
Decidual Killer Immunoglobulin-Like Receptor (KIR)2DL1
Expression and the Onset of Preeclampsia, Birth Weight and
Placental Weight in Early and Late Onset Preeclampsia
Khairunnisa Abd Rauf
1
, Erry Gumilar Dachlan
2
and Ariyanto Harsono
3
1
Master Student of Immunology, Postgraduate School Universitas Airlangga, Surabaya, Indonesia
2
Department of Obstetrics and Gynaecology, RS DR Soetomo, Surabaya, Indonesia
3
Department of Pediatrics, RS Dr Soetomo, Surabaya, Indonesia
Keywords: decidual, immunohistochemistry, KIR2DL1, placenta
Abstract: A
successful spiral artery remodelling ensures adequate uteroplacental perfusion and sufficient nutrient
supply to fetus. HLA-C interaction with maternal KIR determines the outcome of spiral artery remodelling.
Strong KIR2DL1 inhibitory lowers cytokine expression and angiogenic factors that affect uteroplacental
perfusion and nutrient supply. We analysed the decidual expression of KIR2DL1 in early-onset
preeclampsia (EO-PE) and late-onset preeclampsia (LO-PE) groups. We found a significant difference
between KIR2DL1 expression and EO-PE and LO-PE groups (p <0.001), with a strong negative correlation
between decidual expression of KIR2DL1 and EO-PE (p <0.001, r=-0.723), birth weight (p <0.001, r=-
0,.70) and placental weight (p <0.001, r=-0.770).
1 INTRODUCTION
Preeclampsia is a complication of pregnancy
characterised by high blood pressure, with or
without proteinuria. Preeclampsia is the third cause
of maternal mortality after postpartum haemorrhage
and infection. Preeclampsia has a prevalence of 5-
8%. (Say et al., 2014)
In 2004, the main cause of maternal mortality is
preeclampsia (29.9%) and postpartum haemorrhage
(26.12%). These two have become the main causes
of maternal mortality for a long time. In 2014, there
were 567 maternal deaths in East Java, and most
cases occurred in Surabaya. (Dachlan et al., 2016)
The early pathology of preeclampsia is the
failure of spiral artery remodelling. This causes
abnormal placentation and triggers the release of
pro-inflammatory mediators. Spiral artery
remodelling begins with the invasion of vascular
smooth muscle cells and replacement of
endothelium by trophoblasts. (Moffett and Colucci,
2014) The process leads to activation of endothelial
system, causes high blood pressure and increases
protein level in urine. (Kopcow, 2007)
Spiral artery remodelling is related to immune
system of the mother and the fetus. This process is
mediated by extravillous trophoblast (EVT) that
expresses HLA-C molecule. The process will be
recognized by Killer Immunoglobulin-like Receptor
(KIR) of the uterine natural killer (uNK) cells that
produces cytokines and angiogenic factors for
placentation and spiral artery remodelling. (Alicia,
2014)
In preeclampsia, KIR-AA inhibitory receptors
(one of them is KIR2DL1) from uNK cells will
recognize HLA-C molecules from EVT. This lowers
cytokine expression and angiogenic factors and
increases anti-angiogenic factors, such as soluble
endoglin (sENG) dan soluble fms-like tyrosine
kinase-1 (sFLT1) (Alicia, 2014)
In addition to NK cells, CD4, CD8 and γδ T cells
express Killer Immunoglobulin-like receptors (KIR).
Inhibitory KIR on CD8 T cells may modulate the
function of the cell and lessen CD8 respons. During
the activation process, KIR enhances CD8 function.
There is limited information available on how HLA
class I molecules affect T cells as they do on NK
cells (Björkström et al., 2012). KIR expression on T
cells has advantages that T cell may differentiate
self-maternal cells from allogeneic fetal cells and
modulate decidual immune response during
pregnancy. (Tamara et al., 2009)
Rauf, K., Dachlan, E. and Harsono, A.
Decidual Killer Immunoglobulin-Like Receptor (KIR)2DL1 Expression and the Onset of Preeclampsia, Birth Weight and Placental Weight in Early and Late Onset Preeclampsia.
DOI: 10.5220/0007542103210324
In Proceedings of the 2nd International Conference Postgraduate School (ICPS 2018), pages 321-324
ISBN: 978-989-758-348-3
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
321

This paper analysed decidual expression of
inhibitory KIR2DL1 expression and its effect on the
onset of preeclampsia, birth weight and placental
weight.
2 MATERIALS AND METHODS
2.1 Study design
This study was designed to analyse the distribution
and trend of placental KIR2DL1 expression in early
and late preeclampsia group, as well as its effect on
pregnancy outcome, which is the onset of
preeclampsia, birth weight and placental weight.
2.2 Subjects
We examined 35 patients aged 18-40 years old with
preeclampsia, in which 14 patients were diagnosed
with early preeclampsia (onset <34 weeks) and 21
patients with late preeclampsia (onset ≥34 weeks).
Immediately after delivery, placental biopsy with the
measurement of 2x2 cm was performed after written
informed consent, and samples were preserved in
Normal Buffer Formalin. Within 48 hours, paraffin
block was made. Baby’s birth weight was
immediately measured using a standard medical
scale.
Ethical approval was obtained from Ethical
Committee of Dr Soetomo Hospital
(371/Panke.KKE/V/2017) and Dr Soewandhie
Hospital (070/16284/436.8.6/2017), Surabaya,
Indonesia.
2.3 Immunohistochemistry of
KIR2DL1
Immunohistochemistry was performed based on IHC
protocol supplied from LifeSpan BioSciences, Inc.
This study used Primary polyclonal Anti-
KIR2DL1/CD 158a LS-C192811 antibody and
immunohistochemistry kit from ScyTek laboratories.
For interpretation of immunohistochemistry,
manual counting was performed in 10 field of views.
We obtain a mean of positive cells in one field view.
2.4 Statistical Analysis
The obtained data were analysed using unpaired
(two samples) t-test and Pearson and Spearman
correlation test. p-value of ≤0.05 was considered
statistically significant.
3 RESULTS
Placental KIR2DL1 expressions were found in both
early and late preeclampsia groups. KIR2DL1
expression was higher in early preeclampsia group
(4.42 ± 0.84 positive cells/field view) compared to
late preeclampsia group (1.24 ± 0.23 positive
cells/field view). We found that KIR2DL1
expressions were not only found on uterine NK
cells, but also on T cells in decidual. High
expression of KIR2DL1 was not only contributed by
NK cells, but also T cells.
Figure 1: Placental expression of KIR2DL1 in EO-PE and
LO-PE group. A significantly higher expression of
KIR2DL1 was found in early preeclampsia group (p
<0.001)
For the onset of preeclampsia, the mean value for
the onset in EO-PE group was 28 ± 3.84 weeks, and
33.37 ± 5.19 weeks for LO-PE group. Spearman test
showed a significant strong negative correlation
between KIR2DL1 expression and onset of
preeclampsia (p <0.001, r=-0.723).
ICPS 2018 - 2nd International Conference Postgraduate School
322
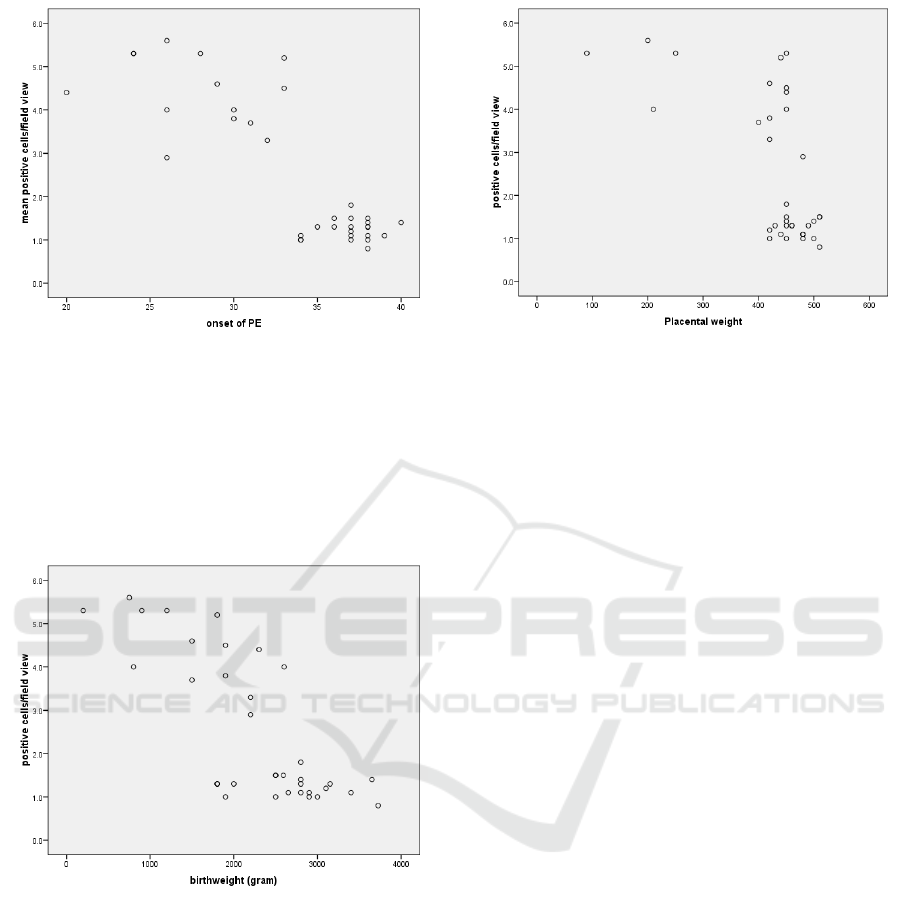
Figure 2: Strong negative correlation between KIR2DL1
expression and the onset of PE (p <0.001, r = -0.723).
A higher birth weight was obtained by LO-PE
with (2726.90 ± 542.45 gram) compared to EO-PE
(1553.57 ± 701.23 gram). There was a strong
negative correlation between KIR2DL1 expression
and birth weight (p <0.001, r=-0.770)
Figure 3: Birth weight is inversely related to KIR2DL1
expression in preeclampsia.
The mean value of placental weight for the
whole 35 samples was 427.14 ± 94.11 gram. A
higher placental weight was found in LO-PE group.
There was a strong negative correlation between
KIR2DL1 expression and placental weight (p
<0.001, r=-0.628)
Figure 4: Strong negative correlation between KIR2DL
expression and placental weight (p <0.001, r=-0.628).
4 DISCUSSION
The main pathological features of EO-PE are
incomplete transformation of spiral artery, which
impairs placental perfusion that results in inadequate
nutrition supply to the fetus. While in LO-PE, there
is a minimal or no failure in spiral artery
remodelling. (Gathiram and Moodley, 2016)
Difference in the main pathology is the cause of
different expression of KIR2DL1 in both early and
late preeclampsia group. KIR2DL1 expression is
also found in T cells, and this might contribute to
high expression of KIR2DL1.
During day 6-7 after fertilization, embryo will be
implanted at the wall of uterus. There are three steps
of implantation, which are apposition, adhesion and
invasion. Invasion of cytotrophoblast into the
vascular system is an important step in spiral artery
remodelling. Failure of spiral artery remodelling is
not a ‘yes’ or ‘no’ phenomenon. Severe failure leads
to preeclampsia with an earlier onset. If moderate or
minimal remodelling happens, the pregnancy will
continue until term, and it is manifested as late
preeclampsia. (Redman, Sargent and Staff, 2014)
Spiral artery remodelling involves invasion of
spiral artery endothelium and smooth muscle by
fetal trophoblast cells. (Whitley and Cartwright,
2010) Uterine NK Cells produces cytokines and
angiogenic factors that facilitate trophoblast
invasion. Secretion of these factors are lowered in
the presence of inhibitory AA haplotype KIR such
as KIR2DL1 (Redman, Sargent and Staff, 2014). We
found that inhibitory KIR2DL1 will lower the birth
weight.
Decidual Killer Immunoglobulin-Like Receptor (KIR)2DL1 Expression and the Onset of Preeclampsia, Birth Weight and Placental Weight
in Early and Late Onset Preeclampsia
323

Spiral artery provides nutrition and oxygenation
that is essential for fetal growth. Failure in spiral
artery remodelling damages uteroplacental perfusion
and thus effecting fetal growth.
One of the angiogenic factors secreted by uNK
cells are the Placental Growth Factor (PlGF), which
is a member of Vascular Endothelial Growth Factor
(VEGF). The function of PlGF is to aggravate the
growth and maturation of placental vascular system,
and also increase trophoblast proloferation. But in
the condition where inhibition signal is dominant,
PlGF production will be low and this will affect
placental growth. (Chau, Hennessy and Makris,
2017)
5 CONCLUSION
Higher expression of decidual KIR2DL1, earlier
onset of preeclampsia, low birth weight and low
placental weight found in EO-PE is consistent with
current concept of different pathophysiologic
pathway, leading to these different PE phenotypes.
ACKNOWLEDGEMENTS
We would like to thank the laboratory staff from
Anatomic Pathology Laboratory of Faculty of
Medicine Universitas Airlangga and Physiology
Laboratory of Brawijaya University Malang for their
assistance in completing this study.
REFERENCES
Björkström, N. K. et al., 2012. CD8 T cells express
randomly selected KIRs with distinct
specificities compared with NK cells, blood,
120(17), pp. 3455–3465.
Chau, K., Hennessy, A. and Makris, A., 2017.
Placental growth factor and pre-eclampsia,
Journal of Human Hypertension. Nature
Publishing Group, 31(12), pp. 782–786. doi:
10.1038/jhh.2017.61.
Dachlan, E. G. et al., 2016. Preeclampsia-Eclampsia
& Postpartum Hemorrhage. Surabaya.
Gathiram, P. and Moodley, J., 2016. Pre-eclampsia:
its pathogenesis and pathophysiolgy,
Cardiovascular Journal of Africa, 27(2), pp. 71–
78. doi: 10.5830/CVJA-2016-009.
Moffett, A. and Colucci, F., 2014. Uterine NK cells:
Active regulators at the maternal-fetal interface,
Journal of Clinical Investigation, 124(5), pp.
1872–1879. doi: 10.1172/JCI68107.
Redman, C. W., Sargent, I. L. and Staff, A. C., 2014.
IFPA senior award lecture: Making sense of pre-
eclampsia - Two placental causes of
preeclampsia?, Placenta. Elsevier Ltd,
35(SUPPL), pp. S20–S25. doi:
10.1016/j.placenta.2013.12.008.
Say, L. et al., 2014. Global causes of maternal death:
A WHO systematic analysis, The Lancet Global
Health, 2(6), pp. 323–333. doi: 10.1016/S2214-
109X(14)70227-X.
Tamara, T. et al., 2009. Expression of NK cell
receptors on decidual T cells in human
pregnancy, Journal of Reproductive
Immunology, 80(1–2), pp. 22–32.
Whitley, G. S. J. and Cartwright, J., 2010. Cellular
and Molecular Regulation of Spiral Artery
Remodelling: Lessons from the Cardiovascular
Field, Placenta, 6(31), pp. 465–474.
ICPS 2018 - 2nd International Conference Postgraduate School
324
