
W2M2: WIRELESS WEARABLE MODULAR MONITOR
A Multifunctional Monitoring System for Rehabilitation
Antonio J. Salazar
1,2
, Ana S. Silva
1,2
, Claudia Silva
3
, Carla M. Borges
1,2
,
Miguel V. Correia
1,2
, Rubim S. Santos
3
and João P. Vilas-Boas
4
1
Instituto de Engenharia de Sistemas e Computadores do Porto (INESC Porto), R. Dr. Roberto Frias 378, Porto, Portugal
2
Faculdade de Engenharia da Universidade do Porto (FEUP), R. Dr. Roberto Frias s/n, Porto, Portugal
3
Centro de Estudos do Movimento e Actividade Humana (ESTSP-IPP), R. Valente Perfeito 322, V. N. Gaia, Portugal
4
CIFI2D, Faculdade de Desporto da Universidade do Porto, Rua Dr. Plácido Costa 91, Porto, Portugal
Keywords: Wearable, Rehabilitation, Modular monitoring system, Biosignal/inertial data logging.
Abstract: Wearable/portable biometric/physiological monitoring devices are rapidly becoming a recognized
alternative in medicine, rehabilitation and sports. Developments in sensors, energy harvesting, embedded
technology, smart textile, to mention a few, are driving the field to more seamless and complex solutions,
sometimes part of pervasive strategies for activity monitoring. Additionally, the number of sensors forming
part of wearable solutions seems to be incrementing thanks to miniaturization and lowering components
cost. Consequently medical and rehabilitation protocols and standards are undergoing the slow process
required for adaptation to such emerging trends. This article presents a simple, modular, low-cost, wearable
device originally intended for rehabilitation data gathering. Such device was based on commercially
available components which can be assembled and managed by physicians, therapist and other healthcare
personnel through a proposed platform. The objective is the familiarization and even active inclusion of
healthcare personnel in the technological development process and, more importantly, the incorporation of
electronic data acquisition in their procedures.
1 INTRODUCTION
Rehabilitation, healthcare and sports share a natural
affinity, especially in this age when healthcare
management seems to focus more on healthy
lifestyles and prevention. Such affinity is not limited
to the upkeep of a healthy condition through
exercise or the recuperation of an injury through
rehabilitation, but also at a technological level.
Nowadays, technology is providing new tools to all
three fields and entering within the individual’s
home at times. Wireless sensor networks,
implantable devices, textile integrated circuitry and
other achievements have allowed for designs that
require less energy and remain on site for longer
periods of time. Some systems are appearing now on
the market capable of human movement analysis and
for physiotherapy assistance. However, their
institutional oriented approach makes them
impractical for widespread usage due to highly
technical learning curves and/or required
accommodations size and electrical requirements;
not to mention prohibitive costs.
An interdisciplinary team was formed in order to
design and implement a simple and low-cost data
gathering platform, originally focused for the
development of quantifiable rehabilitation progress
methodologies. Commercially available components
were considered with the premise of the final
solution being adaptable and maintainable by non-
technical proficient persons; thus, high available
components and user-friendly solutions were
preferred.
1.1 Rehabilitation Protocols and
Procedures
The fields of physiotherapy and rehabilitation are
rapidly developing areas of health science that
covers a wide spectrum of multidisciplinary
intervention with several research and clinical
subspecialties. Rehabilitation in its broaden sense is
becoming a cornerstone of interest for both policy
makers and service providers within health and
213
J. Salazar A., S. Silva A., Silva C., M. Borges C., V. Correia M., S. Santos R. and P. Vilas-Boas J..
W2M2: WIRELESS WEARABLE MODULAR MONITOR - A Multifunctional Monitoring System for Rehabilitation.
DOI: 10.5220/0003785702130218
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2012), pages 213-218
ISBN: 978-989-8425-91-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)
social care agencies, mainly due to the expected
growing number of elderly people. However, the
impact and interweaving of rehabilitation on the
daily activities of an individual are not sufficiently
emphasized. There exists a need for the investment
of resources aimed to promote quality research in
order to overcome challenges that both therapists
and patients face in real life settings. The
rehabilitation process tends to involve and affect a
number of interpersonal relations that go beyond the
therapist-patient dynamics, shaping communal inter-
dynamics at all levels of social structures; from
families to governments, as illustrated on Figure 1.
Modern technological developments for
rehabilitation must consider such inter-dependency
complexity, thus favoring low-cost adaptable
solutions seeking integration in everyday scenarios
as opposed to rigid strategies meant for limited
usability.
Figure 1: Inter-dynamics of social structures involved in
therapy/rehabilitation process.
An in depth understanding of the human body in
everyday scenarios, advanced skills in physical
assessment, and experience in hands-on
management, allow physiotherapists to manage a
broad range of conditions, with the fundamental goal
of promoting wellness, mobility and independent
function, throughout the lifespan of the individual
(Tate, 2006). Rehabilitation interventions should
specifically address the individual’s impairment; be
sufficiently difficulty to challenge the motor system
and integrate strategies to develop transfer of
performance gains from the training situation to
everyday life (Cirstea and Levin, 2007). Being this
the ideal scenario, an enduring question facing not
only rehabilitation as a field, but healthcare in
general, is whether and to what extent
methodologies and protocols used are effective, and,
if so, whether they are efficient (DeJong, Horn,
Gassaway, Slavin, Dijkers, 2004). Clearly the
answer is dependent on the knowledge of the value
of the outcomes, not only for patients, but also for
end-payers and society as a whole.
A crucial aspect guiding physiotherapist’s
clinical reasoning, and thus design of rehabilitation
intervention, is the assessment of motor
performance; in fact, according to Paten et al. (2010)
implementing therapeutically programs require
accurate clinical and field measurements based on
motor pattern identification not readily available
from traditional tools. Standardized clinical motor
assessments rely on physiotherapists observational
skills, which although may be considered useful,
remains insufficient for reliable measurement of
certain quantitative features (e.g., intersegmental
coordination, quality of movement and smoothness).
Moreover observation-based assessment is subject to
observer induced error, resulting from poor training
(thus mostly confined to more experienced
professionals), personal bias, limited capacity of
human visual perception, just to mention some. The
Rivermean motor assesment (RMA), Fugl-Meyer
motor assessment (FMA), postural assesment scale
for stroke patient (PASS) and the reach performance
scale (RPS) are examples of viable and reliable
measurement instrument commonly used in
physiotherapy. In what refers to evaluation
instrumentation encountered in the laboratory
environment, relevant to the field at hand, one can
refer to EMG, force platforms and complex
image/video analysis systems, that introduce a
degree of objectivity in the interpretation of events,
augmenting the therapist/physician perspectives in
what refers to functional and motor characterization.
However, such resources accessibility in clinical
environment is scarce or null, restricting their
routinely usage from clinical rehabilitation practices.
Physiotherapists clinical practice reality
concerning data gathering and recording is far from
being effective, despite general guidelines
concerning this matter. In fact this important step of
the overall rehabilitation process is many times
absent and when present tends to be mainly
subjective and qualitative, based on the therapist
opinions and patient’s provided information,
regarding movement restoration and overall
progress. Such recordkeeping varies from institution
to institution, from therapist to therapist, and are not
necessarily updated at each session; therefore a
progressive evaluation based on such records
remains subjective to the experience and
interpretation of the reader, which clearly
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
214
contributes to a chain-cycle of deteriorating results,
both in progress and outcomes. Quantitative data
records provide a means for efficient and expedient
analysis of the effectiveness of a therapy on a
patient’s progress, safeguarding from negative
activities that can go unnoticed and unrecorded.
Such approach strengthens and streamlines internal
technological platforms, expanding their coverage
and added-value; promoting the formulation of
standards and protocols for patient progress
monitoring, thus compensating current guidelines.
2 W2M2 ARCHITECTURE
The system hereby presented was originally
intended to address post-stroke upper limb
rehabilitation monitoring. Post-stroke rehabilitation
reality within Portugal (and in most parts of the
world for that matter) is far from being ideal or even
effective, from both the clinically and economical
point of view. In fact, given the growing number of
stroke victims in recent years (portuguese statistical
data reported a mortality rate due to cerebrovascular
diseases per 100.000 inhabitants of 133.9, in 2009
(Portuguese Official Statistics, 2009)) this clinical
condition is considered a major burden on the
healthcare system. Despite the elevated related cost,
there is a general agreement of the importance of
addressing the sequelas of stroke, both due to acute
and sub-acute scenarios, albeit the long-term nature
of the chronic phase. In spite of the well establish
beneficial effects of timely and continuous managed
rehabilitation, there is a clear need to improve its
quantity, quality and overall effectiveness.
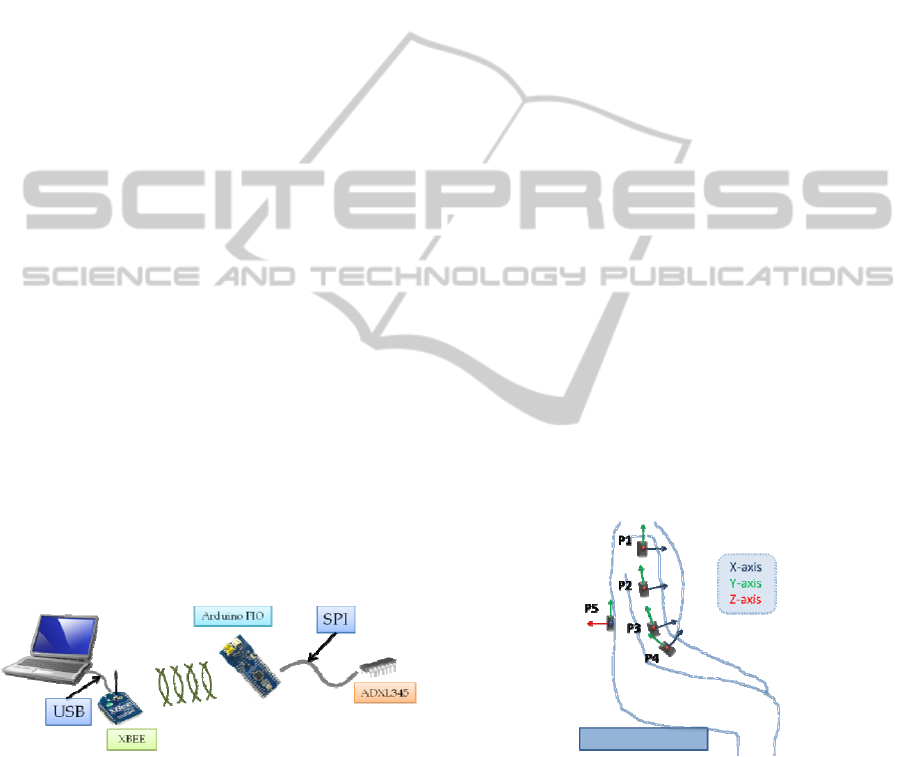
Figure 2: Component view of first W2M2 prototype.
At the request of physiotherapists pursuing
alternative therapies for home-based rehabilitation
for post-stroke individuals, a simple inertial
monitoring device was design and implement. The
device was based on commercially available
components that could be assembled in a fast
manner, without extensive knowledge of electronics;
seeking to reduce overdependence on collaborating
engineers. The system concept seen on Figure 2 is
based on a modular approach and almost out-of-box
ready-to-use.
The module’s main component, the Arduino®
FIO, is accessible at low cost and can be
programmed with a reduced learning curve; while its
numerous features such as communication protocols
(IIC, SPI), external interrupts and a number of
analog and digital I/O pins, provide design
flexibility. Additionally, a large amount of open
source resources are available for fast-paced
prototyping and when combined with an XBEE®
based wireless interface, transforms the module in a
portable, wireless adaptable resource. The XBEE®
modules can be readily purchased and are offered
with varying ranges and antennas versions. A
number of inertial and physiological sensors can be
combined with the module, both digital and analog
in nature. Common communication protocols, such
as the IIC and SPI, can be used to chain a number of
modern sensors. The ADXL345 3-axis
accelerometers break-out board was used in this case
for initial testing, permitting data gathering for upper
limb reach based rehabilitation exercises that seek to
generate inertial based biomechanical models for
compensatory movement determination. The sensor
board was encased in a 5.5 x 3 x 2.5 cm standard
project box and fastened on the target individual’s
body through flexible Velcro ended straps (double
sized athletic/rehabilitation tape can also be used for
awkward positions). Figure 3 illustrates a number of
tested sensor positions, utilized for a reach-press-
return post-stroke patient study.
Figure 3: Sensor locations.
The 3-axis accelerometers data was captured at a
frequency of approximately 100 Hz, which was then
buffered and transmitted wirelessly. After package
format verification, the data was processed in
Matlab by applying a simple smoothing strategy and
an auto movement start/end determination based on
a window differentiation function. Supplementary
lines were added for signal stability referencing as
can be observed on Figure 4 a). An example of the
W2M2: WIRELESS WEARABLE MODULAR MONITOR - A Multifunctional Monitoring System for Rehabilitation
215
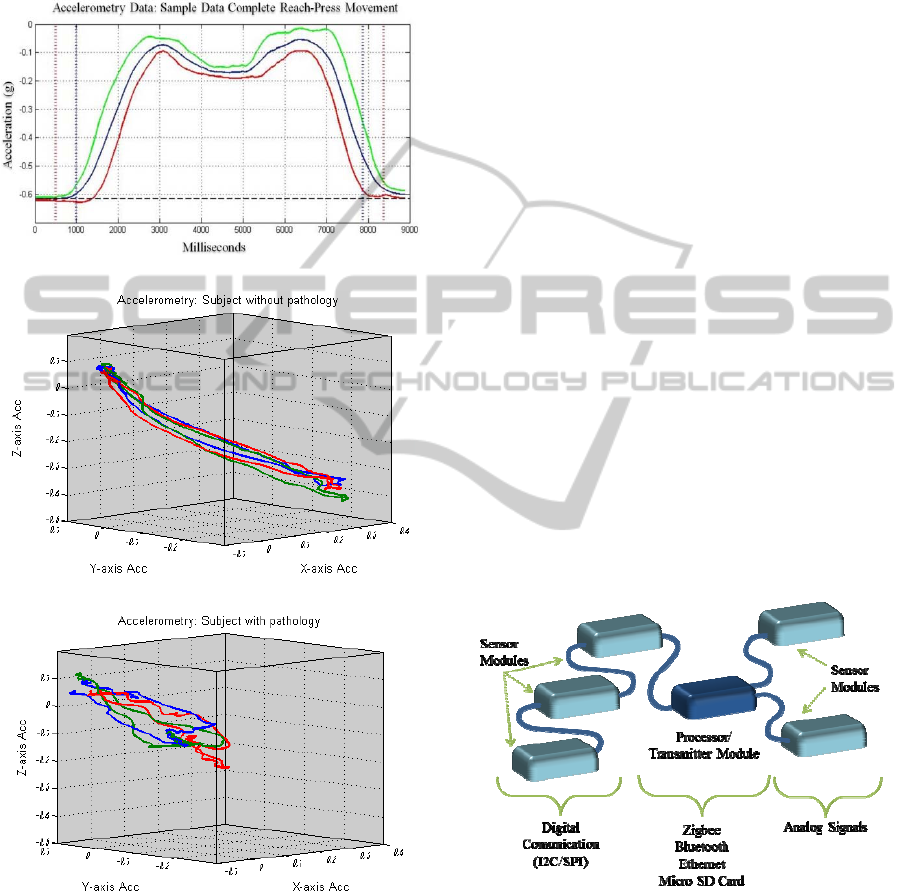
processed data illustrating the difference between
three independent reach-press.return trials by a
subject without pathology and a subject with
pathology can be seen on Figure 4
Figure
4 b) and c)
respectively.
(a)
(b)
(c)
Figure 4: Sample accelerometry data a) single axis
complete reach-press-return; three independent
accelerometry for reach-press-return b) subject without
pathology c) subject with pathology.
Field usage of the prototype generated a number
of requests by physiotherapist and patients, not to
mention an improved appreciation of the undergone
therapy process. Such gain understanding translated
into a conceptual idea for a modular solution which
allows for an integration of different sensor modules
according to the needs of specific rehabilitation
methodologies. The improved concept considered
multiple modules, either through digital or analog
communication, which could be connected to the
processing unit transforming the original W2M2 into
a multi-purpose monitoring system. Due to the
number of current available sensors, the advantage
to incorporate modules provides a flexibility which
permits the system to adapt to the therapist and
patient on a needs-basis.
At this stage, the W2M2 allows the
interconnection of accelerometer and gyroscope
boards, electrodes, capacitive and galvanic sensors
and also an On/Off sensor, nonetheless the use of
standard communication protocols such as IIC and
SPI permit interconnect to a wide variety of
commercially available sensors which may be added
to address a particular purpose (see Figure 5).
Although, emphasis has been on sensor
interconnection for data gathering, feedback
modules have been considered since the preliminary
stages of the project in order to address home-based
or remote rehabilitation assistance. Digital pre-
processing previous to signal transmission allows for
dataset reduction and optimization for data fusion,
pattern recognition, event detection and feature
extraction strategies; not to mention auto-feedback
response for specific situations as compensatory
movement determination or fall scenarios.
Figure 5: Modular approach of the W2M2.
From a user interface side a number of
alternatives exist for development, such as visual
studio based application, java based application,
scripting languages, even data processing
application such as Excel, Matlab and Labview.
Initial data gathering and visualization was
performed using Processing, an open source
programming language which permits interfacing
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
216
with Arduino® based boards with a minimal
learning curve. The language permits for fast
application implementing and can serve for a
number of specific objectives. In order to provide a
more complete solution, which maintained an
organized database of demographic data and clinical
scores in conjunction with the gathered data, that
said, a VB2010 based application for database
management, data visualization and ease of user
interfacing and control was developed. However,
due to the wireless interfacing through an XBEE®
based USB to serial unit base, software counterparts
can be developed in a wide number of platforms as
mentioned previously. The possibility also exist to
use Bluetooth based XBEE® modules in order to
interface with mobile technology such as cell
phones, or directly with most laptops, tablets and
other devices.
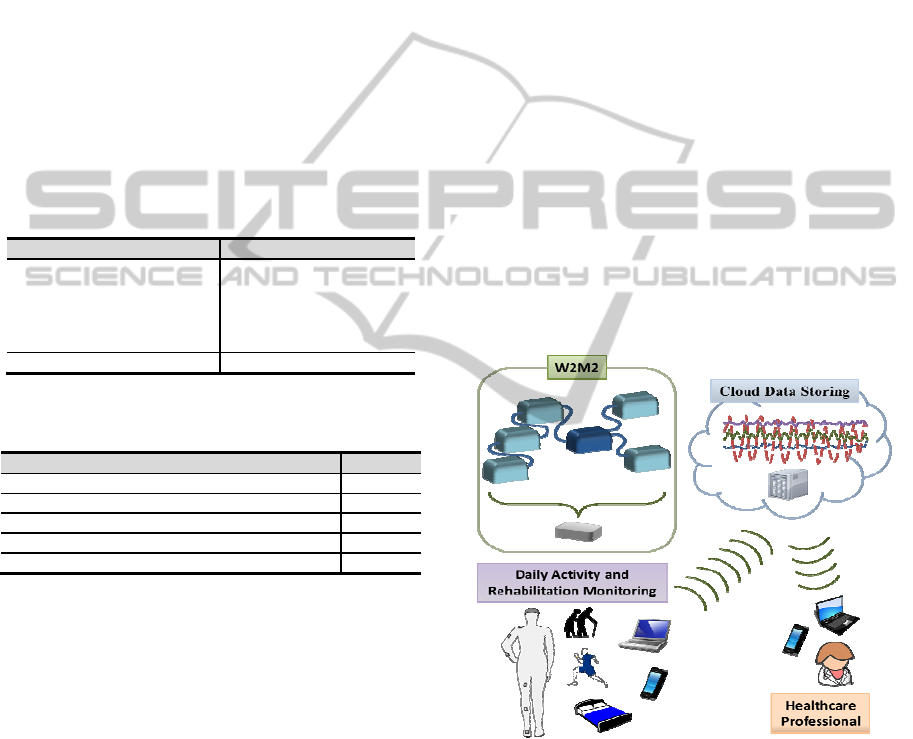
Table 1: Main module and PC interface cost.
Item Cost per Item Total
Arduino FIO 20 20
XBEE modules 30 60
USB – XBEE interface 25 25
Rechargeable Battery 10 10
Misc. (cases, cables, etc) 20 20
Total
- 135
Misc.: miscellaneous
Table 2: Sensor cost examples.
Sensor boards Cost
ADXL 345 3-axis accelerometers 22
IDG500 Dual gyroscopes 34
ITG3200/ADXL345 3-axis acc. & gyr. combo 50
HMC5843 3-axis magnetometer 18
MPR121 12-electrode capacitive touch 9
Acc.: accelerometer; Gyr.: gyroscope
From a cost perspective the W2M2 system is a
low-cost solution, especially when compared to
other physiological and biological signal monitoring
devices available in the market. Devices such as
Biopac, Plux, Biodex and video based solutions
from Qualysis and Viacom are just some examples
of system being used today in rehabilitation and
medical research. These systems retail from
thousands to hundreds of thousands Euros, and tend
to require equally expensive add-ons. In contrast, the
W2M2 can be constructed under 150 Euros and the
sensor components tend to cost less than 50 Euros,
as presented on
Table
1 and
Table
2. In order to
insure good connectivity and measurement
reliability a printed circuit board (PCB) can be
designed for interconnecting the sensor board with
the chosen connector, and sent for manufacturing to
a number of online sites; however such process
tends to cost upwards of 50 Euros for a limited
number of boards. Prototyping boards can offer a
low-cost alternative, especially during initial trials.
Custom sensor solutions, such as electromyography
(EMG) or bioimpedance, can be constructed using
battery based instrumentation amplifiers and
operational amplifiers, and the analog I/O pins of the
main module.
The W2M2 is the key part of a more global data
gathering platform that can be used for home-based
rehabilitation monitoring and as a portable data
acquisition system, as illustrated on Figure 6, which
permits the generation of databases that can be
shared and analyzed for an increase understanding of
human responses to their surroundings under a
number of scenarios (in this case rehabilitation
progress monitoring). There exist a number of
options for remote monitoring interfacing, be it by
periodic data uploading for remote progress analysis,
or real-time one-on-one physiotherapist-patient
sessions. Such interfacing can be achieved through
custom made applications programmed in free
software such as PHP or Visual Basic; or by
utilizing chat applications that allowed for file
sharing and video conferencing.
Figure 6: Complete data acquisition system overview.
3 DISCUSSION
A number of factors have contributed to the fast-
paced development of wearable monitoring
technology of the past decade, where
interdisciplinary collaboration is a factor of
paramount importance. medical/rehabilitation
professionals combining efforts with
scientist/engineers has become commonplace,
W2M2: WIRELESS WEARABLE MODULAR MONITOR - A Multifunctional Monitoring System for Rehabilitation
217

advancing areas which traditionally were slow to
adapt. Some systems are now appearing capable of
human movement analyze and for physiotherapy
assistance (Zhou and Hu, 2007; Pérez et al., 2010);
however, their institutional oriented approach makes
them impractical for widespread usage due to highly
technical learning curves and/or required
accommodations size and electrical requirements;
not to mention prohibitive costs. The system
presented seeks to ease the data gathering process by
offering an adaptable low cost alternative that can be
used and modified by physician, therapist and even
patients (for home-based and/or remote solutions).
Its portability allows for data gathering in a number
of diverse scenarios including home-based
rehabilitation, or even daily-activity, monitoring;
altering the therapist-patient dynamics by extending
the rehabilitation process.
Currently, visually based biomechanical models
seem to dominate the field, probably due to
traditional appreciation methodologies for patient
progression; however, inertial, chemical, electrical
sensors are broadening the perceptual capacities of
current rehabilitation practices, introducing the need
for new approaches and models. Through data
gathering practices by physicians, therapist and even
patients, a body of comparable datasets can be
generated for the formulation of statistical and
analytical methods that can reveal quantifiable
methods that can contribute in the diagnosis,
treatment and follow-up of numerous conditions.
4 CONCLUSIONS
A data acquisition system was designed and
developed as a low-cost, fast implementable
alternative for rehabilitation monitoring. Although
the device was originally thought for post-stroke
upper limb rehabilitation monitoring, its flexibility
and adaptability allowed usage in a number of
monitoring objectives. The device seeks to ease the
data gathering process by therapist and others, in
order to facilitate the development of quantifiable
methodologies and protocols.
ACKNOWLEDGEMENTS
The authors would like to thank the Foundation for
Science and Technology of Portugal for their
support of some of the PhD students involved in this
article (SFRH/BD/61396/2009 and SFRH/BD/609
29/2009). Additionally, the authors would like to
acknowledge the contribution of all volunteers that
took part of the testing procedures.
REFERENCES
Cirstea, M.; Levin, M. 2007. Improvement of arm
movement patterns and end-point control depends on
type of feedback in stroke survivors. Neurorehabil
Neural Repair. 21: 398-411.
DeJong, G., Horn, S., Gassaway, J., Slavin, M., Dijkers,
M. 2004. Toward a taxonomy of rehabilitation
interventions: using an inductive approach to examine
the “black box” of rehabilitation. Arch Phys med
Rehabil. 85: 678-86.
EMB Technical Committee on Wearable Biomedical
Sensors & Syst. Available http://tc-wearable-sensors.
embs.org/
Laerhoven, K. V., Lo, B., Ng, J., Thiemjarus, S., King, R.,
Kwan, S., Gellersen, H. W., Sloman, M., Wells, O.,
Needham, P., Peters, N., Darzi, A., Toumazou, C.,
Yang, G.-Z. 2004. Medical Healthcare Monitoring
with Wearable and Implantable Sensors. Paper
presented at the 3rd Int. Workshop on Ubiquitous
Computing for Healthcare App.
Paten, S., Hughes, R., Hester, T., Stein, J., Akay, M., Dy,
J., Bonato, P.: Tracking Motor Recovery in Stroke
Survivors Undergoing Rehabilitation Using Wearable
Technology. 32nd Annual International Conference of
the IEEE EMBS, pp. 6858 – 6861. IEEE Press, (2010)
Pérez, R., Costa, Ú., Torrent, M., Solana, J., Opisso, E.,
Cáceres, C., Tormos, J., Medina, J., Gómez, E. J.
2010. Upper Limb Portable Motion Analysis System
Based on Inertial Technology for Neurorehabilitation
Purposes. Sensors, 10.
Portuguese Official Statistics. Health Database on Rate of
potential years of life lost due to cerebrovascular
diseases per 100 000 inhabitants, 2009.
Tate, D. 2006. The state of rehabilitation research:art or
science?. Arch Phys Med Rehabil. 87: 160-6
Tufail, F., and Islam, M. H. 2009. Wearable Wireless
Body Area Networks. Paper presented at the
International Conference on Information Management
and Engineering.
Zhou, H., Hu, H. 2007. Upper limb motion estimation
from inertial measurements. International Journal of
Information Technology, 13(1).
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
218
