
Gender Disparity In Awareness and Disease Control among
Indonesia Hypertension Adults Aged 40: Study from Indonesia
Family Life Survey Wave 5
Novi Maulina
1
1Faculty of Medicine, Universitas Syiah Kuala, Banda Aceh, Indonesia
Keywords: Hypertension, Gender Disparity.
Abstract: Hypertension is a known major avoidable risk factor for cerebro- and cardiovascular disease. Awareness of
the disease is required for medication adherence to prevent the complication. Using a cross-sectional
population-based survey data (Indonesia Family Life Survey (IFLS)), we observed the determinant factors
in hypertension awareness and disease control among Indonesia Hypertension adults aged ≥40 (N=2676).
Our finding suggested that 56% of 2676 hypertensive patients were women. Among those patients, only
42.8 % aware that they had high blood pressure and only 14.6 % had the anti-hypertensive drugs. Women
were more aware of hypertension and disease control compared than men. Men and older patients (>60
years old) were more vulnerable to have undiagnosed and untreated hypertensive status. It is substantial to
do regular health screening and society education to improve hypertension awareness and to reduce gender
disparity in cardiovascular problem among Indonesian adults.
1 INTRODUCTION
Hypertension is an important public health issue
since it is a major avoidable risk factor for cerebro-
and cardiovascular diseases, and kidney failure in
Indonesia as one of a low- and middle-income
country (WHO, 2014; Castillo, 2016; Perkovic,
2007). Despite decades of public education efforts to
get lower community-blood pressure, the disease
prevalence remains high due to various factors
affected, such as sociodemographic (older age,
female or male gender, lower education level and
lower household income), geolocality (urban
residence), body size, health behaviour and
psychosocial stress (Ezzati, 2015; Kearney, 2004;
Pereira, 2009). Increasing elder population,
unfavourable behavioural risk factor, low patient
awareness and their adherence to treatment are some
of its challenges (Ong, 2007; Daughterty, 2011).
Precise prevention and treatment strategy is required
to reduce hypertension-related complications and
mortality (Daughterty, 2011).
The management and control of hypertension is
also affected by sex, age and other various factors
(Daughterty, 2011; Sanberg, 2012; Chu, 2015).
However, a study showed that only two-thirds of
adults and the elderly aware of their hypertension
status and gender is known as one of important
factor (Chu, 2015). Determining gender patterns in
hypertension awareness and factors which affect
these patterns in life stage is critical to improve
hypertensive control and reduce cardiovascular
disease risk. In this study, using national-based
survey source, we aimed to investigate sex
difference in hypertension awareness and control
among Indonesian adults aged ≥40 years.
Be advised that papers in a technically unsuitable
form will be returned for retyping. After returned the
manuscript must be appropriately modified.
2 METHODS
2.1 Study Population
We used data from the “Indonesia Family Life
Survey (IFLS-5)”, a sustaining demographic and
health survey that started in 1993 and had four
rounds of data collection, with the fifth wave (IFLS-
5) having been completed in 2015. The surveys
Maulina, N.
Gender Disparity In Awareness and Disease Control among Indonesia Hypertension Adults Aged 40: Study from Indonesia Family Life Survey Wave 5.
DOI: 10.5220/0008789201090113
In Proceedings of the 2nd Syiah Kuala International Conference on Medicine and Health Sciences (SKIC-MHS 2018), pages 109-113
ISBN: 978-989-758-438-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
109

collected data on individual, household and
community level using a multistage stratified
sampling. The original sampling frame of the first
survey in 1993 was based on households from 13 of
27 provinces in Indonesia, which represented
approximately 84% of the Indonesian population in
1993. The detail description of the sampling and
survey methods has been explained elsewhere
(Strauss, 2016).
Randomly selected household members were
asked to provide detailed individual information. In
the IFLS-5, 16,204 households and 29,965 18 years
and older individuals were interviewed and had
complete blood pressure measurements. In the fifth
wave of IFLS, the recontact rate is 92% and for
individual target households, the recontact rate is
90.5% (Strauss, 2016). The survey run
longitudinally and we restricted the data for
participants aged ≥40 years.
In this study, we sorted and filtered the data to
participants aged ≥40 years who had high blood
pressure measurements (systolic blood pressure
≥140 mmHg and diastolic blood pressure ≥90
mmHg) and complete information on other
sociodemographic, body size, self-reported
hypertension and information about medication.
Participants who had not complete information were
excluded.
2.2 Measurement
Measurement included in this study were blood
pressure measurements, anthropometric
measurements, and questionnaire items on
sociodemographic factors and tobacco use.
2.2.1 Blood Pressure Measurement
Systolic and diastolic blood pressure was
measured three times with an Omron meter, HEM-
3204, by regular trained interviewers on household
members 18 years and older at home in a seated
position. The first BP measurement was derived at
the beginning of the interview and subsequent
assessments derived during the interview (Strauss,
2016). The three BP measurements were recorded
and the average BP was then calculated. Blood
pressure was classified using JNC 7 algorithm,
where “Hypertension was defined as systolic BP
≥140 mm Hg and/or DBP ≥90 mm Hg and/or
current use of antihypertensive medication”, while
normotension was defined as BP values <120/80
mm Hg in individuals who were not taking
antihypertensive medication” (Chobanian, 2003).
Aware of being hypertensive was defined if the
participants answered yes of having been diagnosed
of hypertension by a doctor, nurse, paramedic, and
trained mid-wife. Good control of hypertension was
defined if participants responded yes of currently
taking prescribed medication on a weekly basis to
manage hypertension.
The analysis is limited to participants who had
information on hypertension measurement,
awareness, and medication. Participants with
hypertension were defined if they had mean SBP
≥140 mmHg and or mean DBP ≥90 mmHg. Those
hypertensive participants then classified as aware (or
not) and are they on hypertensive medication (or
not).
2.2.2 Anthropometric Measurements
Weights were measured using a Camry model
EB1004 scale and height were measured using a
Seca plastic height board (Strauss, 2016). Body mass
index (BMI) was calculated as weight in kg divided
by height in metre squared and classified according
to Asian criteria: Underweight (BMI <18.5kg/m2),
normal weight (18.5 to 24.9 kg/m2), overweight
(25.0 to 29.9 kg/m2) and obese (BMI ≥30.0 kg/m2)
(Wen CP, 2009). Waist and hip measurement were
measured using a tape and the results was then
recorded to the nearest 0.1 cm. Waist-hip ratio then
calculated by dividing waist to hip measurement.
The WH value >0.9 for man and >0.85 for woman
were then classified as having central obese (Wen
CP, 2009).
2.2.3 Sociodemographic Factors
Sociodemographic data was sourced by list of
questionnaire about sex, age, smoking experience
(ever smoked or not), residential area (urban or
rural), highest level of education (unschooled, grade
school (elementary level), high school (junior or
senior high school) and graduate or above).
2.3 Statistical Analysis
Participants with complete information on blood
pressure measurement and other factors were
included in the analysis. The outcome variables were
mean SBP and DBP, prevalence of hypertension
awareness and disease control. Among hypertensive
patients, the percentage of those aware or not, and
on medication or not, were estimated. Percentage of
factors contributed to gender differences were also
SKIC-MHS 2018 - The 2nd Syiah Kuala International Conference on Medicine and Health Sciences
110
observed. Differences between the groups were
tested using Chi-Square test to observe the
proportion of each factors included. P-value to be
included were set at 0.05. SPSS software version
23.0 were used to analyse the data.
3 RESULT AND DISCUSSION
We sorted and filtered 29,965 total participants aged
≥18 years who had blood pressure measurement to
participants aged ≥40 years who had high blood
pressure (systolic blood pressure ≥140 mmHg and
diastolic blood pressure ≥90 mmHg) and had
complete information on other sociodemographic,
body size, self-reported hypertension and
information about medication. Then we derived
2,893 hypertensive participants aged ≥40 years, but
213 had not complete information and finally 2,676
participants included.
Table 1: Sample Characteristics
Men (%) Women (%)
Age group 44 56
40-49 37.8 36.3
50-59 36.7 36.3
60-69 18.5 18
≥70 6.9 9.3
Body Mass Index
(BMI)
Underweight 5.3 5.1
Normal 50.1 37.4
Overweight 34.7 39.5
Obese 9.9 18
Waist-Hip Ratio
(>0.9 for men and
>0.85 for women)
40.1 59.8
Residence Area
Urban 61 57.7
Rural 38.9 42.3
Education
Unschooled 4.2 14.9
Grade School 41.1 56.1
High School 40.4 23.3
Graduate or above 14.2 5.7
Smoking Experience
Ever 74.6 6.4
Never 25.4 93.6
Of this 2,676 hypertensive participants, we
found that 56% of these hypertensive patients were
women. Women had higher percentage of being
overweight and obese (57.7%), higher waist-hip
ratio (59.8%) and most of them (71%) had lower
education level, compare to men group. It was
consistent with other study in US, that in later life
(>60 years), women had higher risk of being
hypertensive compared to men in the same age
group (Yang Y, 2012). This suggested that in
Indonesia, while women have longer life
expectancy, older women had poorer health than
men. Thus, extending women’s health needs across
the life course beyond reproductive health should be
taken into account.
Among those hypertensive patients, only 42.8
% aware that they had high blood pressure and
women were significantly higher than men patients
(65%, p-value <0.05). Only 14.6 % of the total
sample had the anti-hypertensive drugs, and women
were also significantly higher in men (68%, p-value
<0.05). This result indicates that women had good
awareness of their health condition compared to
men. Other works in US showed that men was more
aware of their hypertension status compared to
women (Guo et al., 2012). The small percentage of
patients who aware of their high blood pressure
could be due to the method we used in collecting
data. In this study, we collected objective measures
of systolic and diastolic blood pressure
(hypertensive patients), followed by self-reported
hypertension, because we thought that the only self-
reported morbidities in general without objective
measurement is a known potential problem in
measuring population health status (Zajacova et al.,
2010).
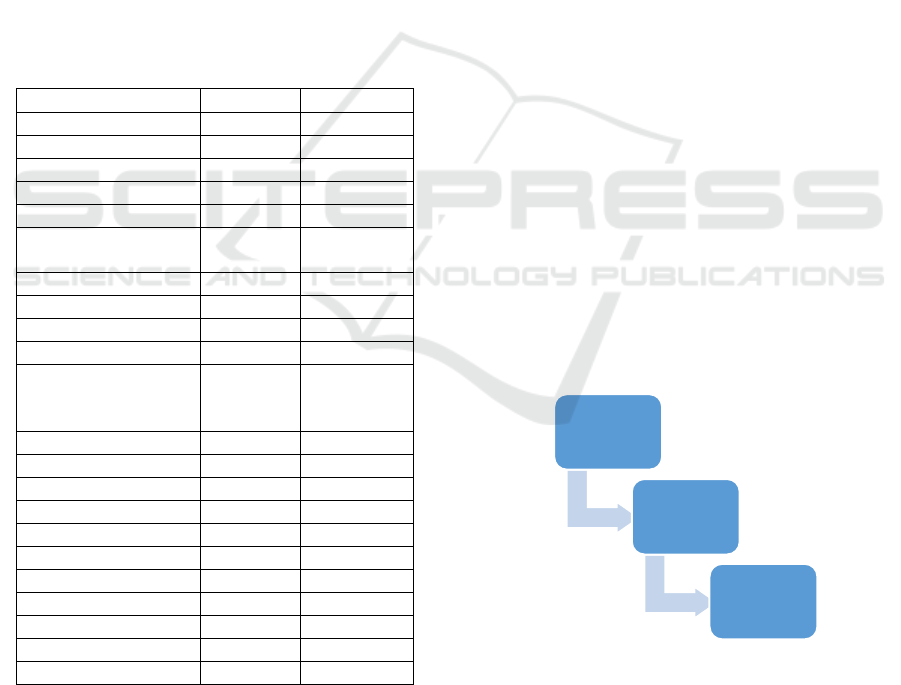
Schema 1. Prevalence of Awareness and Control of
Hypertensive patients
In our data, respondents aged <60 years old
tend to be more aware of their hypertensive status
(69%) because they more likely to see physicians on
a regular basis, increasing the likelihood that they
2,676
Hypertensive
Patients
1,146 Aware
of
Hypertension
265 Patients
on
Medication
Gender Disparity In Awareness and Disease Control among Indonesia Hypertension Adults Aged 40: Study from Indonesia Family Life
Survey Wave 5
111

will get the accurate and up-to-date knowledge of
their blood pressure status.
Both men and women patients (aged >60 years)
had low levels of hypertension awareness and
treatment control compared to those younger
patients aged 40-59 years (31% vs 65%; p-value
<0.05). Body status and education level were
significantly different between men and women in
those who aware. However, area of residence was
not significantly different in awareness and disease
control.
Table 2. Hypertension Characteristic of Study Sample
Men (%) Women (%) p-
value
Aware of
Hypertensi
on
401 (34) 745
(65)
<0.05
Age Range
40-59 276 (24) 523
(45)
>60 125 (10) 222
(19)
BMI
(Overweight
& obese)
223
(55.8)
418
(56.8)
<0.05
Residence
Area
(Urban)
248
(61.8)
452
(60.7)
0.70
Education
Level (High
School &
graduate)
223
(51.8)
214
(28.9)
<0.05
Control of
Hypertensi
on
125 (31) 265
(68)
<0.05
Age Range
40-59 83 (31) 172
(65)
>60 42 (15)
93 (35)
Observed gender disparity in health, typically
in hypertension, is due to both biological (sex
hormones, chromosomal differences, and other
biological differences) and behavioural factors
(high BMI, smoking, physical activity) (Sandberg
and Ji, 2012). Our result showed that women had
higher BMI and waist-hip ratio, since men had
smoking a lot compared to women. The wide range
of this behaviour might be closely related to
Indonesia’s culture, where smoking is considered
forbidden for women but a symbol of masculinity
and bravery for men, socially. Higher percentage of
women with lower education could also be related to
lower socioeconomic status, which limit their access
to employment and curtail opportunities for
practicing healthy lifestyle.
The study described the gender and age proportion
in Indonesia adults with hypertensive status, and the
difference of predicting factors for awareness and
disease control, among men and women. The study
did not asses the biological factors or diet habits,
which may alter the results. This study focused on
the gender differences in hypertension, the
importance of universal health screening access and
society education to be delivered to both men and
women.
4 CONCLUSIONS
In our study, hypertensive women patients were
more than men, and they also had good awareness of
high blood pressure and the disease control. Men
and those of older age patients (>60 years old) were
more vulnerable to have undiagnosed and untreated
hypertensive status. It is substantial to do regular
health screening and society education to improve
hypertension awareness and to reduce gender
disparity in cardiovascular problem among
Indonesian adults.
REFERENCES
World Health Organization (WHO). Non communicable
diseases country problems 2014.
http://apps.who.int/iris/bitstream/10995/128048/1/i38i
26150350i eng.pdf
R. Castillo, “Prevalence and management of hypertension
in Southeast Asia,” JHypertens, supplement 1, p. e6,
2016.
Perkovic V, Huxley R, Wu Y, Prabhakaran D, MacMahon
S. The burden of blood pressure-related disease: A
neglected priority for global health. Hypertension.
2007; 50:991–997. PMID: 17954719
Ezzati M, Obermeyer Z, Tzoulaki I, Mayosi BM, Elliott P,
Leon DA. Contributions of risk factors and medical
care to cardiovascular mortality trends. Nat Rev
Cardiol. 2015; 12:508–530. doi:
10.1038/nrcardio.2015.82 PMID: 26076950
Kearney PM, Whelton M, Reynolds K, Whelton PK, He J.
Worldwide prevalence of hypertension: A systematic
review. J Hypertens. 2004; 22(1):11–19. PMID:
15106785
Pereira M, Lunet N, Azevedo A, Barros H. Differences in
prevalence, awareness, treatment and control of
hypertension between developing and developed
SKIC-MHS 2018 - The 2nd Syiah Kuala International Conference on Medicine and Health Sciences
112

countries. J Hypertens. 2009; 27(5):963–975. PMID:
19402221
Ong KL, Cheung BMY, Man YB, Lau CP, Lam KSL.
Prevalence, Awareness, Treatment, and Control of
Hypertension Among United States Adults
1999±2004. Hypertension 2007; 49(1):69-75.
https://doi.org/10.1161/01.HYP.0000252676.46043.18
PMID: 17159087
Daugherty SL, Masoudi FA, Ellis JL, Ho PM, Schmittdiel
JA, Tavel HM, et al. Age Dependent Gender
Differences in Hypertension Management. Journal of
Hypertension 2011; 29(5):1005±1011.
https://doi.org/10.1097/HJH.0b013e3283449512
PMID: 21330934
Sandberg K, Ji H. Sex differences in primary
hypertension. Biology of Sex Differences 2012; 3:7-7.
https://doi.org/10.1186/2042-6410-3-7 PMID:
22417477
Chu SH, Baek JW, Kim ES, Stefani KM, Lee WJ, Park Y-
R, et al. Gender Differences in Hypertension Control
Among Older Korean Adults: Korean Social Life,
Health, and Aging Project. Journal of Preventive
Medicine and Public Health 2015; 48(1):38±47.
https://doi.org/10.3961/jpmph.14.043 PMID:25652709
J. Strauss, F. Witoelar, and B. Sikoki, The Fifth-Wave of
the Indonesia Family Life Survey (IFLS-5): Overview
and Field Report, vol. 1, RAND Corporation, 2016.
A. V. Chobanian, G. L. Bakris, and H. R. Black, “Seventh
report of the Joint National Committee on prevention,
detection, evaluation, and treatment of high blood
pressure,” Hypertension, vol.42, no.6, pp.1206–
1252,2003.
C. P. Wen, T. Y. David Cheng, S. P. Tsai et al., “Are
Asians at greater mortality risks for being overweight
than Caucasians? Redehning obesity for Asians,”
Public Health Nutrition, vol.12, no.4, pp.497–
506,2009.
Alexandra Kautzky-Willer caTD, 2 Ann Jensby,2 and
Anita Rieder2. Women show a closer association
between educational level and hypertension or
diabetes mellitus than males: a secondary analysis
from the Austrian HIS. 2012 May 30.
Everett B, Zajacova A. Gender Differences in
Hypertension and Hypertension Awareness Among
Young Adults. Biodemography and social biology
2015; 61(1):1±17. https://doi.org/10.1080/19485565.
2014.929488 PMID: 25879259
Yang Y, Kozloski M. Change of Sex gaps in total and
cause-spesific mortality over the life span in the US.
Ann Epidemiol. 2012; 22:94-103
Guo F, He D, Zhang W, et al., Trends in prevalence,
awareness, management and control of hypertension
among United States adults, 1999 to 2010. J Am Coll
Cardiol. 2012;60(7):599-606.
Zacacova A, Dowd JB, Schoeni RF, et al., Consistency an
dprecision of cancer reporting in a multiwave national
panel survey. Popul Health Metr. 2010;8:1-11
Gender Disparity In Awareness and Disease Control among Indonesia Hypertension Adults Aged 40: Study from Indonesia Family Life
Survey Wave 5
113
