
Dilemma of Tobacco’s Policy in Indonesia: Increasing Country’s
Income or Increasing the Country’s Poverty with National Health
Insurance’s Deficit?
Luh Mery Wedayanthi
Faculty of Public Health, Universitas Airlangga, Mulyorejo, Surabaya, Indonesia
mery.wedayanthi@gmail.com
Keywords: Tobacco’s policy, Country’s income, National Health Insurance’s deficit.
Abstract: Tobacco is still an issue in politics, economy and healthy in Indonesia. Indonesia gets attention about its
tobacco’s policy, because Indonesia has not been doing the FCTC’s ratification steps. It’s because Indonesia
still has dilemmas associated with its tobacco’s policy. Cigarette tax can increase the country’s income, but
cigarettes can cause catastrophic illnesses that generate a high absorption of the national health insurance’s
funds. The objective of this study is to describe the tobacco policies in Indonesia from the perspective of the
economy and health in order to provide recommendations. The method of this research is a literature study
with analysis about the topic from previous research studies, journals and other policies in Indonesia. The
result of the research indicated that 95% of Indonesia’s tax income is from cigarette tax. But, in 2015, about
23.90% of the national health insurance fund is for the treatment of catastrophic illnesses associated with
smoking, and this condition can cause the fund to become deficit in the future. The conclusion of this study,
there needs to be an accurate review to resolve the tobacco policy dilemmas in order to avoid the deficit of
BPJS.
1 INTRODUCTION
Cigarette problems are endless to discuss. The issue
of cigarettes is one of the delicate problems faced by
Indonesia. Related to the dangers caused by
cigarettes, WHO published an international
agreement upheld by the parties involved called the
FCTC (Framework Convention of Tobacco
Control). Indonesia is one of the countries that
played an active role in the formulation of FCTC as
a drafting committee. The FCTC has been ratified by
177 governments from 192 countries that are
members of the WHO. Indonesia which was active
in the formulation of FCTC has proven to be the
only country in the Asia Pasific region that has not
ratified this convention (Ahsan, 2013).
Indonesia is still hesitant about ratifying the
FCTC because Indonesia still having dilemmas with
its tobacco policy. On one side, Indonesia relies
heavily on tobacco taxes as a large percentage of the
income for its country. If Indonesia ratifies the
FCTC, people are worried that it could cause
economic upheaval. On the other side of the coin, it
cannot be denied that cigarettes are one of the main
causes of catastrophic diseases that can disturb the
health of society. The health problem due to
smoking behaviour such as lung cancer, heart
disease, chronic kidney failure, stroke, and etc.
2014 was the first year of Indonesia's movement
to start moving forward with the JKN (National
Health Insurance) program to realise and implement
universal health coverage. JKN is commonly
referred to as BPJS, which is the organiser. JKN is
an effort to be able to handle health problems with a
system of working together, where one sick person
is helped by many people. In fact, from year to year,
BPJS’s spending continues to increase beyond its
accepted means. Projections up to 2019 say that the
deficit will continue to occur. One of the reasons for
this is because of the many costs incurred by BPJS
when dealing with patients with catastrophic
diseases, with one of the primary causes being the
consumption of cigarettes (Pardede, 2016).
Wedayanthi, L.
Dilemma of Tobacco’s Policy in Indonesia: Increasing Country’s Income or Increasing the Country’s Poverty with National Health Insurance’s Deficit?.
In Proceedings of the 4th Annual Meeting of the Indonesian Health Economics Association (INAHEA 2017), pages 105-109
ISBN: 978-989-758-335-3
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
105
2 METHODS
The type of data in this study was secondary data
that was obtained through studying the literature. A
literature study is a type of research conducted by
finding references or theories relevant with the case
or problems associated with the study theme or
question that is to be answered. References can be
obtained through books, journals, articles on littering
reports, and internet sites (Kuntjojo, 2009). In
relation to the problem of tobacco policies in
Indonesia, the literature collected relates to the
tobacco policy advantages to do with the cigarette
excise duty in order to see the current Indonesian
tobacco position in relation to production or import
export activities. It will also be in order to see the
negative impact in the health sector, like BPJS, who
have experienced a big deficit caused by them cover
the charges of catastrophic diseases, where one of
the causes is by cigarettes. The literature in this
study is relevant because it’s explain enough about
the condition about tobacco and tobacco’s policy in
Indonesia. In other side, the literature also explain
about the data of BPJS’s financing absorption in
catastrophic disease.
The data analysis that was used in this research
study was the quantitative descriptive analysis
method. This study aims to describe the problems
that occurred, as well as describing the responses or
perceptions of the people about the issues raised.
3 RESULTS
Indonesia is one of big country that provide tobacco
for its own country or for other countries.
Temanggung, Jember, Deli, Madura, and Lombok
are the biggest region that provide tobacco in
Indonesia. In the table 1, there are the data about
tobacco production in Indonesia in 2015-2017.
Table 1: Tobacco Production in Indonesia 2015-2017
Year Production (Ton)
Smallholde
r
Government Private Total
2015 192.899 577 314 193.790
2016** 195.559 462 133 196.154
2017* 197.497 660 139 198.296
Source: Indonesian Plantation Statistics for Tobacco 2015-
2017
Information:
1.Preliminary figures *
2. Estimation Rate **
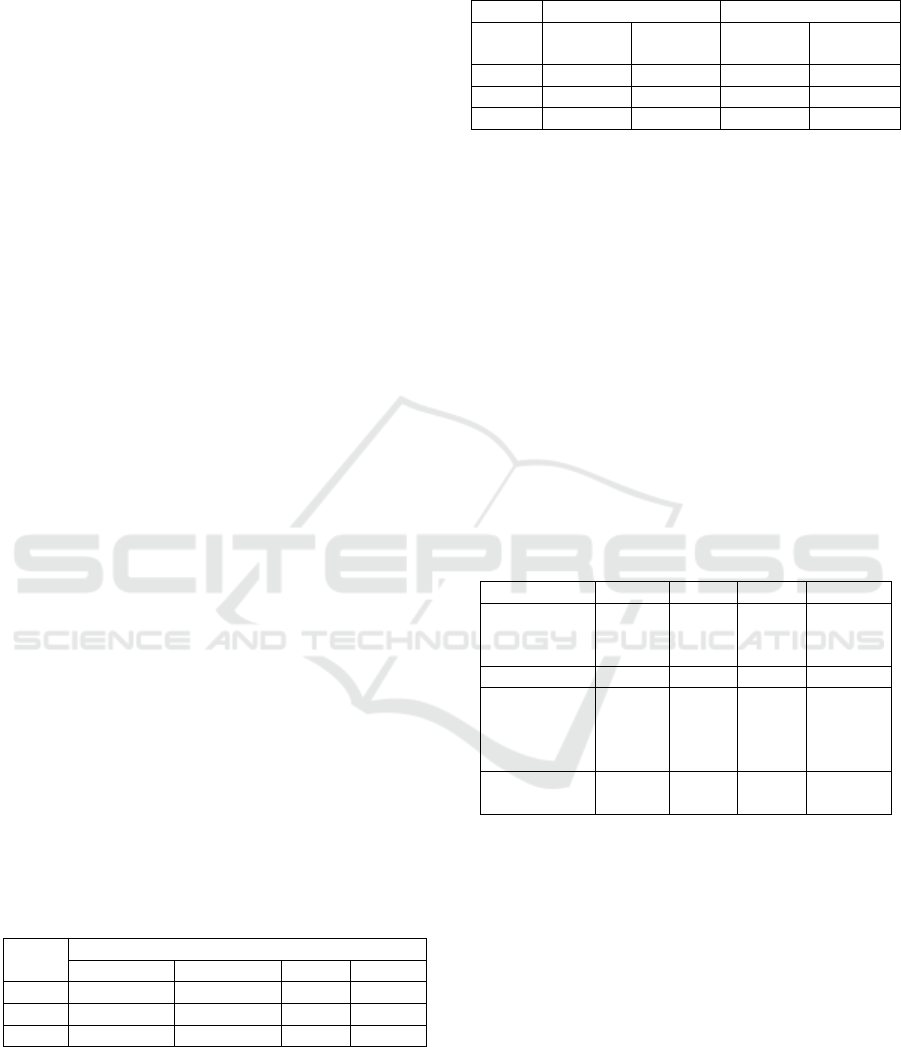
Table 2: Indonesian Tobacco Import- Export in 2014-
2016
4
Yea
r
Ex
p
ort Im
p
ort
Volume
(ton)
Value
(USD)
Volume
(ton)
Value (
USD)
2014 35.009 181.323 95.732 569.776
2015 30.675 156.784 75.353 412.328
2016 21.933 95.236 52.482 328.585
Source: Central Bureau of Statistics
Based on data from the Central Bureau of
Statistics, there has been a downward trend related
to tobacco import and exports from year to year. In
the relation to the ‘agree’ and ‘disagree’ points of
view about tobacco regulation policy in Indonesia,
tobacco farming includes export and import values
that can often be the reason for the disagree side.
The data shows that, for the ingredients of processed
tobacco products in Indonesia, there is more use of
tobacco imports, while the number of exported
tobacco is much smaller.
Indonesia has own regulation about tobacco’s
policy. The policy is about the excise tax of tobacco,
the cigarette tax, and the excise tariff. In the table 3,
there is tobacco excise policy in 2014-2017.
Table 3: Tobacco Excise Policy 2014-2017
Yea
r
2014 2015 2016 2017
Increase in
excise tax
rates
0% 8,7% 11,3% 10,5
Ci
g
arette tax 10% 10% 10% 10%
Total
increase in
excise duty
+ cigarettes
10% 9,6% 12,5% 11,55%
Average
excise tariff
51,4% 48,2% 44,4% 49,1%
Source: Fiscal Policy Office, Ministry of Finance
In 2014, there was a 10% increase in the tax
burden due to the introduction of the cigarette tax -
10% of the excise tax. Thus, the greater the excise
tax, the more it will obtain a greater tax income from
cigarettes too. Based on the table above, there is an
upward trend associated with the average revenue
excise tax per year, so it is not appropriate if it is
said that the excise tax depends on the production of
tobacco. Tobacco production in Indonesia has
always increased as the data indicates in Table 1.
Table 3 show, there was 10% increasing in
excise tax from 2014 to 2017. The increasing of
excise tax make some effect. There is some
INAHEA 2017 - 4th Annual Meeting of the Indonesian Health Economics Association
106
research’s result about the impact of 10% tax rate on
consumption and acceptance of excise duty.
Table 4: Impact of 10% Excise Tax Rate on Consumption
and Acceptance of Excise Duty
5
Study % Decrease in
Consumption
% Increase in
Excise Duty
De Beyer dan
Yurekli, 2000
2,0 8,0
Djutaharta et
al, 2005
0,9 9,0
Adioetomo et
al, 2005
3,0 6,7
Sunley,
Yurekli,
Chaloupka,
2000
2,4 7,4
Source: Fiscal Policy Office, Ministry of Finance
Table 4 shows that an increase in the excise tax
can reduce cigarette consumption by about 0.9% -
2.4%, and increase tax revenue by about 6.7-9.0%.
This means that the increase in excise tax can
increase tax revenues and reduce cigarette
consumption.
As we know, tobacco’s policy in Indonesia is
still dilemma. One side, from the policy Indonesia
can take advantage from the tax to develop the
country. But in other side if we depend on tobacco’s
tax, that can increase the catastrophic disease and
absorb a lot of fund of BPJS.
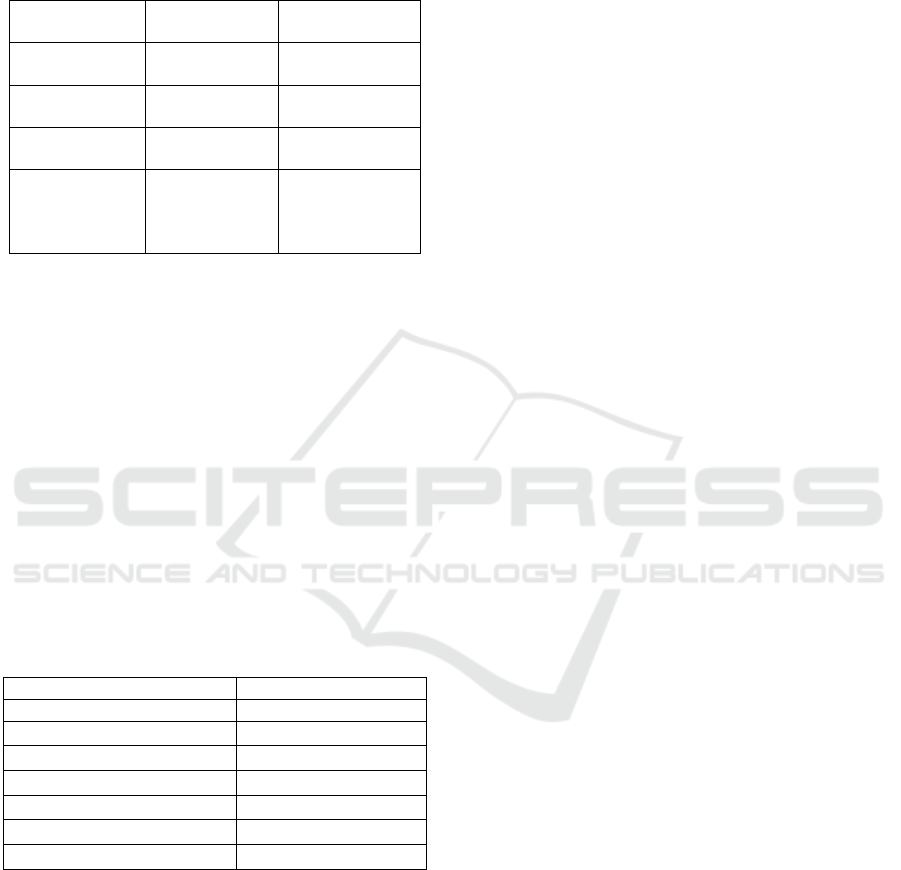
Table 5: Percentage of Health Service Financing with
BPJS related to Catastrophic Disease for about 23.90% in
2015
Disease Health Care Costs
(
%
)
Heart disease 13%
Chronic Kidney Failure 7%
Cancer 4%
Stroke 2%
Thalassemia 0,7%
Haemophilia 0,2%
Leukemia 0,3%
Source: Indonesia National Health Insurance
An expenditure of 23.90% out of BPJS’s fund in
2015 was used to finance health services associated
with catastrophic diseases, of which one primary
cause is due to cigarette consumption. About 1.3
million or 0.8 recipients of national health insurance
received catastrophic services and the most
predominant was chronic renal failure.
4 DISCUSSION
Indonesia is one of the many countries that
producing tobacco. The production of tobacco from
2015-2017 has continued to increase (Kementrian
Pertanian, 2016). The product resulting from
tobacco farming has become an important aspect for
the disagree team, in order for Indonesia to ratify the
FCTC. The side has said that Indonesia is a large
tobacco producing country and that it can disturb
Indonesian agriculture if Indonesia ratifies the
FCTC. In fact, the increase of tobacco production in
Indonesia apparently has not been able to meet the
needs of tobacco in the country. It can be seen in
Table 2 that the value of Indonesian imports of
tobacco is much higher than the value of Indonesian
tobacco exported to other countries (Kementrian
Pertanian, 2016).
Additionally, Indonesia relies heavily on tobacco
excise tax as the main revenue of the State through
excise duty. 95% of excise revenues comes from
tobacco taxes,
6
and it is expected that by 2017, it
will make up 98.7% of the excise revenue out of the
target of APBN (State Budget and Expenditure of
State) in 2016
7
. The way to achieve the target set out
is to increase the excise tax by as much as 10%
7
.
Based on several studies conducted in accordance
with Table 4, it has been stated that a 10% increase
in excise tax can reduce cigarette consumption and
also increase tax revenue
(Directorate General of
Customs and Excise Ministry of Finance Republic of
Indonesia, 2016).
The policy of increasing tobacco excise tax needs
to be viewed wisely from all of the different sides.
Indonesia should not only be driven by revenue in
relation to the tobacco excise duty. According to the
regulation of the Finance Minister (Peraturan
Menteri Keuangan Republik Indonesia Nomor 40
tahun 2016), it was mentioned that the state revenue
on excisable goods includes tobacco excise taxes,
the excise of ethyl alcohol, the excise of ethyl
alcoholic beverages, the fine from excise
administration, other excise income, cigarette tax
and non-tax state revenue (Ministry of Finance
Republic of Indonesian, 2016). Goods subject to
excise are goods that have characteristics such as
their consumption needing to be controlled, their
circulation monitored, having a negative impact, or
their use needs to have imposed on them state levies
for the sake of justice and equilibrium
(Indonesian
Government, 2007). There are many other items
whose use needs to be controlled, such as plastic-
based goods. Indonesia should increase state revenue
through excise with more varied goods. Indonesia is
Dilemma of Tobacco’s Policy in Indonesia: Increasing Country’s Income or Increasing the Country’s Poverty with National Health
Insurance’s Deficit?
107

far behind other countries that have the political will
to impose excise duty on plastic-based goods as a
source of acceptance as well as an effort to control
in order to protect citizens and their respective
countries from negative impacts (Directorate
General of Customs and Excise Ministry of Finance
Republic of Indonesia, 2016).
Cigarettes are small bars that contain substances
that can cause addiction, dependence and even
death. In cigarettes, there are approximately 4000
types of chemicals that can endanger human health.
The diseases caused by smoking are catastrophic
such as cancer, heart disease, kidney failure, and
others. The health impact of tobacco and tobacco
products in the form of cigarettes has been
anticipated with the use of the excise itself. Based on
article 31 of the constitution (UU No. 28 tahun
2009) about district tax and district retribution, the
tax revenue of cigarettes, both in provincial and
district / city sections, is allocated at least 50% (fifty
percent) to fund public health services and law
enforcement by authorised personnel
(Indonesian
Government, 2009). The use of cigarette taxes in the
health sector is among others, for: procurement and
for the maintenance of facilities and infrastructure of
the health care units, the provision of adequate
public facilities for smoker activities (smoking area),
and to popularise the dangers of smoking, and to
generate public service ads about the dangers of
smoking
(Indonesian Government, 2009).
The regulation does not mention the negative
impacts caused by cigarettes, such as medical
expenses for smokers or for the people exposed by
smoke. The treatment of diseases caused by
cigarettes costs a lot of money. Indonesia is
currently in the process of realising universal health
coverage with national health insurance that has
been implemented since 2014. As we knew, BPJS
spending is much more than its revenue. One reason
for this is because 23.90% of BPJS spending is used
to finance the treatment of patients with catastrophic
disease
(Pardede, 2016). It is the reason why deficit
and BPJS has become a big issue in relation to
public health.
Based on article 25 of President Regulation
(Peraturan Presiden No. 111 tahun 2013) about
health insurance, there are several health services
not covered by BPJS, such as health problems due to
deliberate self-harm, and/or the consequences of
self-harmful hobbies. Future discourse to do with
BPJS will include the consumption of cigarettes as
one cause of health problems - a hobby that can
endanger the individual, so the disease and
subsequent cost caused by cigarettes is not borne by
BPJS. It is a discourse that should receive attention
and careful study because the financing of cigarette
disease treatment has swallowed much of the BPJS
budget. For example, in 2015, there were 1,211
cases of cirrhosis renal diseases costing Rp 1,613
billion, 757 cases of cancer costing about of Rp
1,413 billion, and 468 cases of stroke with a Rp 687
billion cost
(Hafizd, 2016). This is only three out of
the many diseases caused by cigarettes. From that,
we can also imagine how much cost has been
incurred, so it is no wonder that the treatment of
diseases caused by smoking causes the budget of
BPJS to become a deficit. In addition, Indonesia also
needs to pursue a health insurance policy
implemented in Thailand that emphasises additional
financing for high-cost diseases that could prevent
budget deficits
(Jongudomsuk et al, 2015).
5 CONCLUSIONS
There is a dilemma to do with the tobacco policy in
Indonesia; one side is favourable because of the high
taxes and help towards the state revenue, and on the
other side, it can bring a negative impact to public
health. The negative health impact also makes the
BPJS budget in deficit in the midst of Indonesia's
efforts to realise universal health coverage. There
needs to be an accurate review to resolve the tobacco
policy dilemmas such as cigarette tax increments,
tax revenue sharing for rehabilitative and curative
services for smokers, and an agreement to include
smoking diseases as a disease not covered by BPJS
in order to avoid the deficit.
REFERENCES
Ade, Mustami Adinda. Tarif Cukai Rokok Naik 10% di
2017 [online]. Kontan Harian 2016 Sept 30.
Available
Ahsan, A. 2013. Ratifikasi FCTC, Kondisi Perekonomian
dan Beban Masa Depan. Available from: URL:
http://www.inahea.org
Badan Kebijakan Fiskal. 2016. Harga Rokok, Dilema
Pembangunan, dan Kualitas Hidup [online].
Available from: URL:http://www.cheps.or.id
Directorate General of Customs and Excise Ministry
of Finance Republic of Indonesia. 2016. Warta
Bea Cukai [online]. Available from: URL:
http://www.Beacukai.go.id
Hafizd, M., Gloria, S. 2016. Dilema Rokok , Antara
Kesehatan Dan Pusaran Duit Triliunan [online].
CNN Indonesia CNN Indonesia 2016 Mei 31.
INAHEA 2017 - 4th Annual Meeting of the Indonesian Health Economics Association
108

Available from: URL:
https://www.cnnindonesia.com
Indonesian Government, 2007. Undang-Undang Nomor
39 tahun 2007 tentang Cukai.
Indonesian Government, 2009. Undang-Undang Nomor
28 tahun 2009 tentang Pajak Daerah dan Retribusi
Daerah.
Indonesian Government, 2013. Peraturan Presiden Nomor
111 tahun 2013 tentang Jaminan Kesehatan.
Jongudomsuk, P, et al. 2015. The Kingdom of Thailand
Health System Review. Jurnal Health Systems in
Transition; 05 (3); 64. Available from: URL:
http://www.wpro.who.int/asia_pasific_observatory/
hal 64
Kuntjojo. 2009 Metodologi Penelitian;
Kementrian Pertanian. Statistik Perkebunan Indonesia
Komoditas Tembakau 2015-2017 [online]. 2016.
Available from: URL:
http://ditjenbun.pertanian.go.id
Ministry of Finance. 2016. Peraturan Menteri Keuangan
Republik Indonesia Nomor 40 tahun 2016 tentang
Pembayaran dan/ atau penyetoran penerimaan
Negara dalam rangka kepabeanan dan cukai secara
elektronik.
Pardede, D. Tantangan dalam Sustainabilitas Pembiayaan
JKN. Indo-Health Care Panel Discussion; 26 April
2016; Jakarta, Indonesia
Dilemma of Tobacco’s Policy in Indonesia: Increasing Country’s Income or Increasing the Country’s Poverty with National Health
Insurance’s Deficit?
109
