
An Integrated Sensing Platform for Remote Fetus Continuous
Monitoring
João Andrade
1
, Artur Arsenio
2
and Andreia Duarte
1
1
Instituto Superior Técnico, Universidade de Lisboa, Porto Salvo, Lisboa, Portugal
2
IST-ID, Universidade da Beira Interior, Covilhã, Portugal
Keywords: Remote Fetus Continuous Monitoring, Wireless Personal Network, Integrated Sensing Platform.
Abstract: Technological developments on health sensing devices, associated with the growing computational
capabilities of mobile devices, enable the creation of solutions that address mobility concerns of patients,
especially those located on remote locations or facing mobility constraints. This paper proposes an
integrated sensing platform, which works transparently with new sensing, portable equipment sensors, but
maintaining as well compatibility with currently deployed commercial tools. This platform targets fetus
health monitoring in pregnant women, presenting a new non-invasive portable alternative system that allows
long-term pregnancy surveillance. Additionally, it can be applied to other users’ communities, such as
remote elderly monitoring at home. We address technology adoption problems related to non-invasive,
portable sensing technologies, data security and equipment heterogeneity.
1 INTRODUCTION
Ubiquitous health sensing technology is becoming a
reality, and it will be part of our lives in the near
future. This trend follows recent technology
advances in sensing, computation, storage, and
communications (Campbell et al., 2008; Lane et al.,
2010) allowing the integration of large scale sensing
with high dataset processing capabilities for
intelligent data analysis (Zhang, Guo, Li, & Yu,
2010). People become the holder of sensing devices,
and both producers and consumers of information
(Miluzzo et al., 2008). As a consequence, the recent
interest by the industry in open programming
platforms and software distribution channels is
accelerating the development of people-centric
sensing applications and systems (Lane et al., 2010;
Miluzzo et al., 2008).
People-centric sensing therefore enables a
different approach to sensing, learning, visualizing
and data sharing. This approach is not only self-
centered, but especially focused on the surrounding
world. Such systems are especially well suited for
Healthcare applications, to facilitate both monitoring
and sharing of automatically gathered health data
(Campbell et al., 2008; Abdelzaher et al., 2007). As
most people possess sensing-enabled phones, the
main obstacle for the widespread adoption of smart
medical devices is not the lack of an infrastructure.
Rather, the technical barriers are related to
performing non-invasive signal acquisition (dealing
eventually with a large set of heterogeneous
equipment), and addressing data privacy and lack of
connectivity issues, whereas supplying users and
communities with useful feedback (Lane et al.,
2010).
This paper addresses these problems, and
presents a solution developed under the scope of a
HMSP collaborative project “Improving Perinatal
Decision-Making: Development of Complexity-
based Dynamical Measures and Novel Acquisition
Systems. The work focus on developing Remote
Fetus Monitoring from biosensors, involving
medical groups at Harvard and Portugal, two sensing
device companies (Omniview Sisporto in Portugal,
and DynaDX in Taywan), and two groups focusing
on applying technologies in biophysics and wireless
communications. This solution can also be applied
for monitoring different user communities, such as
elderly people or physiotherapeutic patients in
recovery (carrying other bio-signal sensors with
them), as addressed by the AHA-Augmented Human
Assistance project.
250
Andrade J., Arsenio A. and Duarte A..
An Integrated Sensing Platform for Remote Fetus Continuous Monitoring.
DOI: 10.5220/0005318302500259
In Proceedings of the International Conference on Biomedical Electronics and Devices (SmartMedDev-2015), pages 250-259
ISBN: 978-989-758-071-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
1.1 Remote Fetus Monitoring
Throughout pregnancy, the placenta is responsible
for supplying the fetus with oxygen and nutrients, as
well as removing carbon dioxide and other waste
gases from the fetal environment. Therefore,
malfunction of the placenta may result in low
oxygen delivery repercussions, in a condition known
as fetal hypoxia. This condition is associated with as
much as 10% of perinatal deaths and 15% of long-
term damage cases, such as cerebral palsy (Graham
et al, 2008).
Electronic fetal monitoring (EFM) may provide
detection of fetal hypoxia on a early stage, thus
enabling medical interventions before irreversible
changes take place, which is why the relevance of
continuous EFM in reducing neonatal mortality and
morbidity has been acknowledged for some years
(Devoe, 2011; Jenkins, 1986; Banta & Thacker,
2001). In fact, nowadays EFM is used as standard
care during pregnancy (Banta & Thacker, 2001) and
labour (Alfirevic et al., 2006) in most developed
countries. Such monitoring has special relevance in
high risk pregnancies, which include maternal
hypertensive disorders and intrauterine growth
restriction (American College of Obstetricians and
Gynecologists, 2009).
Current EFM methods have various
contraindications, which include active genital
Herpes infection, Hepatitis, HIV and lacked
monitoring before 34 weeks of gestation.
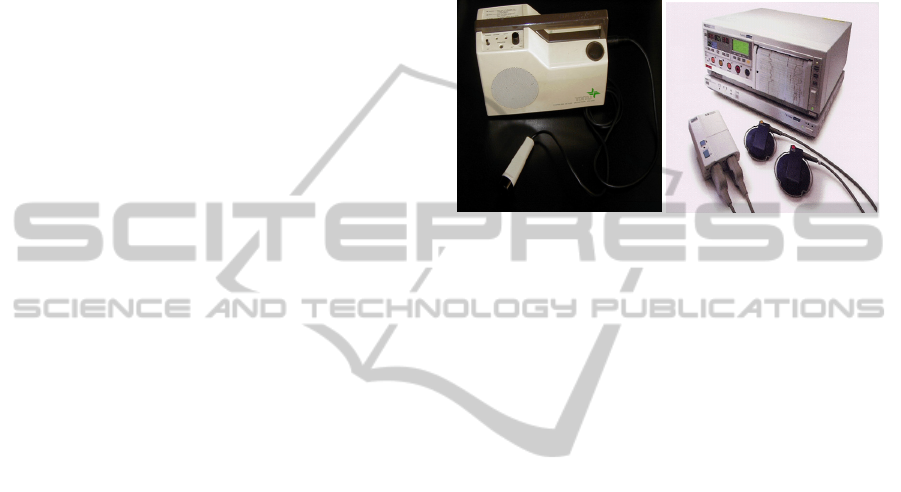
Cardiotocography (CTG, see Figure 1), the most
common EFM method, is associated with highly
complex fetal heart rate (FHR) patterns, making
standardisation difficult (Alfirevic et al., 2006).
Moreover, this method is not suitable for long term
monitoring for a number of reasons, namely: it is
active, restrictive and requires large power (Alfirevic
et al., 2006; Piéri et al., 2001).
On the other hand, the use of transabdominally
recorded electrocardiogram (fECG) carries a number
of advantages: it is passive, uses low-cost electronic
components and standard ECG electrodes. fECG, is
also suitable for long-term ambulatory recording, not
relying on the presence of highly trained
professionals (Crowe, Harrison, & Hayes-Gill, 1995;
Graatsma et al., 2009; Karvounis et al., 2010). Other
benefits include the possibility of extracting beat-to-
beat FHR data, along with averaged fECG
waveforms, which are easier to opine on (Piéri et al.,
2001).
Making fECG a reality will enrich the
knowledge on FHR tracings and improve current
protocols and signal interpretation (Devoe, 2011;
Taylor et al., 2003; Thomas et al., 2008).
Furthermore, computer analysis of fECG is 100%
reproducible and can include parameters difficult to
evaluate visually, something especially important if
we consider reports associating over 50% of
intrapartum deaths with CTG use and interpretation
(CESDI 7
th
Annual Report - CTG Education Survey,
2000).
a) b)
Figure 1: Traditional methods for Fetal heart rate
measurements: auscultation, Doppler ultrasound (a), and
cardiotocography (b).
1.2 Sensing Devices Heterogeneity
The aforementioned heterogeneity found on remote
fetus monitoring poses several challenges,
concerning:
The monitoring device technology
The communication technology, from
traditional cabling systems connecting devices
to printers on hospitals, up to wireless
technology that can transmit signals to the other
side of the planet
The technology for processing the biosignals
Integration of equipment from different vendors
into an integrated platform.
Besides sensing diversity, there is also currently
significant heterogeneity on available wireless
technologies for sensors, from celular comunications
on mobile phones, to WiFi or Bluetooth on mobile
devices, or WiMax.
Under the scope of the HMSP project, our
proposed solution was integrated with current
commercial software: Omniview-SisPorto, which is
employed for monitoring in-loco the patients. This
tool uses a proprietary algorithm for detecting fetus
abnormalities. A new methodoly developed at
Harvard, denoted multi-scale entropy, was also
evaluated. Yet another goal was the upgrade of a
portable ECG device, from DynaDx, to support
wireless, continuous communications (previously,
the device stored 24h of data, to be posteriorly
downloaded at a clinical facility). This portable
AnIntegratedSensingPlatformforRemoteFetusContinuousMonitoring
251

device also uses its own propeietary technology for
the descrimination of the fetus ECG signal from the
mixed pregnant/fetus biosignal.
1.3 Data Security
Respecting users’ privacy is a critical concern for
mobile sensing system (Lane et al., 2010; Zhang et
al., 2010). People are sensitive about how their data
is captured and used, especially if it contains their
location (Lane et al., 2010), speech (Lu et al., 2009),
sensitive images (Lane et al., 2010), or personal
records such as private health information.
Interestingly, social network application’s users may
take privacy as a less relevant concern (Miluzzo et
al., 2008).
Collected data may inadvertently reveal
information about people. For instance, a connection
between mobile sensors and observed parties may be
implicit in their users’ relationships (Abdelzaher et
al., 2007). Revealing personal data can risk privacy
and sharing community gathered data can reveal
information on community behaviours (Zhang et al.,
2010).
Countermeasures such as pausing the collection
of sensor data, are not suitable as they may cause a
noticeable gap in the sensing data stream (Lane et
al., 2010). Revealing too much context can
potentially compromise anonymity and location
privacy. Conversely, the inability to associate data
with its source can lead to the loss of context,
reducing the system’s ability to generate useful
information (Abdelzaher et al., 2007). Some relevant
security concerns for fECG are as follows:
• Privacy: Protection involves different variables,
including identity (who wants data access),
granularity (level of data revealed), and time
(retention time of data) (Zhang et al., 2010).
• Authentication: Deals with validating the user to
the system. The sheer amount of users in mobile
sensing systems might pose impediments to
cryptographic authentication. Nonetheless, there
is the possibility of relying in the redundancy of
sensor data to validate a source anonymously
(Abdelzaher et al., 2007).
• User control: Control over data sharing allows
users to define their participation in the system,
empowering the decision making process
(Zhang et al., 2010). One approach is keeping
sensitive relations from being exposed, either by
local filtering or by providing users with an
interface to review data before it is released
(Abdelzaher et al., 2007). In (Lu et al., 2009),
the user has complete control in how
information is presented in the different system
interfaces.
• Anonymization: Before data release and
processing, different algorithms may be applied
with the objective of not revealing the user
identity (Zhang et al., 2010). In personal
sensing, a solution is processing data locally
(Lane et al., 2010; Lu et al., 2009). In the
context of community sensing, there is the risk
of leaking personal and community information.
A solution is for privacy to be based on group
membership. Sensitive information is only
shared within the groups in which users have
existing trust relationships (Campbell et al.,
2008; Miluzzo et al., 2008).
• Trust: Ensuring both data sources are valid and
that information is accurate should be a system
concern. In addition, correct system usage
should be promoted to prevent abuses. Data
correctness must be verified without violating
privacy (Abdelzaher et al., 2007). In
opportunistic sensing schemes user trust may
become a barrier to wide-scale adoption
(Campbell et al., 2008). These issues may be
addressed by providing sensing device users
with a notion of anonymity through k-
anonymous tasking (Campbell et al., 2008).
Mobile health (mHealth) security has recently
gathered significant attention. New attack and
defense models surged (e.g. unauthorized origin
crossing). Zapata et al. (2014) analyzed with respect
to security issues a total of 24 free mobile personal
health records applications for Android and iOS.
MedApp (Lomotey & Deters, 2014) explores
privacy and security options for the accessibility of
the medical data records in mHealth, enhancing
privacy through the implementation of
authentication policies.
This paper presents a new non-invasive portable
alternative system that allows long-term pregnancy
surveillance. The designed system architecture will
be thoroughly described, as well as the developed
platforms. Connectivity between health sensors and
a healthcare provider over heterogeneous wireless
networks, making use of any available access
network technology, was addressed. In order to
ensure always-on connectivity, our system also
allows the usage of mobile devices (such as a mobile
phone or a tablet) as a bridge between the portable
device and the healthcare provider.
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
252
2 FETUS HEALTH SENSING
A low-cost, ambulatory device will allow fetal
monitoring to be performed at home or in outpatient
clinics during pregnancy (Crowe, Harrison, &
Hayes-Gill, 1995; Graatsma et al., 2009; Karvounis
et al., 2010). In order to provide this kind of
solution, efficient wireless transmission techniques
were investigated to enhance the clinical utility of
the signal processing technology. The portable
monitoring device brings the additional requirement
of internet connectivity, i.e., transmitting FHR
information, and warnings in case of pathological
dynamics detection, from the sensor device to a
healthcare expert at a clinic.
Due to the fetus proximity to the monitoring
device, communications power should be kept to a
minimum for safety reasons (Gandhi et al., 2012).
Information from the recording device will thus be
first relayed through the mobile device employing
low-power wireless technologies for body area
networks like Bluetooth, or through USB cable. The
mobile device therefore acts as an edge gateway,
connecting to the healthcare provider through any of
the available wireless technologies at a specific
location, such as mobile cellular technologies
(supporting various generation mobile technologies),
as well as through WiFi (IEEE 802.11 technology).
In cases where the pregnant woman has internet
connectivity available, our system also supports
direct connection to the internet without bridging
through the mobile device. These capabilities are
currently unmatched by any other fECG sensing
device currently available on the market.
Another challenge to be tackled is energy
consumption, since communications can consume a
significant percentage of a portable device power.
Energy is a scarce resource on these portable devices
and this constraint can directly affect a pregnant
woman’s mobility.
2.1 Use-cases
Current EFM methods still constrain the patient and
thus are not suitable for long-term monitoring. Our
solution allows continuous monitoring of the fetus
throughout pregnancy and antepartum. In fact, using
a low-cost fECG sensing device (appropriately
connected to a mobile phone or a tablet, or directly
to the internet), all the data registered will be
reliably transferred to a remote server.
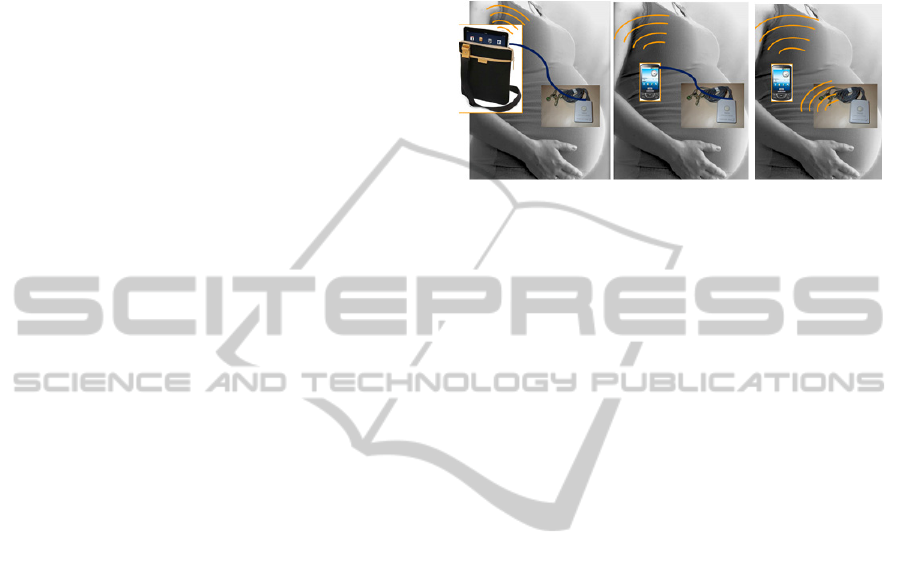
We consider several usage scenarios. Figure 2
presents two of them:
1) USB Tablet/ Mobile Phone: the sensing device
is connected to a tablet or mobile phone using a
USB cable (Figure 2a);
2) Bluetooth Mobile Phone: the sensing device
transmits the data to a mobile phone or a tablet
using Bluetooth technology (Figure 2b).
a) b)
Figure 2: Use-cases including the sensing device and the
mobile device components.
The major advantage of this solution is mobility.
Featuring an always-on connection, the fetal beat-to-
beat data will be available to the health care provider
in quasi-real time, since we have to consider the raw
data must be processed using CPU expensive data
processing algorithms. Furthermore, the mobile
device is provided with an interface that monitors
GPS location of the patient and allows exchange of
alerts between the patient and health care provider.
Both can visualize the data collected by the sensing
device using commercial software Omniview-
SisPorto, or using a new software created under this
project that provides the user an Omniview-like User
Interface on the mobile device.
3 WIRELESS BIOSENSORS
Applications that offer good reliability and user
experience without significantly altering the lifetime
of the sensing devices should be offered (Miluzzo et
al., 2008). Some sensors use a varying amount of
power depending on external factors. Lack of sensor
control limits the management of energy
consumption (Lane et al., 2010).
A real time sensing system should usually supply
sensor data at high rates. However, such an approach
yields high-energy costs. Mobile data upload can
consume a large amount of energy, especially when
the sensing device is far from base stations (Miluzzo
et al., 2008).
The DynaDx device was used to acquire the fetus
ECG. Initially the data was stored in the device’s
internal memory. After the acquisition period ended,
it was then possible to extract this information at a
medical provider. This approach is common in other
AnIntegratedSensingPlatformforRemoteFetusContinuousMonitoring
253

Figure 4: System Components.
marketplace solutions.
To overcome this limitation, the device in this
project was integrated in a first version with a
wireless communication capable Bluetooth Arduino
pro-mini module, allowing the wireless transmission
of stored signals to a mobile phone or a server on a
delivery room. The Arduino program was
responsible for reading data from the sensor and
sending it, as well as for receiving reading
commands and trigger the start of sensor readings.
A second version of the device was created
afterwards enabling the realtime communication of
these signals (see Figure 3). The integration
consisted in connecting the DynaDx device to a
MAX232 circuit board, which converted the RS232
signal to a Transistor-Transistor Logic (TTL) signal.
This board was connected to an Arduino processing
unit, which communicates through a Bluetooth
shield, enabling the device to receive and transmit.
The system is compact, portable, and solely requires
an additional AAA battery, summing to a total of
two AAA batteries per device. All the electronics
fits within the original sensor case.
Figure 3: The upgraded DynaDX ECG sensing device for
continuous, wireless transmission.
Hence, a system for wirelessly acquiring fECG
signals was developed, as shown in Figure 4. In this
system a sensing device carried by a pregnant
woman acquires fetus biosignal data in real-time and
transmits it to a custom hardware module. This
module is capable of offloading data through a
Bluetooth communication interface. Possible
receivers are any such devices that can communicate
in the aforementioned communication protocol. In
the developed system these devices can either be a
mobile device running an Android application or a
machine running the Omniview-SisPorto software
client. The mobile device is also capable of
communicating the acquired data wirelessly in an
opportunistic fashion to a back-end middleware
(also developed under this project), in order to save
energy and to retransmit data after lacking
connectivity.
4 ARCHITECTURE
The architecture for remote fetus health monitoring
comprises two main set of devices (see Figure 5):
sensing modules and handheld devices, which can
be mobile phones or tablets. The mobile device
collects sensor data, being responsible for permanent
updates to a centralized hospital system. The
webserver receives and stores the raw data,
processes it and makes it available for both the
patient and health care provider sites, offering user
interfaces to properly display the data. Furthermore,
users (patients and health professionals) can also use
the web interface at any given time to visualize the
data, with no location restrictions.
This monitoring solution aims to target a large
number of pregnant women, which is feasible given
the conditions it offers, namely: low cost sensing
device, handheld device and cellular technologies
common in developed countries, low restrictions in
mobility of the pregnant women associated with the
sensing device. Furthermore, a network comprising
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
254
pregnant women, physicians and other health care
providers can be established on the solution social
web application. All the gathered information is
securely integrated and made available between
strictly defined subjects.
Figure 5: System Architecture.
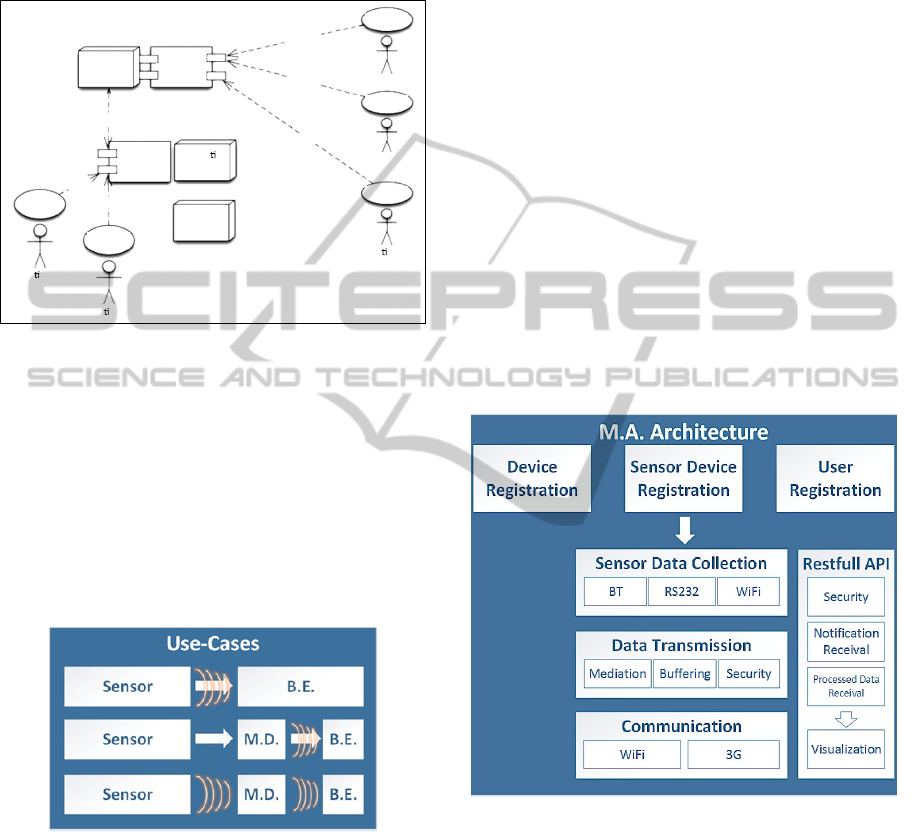
Considering the two aforementioned use-cases,
as well as the customized monitoring system
developed, different methods of communication can
be considered (Figure 6). Either the sensor is directly
connected to the back-end (BE) platform, or it
communicates with the monitoring device (MD),
which then communicates with the BE.
Communications are established by USB (the arrows
in Figure 6) or wirelessly, by WiFi or Bluetooth
technologies.
Figure 6: Communication scenarios’ use-cases.
4.1 Mobile Application Architecture
A mobile application (MA) was designed complying
with the system requirements (see Figure 7). The
first step in using the system is registration. From
the end-user point of view, only the unique pair
username-password (login data) is relevant.
However transparent to the user, there are two
additional authentication levels, related to the
handheld device in use and the communication
protocol with the backend (BE) platform.
Each handheld device (either a tablet or a mobile
phone) has an unique identity, which is recognized
by systems and allows improved security: only
registered devices are able to exchange information
with the BE platform. Upon enrolling in trial with
this platform, the user is provided with a pair
username-password and associated with the
handheld device identity in the BE. The personal
data included also refers name, age, gestation time
and associated doctor, together with relevant
characteristics to the health care provider.
The second level of authentication is transparent
to the user and is renewed each time the application
is started. The first interaction between the end-user
and the MA is authentication using the login data.
This pair is tested using a webservice and, in case of
success, returns a cookie to be used throughout the
session, i.e., until the program is closed and login
verification is required again. This cookie is
associated with each webservice based request used
in the application, to ensure the identification of the
request source by the BE.
Figure 7: Main application architecture.
The next step is the selection of the monitoring
device. With this goal in mind, the mobile
application was built in a modular manner, so that
sensing devices can be exchanged. In fact, the
temporary databases associate a parameter ”type”
with the data, which makes it easier to increment the
available options. The possibilities are nearly
endless. For instance, if the new version of the
current sensing device includes uterine contractions
measurement, the upgrade for this new feature will
be trivial. On the other hand, the connection type
Computer
Computer
Computer
Web
Interface
Web
Server
WebService
Interface
Tablet
Cellphone
Pa ent
Pa ent
Pa ent
Applica on
Server
Database
Server
<uses>
<uses>
<uses>
<uses>
<uses>
<uses>
Doctor
Healthcar
e
Provider
AnIntegratedSensingPlatformforRemoteFetusContinuousMonitoring
255

between the sensing and the mobile devices can be
extended as well, with limitations that can only
include available hardware. For options besides
RS232 and Bluetooth, exposure security cautions
must be of course kept in mind (Gandhi et al., 2012).
Upon authentication, the device connection starts
several actions besides opening the main menu. To
simplify the user experience, all the collecting and
uploading of data is transparent to the user, which
means the user only has to start the connection to the
device by clicking an option and the entire data
gathering and upload processes are done in
background services. The GPS monitoring is
independent of the sensing device, since it is only
based on the handheld device, and is transparent to
the user as well. All the data exchanged between the
mobile application and the webserver is encrypted
using a security certificate created for this system, to
ensure the privacy of all the participants.
The data collected from the sensing device and
internal mobile phone GPS is temporarily saved in
local databases. This method ensures that no
information is lost. The MA is built to choose a
WiFi connection if present, but use 3G if the first is
not available. If there is no internet connection in
any given moment, the data is buffered on the
mobile application until a connection is available
and uploads are re-established.
Besides security, the Restful API has two
additional modules: notification and processed data
reception, which in turn allow for data visualization.
Notification reception refers to the exchange of
private messages between the associated members of
the network, for instance patient and physician.
Whenever a new message is received, the mobile
application generates a user alert, which remains
visible until the message is read. This feature is
relevant namely for recommendations from the
physician or health care provider, as well as doubts
from the patient.
Also concerning the Restful API is the
visualization of data plots. This is relevant for
evaluating the patient’s condition at any given time.
If the user is a physician or health care provider, one
can choose the desired patient and data. There are
relevant options included before visualizing the data
plot, namely type of data and time span wanted. By
default, current time is selected, which results in
quasi-real time monitoring. Acknowledging the
mobile application uploads raw data, which is then
processed by the webserver and sent back to the
MA, then a delay of some seconds is expected and is
tolerable by physicians. Current CTG methods carry
a delay of some seconds as well.
In order to perform the assigned tasks, a MA was
developed for Android mobile devices, including
both tablets and mobile phones. Keeping in mind
always-on monitoring and user friendliness, some
user options were agreed upfront to be present in the
main menu. The end-user might be a patient or a
healthcare provider, and the menu will present
accordingly. The first snapshot in Figure 8 shows the
main options for a patient verifying device and
internet connectivity, visualizing plotted data, using
the web interface to access a restricted social
network, exchanging alerts and updated user
information. The other snapshot shows the options
menu for configuring the visualization of the plotted
data.
Figure 8: Snapshots of Android Mobile Application
Graphical User Interface (GUI).
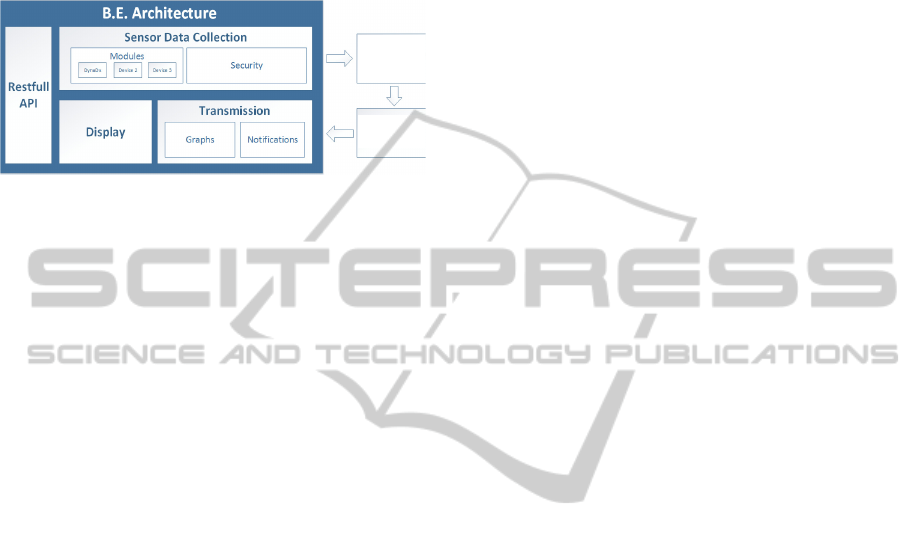
4.2 Backend Architecture
The backend architecture (as shown in Figure 9) is
constituted by the following modules: ”Sensor Data
Collection”, the ”Transmission”, ”Display” and
RESTful API.
The ”Sensor Data Collection” module is
responsible for acquiring system input. It supports
different input sources, such as the DynaDx device.
The communication of this input is performed with
information security concerns: the confidentially of
the transmitted data, supported by users
authentication; the integrity of the backend data,
made possible by the underlying authorisation
system that assigns a profile to a given user upon
registration. It is also assured the mutual
authentication of the backend and its users.
The ”Transmission” module accounts for the
communication of processed data (graphs and
notifications) to the system’s client (the MA).
Notifications result from the complexity analysis of
the pre-processed acquired signal that is performed
by Omniview-SisPorto using MultiScale Entropy
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
256
(MSE) technology developed by Harvard team.
Graphs are built for the visualization of the time
series that results from the acquisition of the pre-
processed sensed signal. Both these data types can
be requested by a mobile device through the
RESTful API.
Figure 9: Backend architecture.
The ”Display” module is capable the different
types of data that compose the system (namely the
sensed signal graphs and associated notifications).
The web application framework ”Lift” is used to
display this information. More specifically, Lift’s
Flot plugin is responsbile for displaying the graphs.
The ”RESTful API” module establishes a
uniform communication interface for the system.
Communication is achieved through the use of a
RESTful webservice-based interface. A webservice
based approach tackles issues of system universality,
as it allows different types of devices to access the
system, providing flexibility in terms of
programming languages (Kansal, Goraczko & Zhao,
2007). This module defines a standard system API
that is composed by a set of services that are made
available.
The exposed services are as follows:
1) Authentication (Login; Logout);
2) Notification (Subscribe; Unsubscribe; Submit
notification);
3) Plotting (Access data plot);
4) Signal Processing (Request signal pre-
processing, Request data loading from the
filesystem; Request data offloading to the
filesystem);
5) Domain (Access all data entries for a given
data domain entity; Access a specific data
entry for a domain entity; Access filtered data
properties for a given domain entity; Access
filtered data properties for a domain entity).
Each of the API’s features is bound to a specific
set of one or more HTTP methods. The system is
flexible regarding data inputs, i.e. both JSON
(Javascript Object Notation) and XML are
supported. Furthermore, all CRUD (Create, Read,
Update, Delete) functions support data that can be
specified in either scalar or vector formats. For
instance, it is possible for the client to update either
one device or a set of them in the same request. It is
also highly extensible, i.e. when a required data type
is defined the system’s standard domain RESTful
API is immediately made available.
Through this interface mobile clients can offload
different kinds of data, such as historical traces of
raw sensory data, the output of signal processing at
the back-end, or notifications (see Fig. 10). Data is
communicated asynchronously and must have an
acquisition timestamp assigned by the client. In this
approach, a publishing client on the sensing devices
phone collects samples and uploads them using the
web service interface, after applying data filters and
according to network availability.
A client (a patient, a doctor, a healthcare
provider, a sensor, or a mobile device) must be
authenticated in the system for information to be
sent to the backend, so prior registration is required.
5 CONCLUSIONS
An integrated sensing platform was presented. This
solution aims at improving the current pregnancy
surveillance paradigm, while taking advantage of the
recent technologies developments in both mobile
devices and communication infrastructures. Mobile
device and Web technologies were integrated into
this paradigm, constituting a flexible modular
platform that could be customised to the application
domain’s requirements.
The development of this solution had to address
several challenges, since both DynaDX sensor and
SisPorto OmniView had already its own
communication technologies implemented, and
upgrading to a wireless protocol had an impact on
these tools workflows.
ACKNOWLEDGEMENTS
Part of this work was supported by Harvard Medical
School Portugal Collaborative Research Award
HMSP-CT/SAU-ICT/0064/2009: Improving
perinatal decision-making: development of
complexity-based dynamical measures and novel
acquisition systems. The second author has also
been partially funded by CMU-Portuguese program
through Fundação para Ciência e Tecnologia, AHA-
Augmented Human Assistance project, AHA,
CMUP-ERI/HCI/0046/2013.
Omniview
Sisporto
Pre‐process
data
to
extract
fetal
signal
AnIntegratedSensingPlatformforRemoteFetusContinuousMonitoring
257
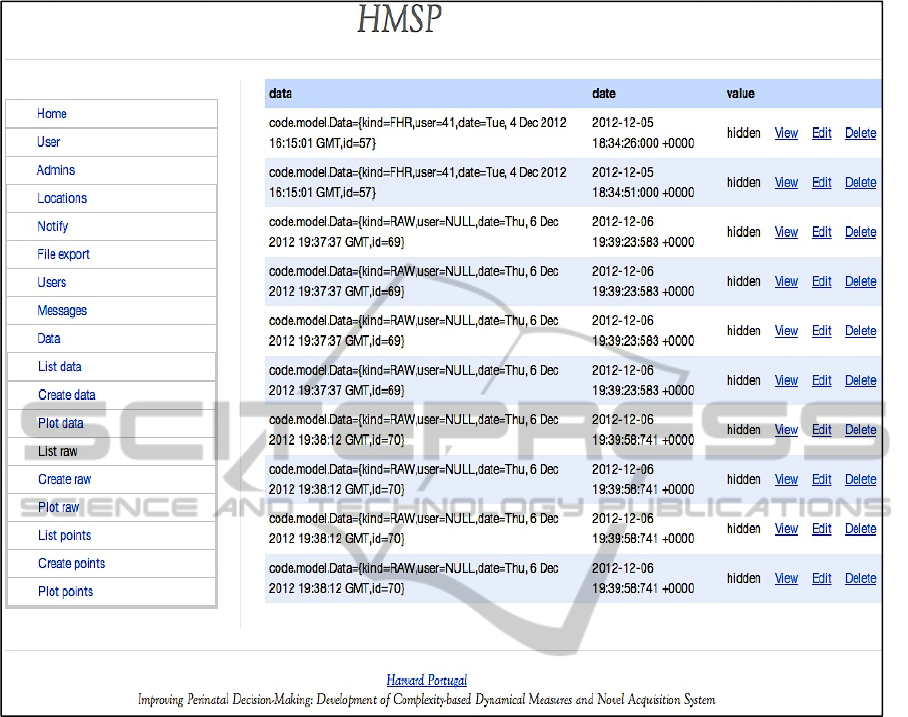
Figure 10: Snapshot of web interface for the backend platform and applications.
REFERENCES
Abdelzaher, T., Anokwa, Y., Boda, P., Burke, J., Estrin,
D., Guibas, L., Kansal, A., et al. (2007). Mobiscopes
for Human Spaces. IEEE Pervasive Computing, 6(2),
20–29. doi:10.1109/MPRV.2007.38.
Alfirevic, Z., Devane, D., & Gyte, G. M. L. (2006).
Continuous cardiotocography (CTG) as a form of
electronic fetal monitoring (EFM) for fetal assessment
during labour. Cochrane database of systematic
reviews (Online), (3), CD006066.
American College of Obstetricians and Gynecologists.
(2009). ACOG Practice Bulletin No. 106: Intrapartum
fetal heart rate monitoring: nomenclature,
interpretation, and general management principles.
Obstetrics and gynecology, 114(1), 192–202.
doi:10.1097/AOG.0b013e3181aef106.
Banta, D. H., & Thacker, S. B. (2001). Historical
controversy in health technology assessment: the case
of electronic fetal monitoring. Obstetrical &
gynecological survey, 56(11), 707–19.
Campbell, A. T., Eisenman, S. B., Lane, N. D., Miluzzo,
E., Peterson, R. A., Lu, H. L. H., Zheng, X. Z. X., et
al. (2008) The Rise of People-Centric Sensing. , 12
IEEE Internet Computing 12–21. IEEE Computer
Society. doi:10.1109/MIC.2008.90.
CESDI 7
th
Annual Report - CTG Education Survey
(2000). Maternal and Child Health Research
Consortium, London, Tech. Report.
Crowe, J. A., Harrison, A., & Hayes-Gill, B. R. (1995).
The feasibility of long-term fetal heart rate monitoring
in the home environment using maternal abdominal
electrodes. Physiological measurement, 16(3), 195–
202.
Devoe, L. D. (2011). Electronic fetal monitoring: does it
really lead to better outcomes? American journal of
obstetrics and gynecology, 204(6), 455–6.
doi:10.1016/j.ajog.2011.04.023.
Gandhi, O. P., Morgan, L. L., De Salles, A. A., Han, Y.-
Y., Herberman, R. B., & Davis, D. L. (2012).
Exposure limits: the underestimation of absorbed cell
phone radiation, especially in children.
BIODEVICES2015-InternationalConferenceonBiomedicalElectronicsandDevices
258

Electromagnetic biology and medicine, 31(1), 34–51.
doi:10.3109/15368378.2011.622827.
Graatsma, E. M., Jacod, B. C., Van Egmond, L. A. J.,
Mulder, E. J. H., & Visser, G. H. A. (2009). Fetal
electrocardiography: feasibility of long-term fetal
heart rate recordings. BJOG : an international journal
of obstetrics and gynaecology, 116(2), 334–7;
discussion 337–8.
Graham, E. M., Ruis, K., Hartman, A. L., Northington, F.
J., & Fox H. E. (2008) “A systematic review of the
role of intrapartum hypoxiaischemia in the causation
of neonatal encephalopathy.” American journal of
obstetrics and gynecology, vol. 199, no. 6, pp. 587–95.
Jenkins, H. (1986). Technical progress in fetal
electrocardiography - a review. Journal of Perinatal
Medicine, 14, 365–377.
Kansal, A., Goraczko, M., & Zhao, F. (2007). Building a
sensor network of mobile phones. Proceedings of the
6
th
international conference on Information processing
in sensor networks. doi:10.1145/1236360.1236433.
Karvounis, E. C., Tsipouras, M. G., Papaloukas, C.,
Tsalikakis, D. G., Naka, K. K., & Fotiadis, D. I.
(2010). A non-invasive methodology for fetal
monitoring during pregnancy. Methods of information
in medicine, 49(3), 238–53. doi:10.3414/ME09-01-
0041.
Lane, N. D., Miluzzo, E., Lu, H. L. H., Peebles, D.,
Choudhury, T., & Campbell, A. T. A survey of mobile
phone sensing. IEEE Communications Magazine 140–
150 (2010).
Lomotey, R. & Deters, R. (2014). Mobile-Based Medical
Data Accessibility in mHealth. 2
nd
IEEE Int.
Conference on Mobile Cloud Computing, Services,
and Engineering (MobileCloud), April, 91-100.
Lu, H., Pan, W., Lane, N. D., Choudhury, T., & Campbell,
A. T. (2009). SoundSense : Scalable Sound Sensing
for People-Centric Applications on Mobile Phones.
Architecture, 165–178.
Miluzzo, E., Lane, N. D., Fodor, K., Peterson, R., Lu, H.,
Musolesi, M., Eisenman, S. B., et al. (2008). Sensing
Meets Mobile Social Networks : The Design ,
Implementation and Evaluation of the CenceMe
Application. Architectural Design, 10, 337–350.
doi:10.1145/1460412.1460445.
Piéri, J. F., Crowe, J. A., Hayes-Gill, B. R., Spencer, C. J.,
Bhogal, K., & James, D. K. (2001). Compact long-
term recorder for the transabdominal foetal and
maternal electrocardiogram. Medical & biological
engineering & computing, 39(1), 118–25.
Taylor, M. J. O., Smith, M. J., Thomas, M., Green, A. R.,
Cheng, F., Oseku-Afful, S., Wee, L. Y., et al. (2003).
Non-invasive fetal electrocardiography in singleton
and multiple pregnancies. BJOG : an international
journal of obstetrics and gynaecology, 110(7), 668–
78.
Thomas, M. J., Cleal, J. K., Hanson, M. A., Green, L. R.,
& Gardiner, H. M. (2008). Non-invasive fetal
electrocardiography: Validation and interpretation. 4
th
IET International Conference on Advances in Medical,
Signal and Information Processing MEDSIP, 1–4.
Zapata, B., Hernandez Ninirola, A., Fernandez-Aleman, J.
& Toval, A. (2014). Assessing the privacy policies in
mobile personal health records. 36
th
Annual Int.
Conference of the IEEE Engineering in Medicine and
Biology Society (EMBC), Aug, 4956 – 4959.
Zhang, D., Guo, B., Li, B., & Yu, Z. (2010). Extracting
Social and Community Intelligence from Digital
Footprints: An Emerging Research Area. Ubiquitous
Intelligence and Computing, Vol. 6406, 4–18.
Springer-Verlag Berlin.
AnIntegratedSensingPlatformforRemoteFetusContinuousMonitoring
259
