
The Difference of Glutathione Peroxidase Levels among Chronic
Atrophic Gastritis, Intestinal Metaplasia, and Dysplasia in Patients
with Helicobacter pylori-associated Gastritis
Masrul Lubis
1
, Taufik Sungkar
1
, Gontar Alamsyah Siregar
1*
, Ginanda Putra Siregar
2
and Darmadi
3
1
Division of Gastroentero-Hepatology, Department of Internal Medicine, Faculty of Medicine, Universitas
Sumatera Utara, Dr Mansyur 5, Medan, Indonesia
2
Division of Urology, Department of Surgery, Faculty of Medicine, Universitas Sumatera Utara, Dr Mansyur 5,
Medan, Indonesia
3
Department of Internal Medicine, Faculty of Medicine, Universitas Sumatera Utara, Dr Mansyur 5, Medan,
Indonesia
ign.darmadi@yahoo.com
Keywords: Glutathione Peroxidase, Helicobacter pylori, Gastritis.
Abstract: Helicobacter pylori infection is the main etiology of chronic gastritis. Chronic mucosal inflammation can
lead to chronic atrophic gastritis, intestinal metaplasia, and gastric dysplasia. Oxidative stress plays a role in
inflammatory and malignancy process. Glutathione peroxidase (GPX) levels will decrease due to oxidative
stress. This study was conducted to evaluate the difference of GPX serum levels among chronic atrophic
gastritis, intestinal metaplasia, and dysplasia in H. pylori-associated gastritis patients. A cross-sectional
study on 70 consecutive gastritis patients who came to the endoscopic unit of Adam Malik General Hospital
and Permata Bunda Hospital in Medan, Indonesia, from April – June 2018. The diagnosis of gastritis was
derived histopathologically. Rapid urease test for diagnosis of H. pylori infection. Serum samples were
obtained to determined circulating GPX. Univariate and bivariate (Kruskal Wallis test) analysis were
performed with SPSS version 22. There were 21 patients (30%) with chronic atrophic gastritis, 15 patients
(21.4%) with intestinal metaplasia, and 8 patients (11.4%) with dysplasia. There were significant differences
in GPX levels among chronic atrophic gastritis, intestinal metaplasia, and dysplasia (p = 0.037). GPX levels
were significantly lower in patients with dysplasia than chronic atrophic gastritis. There were no significant
difference in GPX levels between patients with intestinal metaplasia and chronic atrophic gastritis or
dysplasia.
1 INTRODUCTION
Gastritis is an inflammatory process in mucosa and
submucosa stomach as response to injuries that can
be acute or chronic (El-Zimaity, 2007). It is found
that Helicobacter pylori (H. pylori) is the main
etiology of chronic gastritis, gastric premalignant
lesion, and gastric cancer. H. pylori is a type 1
carcinogen according to International Agency for
Research on Cancer (IARC). Nearly 50% of the
world's population was estimated to be infected with
H. pylori, about 70-90% occur in developing
countries and only 40-50% in industrial Countries
(Chekhonin, 2013). Reactive oxygen species (ROS)
can be generated by H. pylori. H. pylori infection
can cause chronic inflammation resulting in
accumulation of ROS (Suzuki, 2012; White, 2015).
The human body has a protective mechanism that
neutralizes free radicals, with the presence of
superoxide dismutase (SOD), catalase, and
glutathione peroxidase (GPX) enzymes (Birben,
2012). GPX is an enzyme that acts to catalyze
hydrogen peroxide (H
2
O
2
) and organic
hydroperoxide to prevent lipid peroxidation of cell
membranes. GPX can be found in mitochondria,
cytosol or extracellular (Lubos, 2012). In certain
conditions, free radicals can exceed the body's
defense system, this condition is called as oxidative
stres (Ayala, 2014).
ROS that exceeds the capacity of antioxidants to
neutralize free radicals, causing further cell damage.
420
Siregar, G., Lubis, M., Sungkar, T., Siregar, G. and Darmadi, .
The Difference of Glutathione Peroxidase Levels among Chronic Atrophic Gastritis, Intestinal Metaplasia, and Dysplasia in Patients with Helicobacter pylori-associated Gastritis.
DOI: 10.5220/0010070004200424
In Proceedings of the International Conference of Science, Technology, Engineering, Environmental and Ramification Researches (ICOSTEERR 2018) - Research in Industry 4.0, pages
420-424
ISBN: 978-989-758-449-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
ROS will cause mucosal damage by causing basal
epithelial membrane degradation so that there will
be changes in cell metabolism and damage to DNA
(Mahmood, 2009). Tissue damage and DNA lesions
can cause dysregulation of cellular homeostasis in
gastric mucosa that plays a role in gastric
carcinogenesis due to H. pylori from chronic
gastritis, gastric premalignant lesions (atrophic
gastritis, intestinal metaplasia, and dysplasia), to
gastric cancer (Kalisperati, 2017; Dinis-Ribeiro,
2012).
Research on antioxidant level in gastric
premalignant lesion were still limited. The purpose
of this study was to determine the difference of
glutathione peroxidase levels among chronic
atrophic gastritis, metaplasia intestinal, and
dysplasia in patients with H. pylori-associated
gastritis.
2 METHODS
2.1 Patient Selection
This study was a cross sectional study conducted on
70 subjects who came to endoscopy unit at Adam
Malik General Hospital, Medan Indonesia from
April until June 2018. Exclusion criteria were
patients who refuse to participate, patients with
systemic disease like diabetes mellitus,
hypertension, liver disease, kidney disease, heart
disease and malignancy. All patients gave informed
consent, This study was approved by the
Institutional Review Board of Universitas Sumatera
Utara.
2.2 Diagnosis of Gastritis
Diagnosis of gastritis is based on histopathological
examination. During endoscopy, tissue samples were
taken from antrum and corpus gaster. These tissues
were then stained with Hematoxylin-Eosin stain.
Histopathological examinations were examined
under the same pathologist of Pathology Anatomy
Laboratory of Universitas Sumatera Utara.
2.3 Diagnosis of H.pylori
Positive results of CLO test would indicate presence
of H. pylori bacteria. A rapid urease test was
performed within 24 hours after the collection of the
sample.
2.4 Diagnosis of GPX Level
The sample used was venous blood mixed with
heparin as an anticoagulant. The Reagent kit used
was Ransel Glutathione Peroxidase Cat RS505
(Randox Laboratories Ltd., United Kingdom). The
Instrument for measurement was Advia 1800
instrument (Siemens Healthcare GmbH, Germany)
with a reference range of 27.5 – 73.6 U/g Hb.
Processing steps followed instruction kit (Mahmood,
2009). The examination was conducted at Prodia
Research and Esoteric Laboratory.
2.5 Statistical Method
Statistical data composed of univariate and bivariate
were analyzed using SPSS version 22 (SPSS Inc.,
Chicago) with 95% confidence interval. The analysis
was carried out using Kruskal Wallis test with
significance level p<0.05.
3 RESULT
3.1 Baseline Characteristics of Subjects
A total of 40 patients (57.1%) were men with an
average age of 51 years old. Majority of subjects
were Batak ethnicity (68.6%). Two major
occupations of subjects were the private employee
(38.6%), followed by enterpreneur (31.4%). Mean of
subject's BMI was 23.4 kg/m
2
(Table 1).
Table 1: Basic characteristics of subjects.
Variable n = 70
Sex
Male
Female
40 (57.1%)
a
30 (42.9%)
Age, years 51 + 8.9
b
BMI, kg/m
2
23.4 + 4.5
b
Ethnic
Batak
Javanese
Acehnese
48 (68.6%)
a
15 (21.4%)
7 (10%)
Occupation
Private Employee
Enterpreneur
Housewife
Student
27 (38.6%)
a
22 (31.4%)
16 (22.9%)
5 (7.1%)
n = total number of subjects
a
Percentage
b
Mean ± SD
The Difference of Glutathione Peroxidase Levels among Chronic Atrophic Gastritis, Intestinal Metaplasia, and Dysplasia in Patients with
Helicobacter pylori-associated Gastritis
421
3.2 Prevalence of Chronic Atrophic
Gastritis, Intestinal Metaplasia, and
Dysplasia
Through the histopathological examination, a total of
21 patients (30%) were diagnosed with chronic
atrophic gastritis, 15 patients (21.4%) were
diagnosed with intestinal metaplasia, and 8 patients
(11.4%) were diagnosed with dysplasia (Table 2).
Table 2: Prevalence of chronic atrophic gastritis, intestinal
metaplasia, and dysplasia.
Gastritis H. pylori n = 70
Chronic atro
p
hic
g
astritis 21
(
30%
)
Intestinal meta
p
lasia 15
(
21.4%
)
D
y
s
p
lasia 8
(
11.4%
)
3.3 The Difference of GPX Levels
among Chronic Atrophic Gastritis,
Intestinal Metaplasia, and
Dysplasia in Patients with
Helicobacter pylori-associated
Gastritis
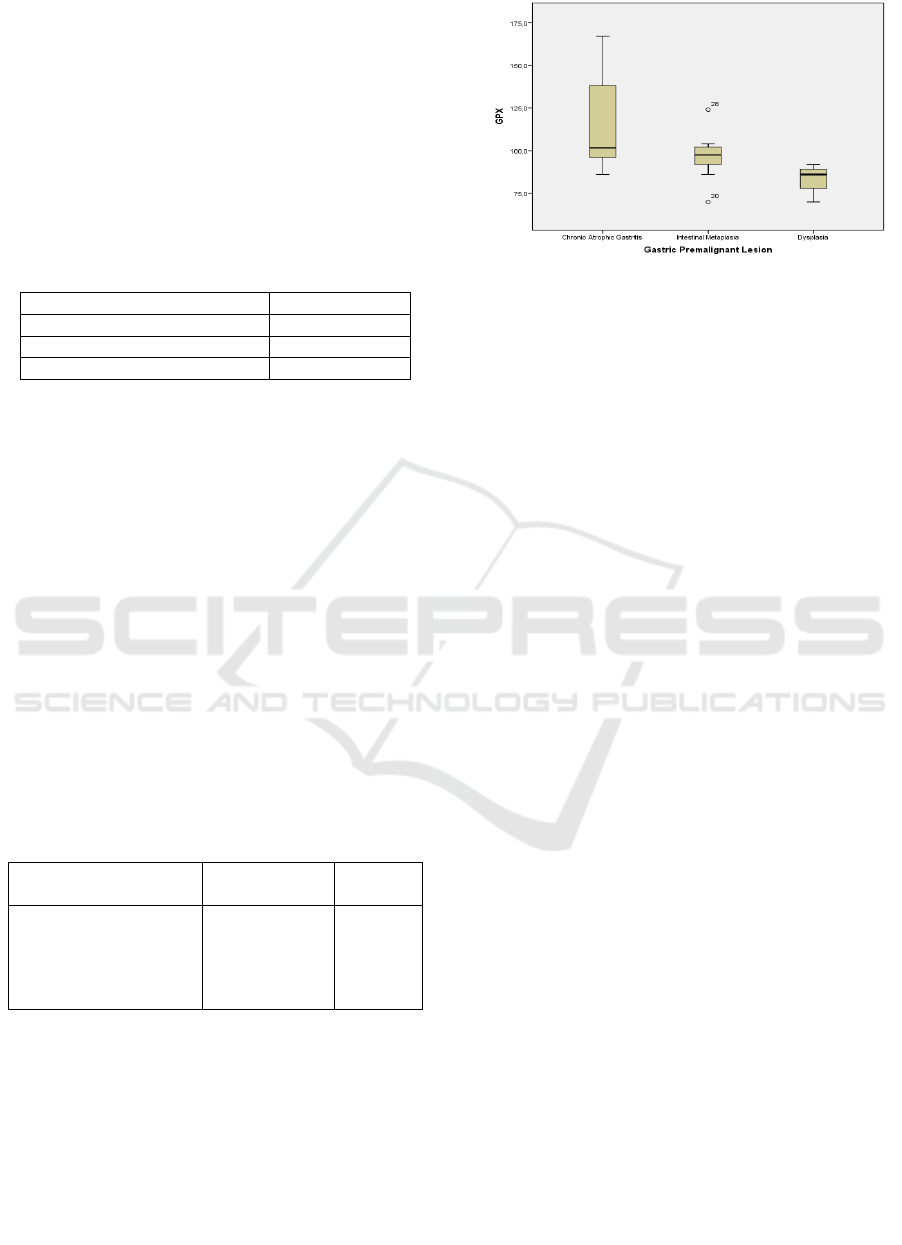
There were significant differences in GPX levels
among chronic atrophic gastritis, intestinal
metaplasia, and dysplasia (p = 0.037). GPX levels
were significantly lower in patients with dysplasia
than chronic atrophic gastritis. There were no
significant difference in GPX levels between
patients with intestinal metaplasia and chronic
atrophic gastritis or dysplasia (Table 3).
Table 3: The differences of GPX levels among chronic
atrophic gastritis, intestinal metaplasia, and dysplasia in
patients with Helicobacter pylori-associated gastritis.
Diagnosis GPX (U/g
HGB)
p
Chronic atrophic
gastritis
Intestinal metaplasia
Dysplasia
101.5 (86 –
167)
97.5 (70 –
124)
86 (70
–
92)
#
0.037*
*p<0.05,
#
there was a significant difference with chronic
atrophic gastritis
Figure 1. Serum GPX levels in chronic atrophic gastritis,
intestinal metaplasia, and dysplasia.
4 DISCUSSION
Gastric carcinogenesis is a multistep and
multifactorial process. Gastric cancer is preceded by
a cascade of precancerous lesions, such as chronic
atrophic gastritis, intestinal metaplasia and
dysplasia. The following step is invasive carcinoma,
which is thought to be associated with degradation
of the intercellular matrix. Besides environmental,
diet and genetic factors, gastric cancer is closely
associated with H. pylori infection (Correa, 2012;
Park, 2015).
Infection of H. pylori is one of the thoroughly
studied risk factors of gastric cancer. A primary
factor that is important in the events that lead to the
progression of the inflammation-to-carcinoma is
oxidative DNA damage induced by H.
pylori infection (Farinati, 1998), which is probably
due to infiltrating neutrophils, and also direct effects
of H. pylori (Obst, 2000). Under normal
circumstances, free radicals are produced in low
quantity. However, this is not pathological because
free radicals will be suppresed by the elevated
amount of endogenous antioxidants (GPX, SOD,
and catalase) as a compensatory mechanism to
prevent further tissue damage (Li, 2015). But in
certain conditions, free radicals can exceed the
body's defense system, this condition is called as
oxidative stres (Mahmood, 2009). Recruitment of
phagocytes in gastritis will induce an increase in free
radicals. Anion superoxide radicals (O
2
-
) are
generated by neutrophil infiltration reactions to
cellular lipid membranes that lead to lipid
peroxidation formation (Li, 2015). These lipid
peroxidation reactions damage the cell membranes,
eventually causing the release of intracellular
components such as lysosomal enzymes, which will
further tissue damage, degradation of epithelial
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
422

basement membrane, disrupt cell metabolism, and
MDA reactions with DNA will form mutagenic
MDA deoxyguanosine (Mi-dG) (Choi, 1999; Drake,
1998).
Production of ROS in the H. pylori-infected
gastric epithelium is linked to the presence of
cagPAI and contribute to the oxidative stress
response in gastric epithelial cells (Ding, 2007). It is
well known that H. pylori infection causes elevated
level of polyamines, in particular spermine and this
is associated with an induction of spermine oxidase
(Cheng, 2009). Action of spermine oxidase on
spermine leads to the production of elevated levels
of hydrogen peroxide, which is a powerful oxidizing
agent and also contributes to the production of free
radicals such as hydroxyl radial (Xu, 2004).
Additionally, H. pylori will activate macrophages
which will result in a significant upregulation of
spermine oxidase, contributing to oxidative stress
and damage to the gastric epithelial cells
(Chaturvedi, 2004).
In a previous study, Subha et al reported that
there were statistically significant decrease of mean
GPX levels in cancer patients compared to control
groups. Cancer patients showed a lower mean of
GPX levels than control group. Research on GPX
levels in patients with premalignant lesions of
gastric is still limited. In this study there were
significant difference in GPX levels among chronic
atrophic gastritis, intestinal metaplasia, and
dysplasia. GPX levels were significantly lower in
patients with dysplasia than chronic atrophic
gastritis and there were no significant difference in
GPX levels between patients with intestinal
metaplasia and chronic atrophic gastritis or
dysplasia. Lower GPX levels are associated with the
progression of precancerous lesions, which is
supported by GPX levels that were significantly
lower in dysplasia than chronic atrophic gastritis.
This study showed that antioxidant supplements may
be considered in patients with gastric premalignant
lesions. A further study is needed to evaluate the
antioxidant options and their role in the
improvement of oxidative stress in patients with
gastric premalignant lesion.
5 CONCLUSION
GPX levels were significantly lower in patients with
dysplasia than chronic atrophic gastritis.
ACKNOWLEDGEMENT
The authors would like to thank for the funding
support by Research Institute, Universitas Sumatera
Utara (Contract number : 61/UN5.2.3.1/PPM-KP-
TALENTAUSU/2018)
REFERENCES
Ayala, A., Muñoz, M., Argüelles, S., 2014. Lipid
Peroxidation: Production, Metabolism, and Signaling
Mechanisms of Malondialdehyde and 4-Hydroxy-2-
Nonenal. Oxid Med Cell Longev. 360438.
Birben, E., Sahiner, U., Sackesen, C., Erzurum, S.,
Kalayci, O., 2012. Oxidative stress and antioxidant
Defense. World Allergy Organ J. 5:9–19.
Chaturvedi, R., Cheng, Y., Asim, M., Bussiere, F., Xu,
H., Gobert, A., et al., 2004. Induction of polyamine
oxidase 1 by Helicobacter pylori causes macrophage
apoptosis by hydrogen peroxide release and
mitochondrial membrane depolarization. J Biol
Chem. 279:40161-73.
Chekhonin, V., Shein, S., Korchagina, A., Gurina, O.,
2013. VEGF in tumor progression and targeted
therapy. Current Cancer Drug Targets. 13:423-43.
Cheng, Y., Chaturvedi, R., Asim, M., Bussiere, F.,
Scholz, A., Xu, H., et al., 2005. Helicobacter pylori-
induced macrophage apoptosis requires activation of
ornithine decarboxylase by c-Myc. J Biol Chem.
280:22492-6.
Choi, M., Kim, B., Yu, R., 1999. Serum antioxidative
vitamin levels and lipid peroxidation in gastric
carcinoma patients. Cancer Lett. 136:89-93.
Correa, P., Piazuelo, M., 2012. The gastric precancerous
cascade. J Dig Dis. 13:2-9.
Ding, S., Minohara, Y., Fan, X., Wang, J., Reyes, V.,
Patel, J., et al., 2007. Helicobacter pylori infection
induces oxidative stress and programmed cell death
in human gastric epithelial cells. Infect Immun.
75:4030-9.
Dinis-Ribeiro, M., Areia, M., de Vries, A., Marcos-Pinto,
R., Monteiro-Soares, M., O’Connor, A., et al., 2012.
Management of precancerous conditions and lesions
in the stomach (MAPS): guideline from the European
Society of Gastrointestinal Endoscopy (ESCE),
European Helicobacter Study Group (EHSG),
European Society of Pathlogy (ESP), and the
Sociedade Protuguesa de Endoscopia Digestiba
(SPED). Virchows Arch. 460: 19-46.
Drake, I., Mapstone, N., Schorah, C., White, K.,
Chalmers, D., Dixon, M., et al., 1998. Reactive
oxygen species activity and lipid peroxidation in
Helicobacter pylori associated gastritis: relation to
gastric mucosal ascorbic acid concentrations and
effect of H. pylori eradication. Gut 42:768-71.
The Difference of Glutathione Peroxidase Levels among Chronic Atrophic Gastritis, Intestinal Metaplasia, and Dysplasia in Patients with
Helicobacter pylori-associated Gastritis
423

El-Zimaity, H., 2007. Recent advances in the
histopathology of gastritis. Curr Diagn Pathol.
13:340-8.
Farinati, F., Cardin, R., Degan, P., Rugge, M., Mario, F.,
Bonvicini, P., et al., 1998. Oxidative DNA damage
accumulation in gastric carcinogenesis. Gut. 42:351-
6.
Kalisperati, P., Spanou, E., Pateras, I., Korkolopoulou,
P., Varvarigou, A., Karavokyros, I., et al., 2017.
Inflammation, DNA damage, Helicobacter pylori and
gastric tumorigenesis. Front Genet. 8:20.
Li, J., Tang, H., Chen, Y., Fan, Q., Shao, Y., Jia, M., et
al., 2015. Malondialdehyde and SOD-induced
changes of gastric tissues in acute gastric mucosal
injury under positive acceleration. Genet Mol.
14:4361-8.
Lubos, E., Loscalzo, J., Handy, D., 2011. Glutathione
peroxidase-1 in health and disease: from molecular
mechanisms to therapeutic opportunities. Antioxid
Redox Signal. 15:1957-97.
Mahmood, N., 2009. Measurement of malondialdehyde
and thiol level in Iraqi patients with gastroduodenal
diseases. Iraqi J Biotech. 8:465-72.
Obst, B., Wagner, S., Sewing, K., Beil, W., 2000.
Helicobacter pylori causes DNA damage in gastric
epithelial cells. Carcinogenesis. 21:1111-5.
Park, Y., Kim, N., 2015. Review of atrophic gastritis and
intestinal metaplasia as a premalignant lesion of
gastric cancer. J Cancer Prev. 20:25-40.
Suzuki, H., Nishizawa, T., Tsugawa, H., Mogami, S.,
Hibi, T., 2012. Roles of oxidative stress in stomach
disorders. J Clin Biochem Nutr. 50:35-9.
White, J., Winter, J., Robinson, K., 2015. Differential
inflammatory response to Helicobacter pylori
infection: etiology and clinical outcomes. J Inflamm
Res. 8:137-47.
Xu, H., Chaturvedi, R., Cheng, Y., Bussiere, F., Asim,
M., Yao, M., et al., 2004. Spermine oxidation
induced by Helicobacter pylori results in apoptosis
and DNA damage: implications for gastric
carcinogenesis. Cancer Res. 64:8521-5.
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
424
