed for the intervention, the
amount of intestinal surface screened, the kills of the
physician in the manipulation of the endoscope, etc.
Moreover, this indicators present a potential value for
the training of future endoscopists as reference values
to measure abilities in and objective way.
1.2 Screening Technics
Intestinal endoscopy is referred to as the technique
for screening the intestinal lumen. For the case
of large intestine, this technique receives the name
of colonoscopy. Fiberoptic colonoscopy (FOC) is
widely accepted as the definitive method for diagno-
sis of colonic polyps. FOC allows direct visualiza-
tion of the intestinal surface and affords the possibil-
ity of obtaining a in-situ biopsy as well as cauteriza-
320
Vilariño F. and Lacey G. (2009).
QUALITY ASSESSMENT IN COLONOSCOPY - New Challenges Through Computer Vision-based Systems.
In Proceedings of the International Conference on Biomedical Electronics and Devices, pages 320-325
DOI: 10.5220/0001780703200325
Copyright
c
SciTePress
tion and clinical intervention such as polyp removal
(Winawer et al., 1997). FOC is a minimal invasive
surgery (Hunter and Sackier, 1993), (Hulka and Re-
ich, 1994) consisting of the introduction through the
anus of a flexible probe which a camera and an il-
lumination device on its tip. The probe consists of
a flexible cable which can be controlled by the ex-
pert in order to reach every part on the intestinal wall.
There exist several reference books regarding clini-
cal colonoscopy for the reader interested in deepen-
ing in the specificities of colonoscopy, amongst which
Kato’s textbook (Kato and Baron, 2003) can provide
an insightful introductory view. Several authors have
assessed that endoscopic images possess rich infor-
mation (Nagasako et al., 1998), which facilitates the
abnormality detection by multiple techniques (Zheng
et al., 2005). The main drawbacks related with FOC
can be enumerated as follows (Winawer et al., 1993),
(Eddy, 1990): risks of perforation; costs of the inter-
vention; difficulty in visualizing the 100% of the in-
testinal surface; high number of patients for a reduced
number of specialists provide a stress and shrink in
the intervention time; difficult visualization due to
the intestinal content; preparation needed; imprecise
localization of events for a subsequent interventions,
and high rate of negative results in inspections look-
ing for polyps (Gokturk and Tomasi, 2001).
In the last years, other modalities for the visual-
ization of the colon have arisen. One of the most
relevant is virtual colonoscopy, a technique consist-
ing of the construction of a virtual 3D model of the
colon from computed tomography (CT) data (Liang
et al., 2004), and for this reason several authors have
proposed automatic techniques for the detection of le-
sions in this modality of images. On the other hand,
Wireless Capsule Video Endoscopy (WCVE) (Iddan
and Meron, 2000) has devoted particular attention, re-
cently. WCVE (Fireman et al., 2002) consists of a
capsule with a camera, a battery and a set of led lamps
for illumination attached to it, which is swallowed by
the patient, emitting a radio frequency signal which is
received and stored in an external device. The result
is a video movie which records the trip of the capsule
along the intestinal tract with a rate of two frames
per second, and that can be easily downloaded into
a PC with the camera software installed. It is much
less invasive, since the patient simply has to swallow
the pill, which will be expelled in the normal cycle
through defecation. Moreover, there is no need of
hospitalization nor expert support through the process
and the patient can lead an ordinary life, since the at-
tached device is recording the video movie emitted
by the camera in the capsule (Vilari˜no, 2006; Vilari˜no
et al., 2009). However, although these new modalities
provide new ways of clinical analysis, colonoscopy is
the reference technique for clinical intervention in the
case of colon screening and colon cancer.
2 COMPUTER VISION FOR
QUALITY ASSESSMENT
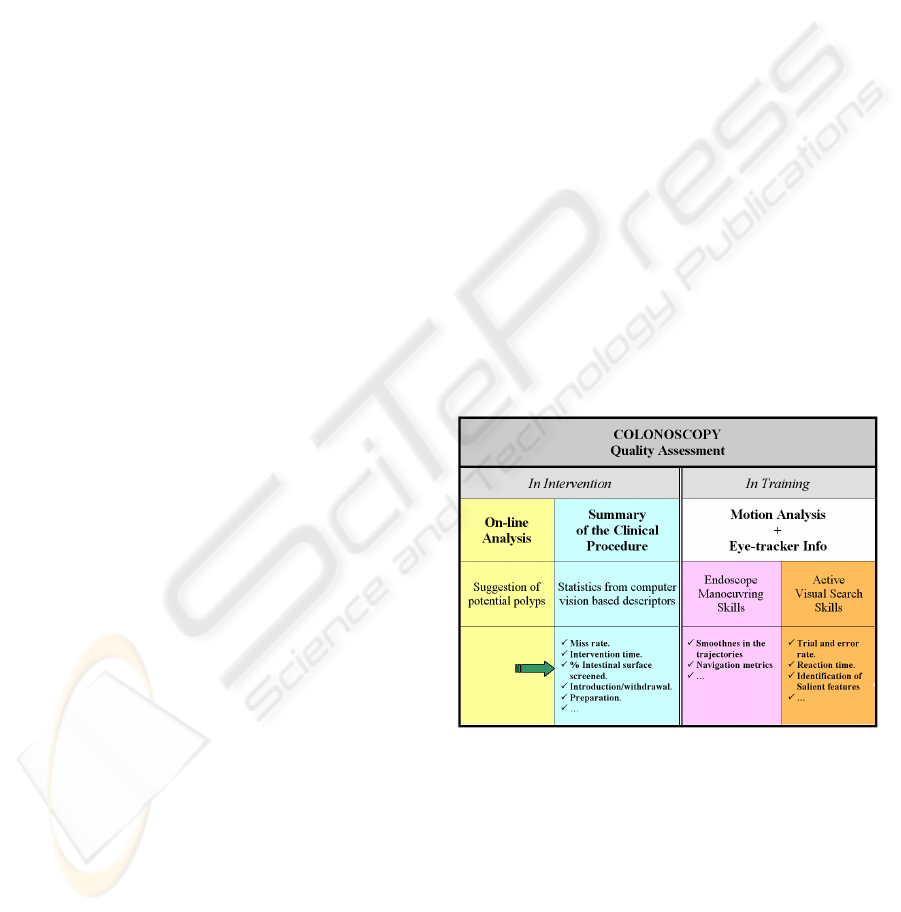
We state that computer vision-based techniques can
be used in order to obtain objective indicators of the
quality of the interventions in an automatic way. Our
approach provides a framework for the quality assess-
ment which is implemented in the following 3 areas
in which we are developing our research, namely: 1)
Computer-aided intervention: On-line detection and
characterization of potential targets in intervention-
time, 2) Post-interventional quality metrics: Auto-
matic computation of the quality measures related
to the intervention such as quality of preparation,
amount of bowel surface visualized, time measures,
etc. 3) Evaluation of skills: Analysis of 3D trajec-
tories of the endoscopes and the screening behavior.
For this final point, we propose to use the trajecto-
ries together with the information obtained from the
tracking of the gaze position of trainees in order to
assess their skills. The perspective presented in this
paragraph is graphically depicted in Figure 1.
Figure 1: Our framework for automatic quality assessment
in colonoscopy.
3 COLON CANCER: CLINICAL
CHARACTERIZATION
Colon cancer has devoted wide attention in many
studies in order to find proper descriptions and cat-
egorization (Rembacken et al., 2000), (Saitoh et al.,
2001), (Paris Workshop Participants, 2003). Adeno-
matous polyps, particularly those larger than 1 cm in
QUALITY ASSESSMENT IN COLONOSCOPY - New Challenges Through Computer Vision-based Systems
321

diameter, are the most likely precursors of colorectal
carcinoma (Gokturk and Tomasi, 2001), (Thoeni and
Laufer, 1994). The main features used for cancer and
general abnormality characterization are: color, shape
and texture.
• Color. Color colonoscopic images tend to ex-
hibit the same color features for the same colon
status (Kato and Baron, 2003). Malignant tu-
mors are usually inflated and inflamed and this in-
flammation is usually reddish and more severe in
color than the surrounding tissues. Benign tumors
exhibit less intense hues. Redness may specify
bleeding and black may be treated as deposits due
to laxatives. Green may be the presence of fae-
cal materials, which are not clear during the pre-
operative preparation, and yellow relates to pus
formation (Tjoa and Krishnan, 2003).
• Shape. Shape is a relevant cue since polyps are
associated to rounded or peduncular shapes. Pe-
duncular polyps are relatively easy to visualize
during a screening session. Flat polyps present
a higher difficulty, and in addition, they are more
likely to develop into malignant polyps.
• Texture. Texture is known to be an important
cue to be evaluated for the discrimination between
malignant and benign lesions (Kudo and Kashida,
2000), (Nagata et al., 2000).
The high-level characterization of cancer ex-
plained above is usually translated into an image-
based feature extraction stage, focused on color, tex-
ture or shape cues. Following the feature extraction,
a discrimination procedure, based on simple compar-
isons or more sophisticated machine learning tech-
niques must be applied. In our approach, efficient
methods for color, texture and shape characteriza-
tion must be oriented towards the high speed require-
ments of on-line procedures. The use of histogram
quantization (HQ) (Swain and Ballard, 1991) and the
use of different color spaces (Paschos, 2001) in a
whole-image level (Hai et al., 2006) or a multi-scale
framework (Li et al., 2005) for color; Gray level
co-occurrence matrices (GLCM) (Srivastava et al.,
2005), fractal dimension (Chaudhuri and Sarkar,
1995), histograms of oriented gradients (HOG) (Won
et al., 2002) and wavelets (Karkanis et al., 2001) for
texture; and MPEG-7 descriptors and others for shape
(Coimbra and Cunha, 2006) should be adapted to run
online in order to provide a efficient characteriza-
tion of our system. This orientation towards the real
time performance of discriminant features is one of
the most relevant challenges of our current line of re-
search.
Figure 2: Three polyps: flat, peduncular and mixed. Pedun-
cular polyps are prone to their development into malignant
cancers.
In recent works we presented preliminary results
of discriminative features and classification systems
for colon cancer detection and its a posteriori char-
acterization in different types of polyps. Figure 2
shows examples of a) peduncular,b) flat and c) mixed
polyps, which have a different degree of clinical rel-
evance, as appearing in our latest contribution (Vi-
lari˜no et al., 2007). Our next step is, hence, to
put these techniques in the horizon of real-time per-
formance. In addition, we argue that the use of
mixed strategies (color/texture/shape) for characteri-
zation would potentially provide a reacher informa-
tion than each of them alone, and the study of the
selection of appropriate features represents an open
field of research.
4 POST-INTERVENTIONAL
QUALITY METRICS
We state that computer vision-based techniques can
be used in order to provide post-interventionalmetrics
in an automatic way. We define four main lines or
research in this area:
1. Automatic estimation of presence of intestinal
content for the assessment of the quality of the
preparation.
2. Percentage of the intestine visualized.
3. Measure of the intervention time.
4. Automatic detection of the different moments
of the intervention (introduction of the endo-
scope/withdrawal).
5. Characterization of the motion of the endoscope.
All these points can be gathered into a general
framework which could be stated in the following
way: The definition of a 2D map of the patient’s gut
in order to have patient-oriented representation of the
colon, together with their singular features, lesions,
etc. In order to get this wide target, color, textural and
motion features must be used together. Color appears
as a main cue for intestinal content characterization
BIODEVICES 2009 - International Conference on Biomedical Electronics and Devices
322

Figure 3: Eye-tracker configuration system.
(Vilari˜no et al., 2006). Texture can provide a descrip-
tion of the intestinal folds, and motion characteriza-
tion is essential for the measure of transition times. In
a addition, deeper studies must be performed in order
to build up a large database of cases which allows us
to carry out statistical test with the aim of unveiling
the most suitable features and indicators for quality
measures.
5 EYE-TRACING INFORMATION
FOR SKILL ASSESSMENT
The last line of research we introduce in this paper is
related to the assessment of the skills of the trainees
in endoscopy training programs. We hold that using
both the information of the trajectories of the endo-
scopes -which can be potentially obtained by means
of the analysis of the camera movement- and the
tracking of the gaze position -which can be obtained
by an eye-tracker device-, we can provide objective
indicators for the evaluation of the skills. Moreover,
it will be possible to characterize those skills sepa-
rately: ability in endoscope manipulation vs. visual
search.
An eye tracker consists of an adjustable device
with a set of cameras pointing towards the user’s eyes.
The eye tracking procedure involves the recording of
the gaze position and the translation of this values into
the location on the image where the user is focusing
the attention. Figure 3 showsa scheme of the EyeLink
II eye-tracker which was used for our experiments.
The video signal from the cameras is sent to a host
PC in which the eye tracker software is installed, and
which communicates to the experiment PC in which
the visual stimuli are shown. The pupil position is
then translated into gaze position on the stimuli screen
at a very high speed (up to one record each four mil-
liseconds).
6 RESULTS
In this position paper, we would like to highlight pre-
liminary results which were obtained in the colon
cancer characterization and eye-tracker based analy-
sis. The computation of automatic quality assessment
measures is a key part of our ongoing research, and
it will be analyzed in more detail in the Discussion
section.
The eye-tracker information can be used to la-
bel massive data by using the gaze position of the
specialist while screening the colonoscopy video off-
line (in a post-interventional session). Those areas
the specialist is steering the sight towards are asso-
ciated to visual salient features which are of inter-
est for the colonoscopists. This has two main con-
sequences: On the one hand, we can build up an an-
notated database of clinical cases in which the posi-
tion of the observer’s gaze determines the position of
the cancer screened. On the other hand, we can use
the information of the the gaze trajectory to charac-
terize the abilities of the experts in the visual search.
In our case, we built up a database consisting of 6
cases, which is freely accessible for the public and
from the following link:
hhtp://www.cs.tcd.ie/
colon/colon_et_database.zip
.
We used this database to for the experiments as-
sociated to the colon cancer detection and character-
ization. We applied support vector machine classi-
fiers (SVM) (Vapnik, 1995) in order to distinguish
between polyp images and random images of 6 dif-
ferent videos. Each image was 500x700 pixels. We
manually selected those frames were the polyps were
present, and then we trained the classifier with exam-
ples of polyps and non-polyps patches of 128x128
pixels by using the gray-level image, achieving a
working point of around 80% of both sensitivity and
specificity. The visual analysis of these data pro-
vided promising results in the clustering of the dif-
ferent types of polyps into three basic types (pedun-
cular, flat and mixed). For a further analysis of these
results we refer to the IbPria conference proceedings
(Vilari˜no et al., 2007).
Regarding the analysis of the visual trajectories
obtained from the eye-tracker, we carried out a new
set of experiments in which 20 full colonoscopy stud-
ies were annotated in a two-stage strategy: 1) First,
the expert manually selected those sections of the
video study in which the expert detected the presence
of cancer -this action was performed by clicking and
holding a mouse during the visualization of the polyp-
. 2) Then, only those parts of the video selected by the
specialist in the previous stage were screened with the
eye-tracker. We repeated this experiment with differ-
QUALITY ASSESSMENT IN COLONOSCOPY - New Challenges Through Computer Vision-based Systems
323

ent experts and novicesin order to look for differences
in annotation. The results, which are to be deeply ana-
lyzed in a current study to be submitted in a forthcom-
ing publication, point out that experts and trainees
show different behaviors in the visual search in terms
of reaction time, frequency of saccades, geometry of
the 3D trajectories of the gaze position, etc. These
preliminary results show statistical significance, and
they must be contrasted in terms of inter- and intra-
observer variability. This is one of the most relevant
drawbacks of this kind of studies since, the time avail-
ability of the physicians is a major constraint for large
validation studies.
7 DISCUSSION
The preliminary results shown above pave the way
to the computation of quality assessment measures.
For the case of polyps detection, the main aim is to
provide the physician with candidates of polyps to
be analyzed during the intervention. Different statis-
tics, such as the number of polyp-candidates analyzed
and not analyzed, total time consumed in this analy-
sis, etc., can be pulled out in order to obtain objective
indicators. These statistics and indicators must be de-
fined together with the physicians in order to get clin-
ical significance and the appropriate tolerance levels.
For the case of eye-tracker data, statistically sig-
nificant indicators of the physicians’ visualization
skills are of relevant importance in a two-fold way:
First, we would be able to provide the physician with
objective metrics that measure high level skills, such
as reaction time, search activity, robustness of the
search pattern, etc., together with general indicators
such as miss rate of polyps. In addition to the for-
mer, we make it possible to decouple the manoeuver-
ing ability from the visual search skills in an objective
way. This information, together with the motion anal-
ysis, can provide indicators regarding the smoothness
of the trajectories that the endoscope performs.
Finally, the automatic estimation of presence of
intestinal content, the quality of the preparation, the
percentage of the intestine visualized, the measure of
the intervention time, and the automatic detection of
the introduction and withdrawal stages must be put
into a clinical framework of quality assessment. This
provides both a study-based assessment and, into a
historical archive, a log of the physician’s indicators
along different interventions. In order to get this done,
a full study is being performed currently together with
the Royal College of Surgeons of Ireland, funded by
an Enterprise Ireland project of the Irish government
for the acquisition and annotation of a full database
of 100 cases of colonoscopy showing colon cancer in
high definition videos. This database comprises sev-
eral tera bytes of video data and its corresponding an-
notation both in manual and eye-tracked versions by
several specialists with different levels of expertise.
8 CONCLUSIONS
Quality assessment of colonoscopy videos is a rele-
vant issue, since the evaluation of different aspects
of the intervention, by providing objective indicators,
sets up the foundations for a control and reduction of
miss rates in colon cancer detection. We proposed an
approach of quality assessment by means of computer
vision-based techniques which is underpinned by: 1)
The automatic suggestion of potential candidates of
colon cancer during the intervention time, 2) The au-
tomatic computation of objective quality metrics after
the intervention, and 3) The use of eye-tracking in-
formation in order to provide metrics to evaluate the
skills of the physician both in the visual search and
in the endoscope manoeuvering. Preliminary results
showed the suitability of such techniques for polyp
detection and experts vs. trainees discrimination. The
deeper analysis of quality metrics and their correla-
tion is devoted to a further piece of research whose
study our team is carrying out currently.
ACKNOWLEDGEMENTS
We would like to acknowledge the collaboration of
M.D Steven Patchett and M.D Hugh Mulcahy, from
the Royal College of Physicians of Ireland, for their
collaboration in the clinical study of this work. This
research is supported by Enterprise Ireland contracts
PC-2006-038 and CFTD-2006-216.
REFERENCES
American Cancer Society (2007). Cancer Facts and Figure.
American CancerSociety.
Chaudhuri, B. and Sarkar, N. (1995). Texture segmentation
using fractal dimension. IEEE Trans. Pattern Anal.
and Mach. Intel., 17:72–77.
Coimbra, M. and Cunha, J. (2006). MPEG-7 visual descrip-
tors: Contributions for automated feature extraction
in capsule endoscopy. IEEE Transactions on Circuits
ans Systems for Video Technology, 16(5):628–637.
Eddy, D. (1990). Screening for colorectal cancer. Annals of
Internal Medicine, 113:373–384.
BIODEVICES 2009 - International Conference on Biomedical Electronics and Devices
324

Fireman, Z., Glukhovsky, A., et al. (2002). Wireless cap-
sule endoscopy. Israel Medical Association Journal,
4:717719.
Gokturk, S. and Tomasi, C. o. (2001). A statistical 3-d pat-
tern processing method for computer-aided detection
of polyps in ct colonography. IEEE Transactions on
Medical Imaging, 20(12):1251–1260.
Hai, V., Echigo, T., et al. (2006). Adaptive control of video
display for diagnostic assistance by analysis of cap-
sule endoscopic images. In ICPR, volume III, pages
980–983.
Hulka, J. and Reich, H. (1994). Textbook of Laparoscopy.
W.B. Saunders, Phipladelphia, PA, 2 edition.
Hunter, J. and Sackier, J. (1993). Minimally invasive
surgery. McGraw-Hill, New York.
Iddan, G. and Meron, G. e. a. (2000). Wireless capsule
endoscopy. Nature, 405:4–7.
Karkanis, S., Iakovidis, D., et al. (2001). Detection of le-
sions in endoscopic video using textural descriptors on
wavelet domain supported by artificial neural network
architectures. In ICIP, volume II, pages 833–836.
Kato, H. and Baron, J. (2003). Electronic Videoendoscopy.
Jpapan: Harwood Academic Publisher.
Kudo, S. and Kashida, H. e. a. (2000). Colonoscopic diag-
nosisi and management of nonpolypod and early col-
orectal cancer. World Journal of Surgery, 24(9):1081–
1090.
Li, P., Chan, K., et al. (2005). Learning a multi-size patch-
based hybrid kernel machine ensemble for abnormal
region detection in colonoscopic images. In CVPR,
volume II, pages 670–675.
Liang, J., Higgins, W., et al. (2004). Introduction to the spe-
cial section on virtual endoscopy. IEEE Transactions
on Medical Imaging, 23(11):1333–1334.
Ministry of Health Singapore (1990). MOH Annual Report.
Ministry of Health Singapore.
Nagasako, K., Fijimori, Y., et al. (1998). Atlas of gas-
troenterologic endoscopy by High-Resolution Video-
endoscopy. Igaku-Shoin Ltd. Tokyo.
Nagata, S., Tanaka, K., et al. (2000). Pit pattern diag-
nosis of early colorectal carcinoma by magnifying
colonoscopy: clinical and histological implications.
International Journal of Oncology, 16(5):927–934.
O’Brien, M., Winawer, S., et al. (1990). The national
polyp study: Patient and polyp characteristics asso-
ciated with high-grade dysplasia in colorectoral ade-
nomas. Gastroenterology, 98:371–379.
Pabby, A., Schoen, R., et al. (2005). Analysis of colorec-
tal cancer occurence during surveillance colonoscopy
in the dietary prevention trial. Gastrointestinal en-
doscopy, 61(3):385–391.
Paris Workshop Participants (2003). The Paris endospcopic
classification of superficial neoplastic lesions. Gas-
trointestinal Endoscopy (Supplement), 58(6):3–23.
Paschos, G. (2001). Perceptually uniform color spaces for
color texture analysis: empirical evaluation. IEEE
Trans. Image Processing, 10:932–937.
Rembacken, B., Fuji, T., et al. (2000). Flat and de-
pressed colonic neoplasms: A pospective study of
1000 colonoscopies in the uk. Lancet, 17:1157–1167.
Saitoh, Y., Waxman, A., et al. (2001). Prevalence and dis-
tinctive biologic features of flat colorectal adenomas
in a north american population. Gastroenterology,
120:1657–1665.
Srivastava, S., Rodriguez, J., et al. (2005). Analysis of con-
focal microendoscope images for automatic detection
of ovarian cancer. In ICIP, volume I, pages 1113–
1116.
Swain, M. and Ballard, D. (1991). Color indexing. Journal
of computer vision, 7(1):11–32.
Thoeni, R. and Laufer, I. (1994). Textbook of gastrointesti-
nal radiology, chapter Polyps and Cancer, page 1160.
Philadelphia, PA: Sanders.
Tjoa, M. and Krishnan, S. (2003). Feature extraction for the
analysis of colon status from the endoscopic images.
BioMedical Engineering OnLine, 2(9).
U.S. Department of Health and Human Services (2003).
Cdc, the importance of prevention and early detection
cdc. http://www.cdc.gov/cancer/colorectal/.
Vapnik, V. (1995). The nature of statistical learning theory.
Springer.
Vilari˜no, F. (2006). A machine learning approach for in-
testinal motility assessment with capsule endoscopy.
PhD thesis, Dept. Computer Science, Universitat Au-
tonoma de Barcelona, Spain.
Vilari˜no, F., Lacey, G., et al. (2007). Automatic labeling
of colonoscopy video for cancer detection. LNCS,
4477:290–297.
Vilari˜no, F., Spyridonos, P., et al. (2006). Automatic de-
tection of intestinal juices in wireless capsule video
endoscopy. In Pattern Recognition, ICPR, volume 4,
pages 719– 722.
Vilari˜no, F., Spyridonos, P., et al. (2009). Intestinal motil-
ity assessment with video capsule endoscopy: Au-
tomatic annotation of phasic intestinal contractions.
IEEE Trans. on Medical Imaging (in press).
Winawer, S., Fletcher, R., et al. (1997). Colorectal cancer
screening: Clinical guideliness and rationale. Gas-
troenterology, 112:594–642.
Winawer, S., Zauber, A., et al. (1993). Prevention of col-
orectal cancer by colonoscopy polypectomy. New
England Journal of Medicine, 329:977–981.
Won, C., Park, D., et al. (2002). Efficient use of MPEG-7
edge histogram descriptor. ETRI, 24(1):23–30.
Zheng, M., Krishnan, S., et al. (2005). A fusion-based clin-
ical decision support for disease diagnosis from endo-
scopic images. Computers in Biology and Medicine,
35(3):259–274.
QUALITY ASSESSMENT IN COLONOSCOPY - New Challenges Through Computer Vision-based Systems
325
