
Effectiveness of Cognitive Behavioral Therapy (CBT) to Reduce
Anxiety in Children with Autism Spectrum Disorder (ASD):
A Literature Review
Gst. Kade Adi Widyas Pranata
1
and A. A.Istri Wulan Krisnandari D.
1
1
ITEKES Bali (Institute of Technology and Health Bali), Denpasar, Bali, Indonesia
Keywords: Cognitive Behavioral Therapy, Autism Spectrum Disorder, Anxiety, Children.
Abstract: Anxiety is the most common problem in children with ASD. Although CBT shown more positive response
in reducing anxiety than pharmacotherapy, the magnitude of effects varies ranging from small to robust
effects. Objective: This review was to summarize the magnitude of CBT’s effects in reducing anxiety in
children with ASD. Methods: Relevant databases including PubMed, CINAHL, Cochrane Library, Science
Direct, and SCOPUS were searched using PICO question with time limit 5 years from 2011-2016. Of the
781 articles reviewed based on inclusion criteria (articles Systematic Review/ Meta-analysis of RCTs/ RCT,
CBT as the main treatment, anxiety as primary output, article is free and no duplication), only 2 articles
were fit and assessed critically. Critical Appraisal Skills Programme (CASP) (2013) was used to assess
systematic review and meta-analysis and Oxford Centre for Evidence Based Medicine (CEBM) (2005) was
used to assess RCTs. Results: CBT (length: 6-32 weeks, duration: 60-120 minutes) was statistically
significant treatment to alleviate anxiety in children with ASD (7-17 years old) in moderate (d = 0.79; g = -
0.76) to large effect size (d = 0.94-1.30). Effect size did not significantly differ reported among child, parent
or clinician. Conclusion: CBT is highly recommended for children with ASD.
1 INTRODUCTION
Autistic spectrum disorders (ASD) or commonly
abbreviated as autism are a collection of
neurological disorders with characteristic problems
in social relations and communication that occur in
childhood (Siegel et al., 2014). Lack of interest in
participating in social contacts or activities, as well
as failure in communication or the use of appropriate
language are two common symptoms that occur in
children with ASD. This problem is compounded by
their limitations in making eye contact and facial
expression. Therefore, it cannot be denied if they
prefer to be alone and live in their own world
(March and Schub, 2016).
Although children with ASD generally have
problems in social aspects such as failure to initiate
communication and relationships, psychological
problems, especially anxiety are the main
comorbidities that often arise besides depression,
cognitive impairment and stereotypical behavior
(Storch et al., 2015). According to the results of
various studies and surveys mentioned that anxiety
disorders and specific phobias occur in more than
50% of cases of children with ASD. Followed by
other types of anxiety such as separation anxiety and
generalized anxiety in more than 20% of cases
(Muris et al., 1998; Leyfer et al., 2006; De Bruin et
al., 2007; Simonoff et al., 2008).
ASD is a lifelong disturbance that requires
continuation of medical therapy (Siegel et al., 2014).
Several survey results have revealed that one of the
continuing medical therapies that is widely accepted
by children with ASD is psycho-pharmacotherapy,
especially serotonin reuptake inhibitors (SSRIs),
which is almost 90%. Although SSRIs have been
clinically proven to be used to reduce anxiety in
children with ASD, the sustainability of this therapy
needs to be considered since the side effects caused
mainly changes in metabolism such as improper
weight gain with growth and development patterns
in a child's body can be very dangerous
(Sukhodolsky et al., 2013).
One of the best solutions that can be given that
involves interdisciplinary teams with the aim of
improving adaptive behavior and emotional well-
Pranata, G. and A. Istri Wulan Krisnandari D., A.
Effectiveness of Cognitive Behavioral Therapy (CBT) to Reduce Anxiety in Children with Autism Spectrum Disorder (ASD): A Literature Review.
DOI: 10.5220/0008199000050011
In Proceedings of the 1st International Conference of Indonesian National Nurses Association (ICINNA 2018), pages 5-11
ISBN: 978-989-758-406-0
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
5

being without side effects is cognitive behavioral
therapy. Cognitive behavioral therapy or commonly
known as CBT is a therapy program that in the last
few decades have been an alternative solution to
address the anxiety problems experienced by
children with ASD because of the long-term benefits
offered. This therapy is useful since no previous
single remedy has proven effective in alleviating
anxiety as one of the core symptoms of ASD
(Hanson et al., 2007). The CBT program for anxiety
disorders is specifically designed to help children
with ASD identify the anxiety they experience, train
and encourage the use of adaptive behaviors and
self-awareness in responding to situations or
conditions that are the source of anxiety (Danial and
Wood, 2013). The two main focus and target of the
implementation of this therapy is the improvement
of the two body’s physiological functions, namely
cognitive functions such as anxiogenic cognitive
factors, and behavioral functions such as avoidance,
both of which are triggering factors for anxiety (Ung
et al., 2015).
The implementation of CBT basically rests on
two main assumptions namely behavior can be
influenced by cognitive activity and changes in
cognitive can affect behavior change (Dozois and
Dobson, 2001). Therefore, this therapy uses both
types of cognitive and associative methods as a
complementary approach. In CBT there are six
component methods, which are commonly
implemented. These components are related to one
another and consist of an assessment of the problems
faced both in nature and level, self-reflection,
training to restructure cognitive and affective
functions, management of anxiety, as well as
creating a new cognitive skills training schedule
(Shaker-Naeeni, Govender and Chowdhury, 2014).
Nowadays, studies of CBT for children has
developed rapidly and evaluated for the efficacy. For
example, in children who experience anxiety
disorders but not including children with ASD, CBT
has been applied in nearly 50 studies with a
randomized control trial design. Evaluations of these
studies show that CBT has had a positive effect with a
moderate effect sizes (ESs) on nearly 60% of
participants (Compton et al., 2004). However, in
children with ASD who experience anxiety, the
magnitude of the effect of this therapy varies or
differs from one another. Inconsistencies are seen in
the results of several studies that found small
therapeutic effects, while others found moderate to
strong effects. Hence, the purpose of this review was
to investigate and summarize the magnitude of CBT’s
effects in reducing anxiety in children with ASD.
2 METHODS
2.1 Literature Search
A systematic search on relevant databases such as
PubMed; CINAHL; Cochrane Library; Science
Direct and SCOPUS and reference lists of published
with time limit 5 years, 2011-2016 was conducted
using the keywords based on the PICO Question.
The entered keyword including the patient
population, intervention and the outcome (“autism
spectrum disorder in children” OR “autistic
spectrum disorder children” AND “cognitive
behavioral therapy” AND “anxiety”).
2.2 Selection of Studies
Studies were included in the literature review if they
meet the following inclusion criteria: (1) The design
or study method must be a Systematic Review/
Meta-analysis for RCT/ RCT or randomized
controlled trials or open trials. The design of studies
who do not meet the criteria such as case studies
were excluded; (2) Participants involved must be
children with ASD under the age of 18 years with a
diagnosis of ASD must be established through valid
and reliable measurements; (3) CBT must be the
main therapy; (4) Anxiety becomes the main output
and must be measured by psychometric instruments
that have been proven valid and reliable; (5)
Research articles must be published in English, are
open access and free to download, and there is no
duplication in the database.
2.3 Selection of Treatment Outcome
Measures
Based on the psychometrically sound properties and
the use of common anxiety severity scales in
children with ASD, the preferred list of outcome
measures need to be considered priori. Preferred
rating scales included Pediatric Anxiety Rating
Scale (PARS) (The Research Units On Pediatric
Psychopharmacology Anxiety Study Group, 2002),
Anxiety Disorders Interview Schedule for Child/
Parent or Clinical Severity Rating (ADIS-IV-C/P or
ADIS-IV-CSR) (Silverman and Albano, 1996),
Clinical Global Impression-Severity and
Improvement scale (CGI-Severity, CGI-
Improvement) (Guy, 1976), Multidimensional
Anxiety Scale for Children (MASC) or with Parent
(MASC-P) (March, 1998), Revised Child Anxiety
and Depression Scales (RCADS) (Chorpita, Moffitt
and Gray, 2005; Sterling et al., 2015), Revised
ICINNA 2018 - The 1st International Conference of Indonesian National Nurses Association
6
Children’s Manifest Anxiety Scale (RCMAS)
(Reynolds and Richmond, 1978), Child and
Adolescent Symptom Inventory-4 Anxiety Scale
(CASI-Anx) (Sukhodolsky et al., 2008), Screen for
Child Anxiety Related Disorders (SCARED)
(Birmaher et al., 1999), and Spence Children’s
Anxiety Scale for Parent or Child (SCAS-P/C)
(Spence, 1998).
2.4 Cohen’s d and Hedges’ g
This study used Cohen’s d and Hedges’ g to measure
the large of treatment effect. For the study that used
Cohen’s d, the values of d = 0.2 indicate small effect
size, d = 0.5 indicate moderate effect size, and d =
0.8 indicate large effect size. Meanwhile, for the
study that used Hedges’ g, the values of g < 0.5
indicate a small effect size, g = 0.5-0.8 indicate
moderate effect size, and g > 0.8 indicate a large
effect size. Hedges’ g was used, as it appropriate for
check biases due to small sample sizes which is not
covered under Cohen’s d (Cohen, 1988).
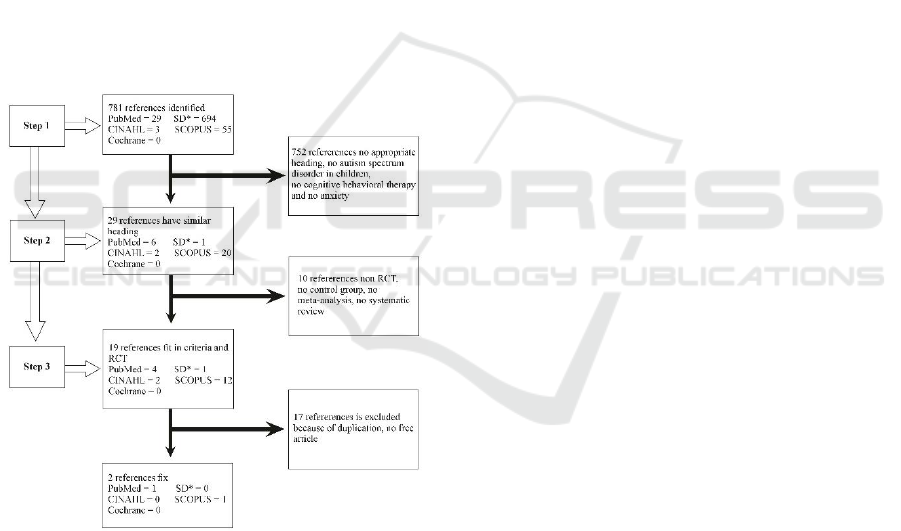
Note: SD* = ScienceDirect
Figure 1: Step-by-step search and selection strategies for
systematic review and meta-analysis of RCT of CBT for
anxiety in children with ASD.
3 RESULTS
3.1 Included and Excluded Trials
A total of 781 articles was identified through
electronic relevant databases of “PubMed”,
“CINAHL”, “Cochrane Library”, “Science Direct”,
and “SCOPUS”. Those articles were reviewed by
read the heading to find articles that fitted to
keyword. Seven hundred and fifty-two articles were
rejected and leaving only 29 articles whose titles
match the keywords. After inspection and check for
the abstract, 27 articles were excluded because they
did not meet the inclusion/ exclusion criteria and
were duplicates (see Fig. 1). The remaining 2
articles then were retrieved for further review. The
title of the articles selected were “a randomized
controlled trial of cognitive-behavioral therapy
versus treatment as usual for adolescents with autism
spectrum disorders and comorbid anxiety by Storch,
et al. (2015)” and “a systematic review and meta-
analysis of cognitive-behavioral therapy for anxiety
in youth with high-functioning autism spectrum
disorders by Ung, et al. (2015)”. Critical appraisal
tools such as Critical Appraisal Skills Programme
(CASP) (2013) was used to assess systematic review
and meta-analysis article and Oxford Centre for
Evidence Based Medicine (CEBM) (2005) was used
to assess RCTs article. All of the search and
selection processes were carried out by the two
authors for 2 weeks.
3.2 Participants
Collectively, the 15 studies of RCT (2 open trial)
that included had a total of 542 participants. Two
hundred ninety-nine participants received CBT and
243 participants as control group and received the
following: treatment as usual (TAU, n = 52),
waitlisted (WL, n = 172), or enrolled in the Social
Recreational Program (SR, n =34). The sample size
of the studies ranged from 6 to 71 participants with
range of age varies from 7 to 17 or under 18 years
(M = 11.92 years). Of the studies that reported
gender distribution, most of the participants were
male (n = 447, 83.4%) and the remaining
participants were female (n = 89, 16.6%).
Of the studies that reported ASD diagnosis
distribution among its participants, 205 (41.7%)
participants were diagnosed with Asperger’s
syndrome, 159 (32.3%) participants were diagnosed
with autistic disorder, 89 (18.1%) were diagnosed
with pervasive developmental disorder not otherwise
specified (PDD-NOS), and 39 (7.9%) participants
were labelled as “high functioning ASD”. In
established a true ASD diagnosis, both of studies
were same in applied a reliable measure of ASD by
used ADI-R, ADOS, or through medical records.
Of the studies that reported anxiety disorder
among its participants, 160 (32.3%) participants
Effectiveness of Cognitive Behavioral Therapy (CBT) to Reduce Anxiety in Children with Autism Spectrum Disorder (ASD): A Literature
Review
7

were reported suffer social phobia, 133 (26.9%)
participants were reported suffer generalized anxiety
disorder (GAD), 79 (15.9%) participants were
reported suffer separation anxiety disorder (SAD),
42 (8.5%) participants reported suffer obsessive-
compulsive disorder (OCD), and 81 (16.4%)
participants reported suffer other comorbid disorder
such as specific phobia, panic disorder, attention
deficit hyperactivity disorder (ADHD),
posttraumatic stress disorder (PTSD), etc.
Of the studies that reported medication usage
among its participants, the following medications
were reported: selective serotonin reuptake inhibitor
(SSRI) or anti-anxiety or anti-depressant (n = 81;
32.9%), stimulant, atomoxetine, or guanfacine (n =
65; 26.4%), atypical anti-psychotic (n = 39; 15.9%),
alpha blocker (n = 6; 2.4%), anti-convulsion (n = 5;
2%), trazodone or mood stabilizer (n = 2; 0.8%), and
other psychotic or non-psychotic medication that
were not specified (n = 48; 19.5%).
3.3 Intervention Characteristic
CBT periods lasted from 6-32 weeks (M = 15.4
weeks) with duration 60-120 minutes. Therapy was
given by therapists who are experienced and highly
trained in CBT, or clinical psychologists or doctoral
psychology students who have clinical experience of
at least 1 year in using CBT to deal with anxiety in
children. Eight studies conducted CBT in individual
child sessions with or without parents, six studies in
group sessions with or without parents, and one
study conducted CBT both, in individual and group
sessions.
In general CBT has a method composed of 6
components. However, in this study there were only
3 reported components, namely cognitive
restructuring, psychoeducation and coping
mechanisms. Specifically, there are themes that are
trained in psychoeducation such as recognition of
anxious feelings in oneself and others, recognition of
anxiety triggers, recognition of somatic reactions to
anxiety, and others. As for coping mechanisms, the
themes being trained include coping skills,
relaxation techniques, creating a hierarchy of fears,
exposure to feared stimuli, and developing social
skills. Sessions of the therapy were often taught
through role play, social stories, structured
worksheets, visual and video modelling, etc.
Treatment protocols used in CBT were based on
manual and/or books that modified CBT to be
appropriate for children with ASD. Of the studies
that reported treatment protocols, the following type
were reported: Cool Kids, Facing Your Fears,
Behavioral Intervention for Anxiety in Children with
Autism (BIACA), Coping Cat, Multimodal Anxiety
and Social Skills Intervention (MASSI), and
Exploring Feeling or Building Confidence.
Meanwhile, for the control group they were only
received treatment as usual (TAU; e.g., psychosocial
or pharmacological treatment or no seek treatment),
social recreational program or even as waitlist.
3.4 Dependent Variables
Two articles were selected and assessed critically
used similar treatment outcome measures. The
primary anxiety outcome measures that were used
included: Pediatric Anxiety Rating Scale (PARS),
Anxiety Disorders Interview Schedule for Child/
Parent or Clinical Severity Rating (ADIS-IV-C/P or
ADIS-IV-CSR), Clinical Global Impression-
Severity and Improvement scale (CGI-Severity,
CGI-Improvement), Multidimensional Anxiety
Scale for Children (MASC) or with Parent (MASC-
P), Revised Child Anxiety and Depression Scales
(RCADS), Revised Children’s Manifest Anxiety
Scale (RCMAS), Child and Adolescent Symptom
Inventory-4 Anxiety Scale (CASI-Anx), Screen for
Child Anxiety Related Disorders (SCARED), and
Spence Children’s Anxiety Scale for Parent or Child
(SCAS-P/C).
3.5 CBT Treatment Efficacy
CBT has proved reducing anxiety in children with
ASD. Of the two evidences, the result showed CBT
was statistically significant treatment to reduce
anxiety in children with ASD in moderate (d = 0.79;
g = -0.71 or -0.76 after removal of the two open trial
studies) to large effect size (d = 0.94-1.30). Effect
size did not significantly differ across anxiety
informant (among child (g = -0.60, 95% CI -1.17, -
0.03, z = -2.05, p < .05), parent (g = -0.82, 95% CI -
1.34, -0.30, z = -3.11, p < .01), or clinician (g = -
1.23, 95% CI -1.19, -0.55, z = -5.29, p < .001)) and
treatment modalities either in group sessions with or
without parents (g = -0.75, 95% CI -1.50, -0.003, z =
-1.97, p = .05) versus individual sessions with or
without parent (g = -0.62, 95% CI -0.92, -0.36, z = -
4.44, p < .01).
Based on the results of the diagnostic status
examination at post-treatment using the ADIS-C/P
instrument in the RCT study it was found that nearly
half (50%) of the participants in the treatment group
who received CBT had no longer experienced
anxiety, whereas in the control group who received
TAU, all participants were still experiencing
ICINNA 2018 - The 1st International Conference of Indonesian National Nurses Association
8

anxiety. Significant changes and improvements in
function were seen mainly in the subscale of
consciousness, cognition and communication. Based
on these results it can be concluded that a significant
effect was observed on the overall function of
autism by considering differences in measurement
results in parents and children after treatment.
Furthermore, significant differences between the
treatment and control groups were also detected in
the reduction in overall impairment of autism
function and the externalization of children's
behavior. However, based on the results of treatment
maintenance and re-examination one month after
treatment, there was no significant reduction
observed in anxiety on any measurement even
though significant improvements were detected in
the subscales of cognition, communication and
mannerism.
4 DISCUSSION
CBT is effective, acceptable and can be applied in
clinical setting since the effect size is moderate to
large. In study with RCTs, CBT was superior to
control waitlist, TAU, and social recreational
program and had a moderate effect size (g = -0.76).
This results were contrary with the previous study
that often reported lower treatment effect size
because of poor parent, clinician and child
diagnostic agreement on anxiety measures for
children (Ishikawa et al., 2007).
CBT as an alternative therapy has been
successful in reducing anxiety in children with ASD.
The success of this therapy in reducing anxiety may
be caused by the following two factors, namely the
CBT procedure which can be modified to match the
anxiety experienced by children with ASD, and the
CBT components implemented that contain high
cognitive and behavioral standards (Ung et al.,
2015). Treatment components adapted to meet the
needs of children with ASD reported by this review
were similar to the components reported by the
previous systematic reviews and meta-analyses (e.g.,
introspection, social skills development, use of
visual aids, systematic reinforcement, exposure to
feared stimuli, and creation of fear hierarchy). This
results suggest that these CBT components are still
commonly used to decrease anxiety in children.
The length of CBT’s session that was administer
until or over 32 weeks also factor that may
contribute to the successful reason of this therapy to
reduce anxiety in children with autism spectrum
disorder, as explained in the previous study (Fujii et
al., 2013). It is possible that the longer period of
CBT, the longer have had time to practice skills
learned, and the more robust effect of treatment. The
results of this review suggest that the length of time
span is an important factor that must be considered if
this therapy is expected to be able to give a positive
effect or even be applied to different settings.
The CBT program can be delivering by group
sessions or individual sessions with or without
parents. Both of this approaches are similarly
efficacious to reducing anxiety in children with
ASD. The results show the overlap in confidence
intervals revealed that they were not statistically
significant different. Ishikawa et al. (2007)
explained that implementation of CBT either
delivered in groups or individually with or without
parents not only provides benefits in the form of
normalization of anxiety symptoms through
increased adaptability. Moreover, the benefits can
also be seen in other aspects such as increased
motivation, acceptance, accountability, self-efficacy,
and support from peers or social. Another study
explained that CBT can help to alleviate impairment
and improving functional social responsiveness,
social skills, daily living skills, awareness, cognition
and communication (Storch et al., 2013, 2015).
CBT also has proved more safe and efficient than
pharmacotherapy. There were no reports that this
therapy is harmful. The cost-effectiveness analyses
results also have shown CBT seems a cost-effective
therapy to treat anxiety disorders in children with
ASD, if decreased anxiety level is used as an output
parameter (Van Steensel, Dirksen and Bögels,
2014).
5 CONCLUSIONS
CBT was statistically significant treatment to reduce
anxiety in children with ASD in moderate (d = 0.79;
g = -0.76) to large effect size (d = 0.94-1.30). Effect
size did not significantly differ reported among
child, parent or clinician. CBT is highly
recommended for children with ASD since this
therapy not only effective but also more safe and
cost effective.
REFERENCES
Birmaher, B. et al. (1999) ‘Psychometric properties of the
screen for child anxiety related emotional disorders
(SCARED): A replication study’, Journal of the
American Academy of Child & Adolescent Psychiatry,
Effectiveness of Cognitive Behavioral Therapy (CBT) to Reduce Anxiety in Children with Autism Spectrum Disorder (ASD): A Literature
Review
9

38(10), pp. 1230–1236. doi: 10.1097/00004583-
199910000-00011.
Chorpita, B. F., Moffitt, C. E. and Gray, J. (2005)
‘Psychometric properties of the revised child anxiety
and depression scale in a clinical sample’, Behaviour
Research and Therapy, 43(3), pp. 309–322. doi:
10.1016/j.brat.2004.02.004.
Cohen, J. (1988). Statistical power analysis for the
behavioural sciences, 2nd ed. Lawrence Erlbaum
Associates, Hillsdale.
Compton, S. N. et al. (2004) ‘Cognitive-behavioral
psychotherapy for anxiety and depressive disorders in
children and adolescents: An evidence-based medicine
review’, American Academy of Child and Adolescent
Psychiatry, 43(8), pp. 930–959. doi:
10.1097/01.chi.0000127589.57468.bf.
Danial, J. T. and Wood, J. J. (2013) ‘Cognitive behavioral
therapy for children with autism: Review and
considerations for future research’, Journal of
Developmental and Behavioral Pediatrics, 34(9), pp.
702–715. doi: 10.1097/DBP.0b013e31829f676c.
De Bruin, E. I. et al. (2007) ‘High rates of psychiatric co-
morbidity in PDD-NOS’, Journal of Autism and
Developmental Disorders, 37(5), pp. 877–886. doi:
10.1007/s10803-006-0215-x.
Dozois, D. J. A., and Dobson, K. S. (2001). Historical and
philosophical bases of the cognitive-behavioral
therapies. Dobson, Keith S. Handbook of Cognitive
Behavioral Therapies.
Fujii, C. et al. (2013) ‘Intensive cognitive behavioral
therapy for anxiety disorders in school-aged children
with autism: A preliminary comparison with
treatment-as-usual’, School Mental Health, 5(1), pp.
25–37. doi: 10.1007/s12310-012-9090-0.
Guy, W. (1976). Clinical global impressions, in ECDEU
assessment manual for psychopharm acology.
National Institute for Mental Health, Rockville.
Hanson, E. et al. (2007) ‘Use of complementary and
alternative medicine among children diagnosed with
autism spectrum disorder’, Journal of Autism and
Developmental Disorders, 37(4), pp. 628–636. doi:
10.1007/s10803-006-0192-0.
Ishikawa, S. I. et al. (2007) ‘Cognitive behavioural
therapy for anxiety disorders in children and
adolescents: A meta-analysis’, Child and Adolescent
Mental Health, 12(4), pp. 164–172. doi:
10.1111/j.1475-3588.2006.00433.x.
Leyfer, O. T. et al. (2006) ‘Comorbid psychiatric disorders
in children with autism: Interview development and
rates of disorders’, Journal of Autism and
Developmental Disorders, 36(7), pp. 849–861. doi:
10.1007/s10803-006-0123-0.
March, J. (1998). Manual for the multidimensional anxiety
scale for children. Mult-Health Systems, Toronto.
March, P. and Schub, T. (2016) ‘Autism spectrum
disorder: Quick lesson’, Cinahl Information Systems.
Muris, P. et al. (1998) ‘Comorbid anxiety symptoms in
children with pervasive developmental disorders’,
Journal of Anxiety Disorders, 12(4), pp. 387–393. doi:
PII S0887-6185(98)00022-X.
Reynolds, C. R. and Richmond, B. O. (1978) ‘What I
think and feel: A revised measure of children’s
manifest anxiety’, Journal of Abnormal Child
Psychology, 6(2), pp. 271–280. doi:
10.1207/s15327752jpa4303.
Shaker-Naeeni, H., Govender, T. and Chowdhury, U.
(2014) ‘Cognitive behavioural therapy for anxiety in
children and adolescents with autism spectrum
disorder’, British Journal of Medical Practitioners,
7(3). Available at: http://www.embase.com/search/
results?subaction=viewrecord&from=export&id=L600
271161.
Siegel, B. et al. (2014) ‘Autism spectrum disorders’,
Encyclopedia of the Neurological Sciences, 1, pp.
339–341. doi: 10.1016/B978-0-12-385157-4.01067-8.
Silverman, W. K., and Albano A. M. (1996). The anxiety
disorders interview schedule for DSM-IV—child and
parent versions. Psychological Corporation, San
Antonio.
Simonoff, E. et al. (2008) ‘Psychiatric disorders in
children with autism spectrum disorders: Prevalence,
comorbidity, and associated factors in a population-
derived sample’, Journal of American Academy of
Child and Adolescent Psychiatry, 47(8), pp. 921–929.
doi: 10.1097/CHI.0b013e318179964f.
Spence, S. H. (1998) ‘A measure of anxiety symptoms
among children’, Behaviour Research and Therapy,
36(5), pp. 545–566. doi: 10.1016/s0005-
7967(98)00034-5.
Sterling, L. et al. (2015) ‘Validity of the revised children’s
anxiety and depression scale for youth with autism
spectrum disorders’, Autism, 19(1), pp. 113–117. doi:
10.1177/1362361313510066.
Storch, E. A. et al. (2013) ‘The effect of cognitive-
behavioral therapy versus treatment as usual for
anxiety in children with autism spectrum disorders: A
randomized, controlled trial’, Journal of the American
Academy of Child and Adolescent Psychiatry.
Elsevier, 52(2), p. 132–142.e2. doi:
10.1016/j.jaac.2012.11.007.
Storch, E. A. et al. (2015) ‘A randomized controlled trial
of cognitive-behavioral therapy versus treatment as
usual for adolescents with autism spectrum disorders
and comorbid anxiety’, Depression and Anxiety, 32(3),
pp. 174–181. doi: 10.1109/CCDC.2016.7531585.
Sukhodolsky, D. G. et al. (2008) ‘Parent-rated anxiety
symptoms in children with pervasive developmental
disorders: Frequency and association with core autism
symptoms and cognitive functioning’, Journal of
Abnormal Child Psychology, 36(1), pp. 117–128. doi:
10.1007/s10802-007-9165-9.
Sukhodolsky, D. G. et al. (2013) ‘Cognitive-behavioral
therapy for anxiety in children with high-functioning
autism: A meta-analysis’, Pediatrics, 132(5), pp.
e1341–e1350. doi: 10.1542/peds.2013-1193.
The Research Units On Pediatric Psychopharmacology
Anxiety Study Group (2002) ‘The pediatric anxiety
rating scale (PARS): Development and psychometric
properties’, Journal of the American Academy of Child
ICINNA 2018 - The 1st International Conference of Indonesian National Nurses Association
10

and Adolescent Psychiatry, 41(9), pp. 1061–1069. doi:
10.1097/00004583-200209000-00006.
Ung, D. et al. (2015) ‘A systematic review and meta-
analysis of cognitive-behavioral therapy for anxiety in
youth with high-functioning autism spectrum
disorders’, Child Psychiatry & Human Development.
Springer US, 46(4), pp. 533–547. doi:
10.1007/s10578-014-0494-y.
Van Steensel, F. J. A., Dirksen, C. D. and Bögels, S. M.
(2014) ‘Cost-effectiveness of cognitive-behavioral
therapy versus treatment as usual for anxiety disorders
in children with autism spectrum disorder’, Research
in Autism Spectrum Disorders, 8(2), pp. 127–137. doi:
10.1016/j.rasd.2013.11.001.
Effectiveness of Cognitive Behavioral Therapy (CBT) to Reduce Anxiety in Children with Autism Spectrum Disorder (ASD): A Literature
Review
11
