
The Effects of Sociocultural Pressures, BMI, Weight Perception and
Body Dissatisfaction on Unhealthy Weight Control Behaviors among
Indonesian Adolescent Girls
Monique Elizabeth Sukamto
1,2
, Fajrianthi
1
, Darmawan Muttaqin
2
and Hamidah
1
1
Faculty of Psychology, Universitas Airlangga
2
Faculty of Psychology, Universitas Surabaya
hamidah}@psikologi.unair.ac.id
Keywords : dieting behaviors, disordered eating, weight concern, body image.
Abstract : Weight control behaviors are prevalent among adolescent girls due to the motivation to avoid obesity and to
improve appearance. While some girls use healthy strategies, others may engage in unhealthy or more
extreme weight control behaviors (UWCBs). A broad range of studies suggested that adolescents engaging
in UWCBs were at risk of a variety of negative consequences, such as greater weight gain and the
development of clinical eating disorders. This study examined a theoretical model of the effects of
sociocultural pressures, body mass index (BMI) and weight perception on unhealthy weight control
behaviors via the mediation of body dissatisfaction among Indonesian adolescent girls. A total of 206 girls
completed a questionnaire assessing sociocultural pressures, weight status, weight perception, body
dissatisfaction and unhealthy (and extreme) weight control behaviors. A structural equation modeling was
conducted to test a hypothetical model. The final model indicated a good fit to the data, with body
dissatisfaction mediating the effects of sociocultural pressures, BMI and weight perception on unhealthy
weight control behaviors. Weight perception also had direct effects on unhealthy and extreme weight
control behaviors. Further exploration of the resulting model may contribute to the refinement of
intervention programs for weight control problems.
1 INTRODUCTION
Weight control or dieting behaviors are prevalent
among adolescents, particularly adolescent girls.
While some girls using healthy weight control
behaviors, such as exercising, eating more fruit and
vegetables or eating less high-fat food, unhealthy
weight control behaviors, such as skipping meals,
eating very little food, fasting or more extreme
behaviors, including taking diet pills, using laxatives
or self-induced vomiting are also common
(Grunbaum et al., 2002; Lampard et al., 2016; Lee
and Lee, 2016; Lõpez-Guimerà et al., 2013;
Neumark-Sztainer et al., 1999; Ojala et al., 2007;
Quick et al., 2013).
A broad range of studies indicate that unhealthy
and extreme weight control behaviors can lead to
negative consequences, such as inadequate nutrition
intake (Neumark-Sztainer et al., 2004), greater
weight gain, overweight status (Field et al., 2010;
Neumark-Sztainer et al., 2012; Stice et al., 2005),
and the development of clinical eating disorders
(Neumark-Sztainer, 2009; Neumark-Sztainer et al.,
2006b; Patton et al., 1999). In addition, Neumark-
Sztainer et al. (2011) indicated that disordered
eating behaviors occurring in adolescence would
continue to be prevalent in young adulthood.
In light of the prevalence of unhealthy weight
control behaviors among adolescent girls and their
negative consequences, an understanding of the
etiological processes leading to unhealthy or
extreme weight control behaviors is indispensable. A
growing number of studies in different countries
(e.g. United States, Hungary, Australia) have
empirically tested theoretical models explaining
dieting behaviors, unhealthy weight control
behaviors or disordered eating behaviors among
adolescent girls, using either structural equation
modeling (SEM) or path analysis (Neumark-Sztainer
et al., 2003; Keery, van den Berg & Thompson,
2004; Shroff & Thompson, 2006; Matera, Nerini &
Stefanile, 2013; Papp et al., 2013; Armstrong,
140
Sukamto, M., Muttaqin, D., Fajrianthi, . and Hamidah, .
The Effects of Sociocultural Pressures, BMI, Weight Perception, and Body Dissatisfaction on Unhealthy Weight Control Behaviors among Indonesian Adolescent Girls.
DOI: 10.5220/0008586401400148
In Proceedings of the 3rd International Conference on Psychology in Health, Educational, Social, and Organizational Settings (ICP-HESOS 2018) - Improving Mental Health and Harmony in
Global Community, pages 140-148
ISBN: 978-989-758-435-0
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Westen & Janicke, 2014; Rodgers, Paxton &
McLean, 2014; Rodgers, McLean & Paxton, 2015).
For example, Neumark-Sztainer et al. (2003) found
a model that explained 76% of the variance in
unhealthy weight control behaviors among US girls.
In addition, Rodgers et al. (2014) examined a
biopsychosocial model that accounted for a very
large proportion of the variance in body image
concerns (87%) and a large proportion of variance in
dietary restraint (50%) among Australian girls.
Several studies in Indonesia focusing on dieting
or weight control behaviors among adolescent girls
(Lintang, Ismanto and Onibala, 2015; Prima and
Sari, 2013; Sulistyan, Huryati and Hastuti, 2016)
have shown that unhealthy dieting behaviors are also
common. For example, Sulistyan et al. (2016) found
that among girls who were trying or had tried to lose
weight, 92% of girls were using unhealthy dieting
(fad diets). However, to date, studies focusing on
explorations of an integrative model of the
development of unhealthy weight control behaviors
or disordered eating behaviors in Indonesia are still
lacking.
The aim of the present study is to examine a
theoretical model explaining unhealthy and extreme
weight control behaviors among Indonesian
adolescent girls. In this hypothetical model, we
deliberately distinguish unhealthy weight control
behaviors from extreme behaviors due to their
differences in severity and impact for health so that
we can explore the possible different pathways of
influence of these two types of behaviors. In
addition, previous research has shown that unhealthy
weight control behaviors are more common than
extreme behaviors (Bucchianeri et al., 2016; Haley,
Hedberg and Leman, 2010; Thøgersen-Ntoumani,
Ntoumanis and Nikitaras, 2010; Vander Wal, 2011),
thus allowing different pathways of influence.
In this model, we also incorporate sociocultural
pressures, BMI and weight perception hypothesized
to have an effect on body dissatisfaction, and
unhealthy and extreme weight control behaviors.
Based on previous research among adolescent girls,
sociocultural pressures from family, peers and media
are hypothesized to predict unhealthy and extreme
weight control behaviors either directly or indirectly
through their influence on body dissatisfaction
(Keery, van den Berg and Thompson, 2004;
Neumark-Sztainer et al., 2003; Rodgers, Paxton and
McLean, 2014; Shroff and Thompson, 2006). Given
the increasing popularity of social media, we add it
as another source of sociocultural pressures in this
study. Additionally, research on social media
(Facebook and Instagram) has shown that Facebook
or Instagram usage had a correlation with body
image concerns (Brown and Tiggemann, 2016;
Fardouly and Vartanian, 2015; Tiggemann and
Miller, 2010).
Body dissatisfaction, the negative evaluation of
part or all of one’s body, is among the most
consistent and robust risk factors for the
development of dieting and eating pathology (Stice,
2002; Bucchianeri et al., 2016). Based on previous
research (Keery, van den Berg and Thompson, 2004;
Matera, Nerini and Stefanile, 2013; Neumark-
Sztainer et al., 2003; Papp et al., 2013; Shroff and
Thompson, 2006; Thøgersen-Ntoumani, Ntoumanis
and Nikitaras, 2010), body dissatisfaction is
hypothesized to have a direct influence on unhealthy
or extreme weight control behaviors.
BMI and weight perception are hypothesized to
have either a direct effect on unhealthy and extreme
weight control behaviors or indirect effect through
their influence on body dissatisfaction. Previous
research has found that BMI was a risk factor for
body dissatisfaction and dieting (Al Sabbah et al.,
2010; Gonsalves, Hawk and Goodenow, 2014;
Lampard et al., 2016; Matera, Nerini and Stefanile,
2013; Neumark-Sztainer et al., 2003; Rodgers,
Paxton and McLean, 2014; Stice, 2002; Vander Wal,
2011). BMI is also hypothesized to have an effect on
sociocultural pressures. Elevated adiposity, which
can be calculated through BMI, is thought to have an
effect on stronger pressure from family and peers to
be thinner, that may range from negative comments
about weight to attempts to limit the caloric intake of
children (Stice, 2002). Evidence from previous
studies has also revealed strong associations
between weight perception and body dissatisfaction
and dieting or weight control behaviors (Armstrong,
Westen and Janicke, 2014; Gonsalves, Hawk and
Goodenow, 2014; Haley, Hedberg and Leman, 2010;
Lee and Lee, 2016; Papp et al., 2013; Vander Wal,
2011). In a previous model, Papp et al. (2013)
indicated that weight perception was a better
predictor of body dissatisfaction than BMI. In
addition, Papp et al. also noted that weight
perception partially mediated the relationship
between BMI and restriction among Hungarian
adolescent girls. Therefore, in this study, it is also
interesting to explore the influence of BMI and
weight perception on body dissatisfaction and
unhealthy and extreme weight control behaviors
among Indonesian adolescent girls. Thus, the
specific study objectives were: (a) to examine a
theoretical model that explained
The Effects of Sociocultural Pressures, BMI, Weight Perception, and Body Dissatisfaction on Unhealthy Weight Control Behaviors among
Indonesian Adolescent Girls
141

Figure 1: Hypothetical model.
unhealthy and extreme weight control behaviors
separately in Indonesian adolescent girls; (b) to
determine how much variance in body
dissatisfaction, unhealthy, and extreme weight
control behaviors could be explained by factors
included in the model; (c) to determine whether
weight status (BMI) or weight perception had a
stronger effect on unhealthy and extreme weight
control behaviors. The hypothetical model is shown
in Figure 1.
2 METHODS
2.1 Participants
A sample of 206 adolescent girls was recruited from
a public middle school (47.1%) and a public high
school (52.9%) from an urban school district in
Surabaya, Indonesia to complete the surveys. The
majority ethnic background of the participants was
Javanese (95.1%). The remaining were Madurese
(1%), Balinese (1%) and mixed or other (2.9%).
2.2 Procedures
The sampling technique used in this study was
convenience sampling where samples were taken
from a group of people who were easily reached.
Female students from participating schools were
invited to participate in the study and completed a
set of questionnaires. Participants also completed a
brief demographics questionnaire asking them to
denote their age, grade, ethnicity, height, weight and
weight perception. Data collection was conducted in
classroom settings and supervised by the
researchers. Informed consent was obtained prior to
administration of the questionnaire packet. The
participants were told that the study concerned their
dieting or weight control behaviors.
2.3 Measures
The first author performed forward translation of all
of the measures into Indonesian. The translator was
a psychologist who was familiar with terminology of
the area covered by the instruments and was
knowledgeable of the English-speaking culture and
Indonesian language culture. This translation
emphasized conceptual translation rather than literal
translation, and the need to use language that was
natural and understandable to participants.
2.3.1 Unhealthy Weight Control Behaviors
Unhealthy weight control behaviors were assessed
using an Indonesian version of a questionnaire
developed by Neumark-Sztainer et al. (2003) and
Mayer-Brown et al. (2016). Unhealthy weight
control behaviors were divided into two sub-scales,
i.e. unhealthy behaviors and extreme behaviors. In
previous studies mostly conducted in the US,
‘smoking more cigarettes’ was categorized in
unhealthy behaviors (Lampard et al., 2014;
Bucchianeri et al., 2016; Lõpez-Guimerà et al.,
2013; Quick et al., 2013). However, the first author's
previous work among Indonesian adolescent girls
using exploratory factor analysis (EFA) found that
‘smoking more cigarettes’ for the purpose of dieting
had a high primary loading in extreme behaviors and
no secondary loading in unhealthy behaviors
(Sukamto, 2017). Therefore, ‘smoking more
cigarettes’ was grouped in extreme behaviors in this
study. Participants were asked to indicate whether or
not they had engaged in each of the four unhealthy
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
142

behaviors (e.g. fasting, eating very little food, using
a food substitute, skipping meals) and five extreme
behaviors (e.g. smoking more cigarettes, taking diet
pills, self-induced vomiting, using laxatives, using
diuretics) to lose weight or keep from gaining
weight during the past year (yes or no for each
method). All “yes” responses were summed to
obtain a total score. If an item was endorsed with
“yes”, then participants were asked to indicate how
often they engaged in the behavior on a 5-point
Likert scale, ranging from “one time” to “every
day”. The frequency of each behavior endorsed was
summed for each participant. In the current sample,
the Cronbach’s alpha was .535 for unhealthy
behaviors sub-scale, whereas for extreme behaviors
sub-scale, the alpha was .890.
2.3.2 Sociocultural Pressures
This present study used the modified Indonesian
version of the family, peers, and media pressures
sub-scales of the Sociocultural Attitudes Towards
Appearance Questionnaire-4 (SATAQ-4; Schaefer et
al., 2015). This modified version consisted of four
sub-scales assessing participants’ perception of
appearance-related pressures from different sources
such as media, family, friends and social media. The
social media pressures sub-scale was added in this
study due to the increasing popularity of social
media (e.g. Facebook, Instagram) among adolescent
girls. In this current study, each sub-scale consisted
of two items that were rated on a 4-point Likert-type
scale ranging from 1 (definitely disagree) to 4
(definitely agree) and summed to get the total
sociocultural pressures score. Higher scores
indicated greater perceived appearance-related
pressures. An example item was “I feel pressure
from the media to look thinner”. In the present
sample, the Cronbach’s alpha was .863.
2.3.3 Body Mass Index (BMI)
BMI was calculated from each participant’s self-
reported weight and height (kg/m
2
).
2.3.4 Weight Perception
Girls’ weight perception was assessed by asking
participants if they perceived their weight as
underweight (1), normal weight (2) or overweight
(3). Responses were then divided into three
categories.
2.3.5 Body Dissatisfaction
Body dissatisfaction was assessed using a modified
Indonesian version of the Body Shape Satisfaction
scale (Pingitore et al., 1997) which consisted of
seven items. Participants rated their satisfaction with
different body elements (i.e. body weight, body
shape, waist, hips, thighs, stomach and overall body
fat) with four Likert responses ranging from very
dissatisfied (1) to very satisfied (4). Items were
reversed scored and summed. Higher scores
indicated greater body dissatisfaction (range = 7 to
28; Cronbach’s α = .887.
2.4 Data Analysis
We used SPSS 21 to calculate internal consistencies
(Cronbach’s alphas), means and standard deviations
for all the scales. We also used SEM to test the
hypothetical model with Amos 21 software
(Arbuckle, 2012). Before relevant pathways between
the factors were examined, confirmatory factor
analysis (CFA) using maximum likelihood
estimation was conducted to test the fit of the
measurement model. After testing the fit of the
measurement model and making appropriate
modifications, we tested the structural model.
Model fit was examined using multiple fit
indices including the χ
2
/df ratio, root mean square
error of approximation (RMSEA), comparative fit
index (CFI), and Tucker-Lewis Index (TLI). Good
model fit was defined by the following criteria: χ
2
/df
ratio below 3.0 (Hair et al., 2010), RMSEA values of
around .08 or below (Browne and Cudeck, 1992),
CFI values of .90 or higher (Bentler, 1990), and TLI
values above around .90 (Hu and Bentler, 1999).
Modification indices and theory were used in order
to guide model improvement.
3 RESULTS
3.1 Prevalence of Unhealthy Weight
Control Behaviors
The use of unhealthy weight control behaviors
(UWCBs) over the past year was reported by 78.2%
of participants. In this current study, UWCBs were
divided into unhealthy and extreme behaviors.
Percentages of girls who reported the use of
unhealthy weight control behaviors over the past
year were as follows: ate very little food (64%);
skipped meals (48%); fasted (31%) and used food
substitutes (26%). Girls who reported engaging in
The Effects of Sociocultural Pressures, BMI, Weight Perception, and Body Dissatisfaction on Unhealthy Weight Control Behaviors among
Indonesian Adolescent Girls
143

extreme weight control behaviors were: self-induced
vomiting (3%); used laxatives (3%); took diet pills
(2%); took diuretics (1%). Yet, only one participant
chose ‘smoking more cigarettes’ as her weight
control strategy.
In the current sample, the mean age of
participants was 14.861 years (SD = 1.514). The
mean of BMI was 20.826 (SD = 4.460), while the
mean of weight perception was 2.252 (SD = 0.729).
The mean for the overall sociocultural pressures
scale was 17.961 (SD = 5.903). The mean scores
were 18.893 (SD = 3.933) for body dissatisfaction,
5.248 (SD = 4.204) for unhealthy behaviors sub-
scale, and 0.291 (SD = 1.859) for extreme behaviors.
3.2 Measurement Models
The CFA for unhealthy and extreme weight control
behaviors indicated a good model fit according to
the criteria (χ
2
/df = 1.956, RMSEA = .068, CFI =
.968, TLI = .955). Similarly for body dissatisfaction,
model-testing statistics suggested that the model
fitted the data well (χ
2
/df = 1.944, RMSEA = .068,
CFI = .987, TLI = .973). The model of sociocultural
pressures also indicated a good fit with the data
according to the criteria (χ
2
/df = 1.299, RMSEA =
.038, CFI = .997, TLI = .991).
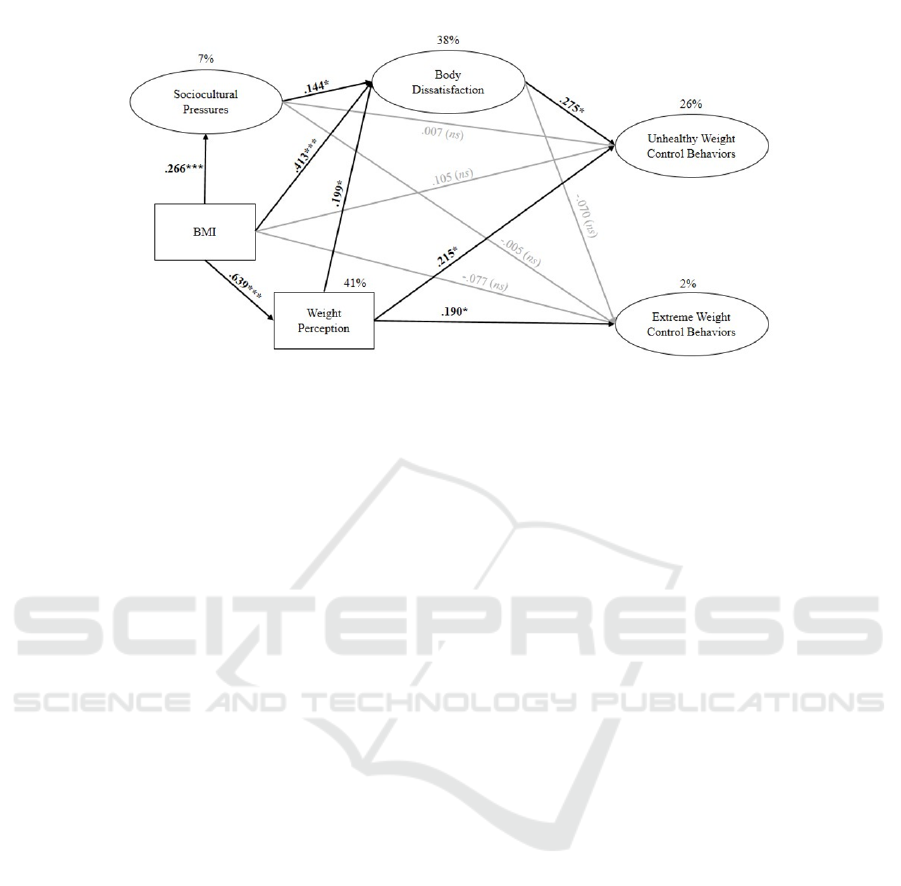
3.3 Structural Model
The testing of the hypothetical model (see Figure 2)
revealed good model fit according to the χ
2
/df
ratio,
RMSEA, CFI, and TLI (χ
2
/df
= 1.640, RMSEA =
.056, CFI = .939, TLI = .927). There were no
modification indices suggested to improve the fit of
the model. This SEM model explained 38% of the
variance in body dissatisfaction, 26% of the variance
in unhealthy weight control behaviors and only
explained 2% of the variance in extreme weight
control behaviors among adolescent girls.
Statistically significant pathways were found
between body dissatisfaction and unhealthy weight
control behaviors; between sociocultural pressures
and body dissatisfaction; between BMI and
sociocultural pressures, body dissatisfaction and
weight perception; and between weight perception
and body dissatisfaction, unhealthy weight control
behaviors and extreme weight control behaviors.
None of the direct pathways from sociocultural
pressures to both unhealthy and extreme weight
control behaviors was statistically significant; rather,
its effect on unhealthy weight control behaviors was
mediated by body dissatisfaction. Likewise, the
direct pathways from BMI to both unhealthy and
extreme weight control behaviors were not
statistically significant. The effect of BMI on
unhealthy weight control behaviors was mediated by
weight perception and body dissatisfaction and its
effect to extreme behaviors was only mediated by
weight perception. The effect of weight perception
on unhealthy weight control behaviors was partially
mediated via body dissatisfaction because there was
also a significant direct path to unhealthy behaviors.
Weight perception was the only variable that had a
significant direct effect on extreme weight control
behaviors.
4 DISCUSSION
The aim of the present study was to examine a
model explaining unhealthy and extreme weight
control behaviors among a sample of Indonesian
adolescent girls. Based on the data of weight
perception in this study, it was found that
participants were more likely to perceive their
weight as normal or overweight. Body weight
perception refers to personal evaluation of one’s
weight as “underweight,” “normal weight” or
“overweight” regardless of the actual body mass
index. Findings from previous studies (Armstrong,
Westen and Janicke, 2014; Gonsalves, Hawk and
Goodenow, 2014; Papp et al., 2013; Vander Wal,
2011) showed that adolescent girls who perceived
themselves as overweight were more likely to
engage in unhealthy or extreme weight control
behaviors than those who perceived they were about
the right weight.
Findings of this study also showed that sociocultural
pressures were quite high in the participants. This
indicated that adolescent girls perceived a great
pressure from family, peers, media and social media
to be thinner in order to meet the social expectations
associated with beauty and attractiveness. There is
strong evidence that sociocultural influences that
range from direct social interactions such as
conversations with peers and parents, mass media
communication which comes from television shows,
magazines, radio, advertisements, music videos, to
interactive social media such as Facebook and
Twitter, are significant in determining young
people's standards of beauty and appearance
(Wertheim and Paxton, 2012). Dissatisfaction with
one’s body can range from a mild preference for
different body characteristics to severe distress and
extreme actions to change the body. Most studies in
adolescent girls have examined body image and
dissatisfaction associated with weight and shape
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
144
concerns (Wertheim and Paxton, 2012). Based on the result of body dissatisfaction in this study, it was
Figure 2: SEM model with standardized path coefficients. Note: bold numbers correspond to standardized path coefficients,
while non-bold numbers correspond to the explained variance for each variable; grey arrows indicate nonsignificant paths.
found that the participants’ dissatisfaction with their
body was quite high. Dissatisfaction with body
weight and shape often leads to attempts to lose
weight, potentially resulting in unhealthy eating,
dieting and/or exercise patterns, and ultimately
clinical eating disorders (Tiggemann, 2012).
The testing of the hypothetical model proved to
be a good fit for the data (Figure 2) and explained
38% of the variance in body dissatisfaction, 26% of
the variance in unhealthy weight control behaviors
and only 2% of the variance in extreme weight
control behaviors. That this model only explained
2% of the variance in extreme weight control
behaviors might be due to the very small prevalence
of Indonesian adolescent girls who engaged in
extreme weight control behaviors. The prevalence of
self-induced vomiting, using laxatives and diuretics
and taking diet pills each was only below 4%. This
small prevalence indicated that there were still very
few Indonesian adolescent girls in this sample who
chose high-risk strategies to control their weight.
Interestingly, there was only one adolescent girl in
this sample who chose smoking more cigarettes as
her weight control strategy. This may be due to
cultural values in Indonesia that tend to perceive
women who smoke negatively, such as naughty,
wild and endangering their own health (Menurut
pendapatmu: Memang benar, cewek perokok itu
nggak bermoral?, 2014; Siamti, 2017).
In our model, there were four mediated pathways
to explain the effect of BMI on unhealthy weight
control behaviors, i.e.: (1) via sociocultural pressures
and body dissatisfaction, (2) via body
dissatisfaction, (3) via weight perception and body
dissatisfaction and (4) via weight perception.
However, there was no significant direct path
between BMI and unhealthy weight control
behaviors. Previous studies were consistent with our
finding that BMI had an indirect effect on unhealthy
weight control behaviors (Neumark-Sztainer et al.,
2003), dieting (Matera, Nerini & Stefanile, 2013),
and dietary restraint (Rodgers, Paxton & McLean,
2014) through body dissatisfaction. Another
previous study (Papp et al., 2013) supported our
findings that the effect of BMI on unhealthy weight
control behaviors was mediated by weight
perception and body dissatisfaction. The study by
Papp et al. (2013) among Hungarian adolescents
indicated that the objective nutritional state leads to
body dissatisfaction and restriction through the
subjective perception of body weight in both
genders. Previous study pointed out that restriction
is a potential risk factor for unhealthy weight
control behaviors in adolescence (Neumark-Sztainer
et al., 2006a). In addition, this study also found that
BMI had a direct effect on sociocultural pressures
and body dissatisfaction. According to Stice (2002),
elevated adiposity can lead to greater pressure from
family and peers to be thinner that may range from
negative comments about weight to attempts to limit
the caloric intake of children. Elevated adiposity is
also likely to contribute to body dissatisfaction
because the prevailing cultural standards for
attractiveness favor thinness.
The effect of sociocultural pressures on
unhealthy weight control behaviors was fully
mediated via body dissatisfaction and no direct
pathway was significant. A previous model
(Neumark-Sztainer et al., 2003) among adolescent
girls also found that family-peer weight norms and
The Effects of Sociocultural Pressures, BMI, Weight Perception, and Body Dissatisfaction on Unhealthy Weight Control Behaviors among
Indonesian Adolescent Girls
145

family connectedness had an indirect effect on
unhealthy weight control behaviors, but through
weight-body concerns (body dissatisfaction). In our
model, sociocultural pressures were measured as an
overall pressure, so the effect of each pressure
(family, peers, media and social media) cannot be
predicted. According to Stice (2002), elevated
pressure to be thin from family, peers and media can
lead to body dissatisfaction, as repeated messages
that one is not thin enough likely causes discontent
with one’s body.
Our model explained 38% of the variance in
body dissatisfaction and body dissatisfaction had a
significantly direct path to unhealthy weight control
behaviors. Body dissatisfaction leads to dieting
because of the belief that this is an effective weight
control technique (Stice 2002). This finding is also
supported by previous studies showing that body
dissatisfaction had a significantly direct effect on
restriction (Keery, van den Berg and Thompson,
2004; Shroff and Thompson, 2006; Papp et al.,
2013), dietary restraint (Rodgers, Paxton and
McLean, 2014), dieting (Matera, Nerini and
Stefanile, 2013), and unhealthy weight control
behaviors (Neumark-Sztainer et al., 2003;
Thøgersen-Ntoumani, Ntoumanis and Nikitaras,
2010).
The present study has a number of limitations.
First, our study relied on participants’ self-reports of
their weight and height when computing their BMIs.
Second, the sub-scale of unhealthy weight control
behaviors still had lower than ideal reliability
coefficient in the current sample. Third, this study
used a composite sociocultural pressures variable,
and thus could not identify the effect of each source
of pressure. Fourth, the appearance comparisons and
internalization of thin ideal which were found to be
important mediational factors in previous studies
(Keery, van den Berg and Thompson, 2004; Shroff
and Thompson, 2006; Rodgers, Paxton and McLean,
2014) were still not included in the current model.
However, despite these limitations, the current
study is able to reveal potential risk factors
contributing to the development of unhealthy and
extreme weight control behaviors among Indonesian
adolescent girls. The study should be of high priority
since the prevalence of unhealthy weight control
behaviors among adolescent girls in Indonesia is
quite high. The still limited number of studies
investigated their risk factors, and the negative
consequences of these behaviors, such as obesity
and eating disorders. Implications for future studies
could include examining sociocultural pressures,
including family, peers, media and social media,
separately and other influential factors relating to
unhealthy weight control behaviors. Future study
should also continue to investigate the psychometric
properties of the unhealthy weight control behaviors
sub-scale in more diverse samples of Indonesian
adolescent girls. Moreover, although our sample size
was sufficient, a larger sample might improve the
statistical power and identify the prevalence of
unhealthy and extreme weight control behaviors
among Indonesian adolescent girls more accurately.
5 CONCLUSIONS
Our study demonstrated the importance of including
sociocultural pressures, biological factor (BMI), and
psychological factors (weight perception and body
dissatisfaction) in a model explaining unhealthy and
extreme weight control behaviors among Indonesian
adolescent girls. Further research is required to
investigate other influential factors relating to
unhealthy and extreme weight control behaviors so
that we can provide an insight for developing more
effective prevention programs to overcome this
problem.
REFERENCES
Anon 2014. Menurut Pendapatmu: Memang Benar,
Cewek Perokok Itu Nggak Bermoral? hipwee
community.
Anon n.d. Menurut Pendapatmu: Memang Benar, Cewek
Perokok Itu Nggak Bermoral? hipwee community.
Arbuckle, J.L., 2012. IBM SPSS Amos 21 user’s guide.
Armstrong, B., Westen, S.C. and Janicke, D.M., 2014. The
role of overweight perception and depressive
symptoms in child and adolescent unhealthy weight
control behaviors: A mediation model. Journal of
Pediatric Psychology, 39(3), pp.340–348.
Bentler, P.M., 1990. Comparative fit indexes in structural
models. Psychological Bulletin, 107(2), pp.238–246.
Brown, Z. and Tiggemann, M., 2016. Attractive celebrity
and peer images on Instagram: Effect on women’s
mood and body image. Body Image, 19.
Browne, M.W. and Cudeck, R., 1992. Alternative Ways of
Assessing Model Fit. Sociological Methods &
Research, 21(2), pp.230–258.
Bucchianeri, M.M., Fernandes, N., Loth, K., Hannan, P.J.,
Eisenberg, M.E. and Neumark-Sztainer, D., 2016.
Body dissatisfaction: Do associations with disordered
eating and psychological well-being differ across
race/ethnicity in adolescent girls and boys? Cultural
Diversity and Ethnic Minority Psychology, 22(1),
pp.137–146.
Fardouly, J. and Vartanian, L.R., 2015. Negative
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
146

comparisons about one’s appearance mediate the
relationship between Facebook usage and body image
concerns. Body Image, 12(1), pp.82–88.
Field, A.E., Haines, J., Rosner, B. and Willett, W.C.,
2010. Weight-control behaviors and subsequent
weight change among adolescents and young adult
females 1 – 3. American Journal of Clinical Nutrition,
91(4), pp.147–153.
Gonsalves, D., Hawk, H. and Goodenow, C., 2014.
Unhealthy weight control behaviors and related risk
factors in massachusetts middle and high school
students. Maternal and Child Health Journal, 18(8),
pp.1803–1813.
Grunbaum, J.A., Kann, L., Kinchen, S. a, Williams, B.,
Ross, J.G., Lowry, R. and Kolbe, L., 2002. Youth Risk
Behavior Surveillance - United States, 2001. Journal
of School Health, 72(8), pp.313–328.
Hair, J.F., Black, W.C., Babin, B.J. and Anderson, R.E.,
2010. Multivariate Data Analysis. Seventh Ed ed.
Pearson Prentice Hall.
Haley, C.C., Hedberg, K. and Leman, R.F., 2010.
Disordered Eating and Unhealthy Weight Loss
Practices: Which Adolescents Are at Highest Risk?
Journal of Adolescent Health, 47(1), pp.102–105.
Hu, L.T. and Bentler, P.M., 1999. Cutoff criteria for fit
indexes in covariance structure analysis: Conventional
criteria versus new alternatives. Structural Equation
Modeling, 6(1), pp.1–55.
Keery, H., van den Berg, P. and Thompson, J.K., 2004. An
evaluation of the Tripartite Influence Model of body
dissatisfaction and eating disturbance with adolescent
girls. Body Image, 1(3), pp.237–251.
Lampard, A.M., Maclehose, R.F., Eisenberg, M.E.,
Larson, N.I., Davison, K.K. and Neumark-Sztainer,
D., 2016. Adolescents who engage exclusively in
healthy weight control behaviors: Who are they? The
international journal of behavioral nutrition and
physical activity, 13(1), p.5.
Lampard, A.M., MacLehose, R.F., Eisenberg, M.E.,
Neumark-Sztainer, D. and Davison, K.K., 2014.
Weight-Related Teasing in the School Environment :
Associations with Psychosocial Health and Weight
Control Practices Among Adolescent Boys and Girls.
Journal of Youth and Adolescence, 43(10), pp.1770–
1780.
Lee, J. and Lee, Y., 2016. The association of body image
distortion with weight control behaviors, diet
behaviors, physical activity, sadness, and suicidal
ideation among Korean high school students: a cross-
sectional study. BMC Public Health, 16(1), p.1.
Lintang, A., Ismanto, Y. and Onibala, F., 2015.
HUBUNGAN CITRA TUBUH DENGAN
PERILAKU DIET PADA REMAJA PUTRI DI SMA
NEGERI 9 MANADO. eJournal Keperawatan (e-Kp),
3(2).
Lõpez-Guimerà, G., Neumark-Sztainer, D., Hannan, P.,
Fauquet, J., Loth, K. and Sánchez-Carracedo, D.,
2013. Unhealthy weight-control behaviours, dieting
and weight status: A cross-cultural comparison
between North American and Spanish adolescents.
European Eating Disorders Review, 21(4), pp.276–
283.
Matera, C., Nerini, A. and Stefanile, C., 2013. The role of
peer influence on girls’ body dissatisfaction and
dieting. Revue europeenne de psychologie appliquee,
63(2), pp.67–74.
Mayer-Brown, S., Lawless, C., Fedele, D., Dumont-
Driscoll, M. and Janicke, D.M., 2016. The effects of
media, self-esteem, and BMI on youth’s unhealthy
weight control behaviors. Eating Behaviors, 21,
pp.59–65.
Neumark-Sztainer, D., 2009. The interface between the
eating disorders and obesity fields: Moving toward a
model of shared knowledge and collaboration. Eating
and Weight Disorders - Studies on Anorexia, Bulimia
and Obesity, 14(1), pp.51–58.
Neumark-Sztainer, D., Hannan, P.J., Story, M. and Perry,
C.L., 2004. Weight-control behaviors among
adolescent girls and boys: Implications for dietary
intake. Journal of the American Dietetic Association,
104(6), pp.913–920.
Neumark-Sztainer, D., Paxton, S.J., Hannan, P.J., Haines,
J. and Story, M., 2006a. Does Body Satisfaction
Matter? Five-year Longitudinal Associations between
Body Satisfaction and Health Behaviors in Adolescent
Females and Males. Journal of Adolescent Health,
39(2), pp.244–251.
Neumark-Sztainer, D., Story, M., Falkner, N.H., Beuhring,
T. and Resnick, M.D., 1999. Sociodemographic and
personal characteristics of adolescents engaged in
weight loss and weight/muscle gain behaviors: who is
doing what? Preventive medicine, 28(1), pp.40–50.
Neumark-Sztainer, D., Wall, M., Guo, J., Story, M.,
Haines, J. and Eisenberg, M., 2006b. Obesity,
disordered eating, and eating disorders in a
longitudinal study of adolescents: How do dieters fare
5 years later? Journal of the American Dietetic
Association, 106(4), pp.559–568.
Neumark-Sztainer, D., Wall, M., Larson, N.I., Eisenberg,
M.E. and Loth, K., 2011. Dieting and disordered
eating behaviors from adolescence to young
adulthood: Findings from a 10-year longitudinal study.
Journal of the American Dietetic Association, 111(7),
pp.1004–1011.
Neumark-Sztainer, D., Wall, M., Story, M. and Standish,
A.R., 2012. Dieting and unhealthy weight control
behaviors during adolescence: Associations with 10-
year changes in body mass index. Journal of
Adolescent Health, 50(1), pp.80–86.
Neumark-Sztainer, D., Wall, M.M., Story, M. and Perry,
C.L., 2003. Correlates of unhealthy weight-control
behaviors among adolescents: implications for
prevention programs. Health Psychology, 22(1),
pp.88–98.
Ojala, K., Vereecken, C., Valimaa, R., Currie, C.,
Villberg, J., Tynjala, J. and Kannas, L., 2007.
Attempts to lose weight among overweight and non-
overweight adolescents: A cross-national survey.
International Journal of Behavioral Nutrition and
Physical Activity, 4(50).
The Effects of Sociocultural Pressures, BMI, Weight Perception, and Body Dissatisfaction on Unhealthy Weight Control Behaviors among
Indonesian Adolescent Girls
147

Papp, I., Urbán, R., Czeglédi, E., Babusa, B. and Túry, F.,
2013. Testing the Tripartite Influence Model of body
image and eating disturbance among Hungarian
adolescents. Body Image, 10(2), pp.232–242.
Patton, G., Selzer, R., Coffey, C., Carlin, J. and Wolfe, R.,
1999. Onset of adolescent eating disorders: population
based cohort study over 3 years. British Medical
Journal, 318(7186), pp.765–768.
Pingitore, R., Spring, B., Garfield, D. and Spring, B.,
1997. Gender Differences in Body Satisfaction. 5(5).
Prima, E. and Sari, E.P., 2013. Hubungan Antara Body
Dissactisfaction dengan Kecenderungan Perilaku Diet
pada Remaja Putri. Jurnal Psikologi Integratif, 1(1),
pp.17–30.
Quick, V., Ph, D., D, R., Loth, K., D, R., Maclehose, R.,
Ph, D., Linde, J.A., Ph, D., Neumark-sztainer, D., Ph,
D. and D, R., 2013. Prevalence of Adolescents ’ Self-
Weighing Behaviors and Associations With Weight-
Related Behaviors and Psychological Well-Being.
Journal of Adolescent Health, 52(6), pp.738–744.
Rodgers, R.F., McLean, S.A. and Paxton, S.J., 2015.
Longitudinal relationships among internalization of
the media ideal, peer social comparison, and body
dissatisfaction: Implications for the tripartite influence
model. Developmental Psychology, 51(5), pp.706–
713.
Rodgers, R.F., Paxton, S.J. and McLean, S.A., 2014. A
Biopsychosocial Model of Body Image Concerns and
Disordered Eating in Early Adolescent Girls. Journal
of Youth and Adolescence, 43(5), pp.814–823.
Al Sabbah, H., Vereecken, C., Abdeen, Z., Kelly, C.,
Ojala, K., Németh, Á., Ahluwalia, N. and Maes, L.,
2010. Weight control behaviors among overweight,
normal weight and underweight adolescents in
Palestine: Findings from the national study of
Palestinian schoolchildren (HBSC-WBG2004).
International Journal of Eating Disorders, 43(4),
pp.326–336.
Schaefer, L.M., Burke, N.L., Thompson, J.K., Dedrick,
R.F., Leslie, J., Calogero, R.M., Bardone-cone, A.M.,
Higgins, M.K., Frederick, D.A., Kelly, M., Anderson,
D.A., Schaumberg, K., Nerini, A., Dittmar, H., Clark,
E., Adams, Z., Macwana, S., Klump, K.L., Vercellone,
A.C., Paxton, S.J., Swami, V., Development, O.,
Sataq-, A.Q.-, Schaefer, L.M., Burke, N.L.,
Thompson, J.K., Dedrick, R.F., Calogero, R.M.,
Frederick, D.A., Anderson, D.A., Schaumberg, K.,
Dittmar, H., Clark, E., Adams, Z., Macwana, S. and
Paxton, S.J., 2015. Development and validation of the
Sociocultural Attitudes Towards Appearance
Questionnaire-4 (SATAQ-4). Psychological
Assessment, 27(1), pp.54–67.
Shroff, H. and Thompson, J.K., 2006. The tripartite
influence model of body image and eating disturbance:
A replication with adolescent girls. Body Image, 3(1),
pp.17–23.
Siamti, W., 2017. Perempuan Perokok dalam Perspektif
Sosial. Kompasiana.com.
Stice, E., 2002. Risk and Maintenance Factors for Eating
Pathology : A Meta-Analytic Review. Psychological
bulletin, 128(5), pp.825–848.
Stice, E., Presnell, K., Shaw, H. and Rohde, P., 2005.
Psychological and Behavioral Risk Factors for Obesity
Onset in Adolescent Girls: A Prospective Study.
Journal of Consulting and Clinical Psychology, 73(2),
pp.195–202.
Sukamto, M., 2017. Measurement of Unhealthy Weight
Control Behaviors among Indonesian Adolescent
Girls. Surabaya.
Sulistyan, A., Huryati, E. and Hastuti, J., 2016. Distorsi
citra tubuh, perilaku makan, dan fad diets pada remaja
putri di Yogyakarta. Jurnal Gizi Klinik Indonesia,
12(3), pp.99–107.
Thøgersen-Ntoumani, C., Ntoumanis, N. and Nikitaras,
N., 2010. Unhealthy weight control behaviours in
adolescent girls: a process model based on self-
determination theory. Psychology & health, 25(5),
pp.535–50.
Tiggemann, M., 2012. Sociocultural Perspectives on Body
Image. In: T.F. Cash, ed., Encyclopedia of Body Image
and Human Appearance. London: Elsevier and
Academic Press, pp.758–765.
Tiggemann, M. and Miller, J., 2010. The Internet and
Adolescent Girls ’ Weight Satisfaction and Drive for
Thinness. Sex Roles, 63, pp.79–90.
Vander Wal, J.S., 2011. Unhealthy weight control
behaviors among adolescents. J Health Psychol, 17(1),
pp.110–120.
Wertheim, E.H. and Paxton, S.J., 2012. Body Image
Development - Adolescent Girls. In: T. Cash, ed.,
Encyclopedia of Body Image and Human Appearance.
London: Elsevier and Academic Press, pp.187–193.
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
148
