
Development of Retention System of the Autonomous Endoscopic
Capsule and Its Functionalities
Dmitry Mikhaylov
1
, Timur Khabibullin
1
, Igor Zhukov
1
, Andrey Starikovskiy
1
,
Landish Gubaydulina
2
, Natalya Romanchuk
2
and Vladimir Konev
1
1
Engineering Centre of the National Research Nuclear University “MEPhI”,
Kashirskoye highway 31, 115409, Moscow, Russian Federation
2
The Clinical Hospital № 85, Moskvorechie street 16, 115409, Moscow, Russian Federation
Keywords: Electroactive Polymer, Endoscopic Capsule Retention System, Expandable Capsule, Angular Orientation,
Cancer, Fluorescent Beacon.
Abstract: The aim of the research is to propose the retention system of the wireless endoscopic capsule allowing more
detailed observation of stomach, small intestine as well as other parts of the digestive tract. The capsule has
an outer layer or whiskers made of an electroactive polymer material that expands under influence of an
applied voltage. An electroactive polymer expands up to 50% of its original size and creates a roughly ball-
shaped object approximately 3 cm in diameter (in case of whiskers – they change their angular orientation).
The performance (changing the size) of the mock-up of the capsule with eight whiskers made of
electroactive polymer was tested using a silicone model with sensitive sensors simulating the digestive tract
of a person. The probability of failure-free operation and the mean time to failure for capsule and recording
device integrated circuits were calculated.
1 INTRODUCTION
Capsule endoscopy is a way to record images of the
digestive tract for use in medical examination and
diagnosis. The patient swallows the capsule which
goes down the digestive tract as ordinary food and
the capsule takes images. They can be obtained at
any point of the stomach or the gastrointestinal tract.
The images are sent to a recording device that the
patient can carry or be close to during the procedure.
The primary use of endoscopic capsule is to
examine areas of the small intestine that cannot be
seen by other types of endoscopy, such as
colonoscopy or esophagogastroduodenoscopy
(EGD).
This type of examination is often done to find
sources of bleeding or abdominal pain. The
procedure was approved by the Food and Drug
Administration of the United States in 2001
(Scherbakov P.L., 2010). Upper endoscopy, EGD
uses a camera attached to a long flexible tube to
view the esophagus, the stomach and the beginning
of the first part of the small intestine called the
duodenum.
A colonoscope, once inserted through the
rectum, can view the colon and the distal portion of
the small intestine, the terminal ileum.
Unfortunately, these two types of endoscopy cannot
visualize the majority of the middle portion of the
gastrointestinal tract, the small intestine. (R. de
Francis, 2012)
Therefore, capsule endoscopy is useful when
disease is suspected in the small intestine and can
diagnose sources of occult bleeding (blood visible
microscopically only) or causes of abdominal pain,
such as Crohn's disease or peptic ulcers (Lecheng
Yu, 2012; Jebarani, W.S.L, 2013; Dongmei Chen,
2011).
Once swallowed, the capsule needs to be
controlled in order to acquire images of the entire
area.
There are two problems that gastroenterologists
face while conducting examination. In the stomach
capsule is relatively fast directed by peristalsis that
does not allow to examine certain parts or areas of
interest. In other parts of the digestive tract the
situation is reverse. In the intestine the peristalsis
may be poor (this is true especially for people with
77
Mikhaylov D., Khabibullin T., Zhukov I., Starikovskiy A., Gubaydulina L., Romanchuk N. and Konev V..
Development of Retention System of the Autonomous Endoscopic Capsule and Its Functionalities.
DOI: 10.5220/0004719400770084
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2014), pages 77-84
ISBN: 978-989-758-013-0
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
gastrointestinal pathologies and diseases) whereby
the capsule may get stuck until it is taken out by the
food. Moreover, because of its small size the capsule
can be subject to a greater rotation in the small
intestine, which could potentially cause missing of
pathologies. (R. de Francis, 2012)
Resently many studies have been carried out to
solve the problem of capsule control (Kim Y.T.,
2010; Woo S.H., 2011; Park H.J., 2005; Zuo J,
2005; Chiba A, 2005; Sungwook Yang, 2011;
Wenwen Chen, 2013). They show good results and
present original ideas; however, the possible
disadvantages of these proposals may be large
capsule power consumption limiting the examination
time, necessity in additional sophisticated
equipment, etc.
Consider conventional capsules that may be
controlled by forces of the magnetic field. For
example, such a capsule is described in DE
102006019986 (Johannes Dr. Reinschke, 2007). The
disclosed endoscopy capsule for use in patient's
gastrointestinal tract has a magnetic element
enabling rotating, swivelling and tilting of the
capsule as well as an adjustable power supply unit
for providing electrical voltage used for creation of
the magnetic field.
However, magnetic field and additional electrical
circuitry increases the cost and possibly size of the
capsule. The system requires external devices that
generate magnetic fields (magnetic materials,
electromagnets). Furthermore, efficiency of the
system can be affected by a secondary magnetic
field that interacts with the metal parts of the
capsule. Essentially, the secondary magnetic field
with the intensity of the controlling field is sufficient
for disruption of capsule’s functionality.
Moreover, because of the anatomical features of
the small intestine, its tortuosity, the control system
based on the magnetic field dors not always allow
precise manipulation with capsule location.
Accordingly, there is a need in the art for an
efficient and effective endoscopic capsule that is
autonomous and can be retained in the stomach and
other parts of the gastrointestinal tract for a long
periods of time and provide easier passage through
intestine if needed.
For this end this paper deals with the new
proposal to provide endoscopic capsule with the
ability of retention enabling more detailed
examination of the digestive tract.
2 EXPANDING ENDOSCOPIC
CAPSULE
The proposed capsule endoscopy system provides an
efficient and safe way to observe a patient’s stomach
and intestinal tract. The capsule remains in the
desired part of the digestive tract acquiring images
and recording them to an external device. The
gastroenterologist can review the images and make a
diagnosis at his convenience.
The capsule does not require a special insertion
system and can be simply swallowed. The expansion
takes place in a standalone mode in response to an
outside command.
The endoscopic capsule can expand not only
inside the stomach, but in any part of the
gastrointestinal tract, for example, in the large
bowel. This enables the capsule to stimulate
peristalsis in order to accelerate its passage through
the intestinal canal.
2.1 Capsule Components
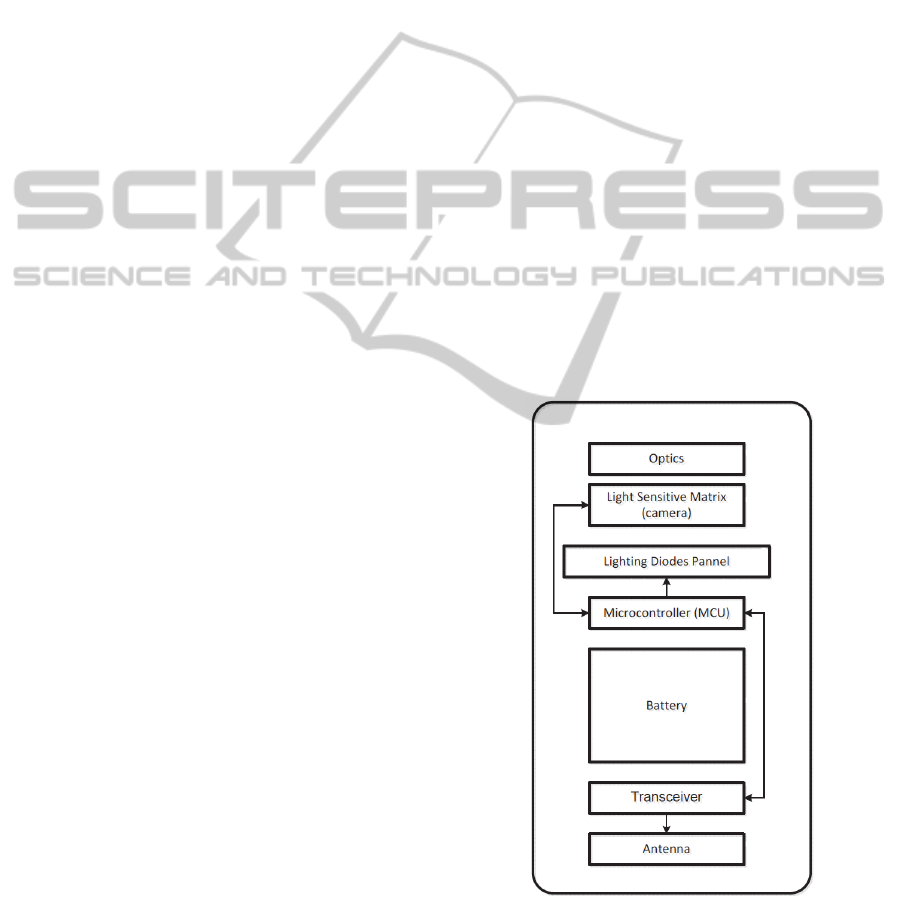
The miniature capsule consists of a light sensitive
matrix, a radio frequency transceiver, a backlighting
device and a battery.
Figure 1: Block-diagram of the wireless endoscopic
capsule.
Figure 1 illustrates an endoscopic capsule. The
capsule includes
an electroactive polymer material that
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
78

increases its volume inside the patient’s stomach or
intestine upon receiving a control radio signal from
an external device.
The endoscopic capsule can be, for example, 24
mm in length and about 10 mm in diameter. It
includes a microcontroller, which controls a light
sensitive matrix with optics (i.e., a miniature
camera). For example, CMOS matrix with resolution
of 640 by 480 pixels can be used. The optics can be
a plurality of lenses.
The endoscopic capsule includes a LED panel
for providing lighting for the light sensitive matrix
for taking images.
The microcontroller controls the light sensitive
matrix and the LED panel in order to synchronize
the light flashes with the image taking (the duty
cycle of the LED illumination can be 6.6%, or two
flashes per second, 1/30 of a second each).
A built-in camera takes two images per second,
which are then compressed and transmitted
according to medical regulations. Since battery life
and transmission speed are limited, a typical
transmission is 240 x 240 pixels per image, with 8
bit colour, which is often insufficient for medical
purposes.
To improve image resolution and reduce power
consumption some data analysis can be performed
locally (i.e., in the capsule), to avoid transmitting
images that have not changed from previous ones.
Also, images that are very similar to previous ones
(even if not identical) also might not be transmitted
depending on degree of similarity (e.g., 90% similar
or 95% similar, etc.). Images that are too dark to
contain much information also might not be
transmitted.
The compression and analysis can be performed
locally by the microcontroller and/or by a custom or
semi-custom integrated circuit, permitting
transmission of, e.g., 320 x 320 or even 480 x 480
pixels, with 16 bit colour.
In order for the images to provide more
diagnosis-related information, the capsule uses a
variety of colour lighting provided by colour high
emitting diodes that turn on each time a picture is
taken. For example, red light helps in detecting
micro bleedings and blue light is beneficial for
detecting structural abnormalities.
The light emitting diodes panel includes white,
red, yellow and blue diodes. The colour diodes
advantageously replace conventional flash lights
(with colour filters) that use a lot of battery charge.
The images are taken using white red, blue and
yellow illuminations in this order. However, a larger
number of the diodes can be used (for example, 8,
12, etc.). The blue lighting allows for better images
of the blood vessels, the red lighting assists in
detection of bleedings, and yellow lighting assists in
adenoma detection.
The diodes are paired by two of the same colour.
This provides for even light distribution.
Alternatively, multi-colour diodes can be used.
Additionally, special mirrors can be used in
combination with the diodes for a more even light
distribution.
The diode panel is located perpendicular to a
vertical (longitudinal) axis of the capsule, with the
diodes facing upwards. The light sensitive matrix
can be implemented in the centre of the diode panel.
The capsule is covered by a phosphorescent layer
for additional lighting. Thus, the pictures taken by
the endoscopic capsule are, advantageously, more
accurate for diagnosis making.
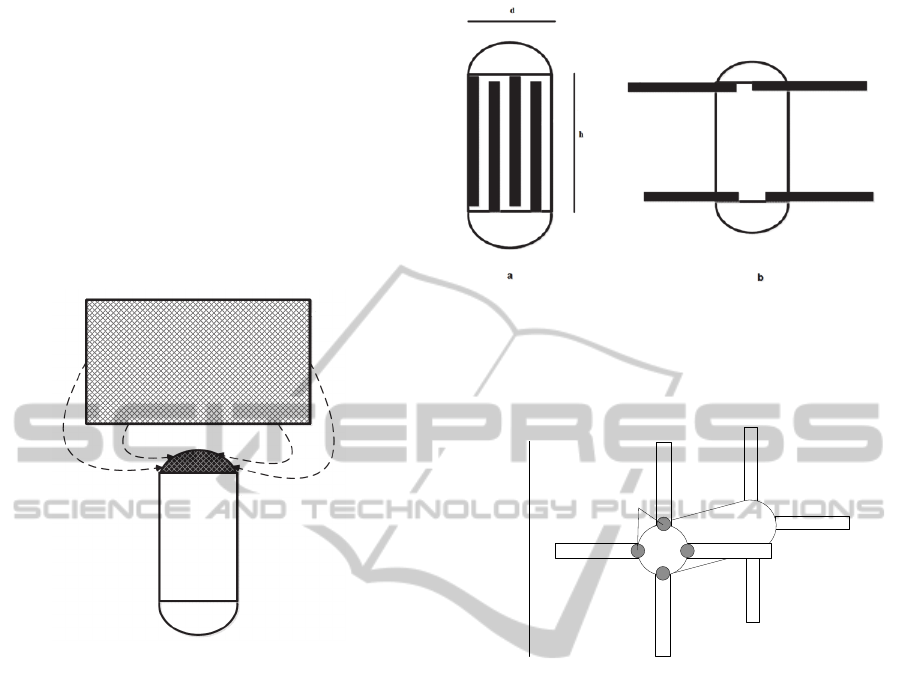
Figure 2 illustrates phosphorescent coating of the
endoscopic capsule. The capsule is covered by the
phosphorescent coating (Fig. 2a). In order to project more
light forward, the cover of the capsule is implemented in a
corrugated shape as shown in Fig. 2b. The corrugation of
the cover is implemented in a lateral plane. If the
phosphorescent coating is used in combination with light
emitting diodes, the frequency of light emission of the
diodes and the phosphorescent coating needs to be
synchronized. Phosphorescent coating of the capsule
should not be affected by the electroactive polymer.
Figure 2: Phosphorescent coating.
The microcontroller is connected to a radio
transceiver having an antenna. For example, a
transceiver made by ZARLINK can be used. This
transceiver uses standard frequency of 403-405 mHz
with a power of 25 mW (Mikhaylov D.M., 2013).
The antenna can be integrated into the body of
the capsule for better reception/transmission
characteristics. The radio transceiver provides
signals to the microcontroller for activation of the
electromagnetic cover and expanding the capsule.
DevelopmentofRetentionSystemoftheAutonomousEndoscopicCapsuleandItsFunctionalities
79

The capsule is wirelessly connected to a portable
recording device that receives images and records
them to an integrated memory for review by a
gastroenterologist.
A battery powers the circuits within the capsule.
The battery can be, for example, shaped as a round
tablet with a diameter of 4-8 mm and a height of 9
mm (or 5-10 mm, generally).
After examination is completed, the
microcontroller receives a signal through the radio
transceiver for reducing the voltage and deactivating
the electroactive polymer outer layer of the capsule.
Subsequently, the capsule (i.e., the electroactive
polymer layer) shrinks back to an original size, goes
down the intestinal tract and leaves the body in a
natural way.
The recorder with the images is then provided to
the gastroenterologist, who analyses the images at a
workstation using medical image processing
applications.
2.2 Capsule Retention System
In quite a number of cases specialists need long-term
visual observation. Such long-term observation may
be easily implemented if capsule endoscopy is
applied using the capsule. The endoscopic capsule
has a possibility of its retention in the stomach for
more detailed study. It is especially important, for
example, when the cancer of the stomach is
suspected or diagnosed.
The system of the capsule retention in the
stomach consists of the following components:
1. A balloon module that includes the following
elements:
a cover made of an elastomeric dispersive
material, such as dimethylpolysiloxane;
a valve made of a sheet dimethyl-polysiloxane
(Med 2174) with a silicone adhesive (Med
4213);
a silicone cover applied by dipping (Med 6607);
a silicone elastomer (Med 4850) and tantalum (in
order to make the valve impenetrable to
irradiation).
2. The cover for a balloon module made of the
following exemplary materials to facilitate the
allocation and intubation of the device:
dimethyl-polysiloxane dispersion;
bicarbonate of soda to ease the installation of the
balloon into the cover and to prevent the
intermolecular cross-linkage during storage.
3. A block of the conductor material made of the
following materials and components:
stainless steel 304, covered with
polytetrafluoroethylene;
polypropylene box-coupling of Lyuer;
an adhesive (Loctite 3201).
4. A filling tube made of the following
components and materials:
the tubes made of a silicone elastomer (Q7-4780)
by extrusion;
a tip of the filling tube made of polypropylene;
a box-coupling of Lyuer made of polypropylene.
As one option, the balloon can be made of
polyvinyl chloride (PVC), and inflated from a built-
in remotely triggered compressed air storage. As a
further option, the balloon can be inflated through a
catheter-like thread that extends through the
oesophagus when the capsule is in the stomach.
In addition the balloon can be made of an
electroactive polymer shaped like a ring (torus)
around the capsule that “unfolds” to a much larger
diameter through a change in angular orientation.
The cover is fixed to the capsule in such a way that
the opaque part is located inside the transparent
balloon.
The outer surface of the capsule is made of an
electroactive polymer material that increases its
volume under influence of a voltage, like a balloon,
or changes its angular orientation.
An electroactive polymer that covers the capsule
expands to 30-50% of its original size and creates a
roughly ball-shaped object approximately 3 cm in
diameter (Fig. 3). This size is sufficient for retention
in the stomach that normally has a passage of
approximately 2-2.5 cm in diameter into the
digestive tract.
Figure 3: Expanded capsule (ball-shaped).
Electroactive polymer materials are widely used
today as artificial muscles in robotics (Henry
Sheppard, 2007) and manufactured by several
companies, for example, Environmental Robots Inc.
(Environmental Robots Inc., 2014).
The capsule is retained in the patient’s stomach
and can be used for a prolonged generation of
images of various areas. This can be especially
useful for observation of influences of new
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
80
medications (for example, stomach cancer
medications).
The voltage is provided by the battery located
within the capsule. The battery charge of the capsule
can last for about 12 hours. As an option, in case
when a longer observation is required, the battery
can be charged wirelessly via magnetic coupled
coils, one inside the capsule and the other (or others)
outside patient’s body, so the capsule in its expanded
(inflated) state can remain in the stomach or in other
part of a gastrointestinal tract for indefinitely long
period of time (Fig. 4).
Figure 4: Capsule battery charged by magnetic field.
The capsule, as needed, can be controlled by a
magnetic field as it has a magnetic element. The
capsule has a magnetic element in a form of a
neodymium tablet about 5 (e.g., about 4-7) mm in
diameter and about 2 (e.g., about 1.5-2.5) mm in
height.
Another unique feature of the capsule is a set of
extendable whiskers that extend from the surface of
the capsule cover. This can be used as an alternative
to the balloon described above, or, as a further
alternative, the whiskers can be inside the balloon
(for example, made of PVC, and used to “inflate”
the balloon).
Figure 5 illustrates expandable whiskers made of
an electroactive polymer implemented on the
endoscopic capsule. An electroactive polymer is
triggered by an electric signal. The whiskers are
positioned along a surface of the capsule (see Fig.
5a) for convenient swallowing by a patient. Once the
capsule is swallowed, a radio signal is received and
created voltage of the opposite sign is applied at the
point of voltage application; the whiskers extend out
(changing their angular orientation) and control
movement of the capsule (see Fig. 5b and Fig.6), so
Figure 5: Expandable whiskers.
the moving stream of food does not take the capsule
down the intestinal tract.
Whiskers
Capsule body
Whi s ker s
L
Poi nts of
voltage
application
Figure 6: Expanded capsule.
The expanded capsule`s size L=d+2h≈3.5 cm (see
Fig. 5a and Fig. 6).
Diameter of the small intestine does not exceed
3-5 cm and about 2.5-3 cm in ileum (Small intestine,
2009). It means that the proposed capsule can stop at
any part of ileum and in some areas of jejunum as
well as stay in the stomach for a long period of time
(as the pylorus does not exceed 2-2.5 cm in
diameter). At the same time the expanded
endoscopic capsule can initiate peristalsis in case the
capsule gets stuck in the intestine in order to
continue the examination (R. de Francis, 2012).
The wireless endoscopic capsule uses eight
extendable whiskers for movement control.
However, an arbitrary number of whiskers can be
used depending on desired retention of the capsule.
Once all required images are taken, another radio
signal is sent to the capsule and the voltage is
terminated. Subsequently, the whiskers fold back to
the original position depicted in Fig. 5a.
DevelopmentofRetentionSystemoftheAutonomousEndoscopicCapsuleandItsFunctionalities
81

2.3 Experiments
While working on the development of the proposed
wireless endoscopic capsule`s retention system the
mock-up of the capsule with eight whiskers made of
electroactive polymer has been created. In the initial
state the capsule has the size of an ordinary pill –
13x29 mm; in the expanded state its size increases to
35x29 mm (as shown in Fig. 6).
The performance of the capsule was tested using
a silicone model with sensitive sensors simulating
the digestive tract of the person. The capsule was
forced to change its size under influence of applied
voltage (Fig. 7).
Figure 7: Experiment scheme.
50 out of 50 attempts have showed desired results.
These experiments showed that it takes on the
average 3 seconds for capsule to expand and 5
seconds to take its original shape.
2.4 Reliability Expectations
The proposed wireless endoscopic capsule
comprises three integrated circuits (light sensitive
matrix, controller and transceiver) responsible for
the execution of its functions. The circuits can be
regarded as series-connected elements in the scheme
of reliability calculation.
Mean time to failure of integrated circuits of
average degree of integration is estimated at 300 000
hours without the presence of ionizing radiation and
strong electromagnetic fields that do not occur under
normal conditions in urban and rural areas.
The probability of failure-free operation is
0.99999000003 and the mean time to failure is 100
000 hours or 11.4 years.
The capsule recording device contains 31 (field
programmable logic device, microcontroller,
memory, and 14 sensors including microcontroller
and the transceiver) microcircuits responsible for the
execution of its functions. The microcircuits can be
regarded as series-connected elements in the scheme
of reliability calculation.
The probability of failure-free operation is
0.999897 and the mean time to failure is 9 678 hours
or 1.1 years.
2.5 Capsule Options
Images acquired by the capsule can be processed
using known in the industry methods. A
gastroenterologist can review images in a real time
and make a rapid diagnosis by reviewing a colour
and a texture anomalies and pathologies of the form
that correspond to a visual manifestation of the
disease (Alexander Kukushkin, 2012; Kukushkin
Alexander, 2013; Bourbakis, N., 2005). After the
capsule remains inside a patient a certain amount of
time, a three-dimensional image of the areas passed
by the capsule can be generated and reviewed.
As a further clinical application, the
electropolymer of the capsule can be used for
dilatation of narrowed areas of the digestive tract
(for example, due to scarring, infection,
inflammation, and similar processes).
The capsule can be used to deliver a drug or
active compound from a reservoir (Fig. 8), which is
covered by a lid, formed of a memory metal, such as
Nitinol.
Figure 8: Drug delivery.
When heated to body temperature inside the
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
82

patient’s stomach, the lid opens (returns to its
original shape), permitting the active compound to
egress.
As a further option, the capsule can be provided
with:
a system for generating the trajectory that the
capsule followed, such as by using a gyroscope
and/or an accelerometer inside the capsule. The
data from these sensors is sent to the external
reader, together with the image data. This makes
it easier to determine the location of the
particular images taken by the capsule, making it
easier to know where the particular problems are
(and exactly where surgical intervention might
be needed);
a heating element, which is activated by an
operator when the capsule is near a location
where coagulation of blood leaking from cuts or
wounds is occurring;
two cameras, one for the “forward” direction,
and one for the “backward” direction, which may
be particularly useful for inspecting the intestine;
additional sensors, such as a pH sensor
(Stepanyan D.А., 2011), to determine acidity;
a magnetic coil, which can be used to increase
the resolution of magnetic resonance imaging.
The coil can be located anywhere in the capsule,
and can have arbitrary orientation.
The capsule of the present invention may be used
for early diagnosis of various oncological diseases,
particularly gastrointestinal cancers. For this
purpose, fluorescent agents/beacons can be used.
These beacons, which interact with cancerous cells,
due to their chemistry, begin fluorescing at a
wavelength in the visible, infrared and/or ultraviolet
portions of the spectrum. This fluorescence permits
diagnosing oncological diseases at an early stage
(which typically does not have noticeable
symptoms), without the use of a biopsy.
If the only purpose is to detect the existence of a
cancerous tumour, there is no need to transmit video
or image frames to a computer in real time. The
processor on the capsule can, by itself, identify those
frames that show fluorescence, based on the average
brightness of the image, and transmit only those
frames. This significantly lowers the time needed for
analysis of the gastrointestinal tract using the
capsule. For example, instead of 2-3 hours, the
diagnosis can be made within 5-10 minutes, if
oncological-related fluorescent activity is detected.
Also, there is no need for additional illumination
sources in the capsule itself. This permits increasing
the length of time of battery operation, since no
energy needs to be used for illuminating the
gastrointestinal tract.
3 CONCLUSIONS
This paper has been demonstrated the idea of
creating a retention system of the wireless
endoscopic capsule using the property of
electroactive polymer to increase the size and
change angular orientation under applied voltage.
This ability of capsule to change the shape will
allow gastroenterologists to carry out more detailed
examination of patient`s digestive tract getting
additional images of suspected areas.
The studies on further capsule construction,
reliability and functionality improvements are
underway. Although the proposed capsule has
shown good results on the silicone model it is
planned to be subjected to further field and lab
studies and tests as well as clinical trials.
REFERENCES
Scherbakov P.L. 2010. Videocapsule endoscopy: history
of development and practical use. Journal Consilium
Medicum. Gastroenterology №2.
R. de Francis, B.S. Lewis, D.S. Mishkin 2012. Capsule
endoscopy in understandable language / trans. from
English. Ed. E.D. Fedorov, E.V. Ivanova. - M:
Practical medicine. - 128 p.: Ills.
Lecheng Yu, Yuen, P.C., Jianhuang Lai 2012. Ulcer
detection in wireless capsule endoscopy images.
Pattern Recognition (ICPR), 21st International
Conference.
Jebarani, W.S.L., Daisy, V.J. 2013. Assessment of Crohn's
disease lesions in Wireless Capsule Endoscopy images
using SVM based classification. Signal Processing
Image Processing & Pattern Recognition (ICSIPR),
International Conference.
Dongmei Chen, Meng, M.Q.-H.; Haibin Wang; Chao Hu;
Zhiyong Liu 2011. A novel strategy to label
abnormalities for Wireless Capsule Endoscopy frames
sequence. Information and Automation (ICIA), IEEE
International Conference.
Kim Y.T., Kim D.E. 2010. Novel Propelling Mechanisms
Based on Frictional Interaction for Endoscope Robot.
Tribology Transactions, 53:203-211.
Woo S.H., Kim T.W., Mohy-Ud-Din Z, Park I.Y., Cho
J.H. 2011. Small intestinal model for electrically
propelled capsule endoscopy. BioMedical Engineering
OnLine, 10:108.
Park H.J., Lee J.H., Moon Y.K., Yoon Y.H., Won C.H.,
Choi H.C., Cho J.H. 2005. New method of moving
control for wireless endoscopic capsule using
electrical stimuli. IEICE Transactions on
DevelopmentofRetentionSystemoftheAutonomousEndoscopicCapsuleandItsFunctionalities
83

Fundamentals of Electronics Communications and
Computer Sciences, E88a:1476-1480.
Zuo J, Yan G, Gao Z. 2005. A micro creeping robot for
colonoscopy based on the earthworm. Journal of
Medical Engineering & Technology, 29. Pages: 1-7.
Chiba A, Sendoh M, Ishiyama K, Arai I. 2005. Magnetic
actuator for capsule endoscope navigation system.
Magnetics Conference, 2005. INTERMAG Asia 2005.
Digests of the IEEE International. Pages: 1251 –
1252.
Sungwook Yang, Kitae Park, Jinseok Kim, Tae Song Kim,
Il-Joo Cho, Eui-Sung Yoon. 2011. Autonomous
locomotion of capsule endoscope in gastrointestinal
tract. Engineering in Medicine and Biology Society,
EMBC, Annual International Conference of the IEEE.
Pages: 6659 – 6663.
Wenwen Chen, Guozheng Yan, Shu He, Quan Ke, Zhiwu
Wang, Hua Liu and Pingping Jiang. 2013. Wireless
powered capsule endoscopy for colon diagnosis and
treatment. Physiological Measurement, 34. Pages:
1545–1561.
Johannes Dr. Reinschke 2007. Endoscopy capsule for use
in patient`s gastrointestinal tract, has magnetic
element provided for rotating, swiveling and tilting
capsule, and adjustable power supply unit for
subjecting electrical conductors with electrical
voltage. German Patent DE102006019986. URL:
http://www.freepatentsonline.com/DE102006019986A
1.html.
Mikhaylov D.M., Zhukov I.U., Froimson М.I. 2013.
Review of radio transceivers used in implantable
devices. Scientific and technical Journal “Specialized
machinery and communication”, №4. Moscow. Pages:
38-40.
Henry Sheppard 2007. Artificial muscles. Journal Around
the world №6 (2801) | June 2007. URL:
http://www.vokrugsveta.ru/vs/article/3910.
Official web-site of Environmental Robots Inc. 2014.
URL: http://www.environmental-
robots.com/home.html.
Small intestine. 2009. Encyclopaedia Dic.academic.ru.
URL: http://dic.academic.ru/dic.nsf/es/55934/тонкая.
Alexander Kukushkin, Mikhaylov Dmitry, Ekaterina
Ivanova 2012. Recognition of Hemorrhage in the
Images of Wireless Capsule Endoscopy. The 16th
IEEE Mediterranean Electrotechnical Conference
MELECON. b2p-p07-6318 – p 899-902.
Kukushkin Alexander, Mikhaylov Dmitry, Zhukov Igor,
Starikovski Andrey, Konev Vladimir, Tolstaya
Anastasia, Khabibullin Timur 2013. Recognition of
polyps in the images of wireless capsule endoscopy.
International Journal of Emerging Trends &
Technology in Computer Science (IJETTCS), Volume
2, Issue 2. 485-488 p.
Bourbakis, N. 2005. Detecting abnormal patterns in WCE
images. Bioinformatics and Bioengineering. BIBE.
Fifth IEEE Symposium.
Stepanyan D.
А., Fedorov Е.D., Ivanova Е.V. 2011.
Capsule complex for recognition of рН- acidity of
digestive tract. XIV International telecommunication
conference of young scientists and students «Youth
and science». Abstracts. In 3 volumes. V.3. Мoscow:
NRNU MEPhI. – 270 p. P 190-191.
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
84
