
Profile and Risk Factor of Hepatocellular Carcinoma Patients
Siti Hasnita O. Purba
1
, Imelda Rey
2, 3
1
Student of Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
2
Division of Gastroenterohepatology, Internal Medicine Department, Universitas Sumatera Utara, Medan, Indonesia
3
Adam Malik General Hospital, Bunga Lau Street, Medan, Indonesia
Keywords: Hepatocellular Carcinoma, Profile, Risk Factors.
Abstract: Hepatocellular carcinoma (HCC) is the most common primary liver malignant tumor in the world. The
incidence of hepatocellular carcinoma varies worldwide and is correlated with the incidence of hepatitis B
virus and hepatitis C virus. In addition to viral hepatitis, there are other risk factors such as alcohol
consumption that causes alcoholic liver disease and obesity and diabetes associated with non-alcoholic fatty
liver disease (NAFLD) / non-alcoholic steatohepatitis (NASH). Most of these risk factors lead to the
development of liver cirrhosis. One of the most commonly used stages of hepatocellular carcinoma is
Barcelona Clinic Liver Cancer (BCLC) staging system that can also determine which therapy will be given
to patients with hepatocellular carcinoma. The aim of this study was to determine the profile and risk factors
of hepatocellular carcinoma patients. This cross-sectional study using HCC patient’s medical records in
Adam Malik General Hospital from January 2016 – June 2017. There were 182 patients with hepatocellular
carcinoma with the highest age group 40-60 years (54.4%), dominated by male sex (80.2%), occupation
with the highest prevalence is self-employed (27.5%), has no family history (97.8%), risk factors with the
highest prevalence is hepatitis B (47.3%), Child-Pugh B (57.1%), multinodular radiology (51.1%), AFP
increased, BCLC stage B (40.7%) and treated with symptomatic treatment (78%). The highest risk factor in
patients with hepatocellular carcinoma is hepatitis B.
1 INTRODUCTION
Hepatocellular carcinoma (HCC) is a primary
malignant liver tumor that originating from
hepatocytes (Budihusodo, 2014). HCC is the ninth
most common cancer in women and fifth in men.
HCC mortality rate is also very high, in second place
of cancer-related death after lung cancer
(GLOBOCAN 2012).
The incidence of HCC varies worldwide and
correlates with regional prevalence of Hepatitis B
Virus (HBV) and Hepatitis C Virus (HCV)
(Budihusodo, 2014). In the endemic areas, HBV is
majority obtained by vertical and perinatal
transmission more than 90% of these cases changes
to chronic HBV carriers. HBV is a well-known
cause of HCC because it can become HCC without
cirrhosis, although most HBV (70-90%) develop
into cirrhosis prior to becoming HCC (Yang et al,
2011). Some cases of HCV has been reported, in
Italy 44-66% turn in to HCC cases and about 80% in
Japan. Whereas, in United States, the chronic HCV
was also a major risk factor for HCC (El-Serag,
2007).
Other risk factors of viral hepatitis, such as
alcohol consumption that associated to alcoholic
liver disease and obesity and diabetes associated
with non-alcoholic fatty liver disease (NAFLD) /
non-alcoholic steatohepatitis (NASH). Most of these
risk factors lead to the development of liver cirrhosis
present in 80-90% of HCC patients (El-Serag, 2011).
Several studies reported that risk of developing HCC
through NASH-associated cirrhosis is lower than
other liver diseases, such as HCV and HBV
(Takuma, 2010).
Although the prevalence of HCC in patients with
NASH is low, but the prevalence of obesity-related
NASH in the United States is high and it is a leading
to indicated a major causes for liver transplantation
(Wong, 2014).
Purba, S. and Rey, I.
Profile and Risk Factor of Hepatocellular Carcinoma Patients.
DOI: 10.5220/0010070204250428
In Proceedings of the International Conference of Science, Technology, Engineering, Environmental and Ramification Researches (ICOSTEERR 2018) - Research in Industry 4.0, pages
425-428
ISBN: 978-989-758-449-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
425
2 METHODS
This study was a cross-sectional study design. Data
were taken by using secondary data from medical
record of hepatocellular carcinoma patients at RSUP
Haji Adam Malik Medan period 1
st
of January 2016
until 30
th
of June 2017. The sampling method was
done by total sampling method. Data taken include
age, sex, risk factors, laboratory results, child-pugh
classification, radiological results, BCLC stage,
tumor marker results and therapy provided.
3 RESULT
This study was obtained 182 patients hepatocellular
carcinoma who visited the RSUP Haji Adam Malik
Medan during the period 01 January 2016 - 30 June
2017.
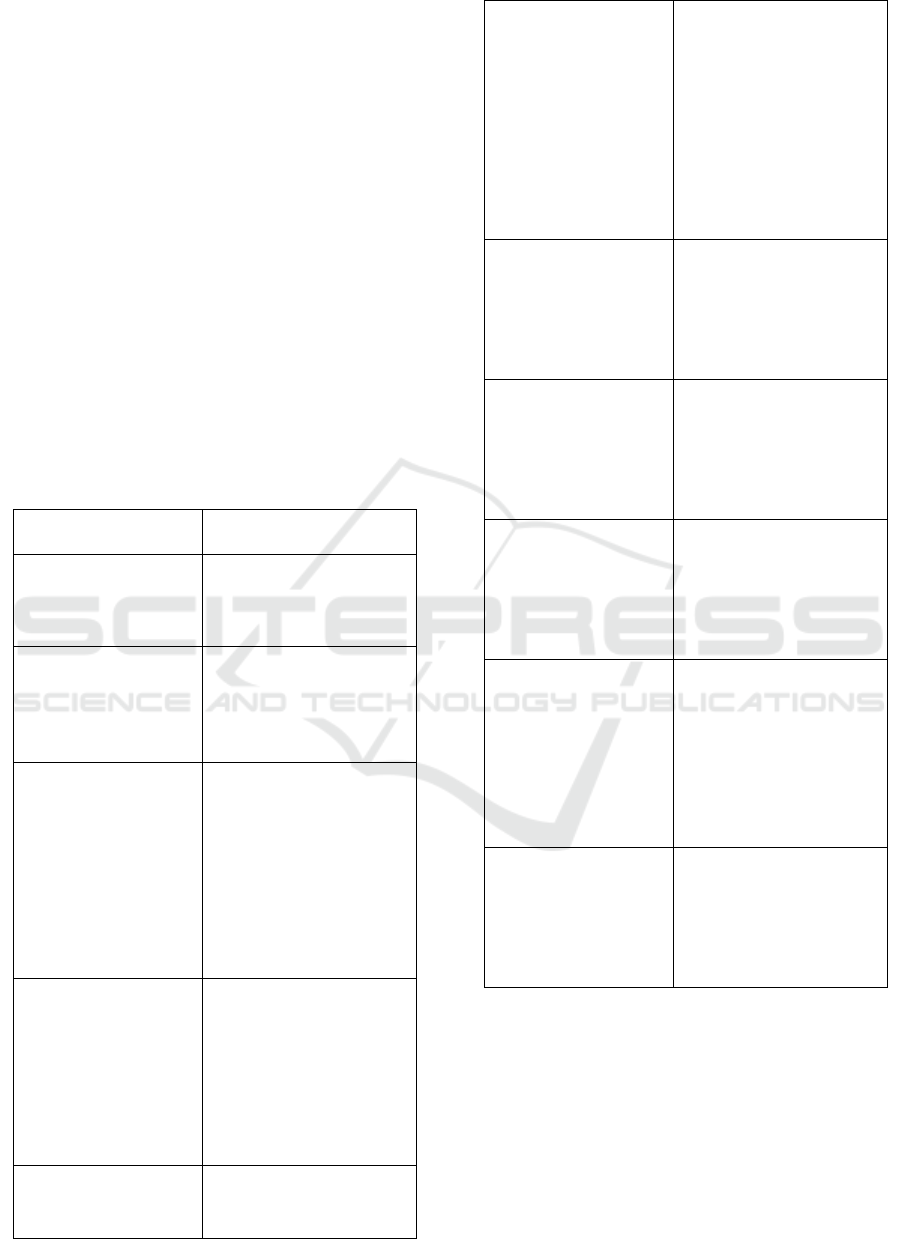
Table 1 : Characteristics of HCC patients
Characteristic n = 182
Sex
Men
Women
146 (80,2)
36 (19,8)
Age (years)
< 40
40-60
> 60
25 (13,7)
99 (54,4)
58 (31,9)
Occupation
Government
employees
Private employees
Entrepreneur
Farmers
Housewife
Retired
Others
18 (9,9)
19 (10,4)
50 (27,5)
39 (21,4)
17 (9,3)
17 (9,3)
22 (12,1)
Risk factors
HBV
HCV
Cirrhosis
Alcohol
Diabetes
Obesity
86 (47,3)
10 (5,5)
60 (33)
41 (22,5)
16 (8,8)
29 (15,9)
Laboratory data
Hb (g/dL)
Leucocyte
10,9±2,7
10.705,13±4957,31
(cells/mm
3
)
Trombosite
(thousand/mm
3
)
ALT (U/L)
ASP (U/L)
ALP (U/L)
Gamma-GT (U/L)
Bilirubin (mg/dL)
Albumin (g/dL)
INR
275.756,90±1,60
69,81±76,09
201,65±252,12
277,18±265,64
345,88±305,02
3,8±6,4
2,7±0,65
1,2±0,39
Tumor marker
AFP (ng/ml)
CEA (ng/ml)
CA125 (u/ml)
CA19-9 (u/ml)
26.728,84±1,67
464,33±1856,02
286,26±261,67
161,09±351,64
Child-Pugh score (%)
A
B
C
Missing
47 (25,8)
104 (57,1)
27 (14,8)
4 (2,2)
Tumor type (%)
Soliter
Multinoduler
Diffuse
Missing
52 (28,6)
93(51,1)
7 (3,8)
30 (16,5)
BCLC stage (%)
0
A
B
C
D
Missing
14 (7,7)
30 (16,5)
74 (40,7)
13 (7,1)
25 (13,7)
26 (14,3)
Treatment (%)
Hepatic resection
TACE
Liver transplantation
Symptomatic
2 (1,1)
37 (20,3)
142 (78)
1 (0,5)
4 DISCUSSION
Table 1 shows the characteristics of patients in
which the largest number of hepatocellular
carcinoma patients were men. This is in accordance
with previous study that found the most sex in
hepatocellular carcinoma patients were male
(Karageorgos et al, 2017; Mittal et al, 2015). Sex
influences are also associated to sex hormones
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
426

namely androgens and estrogens which is main
regulated the progression of HBV infection and the
incidence of HBV-associated to hepatocellular
carcinoma, in which androgens increase the
transcription and replication of the HBV gene
whereas the estrogen plays a protective role by
decreasing the transcription of HBV RNA and the
number of inflammatory cytokines (Montella, 2015).
In addition, high alcohol consumption in men also
increases the hepatocellular carcinoma incidence
risk in people that infected by hepatitis B and
hepatitis C virus (Budihusodo, 2014).
The most risk factor in hepatocellular carcinoma
patients in this study is hepatitis B. Chronic hepatitis
B infection was a major risk factor for hepatocellular
carcinoma in the world (El-Serag, 2011). About 80%
of the world's hepatocellular carcinoma cases are in
developing countries such as East Asia and
Southeast Asia and Central Africa, which is known
to be a high prevalence of viral hepatitis
(Budihusodo, 2014).
Chronic hepatitis B can progress to
hepatocellular carcinoma without cirrhosis, although
most develop into cirrhosis before it becomes
hepatocellular carcinoma (Yang et al, 2011). In this
study, the second highest risk factor was cirrhosis
hepatis. This is associated with high incidence of
hepatitis B and other risk factors that can develop
into cirrhosis before becoming hepatocellular
carcinoma.
The laboratory results of hepatocellular
carcinoma patients where the mean Hb decreases,
normal leukocytes, normal platelets, ALT increases,
ASP increases, ALP increases, Gamma-GT
increases, bilirubin increases, normal albumin and
normal INR. The most common abnormalities in
liver tumors are elevated alkaline phosphatase
(ALP) and GT gamma. The concentrations of SGOT
/ AST and SGPT / ALT enzymes in hepatocellular
carcinoma at baseline did not show an increase
unless the underlying disease was cirrhosis of the
liver. When the tumor gets bigger and greater liver
damage can also be found an increase in AST and
ALT (Amirudin, 2014).
In the results of tumor marker examination of
hepatocellular carcinoma patients found the average
AFP increased, the average CEA increased, the
average CA125 increased, and the average CA19-9
increased. AFP is a specific tumor marker in
diagnosing hepatocellular carcinoma, whereas other
tumor markers such as CEA, CA125 and CA19-9
are not specific but may increase with worsening
disease (Li et al, 2015).
In Asia, hepatocellular carcinomas usually
appear as well-described, solitary or multifocal
masses and are associated with secondary cirrhosis
due to hepatitis B. In western countries,
hepatocellular carcinomas usually appear as diffuse
infiltration masses and are associated with alcohol-
induced cirrhosis (Sharma, 2009). In this study, the
most radiology results in patients with hepatocellular
carcinoma multinodular. It is accordance with the
previous study that get the most tumor type is
multinodular (Su et al, 2017) .
The most common of Child-Pugh classification
in hepatocellular carcinoma patients was Child-Pugh
B. This study is in accordance with the previous
study which received the most Child-Pugh
classification is Child-Pugh B (Nadhim, 2016). The
most BCLC staging in patients with hepatocellular
carcinoma is stage B. According to previous study, it
showed that the highest stage of BCLC in
hepatocellular carcinoma hepatitis B virus etiology
is stage B (Nadhim, 2016). While in another study
received the highest stage BCLC was stage C (Mittal
et al, 2015; Hidayat, 2007). BCLC staging is closely
related to the Child-Pugh classification and
radiology results in patients, where in this study the
most Child-Pugh classifications are Child-Pugh B
and multinodular radiology results. That all
determine the choice of therapy which in this study
the most common treatment to the patients with
hepatocellular carcinoma is symptomatic treatment.
5 CONCLUSION
Most of patients were in BCLC staging B , with the
highest risk factor in patients with hepatocellular
carcinoma is hepatitis B.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge that the present
research is supported by Ministry of Research and
Technology and Higher Education Republic of
Indonesia.
REFERENCES
Amirudin, R. 2014, ‘Fisiologi dan Biokimia Hati’, in
Setiati, S. et al. (eds) Buku Ajar Ilmu Penyakit Dalam
Jilid II. Interna Publishing. Jakarta, 6
th
Edition.
Budihusodo, U. 2014, ‘Karsinoma Hati’, in Setiati, S. et
Profile and Risk Factor of Hepatocellular Carcinoma Patients
427

al. (eds) Buku Ajar Ilmu Penyakit Dalam Jilid III.
Interna Publishing. Jakarta, 6
th
Edition.
El–Serag, H. B., & Rudolph, K. L. 2007. Hepatocellular
carcinoma: epidemiology and molecular
carcinogenesis. Gastroenterology, 132(7), 2557-2576.
El-Serag, H. B. 2011, ‘Hepatocellular carcinoma’, The
New England Jorunal of Medicine, 365, pp. 1118–
1127.
Hidayat, H. 2007. Perbedaan profil klinik karsinoma
hepatoseluler yang terinfeksi kronik virus hepatitis B
dengan virus hepatitis C (Doctoral dissertation,
FacultyofMedicine).Availableat:http://eprints.undip.ac
.id/22680/1/Hendri_Hidayat.pdf
International Agency of Research on Cancer 2012,
GLOBOCAN 2012: Estimated Cancer Incidence,
Mortality and Prevalence Worlwide in 2012.
Available at:
http://globocan.iarc.fr/Pages/fact_sheets_population.as
px.
Karageorgos, S. A., Stratakou, S., Koulentaki, M.,
Voumvouraki, A., Mantaka, A., Samonakis, D., et al.
2017. Long-term change in incidence and risk factors
of cirrhosis and hepatocellular carcinoma in Crete,
Greece: a 25-year study. Annals of
gastroenterology, 30(3), 357.
Li, Y., Li, D. J., Chen, J., Liu, W., Li, J. W., Jiang, P., et
al. 2015. Application of Joint Detection of AFP,
CA19-9, CA125 and CEA in Identification and
Diagnosis of Cholangiocarcinoma. Asian pac J Cancer
prev, 16, 3451-3455.
Mittal, S., Sada, Y. H., El-Serag, H. B., Kanwal, F., Duan,
Z., Temple, S., et al. 2015. Temporal trends of
nonalcoholic fatty liver disease–related hepatocellular
carcinoma in the veteran affairs population. Clinical
Gastroenterology and Hepatology, 13(3), 594-601.
Montella, M., D’Arena, G., Crispo, A., Capunzo, M.,
Nocerino, F., Grimaldi, M., et al. 2015. Role of sex
hormones in the development and progression of
hepatitis B virus-associated hepatocellular
carcinoma. International journal of
endocrinology, 2015.
Nadhim, M., Suharti, C., Hardian. 2016. 'Distribusi
Geografis dan Tingkat Keparahan Pasien Karsinoma
Hepatoseluler Etiologi Virus Hepatiis B di RS Kariadi
Semarang', Jurnal Kedokteran Diponegoro, 5(4),
pp.1290-1302.
Sharma, R. and Madhusudhan, K. S. 2009, ‘Malignant
Focal Lesions of The Liver’, in Gupta, A. K.,
Chowdhury, V., and Khandelwal, N. (eds) Diagnostic
Radiology Gastrointestinal and Hepatobiliary
Imaging. Jaypee. New Delhi, 3
rd
Edition.
Su, Y. W., Liu, P. H., Hsu, C. Y., Lee, Y. H., Hsia, C. Y.,
Ho, S. Y., et al. 2017. Prognostic impact of diabetes
mellitus on hepatocellular carcinoma: Special
emphasis from the BCLC perspective. PloS
one, 12(3), e0174333.
Takuma, Y., & Nouso, K. 2010. Nonalcoholic
steatohepatitis-associated hepatocellular carcinoma:
our case series and literature review. World journal of
gastroenterology: WJG, 16(12), 1436.
Wong, R. J., Cheung, R., & Ahmed, A. 2014.
Nonalcoholic steatohepatitis is the most rapidly
growing indication for liver transplantation in patients
with hepatocellular carcinoma in the
US. Hepatology, 59(6), 2188-2195.
Yang, J. D., Kim, W. R., Coelho, R., Mettler, T. A.,
Benson, J. T., Sanderson, S. O., et al. 2011. Cirrhosis
is present in most patients with hepatitis B and
hepatocellular carcinoma. Clinical Gastroenterology
and Hepatology, 9(1), 64-70.
.
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
428
