
ENHANCING CONTEXT ANALYSIS WITH INTELLIGENCE IN
PROVIDING e-HEALTH SERVICES
Less Infrastructure Dependency in Supporting Cardio-Vascular Patients
Boris Shishkov
IICREST / Department of Systems Engineering, TU Delft, Jaffalaan 5, Delft, The Netherlands
Alexander Verbraeck
Department of Systems Engineering, TU Delft, Jaffalaan 5, Delft, The Netherlands
Ing Widya
Department of Computer Science, University of Twente, Drienerlolaan 5, Enschede, The Netherlands
Keywords: Context-aware applications, Software components, e-Health services, Intelligent patient support.
Abstract: In Europe, we observe an increasing number of people with health problems, who could theoretically
receive care outside of a hospital when their condition could be properly monitored. Not being able to
provide this monitoring leads to an increasing pressure on an already overcrowded hospital system and
increased costs. Ubiquitous technology on top of a high-quality IT infra-structure has already proven to be
able to provide partial solutions. However, such infrastructure is not available throughout Europe. This
brings the challenge of finding cheap, adaptive, and less infrastructure-dependent technological solutions. In
the current paper we propose some solution ideas concerning the mentioned problems, which ideas are
rooted in context analysis. In particular, we take context into account because adequately adapting the
delivered services to the situation of the patient could result in more effective support. We incorporate
multi-level context states and distinguish between some perspectives on context states for the design of
flexible and adaptive ICT applications. The IT system autonomously considers context not only for the
patient but also for the other related stakeholders such as caregivers. We illustrate our ideas with an example
concerning cardio-vascular patients and expect the solutions to be extendable to other health care domains.
The results can be generalized to also derive more fundamental knowledge on the possible ways in which
context-aware solutions can be applied.
1 INTRODUCTION
In Europe, we observe an increasing number of
people with health problems, who could
theoretically receive care outside of a hospital when
their condition could be properly monitored. Not
being able to provide this monitoring leads to an
increasing pressure on an already overcrowded
hospital system and increased costs.
Ubiquitous technology on top of a high-quality
IT infrastructure has already proven to be able to
provide partial solutions. Tele-monitoring has been
researched for years and the achieved results are
more impressive than just hearing the heartbeat of a
patient in Australia from The Netherlands, for
example. There are more advanced things that could
be done, such as the monitoring of epileptic patients
at home and offering them immediate help when
needed (A-MUSE Project, 2008), to mention just an
example. These examples point, nevertheless, to
multidisciplinary challenges, as they involve
medical, logistical, and ICT issues. We approach the
development of ICT applications from this
multidisciplinary perspective, analyzing achieved
results and proposing new solutions. A starting point
we consider is appropriately analyzing context in
414
Shishkov B., Verbraeck A. and Widya I. (2009).
ENHANCING CONTEXT ANALYSIS WITH INTELLIGENCE IN PROVIDING e-HEALTH SERVICES - Less Infrastructure Dependency in Supporting
Cardio-Vascular Patients.
In Proceedings of the 4th International Conference on Software and Data Technologies, pages 414-420
DOI: 10.5220/0002314004140420
Copyright
c
SciTePress

developing applications and this concerns context
modeling abstractions and a context handling
platform. The context modeling abstractions provide
application developers with proper conceptual
foundations that can be extended and specialized
with specific application requirements. The context
handling platform allows some application
functionality to be delegated to the platform, which
reduces application development effort, time and,
therefore, costs.
Until recently, computation was limited to an
interaction style in which users provide to a desktop
computer all the required input to perform particular
tasks. Nowadays, computation is evolving to an
interaction style in which explicit user intervention
is gradually less required (Shishkov & Van
Sinderen, 2008). Explicit user inputs are being
progressively replaced by conditions detected by
sensors, devices and computers distributed in the
environment. Hence, technological advances support
(or enable) the shift of computing from the desktop
paradigm into a paradigm in which computing is
immersed in the dynamic world where we live and
act (Moran & Dourish, 2001). This paradigm shift
poses many challenges, mainly related to whom,
how, when and where to deliver services in the
myriad of situations that can be encountered in the
real world, which is the ever-changing context of
use. In this view, capturing and monitoring the
context in which services should be delivered, and
adapting services according to the context and user
preferences are essentially needed.
The underlying goal considered in this paper is
finding cheap, adaptive, and less infrastructure-
dependent technological solutions in the above-
discussed perspective. We propose solution
directions concerning these problems, which are
rooted in context analysis. In particular, we take
context into account because adequately adapting
the delivered services to the situation of the patient
could result in more effective support. We
incorporate multi-level context states and distinguish
between some perspectives on context states for the
design of flexible and adaptive ICT applications.
The IT system autonomously considers context not
only for the patient but also for the other related
stakeholders. We illustrate our ideas with an
example concerning cardio-vascular patients and
expect the solutions to be extendable to other health
care domains. The results can be generalized to also
derive more fundamental knowledge on the possible
ways in which context-aware solutions can be
applied.
With respect to the issue of providing support to
cardio-vascular patients, it is to be noted that
solutions to support the monitoring and help in case
of emergency of patients require big investments and
good IT infrastructure, which is often not the case in
more isolated European countries, such as Bulgaria
and Romania, while at the same time the severity of
cardio-vascular problems is high there also. In these
countries, some people with heart problems (often
elderly people) who sometimes have nobody to take
care of them, and who often suffer from lung and
other problems (for instance, Chronic Obstructive
Pulmonary Disease - COPD) at the same time, can
rely on very limited support from the state, which
makes it unrealistic to expect to apply advanced
technology in the same way in which this is done in
countries, such as Switzerland and The Netherlands.
Therefore, innovative solutions building on a robust
IT architecture are needed. For these particular
problems, the use of context awareness is expected
to provide the basis for a multidisciplinary solution.
The outline of this paper is as follows: Section 2
is furthering the discussion on context-awareness,
including a detailed analysis and presenting our
proposed views. Section 3 contains the running
example that will be reflected in Section 4 in which
we will partially illustrate our proposed views,
elaborate more on our solution directions, and
generalize the results accomplished. Finally, Section
5 contains the conclusions.
2 ENHANCING CONTEXT
ANALYSIS
Context-aware applications are (in tune with the
discussion so far) primarily motivated by their
potential to increase user-perceived effectiveness,
i.e. to provide services that better suit the needs of
the end-user, by taking into account the user
situation (Shishkov & Van Sinderen, 2008). We
refer to the collection of parameters that determine
the situation of an end-user, and which are relevant
for the application in pursue of user-perceived
effectiveness, as end-user context, or context for
short (as according to literature (Shishkov et al.,
2008)). Context-awareness implies that information
on the end-user context must be captured, preferably
without conscious or active involvement of the end-
user. Although in principle the end-user could also
provide context information by directly interacting
with the application, one can assume that in practice
this would be too cumbersome if not impossible; it
ENHANCING CONTEXT ANALYSIS WITH INTELLIGENCE IN PROVIDING e-HEALTH SERVICES - Less
Infrastructure Dependency in Supporting Cardio-Vascular Patients
415
would require deep expertise to know the relevant
context parameters and how these are correctly
defined, and furthermore be very time consuming
and error-prone to provide the parameter
specifications as manual input. In case of health
applications, context information is needed when
end-users are least likely to be able to provide the
input themselves. For these applications, it is even
more important that the applications gather the
context information independently of the end-user
providing manual input. Context-aware applications
can be particularly effective if the end-user is mobile
and uses a personal handheld device for the delivery
of services. The mobile case is characterized by
dynamic context situations often dominated by
changing location (however not necessarily
restricted to this). Different locations may imply
different social environments and different network
access options, which offer opportunities for the
provision of adaptive or value-added services based
on context sensitivity. Especially in the mobile case,
context changes are continuous, and a context-aware
application may exploit this by providing near real-
time context-based adaptation during a service
delivery session with its end-user. The adaptation is
‘near real-time’ because context information is an
approximation (not exact representation) of the real-
life context and thus there may be a time delay.
Through context-awareness, applications can be pro-
active with respect to service delivery, in addition to
being just re-active, by detecting certain context
situations that require or invite the delivery of useful
services which are then initiated by the application
instead of by a end-user request. Otherwise said,
traditional applications provide service in reaction to
user requests (re-active), whereas context-aware
applications have also the possibility of initiating a
service when a particular context situation is
detected, without end-user input (pro-active).
Although context-aware applications have received
much attention within the research community, they
have not been fully successful so far from a business
point of view. This situation may change rapidly
however, due to the observed growing power and
reduced prices of mobile devices, sensors, and
wireless networks, and due to the introduction of
new marketing strategies and service delivery
models (A-MUSE Project, 2008; Mei et al, 2007).
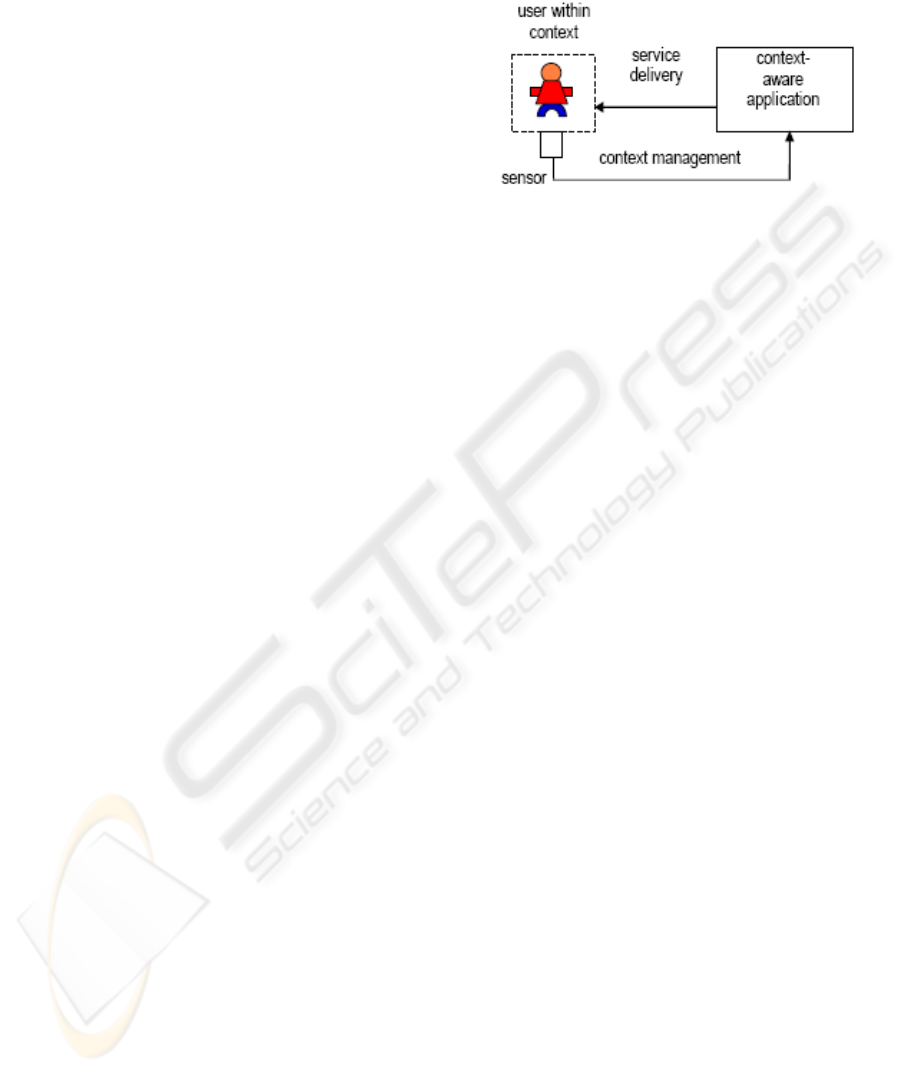
A context-aware application is (usually)
expected to have the ability of adapting its service
delivery depending on the information about the
user’s state (which information the application
certainly must have received); this is illustrated in
Figure 1.
As mentioned before, we are proposing a
solution to some health-monitoring-related
problems, which is rooted in context analysis. In
Figure 1: Schematic representation of a context-aware
application (Shishkov & Van Sinderen, 2008).
particular, we take context into account because
adequately adapting the delivered services to the
situation of the patient would result in more
effective support. We incorporate multi-level
context states and distinguish between different
perspectives on context states for the design of
flexible and adaptive ICT applications. The IT
system autonomously considers context not only for
the patient but also for the other related stakeholders.
We address hence these two innovative
proposals, namely concerning: (i) multi-level
context states and (ii) different perspectives on
context states, in the remaining part of this section.
2.1 Multi-level Context States
In previous research (Shishkov et al, 2008; Shishkov
& Van Sinderen, 2008; A-MUSE Project, 2008), we
have explored to some extent the possibilities to
enforce context driven application adaptability,
taking into account the situation of the end-user.
What has not been exhaustively addressed
nevertheless is how we take also into account the
situations of other related entities. This we focus in
the current paper. In particular, we suggest
innovative ways of modeling context situations at
different levels and we as well relate this to the
mentioned already achieved results.
These different levels are needed because it is
often not only the end-user whose situation is
relevant. Taking for example the situation in which a
patient is receiving support from a distance. We
would often face the problem of considering other
related entities as well – if the sensed vital signs of
the patient indicate possible problems, it might be
needed to provide careful analysis of a doctor,
preferable the patient’s own doctor, and if the
situation gets worse, to send an ambulance to the
patient. It has to be taken into account what the
ACT4SOC-EHST 2009 - 4th International Conference on Software and Data Technologies
416
context situation of the doctor and the ambulance is.
Maybe the ambulance of the local service point is in
a traffic jam and it would be necessary to find
another ambulance. It may be that the medical
doctors in the emergency department of the hospital
to which the patient is to be sent are busy with
another emergency case and it would be wise
sending the patient to another hospital in the area.
Concluding, it can be stated that better care could be
provided when a rich set of state information would
be available, and could be combined appropriately
for the particular case of the patient.
application
UCS
1
UCS
2
UCS
i
UCS
n
…
…
ECS
i1
ECS
i2
…
ECS
iu
…
…
...
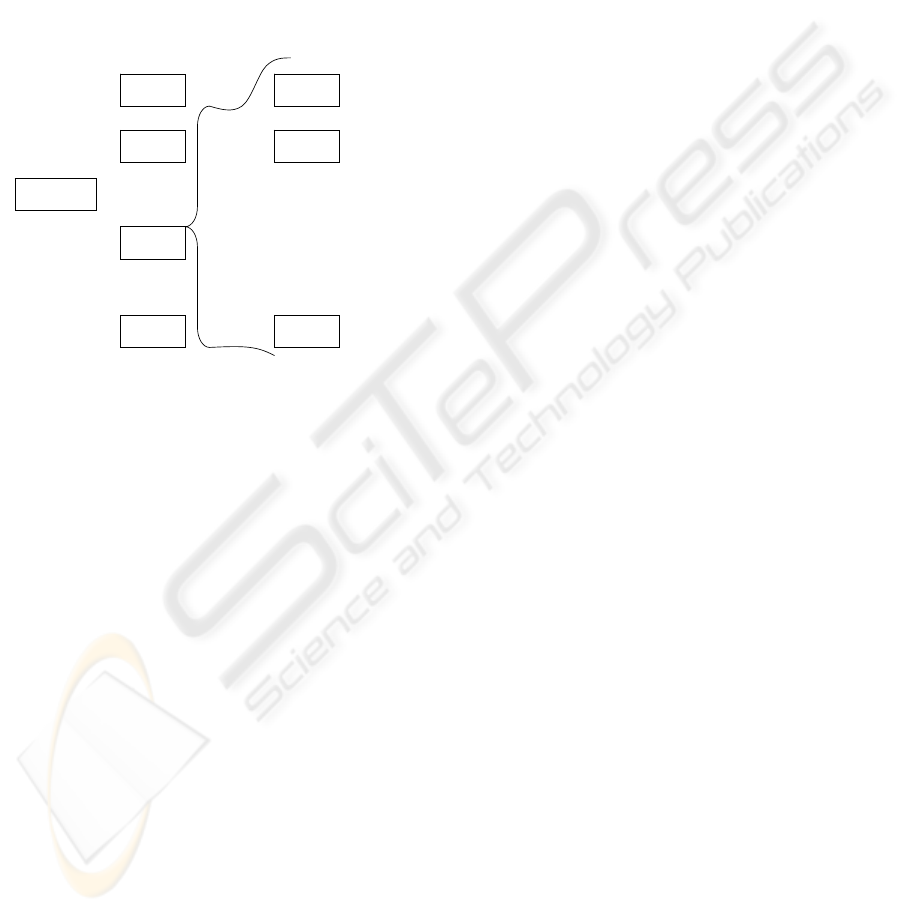
Figure 2: Considering many inter-dependent context
situations.
Hence, we have (as Figure 2 suggests) a number
of User Context States – UCS, based on which states
the application should adapt its behavior, and each
of these states points to a number of states of
relevant entities.
We might like to further our previous work that
puts all in a simpler setting where we abstract from
the context situations of all other entities (ECS)
which situations would be relevant to the desirable
application service delivery.
2.2 Different Perspectives on Context
States
Monitoring of patients remotely, especially for
disease management or supervision of elderly
persons with systemic diseases, is often a multi-
facetted process. The current perspective of the
World Health Organization (WHO) on health is in
fact extended from a bio-psycho health model,
typically expressed in terms of body functional and
structural impairments and disabilities, to a bio-
psycho socio model, additionally expressed with
terms of person’s participation in the society (WHO,
2001). This vision on health and the current trends
for patient self-management require orchestrated
multi-level loops of monitoring and treatment
controls because of the different dynamic properties
that concern the management of the systemic
diseases and the person’s participation.
A patient suffering from a chronic cardio-
vascular disease, for example, may need continuous
monitoring of his or her heart condition. The
dynamics of the monitoring or treatment of this
patient would often depend on the selected post
diagnostic treatment protocol (Von Wright, 1963).
In case of COPD as well, there would be an
additional disease management protocol needed, and
it would be of course necessary to appropriately
align this protocol with the (primary) cardio-
vascular disease management protocol.
The ICT facilities that should support the patient
are to be configured therefore in accordance with the
different disease management dynamics. This would
involve in turn several context state trajectories,
each of which reflecting the particular disease
management protocol. Consequently, the patient
supervision processes would also require several
context state trajectories, each one in conformity
with the dynamics of the specific disease
management protocol (Moran & Dourish, 2001;
Meinert, 1986).
Besides these multiple bio-medical context state
trajectories, another context state trajectory is
needed in order to reflect the supervision of the
participation of the patient. Such supervision may
provide a better feeling of safety and availability of
on demand assistance; these often lower the
thresholds of participation. State changes of the
patient’s external environment are typically slow;
this is in contrast to emergency care or some
warning events in chronic care. Accordingly, other
control or management techniques may apply for
monitoring of patients to improve participation.
Hence, treating the discussed context state
trajectories separately, while maintaining
coordination at the same time, is believed to be a
better design practice of separation of concerns.
In the following section - Case Example, we
present a scenario that illustrates a contextual setting
for patient monitoring to improve patient’s
participation.
3 CASE EXAMPLE
As mentioned already, we will present in this section
a case example through which we will illustrate our
ideas.
ENHANCING CONTEXT ANALYSIS WITH INTELLIGENCE IN PROVIDING e-HEALTH SERVICES - Less
Infrastructure Dependency in Supporting Cardio-Vascular Patients
417
Our scenario envisions Rob Martens who is 70
years of age; he lives in a service apartment complex
for elderly. Being diagnosed as a heart patient, he
participates in a cardio-vascular monitoring program
of the local hospital’s Cardiology Department. As
many others of his age with a heart problem, Rob
also suffers from COPD. Although Rob can live on
his own, he often gets out of breath and falls if not
being able to find out a nearby place to sit.
For the monitoring program, Rob wears a
garment with dry ECG electrodes, a 3D acceleration
activity sensor with GPS and as well a PDA which
collects, processes, multiplexes and transfers Rob’s
vital signs continuously and wirelessly to the
Cardio-Care portal of the Cardiology Department. A
specialized nurse continuously occupies this portal
and a junior cardiologist is always on duty at the
department.
Being reluctant (before participating in the
monitoring program) to go out of his apartment for
socialization and even preferring to stay in his
bedroom (because of his feeling insecure), Rob feels
more secure when he knows that they continuously
monitor him and he goes down often, visiting the
common room in the complex.
On Day X, Rob goes early to the common room,
but after a few hours he feels tired and he walks
back to his apartment. In the elevator, Rob feels
dizzy and falls down. He does not manage to sit on
the bench in the elevator, neither to reach the
elevator’s alarm button. Rob’s sensory system
detects the fall however; the system is aware that he
is in the elevator and thus this is known at the
Cardio-Care portal. The portal also detects an
increase of Rob’s heart rate, it beeps for the attention
of the nurse on duty, Marit, renders Rob’s data from
his electronic patient record and switches on the
audio-visual system (display, speakers, microphone
and remotely controllable camera) in the elevator
that is usually switched off for privacy and energy
saving reasons. Via the Hi-Fi audio link Marit calms
Rob down, which effect she observes from his heart
rate reading. The trained nurse concludes from the
vital sign readings and the camera display on her
monitor that Rob’s condition is not acute and
decides therefore not to ask for an ambulance and
not to reset the elevator to go to the ground floor,
Instead, Marit clicks on her screen for a window
presenting the nurses in the vicinity of Rob
including their prioritized activity from their
electronic work schedule and their ability to assist
Rob, taking into consideration that Rob is too heavy
for many of the nurses. Marit only detect Dewi at a
floor higher and who needs a lift device to help Rob.
Marit reset the lift to go a floor higher and beeps
Dewi, who finds immediately the location of the
nearest lift device since all devices have RFD tags,
and who thus can help Rob to go back to his
apartment. In the mean time, Marit sends a report
containing the vital sign readings, the video clip and
the symptoms to John, a Cardio-Care nurse
practitioner who is assigned to Rob.
In the following section, we will further
elaborate our ideas, reflecting them in the partial
application of this case scenario.
4 SUPPORTING
CARDIO-VASCULAR
PATIENTS INTELLIGENTLY
We will analyse the scenario presented in the
previous section, in a practical application, and
while doing this, we will elaborate our innovative
ideas, that have already been presented in Section 2.
Logically, the identification of the domain-
imposed requirements should be firstly done. The
entities and some of their activities, in a typical
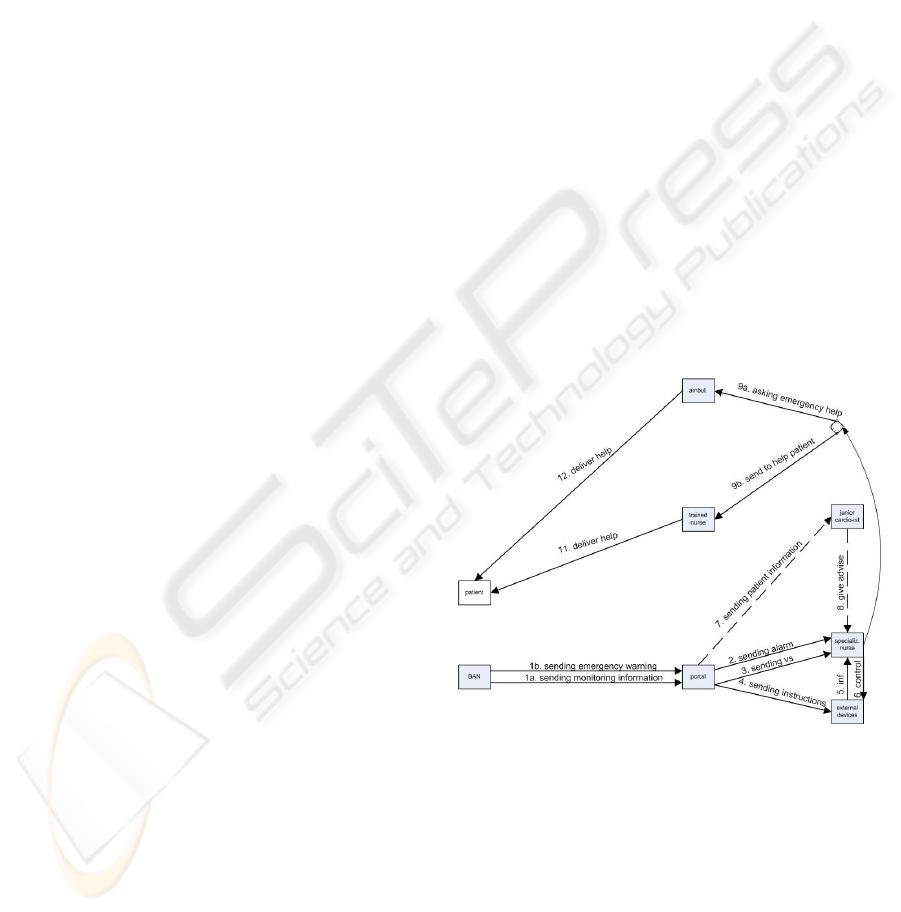
scenario, are represented in Figure 3.
Figure 3: Entities and activities in a typical scenario.
In the Figure, the BAN (Body Area Network) is
associated with the Patient but it is another entity
because it is not the patient who controls the BAN
sensors but they are performing their tasks on their
own, together with the BAN intelligent devices. The
BAN usually sends monitoring information to the
Portal (1a) and in cases of a (sensed) emergency it
can also send an emergency warning (1b). We will
consider only the emergency case further. Hence,
following the warning (1b), the Portal should send
ACT4SOC-EHST 2009 - 4th International Conference on Software and Data Technologies
418
an alarm to a specialized nurse (2) and it should
transmit the sensor readings (3). At the same time,
instructions could be given to external devices, such
as cameras in elevators, for instance. This triggers
the devices to send some actual information to the
specialized nurse (5) who can manage in turn to
control these devices for even better results (6).
Sometimes, when the case appears to be of great
complexity, the specialized nurse may ask a junior
cardiologist to get involved in the decision making
(8), supported by information concerning the patient,
which can be received from the Portal (7). Based on
all the information and the potential input of the
junior cardiologist, the specialized nurse should
decide whether the situation is urgent or not. If not,
then a trained nurse is to be asked to deliver help
(9b). In case of emergency nevertheless, the
specialized nurse must ask help from an ambulance
(9a). No matter what the choice, the patient is to
receive help – either from the trained nurse (11) or
from the emergency team (12).
This information can be reflected usefully in
other models, as according to the SDBC approach
(Shishkov, 2005).
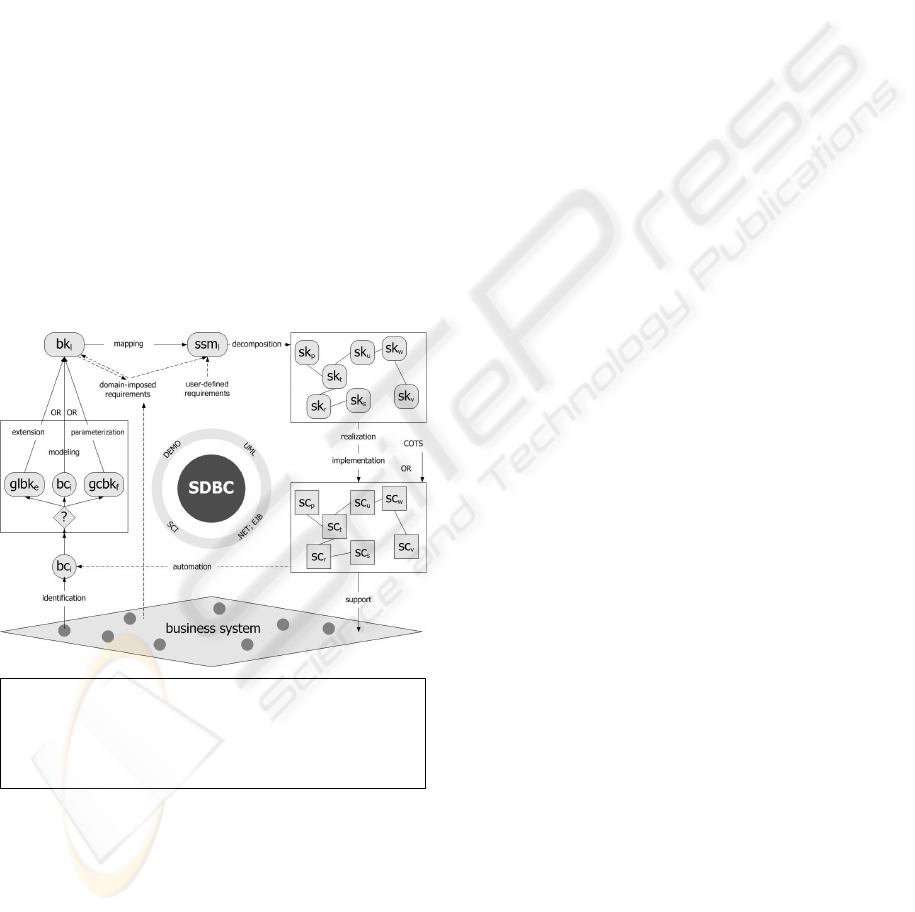
Abbreviations:
bc – Business Component ssm – Software specific. model
bk – Business CoMponent sc – Software Component
glbk – General Bus. CoMponent sk – Software CoMponent
gcbk – Generic Bus. CoMponent
Figure 4: SDBC Approach (Shishkov, 2005).
As presented in Fig. 4, we consider a Business
System (with a static perspective and a dynamic
perspective, which both can be projected on the
model we have presented in Figure 3; we omit a
discussion on these modeling transformations for
reasons of brevity) from which Business
Components are to be identified (these are just parts
of the Business System). The component should be
then reflected in a relevant model – a Business
CoMponent (these are business models (Van Hee &
Reijers, 2000) that are to be used as foundation in
deriving the specification of an automated system).
Another way for arriving at a Business CoMponent
is through re-use, which we also omit for brevity.
The Business CoMponents should then be
elaborated with more domain-imposed requirements,
in order to add elicitation on the particular context in
which its corresponding Business Component exist
within the Business System, and these are
elaborations added to the relationships expressed in
Figure 3. Then, a mapping towards a software
specification model should take place (Rational:
OMG, 2007), through a modeling transformation,
taking into account that all that is not to be
automated appears as the environment of the ICT
system (Liu, 2000) and all that affects its
functionality – as context.
We are therefore able to define generic ICT
components that are adjustable based on the
particular situation in the business world. These
could be used in the specification of context-aware
applications that effectively support patients. The
component-based approach has a crucial advantage
with respect to the service-orientation since
technical components and corresponding business
services are to be considered in concert, setting up
an orchestration of the services with the users (not
burdened with technology) and adequately tracing to
the technology, keeping track also which part of the
delivered functionality is the responsibility of an
application component and which part is the
responsibility of the underlying infrastructure.
On the basis of this study, we claim that
components are a good foundation for service-
orientation and that service-orientation in turn is a
good foundation for context awareness (because
context awareness means different functionality
versions, which naturally projects to different related
services). All this in combination can be of
particular value, nevertheless if only the real-life
information is adequately captured and processed, as
we have suggested in this section.
5 CONCLUSIONS
In this paper, we have reported follow-up research
from previous studies on context-aware application
support to patients, mainly envisioning tele-
monitoring. We have added contribution on how to
better describe, present and capture the real-life
ENHANCING CONTEXT ANALYSIS WITH INTELLIGENCE IN PROVIDING e-HEALTH SERVICES - Less
Infrastructure Dependency in Supporting Cardio-Vascular Patients
419

information and reflect it in software components in
a consistent way.
We have omitted for brevity discussions on
modeling transformations that have been considered
exhaustively in literature, especially in materials
focusing on model-driven engineering. What is
missing in most of these materials nevertheless is
sound guidelines on the identification of
computation-independent models and in the paper
we have delivered some useful contribution relevant
to this. Furthermore, we have put some concreticity
with regard to more general results from previous
studies, considering especially the health care
perspective where context-awareness is of crucial
importance. Finally, we have also illustrated
partially the early stages of deriving a computation-
independent model, by emphasizing on the need for
structuring information as good as possible.
In the analysis preceding the proposed
methodological guidelines, we have suggested how
multi-level context states can be incorporated and
how context states can be considered from different
perspectives, for the design of flexible and adaptive
ICT applications.
The achieved results can be generalized to also
derive more fundamental knowledge on the possible
ways in which context-aware solutions can be
applied.
We plan for further research reflecting the
mechanisms of the SDBC approach for structuring
early requirements in a separate methodology,
applied in different domains including the health-
care domain.
REFERENCES
A-MUSE Project, 2008: http://a-muse.freeband.nl.
Liu, K., 2000. Semiotics in Information Systems
Engineering, Cambridge University Press. Cambridge.
Mei, H., Widya, I.A., Broens, T.H.F., Pawar, P., Van
Halteren, A.T., Shishkov, B., Van Sinderen, M.J.,
2007. A Framework for Smart Distribution of Bio-
signal Processing Units in m-Health. In ICSOFT’07,
2nd International Conference on Software and Data
Technologies. INSTICC Press.
Meinert, C.L., 1986. Clinical Trial: Design, Conduct and
Analysis, Oxford University Press, New York.
Moran, T.P. and Dourish, P, 2001. Introduction to
Context-Aware Computing, Special Issue of Human-
Computer Interaction, Volume 16, IBM Almaden
Research Center, University of California, Irvine.
Rational / OMG UML, 2007. Unified Modeling Language,
Object Management Group, http://www.omg.org/uml.
Shishkov, B., 2005. Software Specification Based on Re-
usable Business Components, Delft University Press,
Delft (PhD Thesis).
Shishkov, B., Van Sinderen, M.J., Liu, K., Du, H., 2008.
Norm Analysis Supporting the Design of Context-
Aware Applications. In ICEIS’08, 10th International
Conference on Enterprise Information Systems.
INSTICC Press.
Shishkov, B. and Van Sinderen, M.J., 2008. On the Design
of Context-Aware Applications. In I-WEST’08, 2nd
International Workshop on Enterprise Systems and
Technology. INSTICC Press.
Van Hee, K. and Reijers, H.A., 2000. Using Formal
Analysis Techniques in Business Process Re-Design.
W. van der Aalst et al. (Eds.): Business Process
Management, LNCS 1806.
Von Wright, G. H., 1963. Norms and Action - a Logical
Enquiry. Routledge and Kegan Paul, New York.
World Health Organization - WHO. 2001. International
Classification of Functioning, Disability and Health:
ICF. Geneva, Switzerland.
ACT4SOC-EHST 2009 - 4th International Conference on Software and Data Technologies
420
