
ENDOBRONCHIAL TUMOR MASS INDICATION IN
VIDEOBRONCHOSCOPY
Block based Analysis
Artur Przelaskowski, Rafal Jozwiak
Institute of Radioelectronics, Warsaw University of Technology, Nowowiejska 15/19, 00-665, Warsaw, Poland
Tomasz Zielinski
Department of Telecommunications, AGH University of Science and Technology, Al. Mickiewicza 30, 30-059, Krakow, Poland
Mariusz Duplaga
Collegium Medicum, Jagiellonian University in Krakow, Sw. Anny 12, 31-008, Krakow, Poland
Keywords:
Bronchoscopy, Pattern recognition, Feature selection, Multiscale image processing.
Abstract:
Computer-assisted interpretation of bronchial neoplastic lesion is an innovative but exceptionally challeng-
ing task due to highly diversified pathology appearance, video quality limitations and the role of subjective
assessment of the endobronchial images. This work is focused on various manifestations of endobronchial
tumors in acquired image sequences, bronchoscope navigation, artifacts, lightening and reflections, changing
color dominants and unstable focus conditions. Proposed method of neoplasmatic areas indication was based
on three steps of video analysis: a) informative frame selection, b) block-based unsupervised determining
of enlarged textual activity, c) recognition of potentially tumor tissue, based on feature selection in different
domains of transformed image and Support Vector Machine (SVM) classification. Prior to all of these pro-
cedures, wavelet-based image processing was applied to extract texture image for further analysis. Proposed
method was verified with a reference image dataset containing diversified endobronchial tumor patterns. Ob-
tained results reveal high accuracy for independent classification of individual (single video record) forms of
endobronchial tumor patterns. The overall accuracy for whole dataset of 888 test blocks reached 100%. Less
complex (approximately two times) procedure including initial blocks of interests selection reached accuracy
of 96%.
1 INTRODUCTION
Recent advances in video technology enable for
highly effective and safe diagnostic and therapeutic
procedures of limited invasiveness, which is one of
a key postulates in modern medicine. The quest for
more sophisticated techniques in endoscopy is closely
related to this trend (Duplaga, 2007). Even though,
endoscopic examination remains stressful procedure
for a patient and its outcome depends strongly on
physician’s skills and his subjective assessment of en-
doscopic images. Video recordings of endoscopic
procedures stored in digital libraries are the source of
diversified and often ambiguous information in terms
of computer-assisted analysis. For example, video
recordings of endoscopic examinations (e.g. gas-
troscopy, colonoscopy, bronchoscopy, etc.) contain
not only images of normal and pathological endolu-
minal structures or diagnostic and therapeutic proce-
dures, but also many poor quality or completely non–
informative frames (e.g. blurred, out-of-focus, dis-
torted, etc.).
1.1 Bronchoscopy
Bronchofiberoscopy is one of key diagnostic proce-
dures employed in respiratory medicine and enabling
direct visualization of the endoluminal structure of
tracheobronchial tree. There are many indications
when bronchofiberoscopy is performed, but in the
536
Przelaskowski A., Jozwiak R., Zielinski T. and Duplaga M. (2010).
ENDOBRONCHIAL TUMOR MASS INDICATION IN VIDEOBRONCHOSCOPY - Block based Analysis.
In Proceedings of the International Conference on Computer Vision Theory and Applications, pages 536-542
DOI: 10.5220/0002924405360542
Copyright
c
SciTePress

case of lung cancer suspicion it is obligatory. The
procedure is usually accompanied by other diagnos-
tic modalities enabling tissue sampling for pathologic
evaluation. The progress in video technology had also
its impact on bronchoscopy both in terms of available
equipment and the scope of possible diagnostic and
therapeutic techniques. Modern video bronchofibero-
scopes contain an integral video camera system at the
distal end and illumination system based on optical
fibers assuring appropriate visibility of endobronchial
structures. Endobronchial image is captured by the
camera and displayed on the screen which can be con-
veniently placed in the bronchoscopy lab. The ex-
perience of performing physician considerably influ-
ences the effectiveness of the procedure and usually
progress in the skill depends on the intensity of super-
vised training. The assessment of bronchoscopic im-
ages is poorly standardized and currently relies solely
on procedure logbooks and subjective letters of com-
petency (Bowling, 2007).
Video recording of bronchoscopic examinations
demonstrate many common features with natural
video sequences, e.g. general image features and nat-
ural content perception, color space, textural features,
data dynamics, dominant objects properties. Different
parts of bronchoscopic examinations differ in move-
ment characteristics - from slow motion to dynamic
video with fast camera movement across variable di-
agnostic content. Detection of pathological changes
in bronchoscopy frame which comes after a sequence
of normal images may be diagnostically challenging
task.
Video recordings of bronchoscopy procedures are
characterized by a considerable number of illegi-
ble sequences. Furthermore, great part of recorded
frames brings images of normal tracheobronchial tree
which must be also inspected during examination.
While the content of the frames cannot be recognized
and interpreted by any means because of limited ac-
quisition conditioning or case-dependent specific im-
age appearance, it is impossible to extract from it
any diagnostic information. Such frames with unrec-
ognized content were described as non-informative
frames (Hwang, 2007). The appearance of these
frames is highly diversified due to many factors in-
fluencing the quality of the endobronchial image. Es-
sentially, we can distinguish: out-of-focusframes (oc-
curred due to wrong camera position - too far/too
close focus into/from mucosa of bronchi), blurred
(motion blur due to rapid endoluminal camera move-
ment), with sanguination (due to pathology presence
or as a result of sampling of suspected tissues for
pathology evaluation) and bubbled (as a result of cam-
era lens cleaning). Informative frames carry poten-
tially important amount of diagnostic information.
However informative frames are not equal in the
sense of visual quality, which change rapidly depend-
ing on current camera situation, position and move-
ment. For example, any camera movement introduces
versatile amount of motion blur (rapid or very fast
camera movement can even lead to total loss of frame
readability), while coverage of the camera lens with
fluids or secretions results in loss of global focus con-
dition. Despite of the diversified visual quality, most
of informative frames collected in medical video li-
brary represent statistically normal images of differ-
ent anatomical parts of tracheobronchial tree. The
most significant video sequences in terms of patho-
logical findings make relatively small part of reg-
istered frames. The appearance of various patho-
logic manifestations remains strongly highly diversi-
fied both inter-class (between different types of le-
sions) as well as intra-class (between different man-
ifestations of the same type of pathology). Addition-
ally every informative frame can be potentially af-
fected by additional artifacts or distortions (e.g. spec-
ular reflections, lightening, etc.) which additionally
hamper process of analysis. Examples of the con-
tents of bronchoscopy video recordings, including
non-informative and informative frames, different le-
sions manifestations and their diversification as well
as possible distortions are presented in Fig. 1.
1.2 Pathology Recognition in
Bronchoscopy Video
Computer-based tools developed for bronchoscopy
support were designed with the objective of ad-
vanced visualization aspects like virtual bron-
choscopy (Chung, 2006; Duplaga, 2005) or video
(camera motion) tracking (Rai, 2006; Mori, 2002).
Our work is focused on computer assisted automatic
detection of lesions in bronchoscopy video. To the
best of our knowledge, similar researches have been
reported so far only for endoscopic modalities within
gastrointestinal tract e.g. colonoscopy (Iakovidis,
2006), but not for bronchoscopy.
Among different pathologic endobronchial man-
ifestations, detection of the features of the neoplas-
tic process remains top interest. Endobronchial tumor
mass constitutes relatively common manifestation of
tumors affecting proximal parts of tracheobronchial
tree - Fig. 2. Endobronchial tumor represents it-
self usually as a mass of different consistency in most
cases with dense vasculature and having pink to pur-
plish color.
The purpose of our work was to develop an ef-
ficient method for computer assisted interpretation
ENDOBRONCHIAL TUMOR MASS INDICATION IN VIDEOBRONCHOSCOPY - Block based Analysis
537
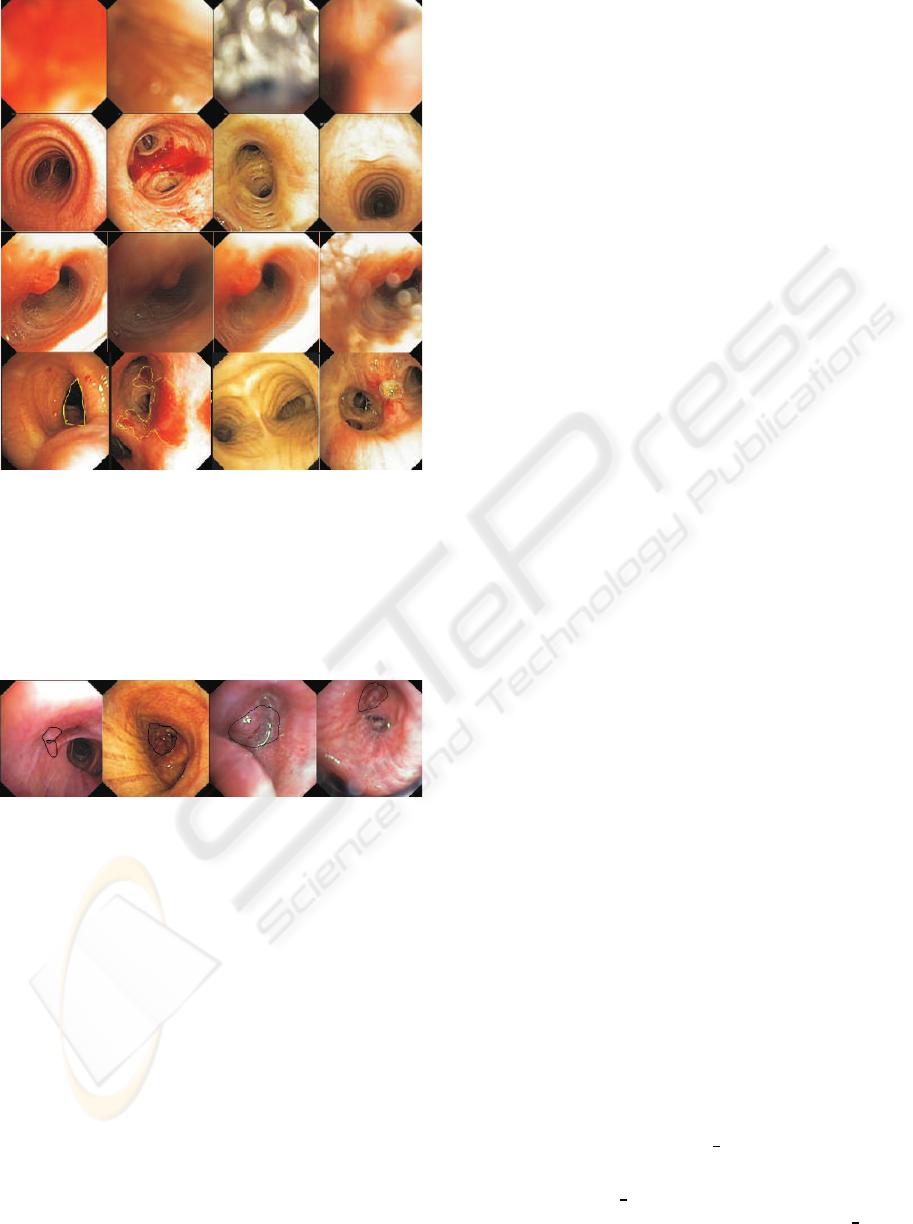
Figure 1: The examples of the content of bronchoscopy
video. The first row shows examples of non-informative
frames. The second row illustrates informative frames,
readable with good visual quality. Example of onerous vi-
sual quality diversification is presented in the third row (ad-
jacent frames from the same part of video examination). Fi-
nally, various bronchial lesions are presented in the fourth
row (from left: tracheal stenosis, extravasations, widened
main carina and mucous ulceration).
Figure 2: Examples of different endobronchial tumors.
Pathology were outlined manually by experienced pul-
monary medicine specialist.
of neoplastic lesions in bronchoscopy images. Sug-
gested method exploits different image preprocess-
ing techniques and is concentrated on texture-based
image analysis. We proposed normalization of ana-
lyzed images, texture feature extraction in different
domains (image, frequency, wavelet and contourlet),
feature selection and unsupervised as well as super-
vised (SVM) classification, carried out at different
stages of video content analysis. Implemented algo-
rithms were optimized and verified experimentally.
2 MATERIAL AND METHODS
General task of diagnostically significant pattern
recognition in bronchoscopic images is tough, chal-
lenging and technical conditions dependent because
of mentioned above, seriously limited quality of im-
age information. To succeed, recognition of en-
dobronchial tumor mass was based on an analysis
of bronchoscopy video frames according to precise
successive selection of specified regions of interests
(ROIs): informative frames, blocks of important con-
tent and blocks of potentially mass appearance.
Because dominant image feature used for recog-
nition was texture, ROIs selection was based gen-
erally on textural data characteristics complimented
with the factors of energy distribution in different data
domains, entropy-based characteristics of stochastic
information and other statistical measures of domi-
nant signal trends.
2.1 Block-based Method Description
Proposed method of neoplasmatic areas indication is
based on three steps of video analysis:
• IFS procedure, i.e. Informative Frame Selection,
based on a whole frame characteristics of possi-
ble artifacts, unusual data and dominant texture
recognition (SVM classifier);
• BUD method, i.e. Block-based Unsupervised De-
termination of enlarged textual activity areas in
the IFS frames, based on energy distribution anal-
ysis and directional image characteristics in polar
2D Fourier space;
• BRT method, i.e. Block-based Recognition of Tu-
mor tissue, based on feature extraction and 48 fea-
ture selection in image, frequency, wavelet, and
contourlet domains, followed by the SVM classi-
fication.
Prior all of these successive procedures, wavelet-
based image preprocessing was applied to extract tex-
ture image for further analysis.
2.1.1 Texture Extraction Preprocessing
A sequence of the following procedures was used:
• bronchoscopic frame normalization by successive
conversions: a crop of source image area with
mirror fulfilling of irregular corners, and conver-
sion to grayscale image (G I) - see Fig. 3;
• contrast-limited adaptive histogram equalization
(CLAHE) of G I with 4×4 pixel blocks and con-
trast function adjusted to 0.02: CL
4×4,0.02
(G I) =
I
AC
;
VISAPP 2010 - International Conference on Computer Vision Theory and Applications
538
• distorted wavelet synthesis of smoothed source
image I
S
= W
−1
(W (I
AC
)) and differential, tex-
ture image estimation as: I
T
= |I
AC
−I
S
|, where
W is 2-scale dyadic wavelet transformation based
on non-perfect reconstruction filter bank;
• adaptive histogram equalization of texture image
as follows: I
AT
= CL
4×4,0.02
(I
T
).
Exemplary results of texture extraction procedure
were presented in Fig. 3.
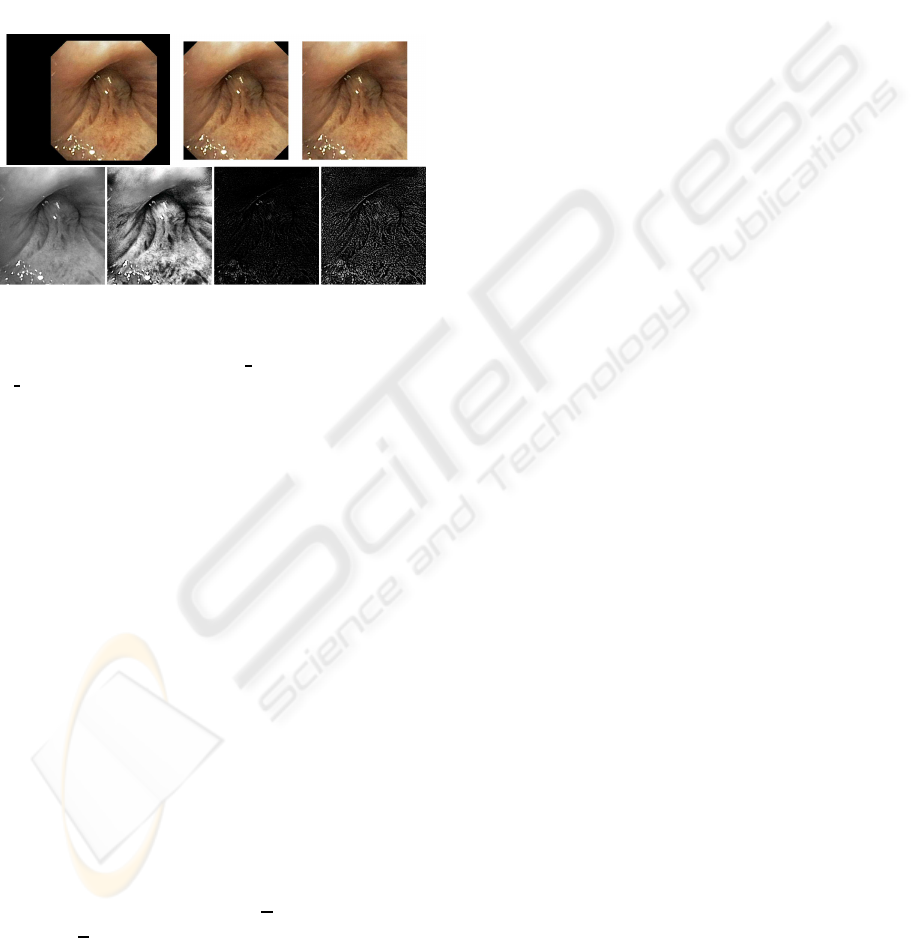
Figure 3: The effects of successive image preprocess-
ing procedures: (left-right, top-down) source broncho
frame, cropped image window, image with fulfilled corners,
greyscale normalized version (G I), adaptively enhanced
G I, textures extracted by wavelet-based procedure, texture
enhanced by CLAHE.
Histogram equalization is used for imaging
conditioning-invarianceand texture extraction even in
weak signal areas. CLAHE enhances local contrast of
images by transforming the values into the intensity
image. It operates on small data blocks so that the his-
togram of the output region approximately matches
the uniform histogram. The neighboring blocks are
bilineary interpolated to eliminate induced disconti-
nuities on the block boundaries. The contrast, espe-
cially in homogeneous areas, is limited by contrast
enhancement limit parameter to avoid amplifying the
actual image noise or insignificant textures.
Multiresolution Signal Analysis according to
wavelet-based concept is typically implemented
with specific types of digital filter banks (FBs)
known as two- channel perfect reconstruction (PR)
filter banks. Those filters are associated with scal-
ing functions (low pass one h) and the wavelets
(high pass one g) of the transform kernel accord-
ing to the following two equations (scaling and
wavelet, respectively): φ(t) =
√
2
∑
n
h
n
φ(2t −n) and
ψ(t) =
√
2
∑
n
g
n
φ(2t −n). Conditions of the perfect
reconstructions (Y is almost, i.e. according to the
assumed precision, equal to X) with l delays for
two-channel FB are as follows:
h(z)
˜
h(−z) + g(z) ˜g(−z) = 0 (1a)
h(z)
˜
h(z) + g(z) ˜g(z) = 2z
−l
(1b)
Generally, wavelet decomposition requires the fil-
ters to be FIR (finite impulse response) and linearly
phased to form orthogonal FBs. However, only Haar
filter fulfill such requirements. Often used solution
is biorthogonal FBs with insignificant redundancy of
wavelet representation. For texture-oriented image
processing we decided to design orthogonal FB by
softening PR condition. The first term (eq. 1a) tra-
ditionally called the alias (cancellation) term is of-
ten fulfilled by using quadrature mirror filters (QMFs)
with conditions: h(z) = ˜g(−z) and g(z) = −
˜
h(−z), as
we did. However, the second term (eq. 1b) called
the distortion elimination term was used to control
the distortion introduced in data processing to ex-
tract basic (lower frequency) signal content. Result-
ing filter proposition was spline non–PR FB with
h = [1/4,1/2,1/4] and miror g = [−1/4,1/2,−1/4]
for signal smoothing by wavelet preprocessing (Prze-
laskowski, 2007).
2.1.2 Texture Characteristics and Recognition
We considered energy distribution characteristics
across scales and subbands of wavelet domain diver-
sified significantly classified tissue. Different classes
of wavelet energy based features and histogram-based
features from normalized wavelet coefficients were
used. Moreover, entropy features (based on memory-
less and joint source) for subbands compositions and
homogeneity, correlation, energy and contrast of suc-
cessive scale co-occurrence matrix of quantized coef-
ficients were applied. SVM with optimized kernels
and quality criteria was applied for classification and
feature reduction procedures.
More precisely, the following textural features
were estimated:
• in image domain:
– statistical (variance, kurtosis, skewness, 0-
order entropy, energy)
– based on co-occurrence matrix (joint entropy,
contrast, correlation, energy, homogeneity)
– Tamura textural features (coarseness, direction-
ality, contrast) (Tamura, 1978)
• in wavelet domain (symlet2 from nearly symmet-
rical wavelets, 2 scales of decomposition):
– energy of approximation related to the energy
of details
– distribution of detail energy and entropy across
scales
ENDOBRONCHIAL TUMOR MASS INDICATION IN VIDEOBRONCHOSCOPY - Block based Analysis
539

– joint entropy of distribution if max magnitude
details for successive scales
– joint entropy, contrast, correlation, energy, ho-
mogeneity for co-occurrence matrix of quan-
tized max magnitude details
– max detail value of different subbands related
to mean approximation energy
• in polar 2D Fourier domain:
– statistical moments of angle histogram of coef-
ficient magnitudes
– energy of angle histogram
– parameters of polynomial approximation of an-
gle histogram
• in contourlet domain – entropy of directional
spectrum of two scales
Selected textural feature spaces were used for IFS
and BRT procedures.
Informative frame selection (IFS) was based on a
whole image I
AT
characteristics for possible artifacts,
regions of unusual data (non–informative) and infor-
mative regions with dominant texture recognition. 48
textural feature space was initially used for frame
classification. Informative frames were extracted ac-
cording to supervised classifier of over 800 training
frames. SVM classifier with regularization and radial
kernel was optimized for universal broncho applica-
tions.
Block-based unsupervised determination (BUD) of
enlarged textual activity areas was used for fast defin-
ing of block of interests. Idea of second step of tumor
extraction was high risk area segmentation through
block-oriented cover of the image. Blocks of 50×50
pixels were verified basing on energy distribution
analysis and directional image characteristics in po-
lar 2D Fourier space. Two phase threshold selection:
for energy distribution factors and directional factors
was optimized for over 1000 test cases.
Block-based recognition of tumor tissue (BRT) was
designed for final recognition of selected, active im-
age blocks as potentially covered by tumor mass tis-
sue. Recognition scheme was optimized for large test
set of several thousand of test BUD blocks basing on
textual feature extraction and selection for effective
case classification. SVM procedure with regulariza-
tion and radial kernel was used to classify each BUD
block as diagnostically suspected of having pathology
symptoms or normal.
Graphical form of selection and recognition re-
sults was used for indication of frame status as non–
informative (purple mark in top left corner) or infor-
mative (lack of purple mark), while informativeframe
regions could be covered by red (i.e. BUD) or yellow
(i.e. BRT) blocks.
The proposed block-based method assisting intra-
bronchial tumor mass recognition was implemented
in MATLAB environment. For classification purpose
we used standard SVM classifier from Matlab Bioin-
formatics Toolbox. Additionally we used some ex-
tra procedures form Contourlet Toolbox (Do, 2005),
Beamlab (Donoho, 2001) and Wavelab (Buckheit,
1995).
2.2 Test Bronchoscopic Material
The proposed method was verified with a reference
image data set containing different bronchoscopy
video content exemplification (e.g. varied patholo-
gies, diversified anatomical bronchi structures, ther-
apeutic and diagnostic interventions, possible arti-
facts, etc.) clinically selected by experienced pul-
monary medicine specialist from near 600 recorded
and stored videos of bronchoscopy examinations. A
reference set of close to 1300 images containing
informative/non-informativeframes was used to asses
IFS efficiency.
For the purpose of BUD and BRT assessment 14
diversified cases of intrabronchial tumor manifesta-
tions were considered, each containing several espe-
cially selected frames with additional manual pathol-
ogy outline. Every frame was divided into blocks
of size 50x50, where each block was categorized to
norm or pathology according to available physician
outline. Near 900 selected blocks were finally used
as a test set. Among these blocks, a small set of 38
blocks of one distinct case of intrabronchial tumor
was selected. 16 of these blocks contained representa-
tive patterns of clear, high quality manifestation of the
tumor completed with 22 blocks of surrounding, nor-
mal tissues. Such test sets were used for BUD/BRT
verification and optimization.
3 EXPERIMENTS AND RESULTS
Examples of results achieved for the Matlab imple-
mentation of the described algorithm were presented
and explained in Fig. 4. Illustration of the method ad-
justing to concreteexamination and user requirements
were outlined in Fig. 5.
IFS step tested against 1228 test frames gave even
100% accuracy of informative/non-informative selec-
tion with optimally adjusted radial kernel of SVM for
complete space of extracted features. Optimization
procedure indicated that IFS efficiency moderately
VISAPP 2010 - International Conference on Computer Vision Theory and Applications
540
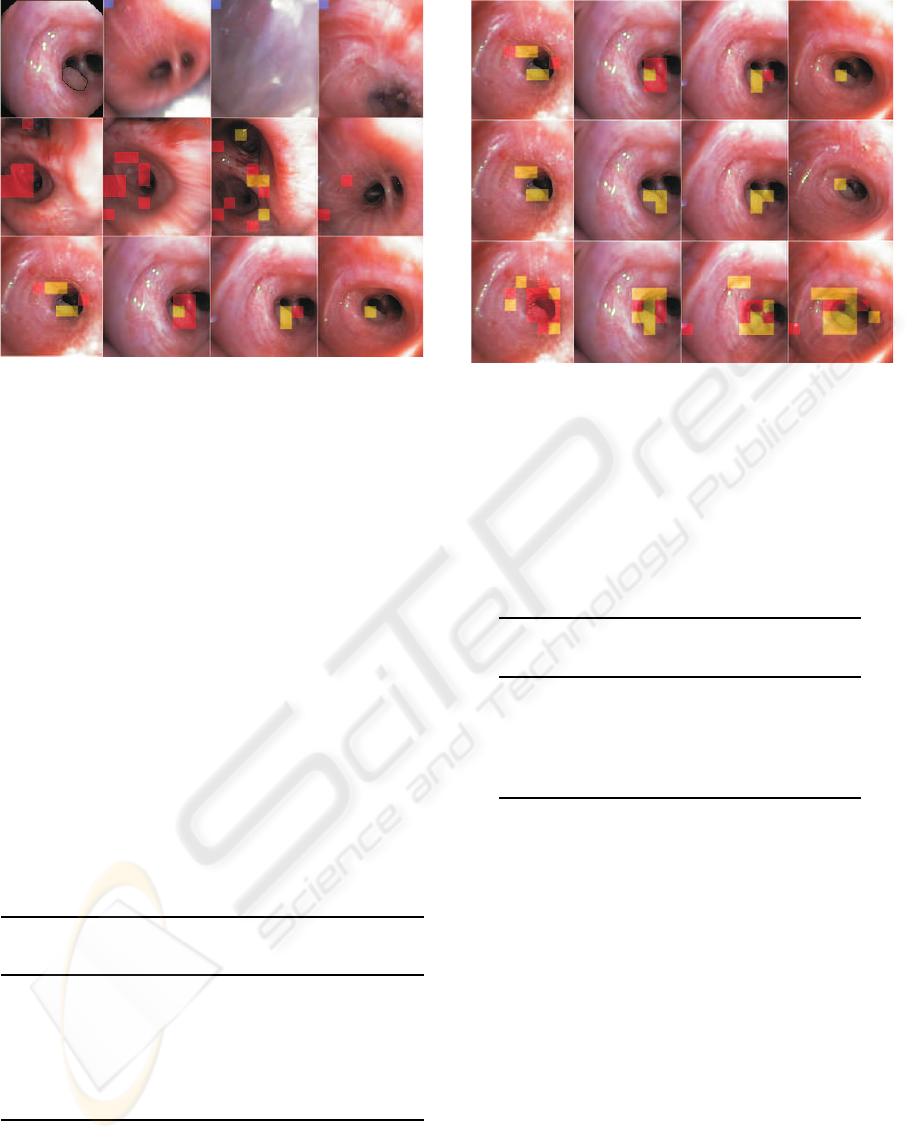
Figure 4: Exemplary results of the proposed block-based
method applied to selected video examination with en-
dobronchial tumor mass (reference frame with outlined
pathology is presented in top left corner). Other frames of
first row, marked with purple block, were classified as non-
informative (first stage of algorithm). Red blocks represent
areas with high texture information activity (related directly
to second stage of proposed method) while yellow blocks
marked out presence of pathology area (related directly to
third stage of proposed method). Second row illustrates in-
formative frames without clearly visible pathology (frames
preceding appearance of pathology). Yellow blocks notice-
able on third frame in this row (from left) represent false
positive (FP) indications. Frames with visible pathology
are present in third row. As we can see, pathology exis-
tence are indicated more or less precisely, but mainly cor-
rectly (yellow block are present in places corresponding to
area outlined originally on reference frame). Some miss-
classification examples can be seen on first frame (form left)
- two yellow blocks located above pathology area.
Table 1: IFS effectiveness for selected sets of textural fea-
tures and adjusted classifier; six the most useful features
are: entropy of contourlet coefficients, ratio of approxima-
tion to detail wavelet coefficients, Tamura coarseness, en-
tropy of wavelet details in successive scales, entropy and
variance of extracted textures in image domain.
Number of
the features Classifier Sensitivity Accuracy
48 SVM/rbf 1 1
48 SVM/linear .9 .92
24 SVM/rbf 1 1
24 SVM/linear .89 .92
6 SVM/rbf .91 .94
6 SVM/linear 0.87 0.87
depends on classification procedure and even signifi-
cant reduction of the number of textural features. Ex-
emplar results were presented in Tab. 1.
Sensitivity of BUD method was optimized in re-
lation to high enough specificity through adjusting of
Figure 5: Impact of method parametrization for overall de-
tection efficiency. Each row illustrates results for different
set of method parameters. Depending on the selected set of
initial presets proposed method is more or less sensitive. Se-
lection of this parameters should set a compromise between
method sensitivity and specificity.
Table 2: Adjusting of BUD parameters to select the best
balance between sensitivity and specificity of the method.
Threshold values of 4.35/1 (4.35 for normalized energy dis-
tribution and 1 for directional image characteristics) were
used finally.
Two threshold
values of BUD Sensitivity Specificity
4.35/4 .65 .58
4/4 .70 .36
4.35/3 .81 .44
4.35/1 .89 .38
4/2 .95 .1
two selective thresholds. Diversified in local energy
test set of 888 image blocks was used to make the
procedure more universal, sufficiently efficient as on-
line detector of suspicious to tumor areas and selec-
tive enough for more precise supervising of BRT pro-
cedure.
Satisfying sensitivity of 94% with specificity up
to 86% was achieved for more distinct test set of 38
selected blocks. The balance range between sensitiv-
ity and specificity for total test set of 888 blocks was
presented in Tab. 2. Maximum accuracy was limited
to 61%.
Accuracy of BRT method was adjusted to 98% for
888 test control or pathology blocks. Selected 30 tex-
tural feature space was used. Six the most useful fea-
tures are: entropy of contourlet coefficients, mean of
angle histogram and the parameter of polynomial ap-
proximation of angle histogram in polar 2D Fourier
domain, mean local entropy in image-texture domain
ENDOBRONCHIAL TUMOR MASS INDICATION IN VIDEOBRONCHOSCOPY - Block based Analysis
541

combined with texture energy, global entropy and en-
ergy in image-texture domain. However, accuracy for
these 6 features was only 75%. Accuracy of BRT for
more flexible and universal linear kernel of SVM was
only 76%.
Obtained results reveal high accuracy for indepen-
dent classification of individual differential forms of
endobronchial tumor patterns, especially basing on
time consuming IFS-BRT procedure. The overall ac-
curacy for whole dataset of 888 test blocks reached
100%. Thus, time consuming IFS-BRT combination
that assumed feature extraction and SVM classifica-
tion for each frame and next successively for all frame
blocks is effective enough to fit classification rules
to tumor detection problem. Less complex (approx-
imately five times) procedure of complete IFS-BUD-
BRT reached accuracy of 96%.
All verified procedures were designed to analyze
bronchoscopic video in order to indicate the blocks of
high susceptibility to tumor mass. A way of frame
and frame block selection to be analyzed depends
on application requirements. Because of computa-
tional complexity of BRT, which is fundamental pro-
cedure for tumor recognition, ad-hoc section method
of blocks of interests, similar to BUD or other inter-
active methods based on human-computer interfaces,
are useful for close to on-line application.
4 CONCLUSIONS
Clinical usefulness of the proposed method should
be further tested in conditions of bronchoscopy suit.
Reliable experimental procedure strongly depends on
significantly diversified technical conditions of bron-
chofiberoscopes and test cases. Moreover, the fea-
sibility of this method may be affected by the lim-
ited standardization of the procedure and significant
role of subjective assessment. However, automatic
indications in almost on-line mode (second stage of
the method) or more reliable in off-line mode (full
method application) seems to be useful as an assistant
tool for more careful bronchoscopic video analysis.
Objectified indicators of special regions of interests
are useful for standardized protocol design, compara-
tive analysis and education of inexperienced doctors.
As far as the authors are aware, it is the first attempt of
development of the tool based on the automatic prob-
able pathology indication supporting bronchoscopic
examination.
REFERENCES
Duplaga, M., Leszczuk, M., Przelaskowski, A., Janowski,
L. and Zieliski, T. (2007). Bronchovid - zin-
tegrowany system wspomagajcy diagnostyk bron-
choskopow. Przegld Lekarski 64:42-48.
Bowling, M., Downie, G., Wahidi, M. and Conforti, J.
(2007). Self-Assessment Of Bronchoscopic Skills In
First Year Pulmonary Fellows. Chest Vol. 132, Issue
4.
Hwang, S., Oh, J., Lee, J., Tavanapong, W., de Groen, P. C.
and Wong, J. (2007). Informative Frame Classification
for Endoscopy Video. Medical Image Analysis Vol.
11, No 2:100-127.
Chung, A. J., Deligianni, F., Shah, P., Wells, A. and Yang,
G. Z. (2006). Patient Specific Bronchoscopy Visu-
alisation through BRDF Estimation and Disocclusion
Correction. IEEE Transactions of Medical Imaging
25(4):503- 513.
Duplaga, M. and Socha, M. (2005). Aplikacja oparta na bib-
liotece VTK wspomagajca zabiegi bronchoskopowe.
Bio-Algorithms and Med-Systems I(l/2):191-196.
Rai, L., Merritt, S. A. and Higgins, W. E. (2006). Real-
time image-based guidance method for lung-cancer
assessment. IEEE Conf. Computer Vision and Pattern
Recognition 2:2437-2444.
Mori, K., Deguchi, D., Sugiyama, J., Suenaga, Y., Toriwaki,
J., Maurer, C. R. Jr, Takabatake, H. and Natori, H.
(2005). Tracking of a bronchoscope using epipolar
geometry analysis and intensity-based image registra-
tion of real and virtual endoscopic images. Med. Im-
age Anal. 6:321-365.
Iakovidis, D. K., Maroulis, D. E. and Karkanis, S. A.
(2006). An Intelligent System for Automatic De-
tection of Gastrointestinal Adenomas in Video En-
doscopy Computers in Biology and Medicine. Vol. 36,
10:1084-1103.
Przelaskowski, A., Bargiel, P., Sklinda K. and Zwierzynska
E. (2007). Ischemic stroke modeling: multiscale ex-
traction of hypodense signs Lecture Notes in Artificial
Intelligence 4482:171-181, Springer Verlag.
Tamura, H., Mori, S. and Yamawaki, T. (1978). Textu-
ral features corresponding to visual perception IEEE
Trans. Systems, Man. and Cybern. Vol. 8, 6:460-472 .
Do, M. N. and Vetterli, M. (2005). The contourlet trans-
form: an efficient directional multiresolution image
representation IEEE Trans Image Proces. Vol. 14,
12:2091-2106 .
Donoho, D. L. and Huo, X. (2001). Beamlets and Multi-
scale Image Analysis Computational Science and En-
gineering, Multiscale and Multiresolution Methods,
Springer.
Buckheit, J. B. and Donoho, D. L. (2005). WaveLab and
Reproducible Research Dept. of Statistics, Stanford
University, Tech. Rep. 474.
VISAPP 2010 - International Conference on Computer Vision Theory and Applications
542
