
Fighting Substance Dependency Combining AAT Therapy and Virtual
Reality with Game Design Elements
Tanja Joan Eiler, Armin Gr
¨
unewald and Rainer Br
¨
uck
Medical Informatics and Microsystems Engineering, University of Siegen, H
¨
olderlinstraße 3, 57076 Siegen, Germany
Keywords:
VR Applications, Virtual Reality, Digital Medicine, Game Design, Therapy, Substance Dependency, Ap-
proach Avoidance Task, Cognitive Bias Modification, Approach Bias.
Abstract:
Smoking poses a significant health risk and is still the main cause of premature mortality today. The Approach
Avoidance Task (AAT) developed by Rinck and Becker aims to develop a substance dependence therapy that
can reach the digital society. In this paper, a demonstrator that transfers the AAT procedure into virtual reality
(VR) is presented. This demonstrator was used to carry out an evaluation with twenty participants who were
asked to use the program and evaluate it by means of questionnaires and interviews. In addition, the reaction
times (RTs) of the test persons were recorded and evaluated. The results show that the transfer of the AAT
procedure to VR is possible and promising. Above all, the use of three-dimensional scenarios and objects,
with which one interacts during the training, were well received and increased the immersion as well as the
felt embodiment. The use of game design elements has also proved helpful and has had a positive influence
on user motivation.
1 INTRODUCTION
1.1 Motivation
Tobacco products are among the most consumed ad-
dictive substances along with alcohol (Batra et al.,
2015). In Germany, approx. 29 % of adults and 9.6
% of adolescents between twelve and seventeen years
are smokers, which is one of the many reasons why
smoking is still one of the leading causes of prema-
ture mortality today (Donath, 2017).
Nevertheless, little attention is paid to this addic-
tion disorder. Hardly any therapy or prevention pos-
sibilities are offered or (further) developed. Anyone
who wants to start a therapy must expect long waiting
times and stigmatization.
The aim of this and our further studies is to de-
velop new and innovative methods of intervention us-
ing digital media, which can be used for the treat-
ment of substance dependency and thereby improve
the success of therapy. The use of digital medicine
(Elenko et al., 2015), in the form of virtual reality
(VR) and mobile applications, is not only intended
to reduce the inhibition threshold for starting a ther-
apy, but also to improve its availability to the general
public and its effectiveness.
The Approach Avoidance Task (AAT) was cho-
sen as the basis therapy procedure for this cause, as
past and recent research has already provided promis-
ing results, which show that AAT is an effective addi-
tional method for the treatment of addiction diseases
like smoking or eating disorders (for an overview see
(Kakoschke et al., 2017)).
Whereas conventional methods of smoking ces-
sation address reflective processes by, for example,
informing patients about the negative consequences
of their behavior, AAT uses the cognitive bias mod-
ification (CBM) method to cover implicit processes
in addition to conventional therapy. Cognitive biases
are responsible for the selective processing of stimuli
in the environment, and thus influences the emotions
and motivation of the viewer (MacLeod and Mathews,
2012). In this context, smokers show a specific ap-
proximation behavior for images containing smoking-
related stimuli, and, at the same time a comparatively
reduced approximation to alternative images. This be-
havior is measurable and can be observed in the ap-
proach and avoidance biases. Due to this fact, the
AAT approach is well suited for additional smoking
cessation therapies using smoking-related stimuli, as
described in (Machulska et al., 2016).
The rest of this paper is structured as follows:
First, the theoretical background is explained. This
includes the AAT procedure, VR and game design
elements. Subsequently, the state of the art and the
28
Eiler, T., Grünewald, A. and Brück, R.
Fighting Substance Dependency Combining AAT Therapy and Virtual Reality with Game Design Elements.
DOI: 10.5220/0007362100280037
In Proceedings of the 14th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2019), pages 28-37
ISBN: 978-989-758-354-4
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

background knowledge will be summarized. Then,
the concept as well as the game elements used in this
application will be presented. The following section
describes the implementation itself and the evalua-
tion. Finally, the results are summarized, conclusions
will be drawn and an outlook is given.
1.2 Theoretical Background
1.2.1 The Approach Avoidance Task (AAT)
The AAT is a psychological procedure based on the
hierarchical model of Approach Avoidance Motiva-
tion. This assumes that each individual follows posi-
tive stimuli and moves towards them (”approach”) to
capture and hold them. In contrast, negative stimuli,
such as pain, are avoided, resulting in a movement
away from them (”avoidance”) to correct or escape
them. These movements are not only physical, but
also psychological, making this model a fundamen-
tal component for understanding and generating mo-
tivation or self-regulation (Elliot, 2006). Past stud-
ies have shown that people evaluate almost all stimuli
as positive or negative (Bargh, 1997), and according
to their evaluation react with approach or avoidance
to them (Lewin, 2013). Moreover, it was repeatedly
noted that this is accompanied by a pushing or pulling
movement of the arms (Chen and Bargh, 2016; Marsh
et al., 2005).
Based on this knowledge, the AAT procedure was
developed by Rinck and Becker (2007) . For this
method, participants were shown individual pictures
on a computer screen, to which they should react uti-
lizing a joystick. Depending on its movement, the size
of the currently displayed image changed: by pulling
the joystick, it became larger, while pushing made it
smaller (see Fig. 1). Instructed not to pay attention
to the content of the images, but only to a certain dis-
tinguishing feature, like the image format (portrait or
landscape) or its clearly visible tilting, the test per-
sons should thus subconsciously learn to push away
stimuli related to their addiction, as these are always
shown in the format that should be avoided. In ad-
dition, the reaction times (RTs) were measured and
evaluated to determine the approach/avoidance bias
of the participants. The calculation for each stimuli
type is as follows:
Bias = MedianRT [PUSH]− MedianRT [PULL] (1)
A positive value implies an approach bias and
suggests an affirmative attitude towards the stimulus,
which is reflected in an approaching behavior. A
negative value represents an avoidance bias, result-
ing in an unfavorable attitude and averting behavior.
Figure 1: Idea of the Approach Avoidance Task.
Smokers should therefore get a higher approach bias
in smoke-related stimuli than non-smokers, as this
would imply an approaching behavior towards them.
The results of various studies (Kakoschke et al.,
2017) have shown that the AAT method could be used
for therapeutic purposes. Studies to this topic are still
undergoing, and this motivated us to transfer the AAT
procedure to VR in order to treat addiction disorders
more efficiently.
1.2.2 Virtual Reality and Game Design Elements
VR is a computer-generated three-dimensional alter-
native reality in which a person can interact and move
(Sherman and Craig, 2003; Simpson et al., 2000).
This virtual environment (VE), into which the user
can immerse, can be used in a wide range of applica-
tions, such as the simulation of an alternative reality
(duPont, 1995) or for the representation of complex
data (Pickover and Tewksbury, 1994; Simpson et al.,
2000). But it is also possible to use VR in quite dif-
ferent environments, e.g. in medical or military con-
text. Applications are also seen in education, archi-
tecture (virtual house inspections), psychology (treat-
ment of phobias and dependence illnesses), entertain-
ment (video games) and many other domains (Giraldi
et al., 2003).
Since users can immerse into the virtual world on
a visual, auditive, and motoric level, the feeling of
immersion is significantly higher compared to con-
ventional systems. This type of human-computer in-
teraction is called ”presence” and can increase the ef-
fectiveness of interactions in VE (Schultze, 2010). If
implemented correctly, the VE can generate a high
cognitive absorption in the users, which means that
they lose the sense of time, can focus better, and feel
that the content is entertaining and arouses the curios-
ity for more. Temporarily, the user tends to get the
feeling that he has full control over the system and is
not depending on it (Agarwal and Karahanna, 2000).
This effect can be enhanced by the use of game de-
sign elements. The aim is to motivate users to act in a
Fighting Substance Dependency Combining AAT Therapy and Virtual Reality with Game Design Elements
29

more targeted manner and thus increase their general
motivation to interact with the system (Sailer et al.,
2017). In addition, AAT can contribute a lot to early
intervention when used in a timely manner, especially
to ensure that the users stay motivated for a sufficient
period of time to carry out the therapy and do not drop
out prematurely (Boendermaker et al., 2015).
2 RELATED WORK
Lee et al. (2004) linked a VE to cue exposure ther-
apy (CET), which aim is to reprogram the behavior of
patients by learning to deal differently with situations
that trigger addiction. They are regularly exposed to
stimuli that cause craving until their respective toler-
ance level towards them has increased to such an ex-
tent that they can think about their actions in risk sit-
uations instead of involuntarily giving in to their urge
(Murphy, 2014). In the experiment of Lee and his col-
leagues, a VE was created which was composed of ad-
dictive environments and components. In their case,
it was a bar containing various objects such as ash-
trays, cigarette packs, or lighters, a smoking avatar,
and the audio track of a noisy restaurant. For all ob-
jects, three-dimensional models were used, since Lee
et al. had already found out in a previous study that
these trigger a much higher addiction pressure than
two-dimensional images (Lee et al., 2003). The study
participants, sixteen late adolescent men who con-
sumed at least ten cigarettes a day, were repeatedly
exposed to addictive stimuli in six sessions. The re-
sults showed that in the course of the test series the
number of cigarettes consumed as well as the addic-
tion pressure has gradually decreased, which is why it
can be assumed that the use of a VE within treatment
programs can be extremely helpful.
In the pilot study of Girard et al. (2009) , the
participants should find, grasp and destroy up to 60
cigarettes, which were hidden in a medieval VE. Over
a period of four weeks, one session was held every
week, each lasting 30 minutes. The control group
had similar conditions, however, no cigarettes were to
be destroyed here, but balls were to be collected and
taken along. The results showed a statistically sig-
nificant reduction in nicotine use and the abort rate of
the accompanying treatment program as well as an in-
crease in the abstinence rate compared to the control
group. In addition, 23 % of the participants stated that
they repeatedly remembered destroying the cigarettes
within the VE, which only 3 % of the participants in
the control environment did. This could indicate that
an increased belief in self-efficacy can be achieved
if an individual watches himself destroying cigarettes
and also invests time and effort in finding others to de-
stroy them as well. The perceived embodiment within
the VE additionally contributed to the effectiveness.
A first attempt to transfer CBM to VR for the
treatment of eating disorders was made in 2016 by
Schroeder et al. (2016) . Here, 23 participants were
asked to interact in a VR scenario with 3D objects
representing either a food item or a ball by making
a rejecting or gripping hand movement. The RT is
measured at three different points in time: At the be-
ginning of the hand movement, at object contact, and
as soon as the object has been collected. During the
study, the participants sat on a chair and wore an Ocu-
lus Rift DK2 as a Head-Mounted-Display (HMD). In
addition, the Leap Motion infrared sensor (Leap Mo-
tion, 2018) was used to track the hand movements
and transfer them to the VE. The visible virtual hand
should help the users think that it was their own hand
(body-ownership) (Slater et al., 2009). As soon as the
starting conditions (placing the dominant hand at a
predefined starting position, HMD oriented centrally
and no head movements for 1.000 ms) were met, a 3D
object appeared in front of the players, to which they
should either react with a defensive hand movement,
or grab and collect it. During the game, a progress
bar filled up, and the last six collected objects were
displayed at the top of the screen. The study results
showed that food objects, especially with increasing
body mass index (BMI) of the test persons, were col-
lected significantly faster than ball objects. In sum-
mary, VR in conjunction with CBM, possibly also to-
gether with other technologies, such as eye-tracking,
can be a helpful tool for the detection and treatment
of addiction disorders.
3 CONCEPT AND GAME DESIGN
3.1 Requirement Analysis
Figure 2: Three-dimensional mock-up of the virtual house.
As a pilot study (Eiler, 2018), a basic VR demon-
strator had to be implemented that should compare
the original desktop AAT (DAAT) procedure with a
slightly extended version that contains more game de-
HUCAPP 2019 - 3rd International Conference on Human Computer Interaction Theory and Applications
30

sign elements. The Unreal Engine and a HTC VIVE
HMD with a resolution of 2160 x 1200 pixels and a
refresh rate of 90 Hz will be used. The training con-
cept, e.g. the tilting of the images as a distinguishing
feature, is based on the AAT studies of Machulska
et al. (2016) . To make the two scenarios compa-
rable, the VE should consist of two rooms, one for
each procedure. Free movement within an area of 2
m x 2 m will be permitted. A mock-up for the three-
dimensional layout and design of the rooms, created
with eTeks Sweet Home 3D, Version 5.6, is shown in
Fig. 2. Within these rooms, in the sense of the AAT
procedure, various stimuli ought to be shown one after
another and have to be interacted with. They display
either addiction-related or neutral stimuli. As imple-
mented in the studies of Machulska et al. (2016) , the
addiction-related 2D images in the first room have to
be tilted to the right and should be pushed, while the
neutral ones have to be tilted to the left and require to
be pulled. In the second room, where 3D objects in-
stead of 2D images should be used, the distinguishing
feature will be the border color of the stimuli: Red-
bordered objects ought to be thrown away into a trash
can and blue-bordered ones pulled and collected in-
side a cardboard box. Correctly treated stimuli will
disappear immediately. Following the original proce-
dure the next stimulus appears after the thumb stick
on a controller is pressed. Within the VE short in-
structions on the wall will show how the task should
be fulfilled in case the participants need to reassure
themselves within the training scenario.
While the participants complete the AAT train-
ing, their reaction times have to be recorded twice:
The time that has passed between the appearance of
the stimulus and the first contact by the user, and the
time that has passed until the correct action has been
taken. Time measurements have to be taken as ac-
curate as possible, ideally in the millisecond range,
to calculate the approach/avoidance bias. This is due
to the fact that we want to measure and alter auto-
matic processes, which happen very fast. Reactions
lasting longer than 300 ms are accessible to rational
consciousness and therefore are no longer involuntary
(see P300 wave). In addition, the differences resulting
from AAT training are often only a few milliseconds,
and such accuracy is needed to validate these differ-
ences.
A configuration file should allow the test leader to
specify the test subject ID, the degree of tilting, the
number of stimuli shown, how many of these stimuli
should show an addiction-independent distinguishing
feature and if a 3D model of the HTC Vive controller
or a robotic hand should be used to represent the in-
teractions of the users.
Our aim was to find out if a transfer of the AAT
procedure to VR is possible and if so, which room
works better and what has to be changed in the de-
sign for the further course of the study. The measured
RTs and the biases derived from the measurement re-
sults were compared to the results of the studies by
Machulska et al. (2015) . Due to the fact that the
psychologists involved wanted as few distracting el-
ements as possible in order to make the results com-
parable, game design elements were kept to a mini-
mum in this pilot study. The evaluation carried out
should provide initial results in terms of design, user-
friendliness and immersion in order to develop an im-
proved demonstrator which will be used for the elab-
orated studies in the future.
The two rooms, the VE, and the training execution
are described in more detail below.
3.2 The Desktop Room
Figure 3: Interaction within the desktop room.
The first room, called ”desktop room” (DR), should
differ as little as possible from the DAAT and con-
tains hardly any game design elements. For this rea-
son, 2D images floating in the middle of the room are
used here (see Fig. 3). These images, kindly provided
by Rinck and his colleagues (2007) , are either tilted
to the left or right because the distinguishing feature
ought to be clearly recognizable, but should not dis-
tract too much from the image content, as the avoid-
ance of addiction-specific stimuli is to be automated.
Since the zooming factor is extremely decisive in the
AAT procedure, the images pushed away are artifi-
cially reduced in size, whereas the enlarging perspec-
tive effect is sufficient when pulled. Correct actions
are rewarded with a positive sound effect, and press-
ing the thumb stick will display the next image. In the
event of an error, a negative-sounding tone rings out
and the ceiling light turns red until the correct move-
ment is done. In addition, the interactions are visu-
ally represented with two different 3D models (see
Fig. 4), which can be set via the configuration file.
The first model represents the HTC Vive Controllers,
which the test subjects will hold in their hands during
Fighting Substance Dependency Combining AAT Therapy and Virtual Reality with Game Design Elements
31

the experiment and which can also be seen on the in-
structions. The second model is a robotic hand with
gripping animations.
Figure 4: The two models that can be used for the interac-
tion.
3.3 The VR Enrichment Room
In the second room, the ”VR enrichment room”
(VRER), more game design elements are used, like
3D modeled surroundings as well as a particle effect
accompanying the appearance of the stimuli (Fig. 5).
The most important elements for the training are a ta-
ble and two containers: a cardboard box and a trash
can. The box stands between the users and the table
on which the objects will appear. Since the users stand
directly in front of the box and the trash can is lo-
cated behind the table, arm movements necessary for
the AAT training can thus be transferred into three-
dimensional space. Instead of 2D images, 3D objects
are used to further increase immersion since the stud-
ies by Lee et al. (2003) and Gorini et al. (2010) could
prove that they produce a higher craving than 2D im-
ages. The objects are to be sorted according to their
border color: In case of having a blue border, they
should be placed in the box, if they have a red bor-
der, they have to be thrown into the trash can. Visual
and acoustic feedback is the same as in the DR. The
appearance of the objects is accompanied by a purple
cloud of smoke, so that they, unlike the images in the
first room, do not appear ”out of nowhere”. The added
elements should have the benefit that the training is
more entertaining, which would increase motivation
and therefore the success rate of the therapy.
3.4 The Virtual World
The two rooms are connected by an elevator, which
has an operating panel and a level indicator. After
the successful completion of the first room, which is
indicated by a green light, the elevator opens its door
so that the user can enter and proceed to the second
floor. The ride is accompanied by a sound file that
reproduces the sounds of a moving elevator. After
the user has reached the upper level, a bell sounds,
and at the same time, the door opens again so that
the user can step outside. The main purpose of the
elevator is to ensure that the start and end points are
always identical when changing rooms. If the rooms
were connected by a door, the user would have to turn
180 degrees to enter the next room without leaving
the boundaries of the tracking area, which would feel
unnatural and therefore disrupts the immersion.
Outside the house a virtual environment was cre-
ated, which is visible through the windows. It consists
of an extensive grassy landscape with trees, flowers
and bushes. This should help ensure that the VE has
no visible end and appears more natural. In addition,
the oppressive feeling within the small rooms should
be reduced so that the users feel more comfortable
during the training.
3.5 Conducting the Training
Figure 5: The VR enrichment room.
In summary, the training is conducted as follows: The
user starts in the DR, where the thumb stick of the
controller needs to be pressed to start the training and
the first run. Each run includes one stimulus. The
recording of the RT also starts at this point. After
pressing the button, the first image appears, to which
the user must react according to its tilting. When the
image is grasped, by pressing the trigger, the first RT
is saved. If the user’s subsequent action was cor-
rect, the image disappears, a positive-sounding tone
is played, the second RT is saved and the run is con-
sidered finished. However, if the action is faulty, the
ceiling light in the room turns red and a negative-
sounding tone rings out to signal the error. The im-
age is also moved back to its original location and the
current run continues until the correct action has been
executed. Once the image has been moved correctly,
the ceiling light returns to its natural color. In this case
the run is finished and the next one can be started by
pressing the thumb stick. Errors are also recorded,
since incorrect runs must not be taken into account
when calculating the bias. Once the amount of images
specified in the configuration file have been handled
correctly by the user, the light turns green for one sec-
ond and the elevator opens. If this happens, the DR is
HUCAPP 2019 - 3rd International Conference on Human Computer Interaction Theory and Applications
32

considered finished. Via the lift the user now enters
the VRER, which is similar in functionality, with the
exception that 3D objects are used here whose bor-
der color specifies into which container they must be
sorted. The ID of the user and the recorded data are
exported to an external .csv file.
4 IMPLEMENTATION
The Unreal Engine (UE) (Epic Games, 2017), in the
version 4.18, was used for the implementation of this
Windows x64 application. Mainly Blueprints were
used, a kind of visualized programming language of
the UE. However, some functions, e.g. for reading
and writing external files, have been programmed in
C++.
A ”canvas” is placed in the middle of the DR (see
Fig. 3), whose blueprint controls the entire function-
ality of this room. It contains an array in which all
pictures that can appear are stored. File names and
substring queries are used to determine whether the
stimulus is negative or positive. To determine whether
the executed movement was an pulling or pushing ac-
tion, the difference between the image distance be-
fore and after the participant grasps and releases it is
calculated. A buffer area of 6 cm in both directions
was implemented in order to ensure that the program
does not evaluate the slightest movement as pushing
or pulling away.
The VRER works very similarly, although 3D ob-
jects are used here. These are taken from the Google
Poly database (Google LLC, 2018). The border color
that decides into which container the item is to be
sorted, was implemented using Tom Looman’s ”Multi
Color Outline Post Process” extension (Tom Looman,
2015), which requires a post-process volume and the
use of a custom stencil. In order to be able to deter-
mine whether the objects have been sorted correctly,
they were provided with tags, which are queried in
the event of a collision with one of the trigger boxes
inside the containers. An ongoing sorting process can
be seen in Fig. 6. The smoke effect was taken from
the ”Infinity Blade Effects” asset collection made by
Epic Games and adapted for the use inside the demon-
strator.
A challenge was the accuracy of the time record-
ing. This must be very precise, since even a few mil-
liseconds make a difference in the evaluation of the
recorded RTs in order to determine the cognitive bias.
Initially, it was attempted to achieve this over the sys-
tem time, but the result was not satisfactory because
the function call, implemented in C++, was made via
a custom blueprint node. Due to our inexperience in
Figure 6: Sorting within the VR enrichment room.
VR programming at this time, after some research we
found out that blueprints have a frame dependency.
This means that function calls are always executed
with the next frame, never between two frames, which
in turn means that the accuracy depends on the per-
formance of the used computer. Due to these circum-
stances, a time recording accurate to the millisecond
is not feasible using blueprints. Next, the time mea-
surement was implemented using a time line, which,
while it is running, continuously updates a variable in
which the time that has passed so far is stored. For
time measurement, this variable can simply be read
and the return value saved in further variables. This
resulted in an accuracy of 12 ms to 16 ms on the work-
ing machine, which is critical in terms of precision,
especially since less powerful computers are therefore
unsuitable.
5 METHOD
5.1 Participants and Design
Twenty participants (ten females and ten males; mean
age: 29.74 years, range: 18-60; five smokers) took
part in the evaluation. For 75 % of the test persons,
the experiment was their first point of contact with
VR.
The experimental design required the participants
to be shown twenty stimuli in each room, the first ten
of which show a tilting or border color independent of
the image content, which means that addiction-related
stimuli may be pulled and neutral ones pushed. In the
last ten stimuli, each smoking-related stimulus had
to be pushed away and vice versa. All participants
started in the DR and completed both rooms. They
conducted one test run to learn the controls and to de-
termine how understandable the demonstrator is only
with the contained instructions.
After signing a declaration of consent, the test per-
sons were introduced to the framework plot and func-
tionality of the program, while it was already known
that the demonstrator was aimed at the therapy of
Fighting Substance Dependency Combining AAT Therapy and Virtual Reality with Game Design Elements
33

nicotine addiction. After the participants put on the
HTC Vive HMD the application was started. During
the test run, the controller model was used in the DR
to visually represent the interaction, while the hand
model was used in the legitimate run whose RTs were
used for bias calculations.
Afterwards, all subjects were asked to complete
a non-standardized questionnaire containing fifteen
questions to determine how they perceived the pro-
gram with regard to various components like compre-
hensibility of the task, control, user-friendliness, en-
joyment or the perception of certain game design el-
ements. By means of a short interview, some of the
answers had to be explained in more detail.
6 RESULTS
6.1 Observations
As anticipated, observations during the experiment
have shown that while using the DR especially those
participants who have not had any previous experi-
ence with VR have found it difficult to perform the
correct arm movements. Only after a verbal instruc-
tion on how the movement should be carried out,
these test persons were able to continue the AAT
training correctly. Further problems that could be ob-
served in the DR include participants having difficulty
gripping the pictures. Often, despite the feedback
given by the vibration of the controller, they were un-
certain whether they were close enough to the image
to be able to grasp it. For the majority of the test sub-
jects, it was difficult to determine which arm move-
ment is required by the tilting of the images, which is
why they often positioned themselves in such a way
that they always had the instructions in view. In addi-
tion, it was tedious for most participants to press the
thumb stick after each stimulus to make the next one
appear. Each subject forgot this at least once during
the training.
The observations in the VRER differ greatly from
those in the DR. Surprisingly, even the inexperienced
participants had significantly fewer problems in carry-
ing out the required task, and instead began to experi-
ment with the objects during the test run. By using the
three-dimensional scenario and virtual hands, the sub-
jects had virtually no problems gripping and sorting
the objects. In addition, significantly fewer mistakes
were made. Furthermore, the test persons felt more
comfortable and less oppressed in this room, which
led to a stronger immersion. Moreover, they had sig-
nificantly more enjoyment performing the task, which
contributes positively to their motivation. However,
pressing the thumb stick to make the next object ap-
pear was also perceived as disrupting in this room. It
should be noted that the participants forgot to trigger
it much less frequently, which may be caused by the
fact that they could already internalize this behavior
through training in the DR.
6.2 Questionnaires
The evaluation of the questionnaires showed that both
immersion and embodiment were rated very well (on
average 7.5 and 7.4 points on a scale between 1 and
10). User-friendliness was generally perceived as
very good and beginner-friendly. The execution of the
task did not cause any further problems, except for the
difficulties in the DR mentioned above. The move-
ments felt natural, especially the VRER received very
good ratings. However, six people (30 %) stated that
they found the movements in the DR unnatural and
unusual. Two of them explained that this was due to
the fact that grasping ”floating images” felt peculiar.
Regarding the 3D models, 65 % of the participants
thought that the robotic hand model is more realis-
tic and makes the gripping movement, not only vi-
sually, more intuitive. 15 % of them found the hand
model to be better in principle, but noted that the con-
troller model is better suited for beginners, since the
instructions are easier to understand with it. 10 %
considered the controller model better because it re-
flects reality due to the fact that this controller is held
in the real world. However, it was emphasized that the
hand model would be preferred instead if a glove or
another technique would be used that would transfer
own hand movements realistically into the VE. The
remaining 25 % of the respondents stated that they
found both models to be of equal value.
Only 5 % of the participants expressed a negative
opinion about the particle effect used because it felt
too intrusive. Another 5 % stated that although the
smoking effect was not disturbing, ideally it should
only be used for smoking-related stimuli and the pos-
itive stimuli should have a different effect. 55 % con-
sidered the effect to be appropriate, as the objects do
not appear ”out of nowhere”, instead their appearance
is ”spectacular and made interesting”. Surprisingly,
35 %, including 60 % of the participating smokers,
stated that they did not notice the effect during the
experiment.
6.3 Evaluation of RTs and Comparison
with the Desktop AAT
Fig. 7 and Fig. 8 summarize the RT distribution
of smokers and non-smokers per image category and
HUCAPP 2019 - 3rd International Conference on Human Computer Interaction Theory and Applications
34
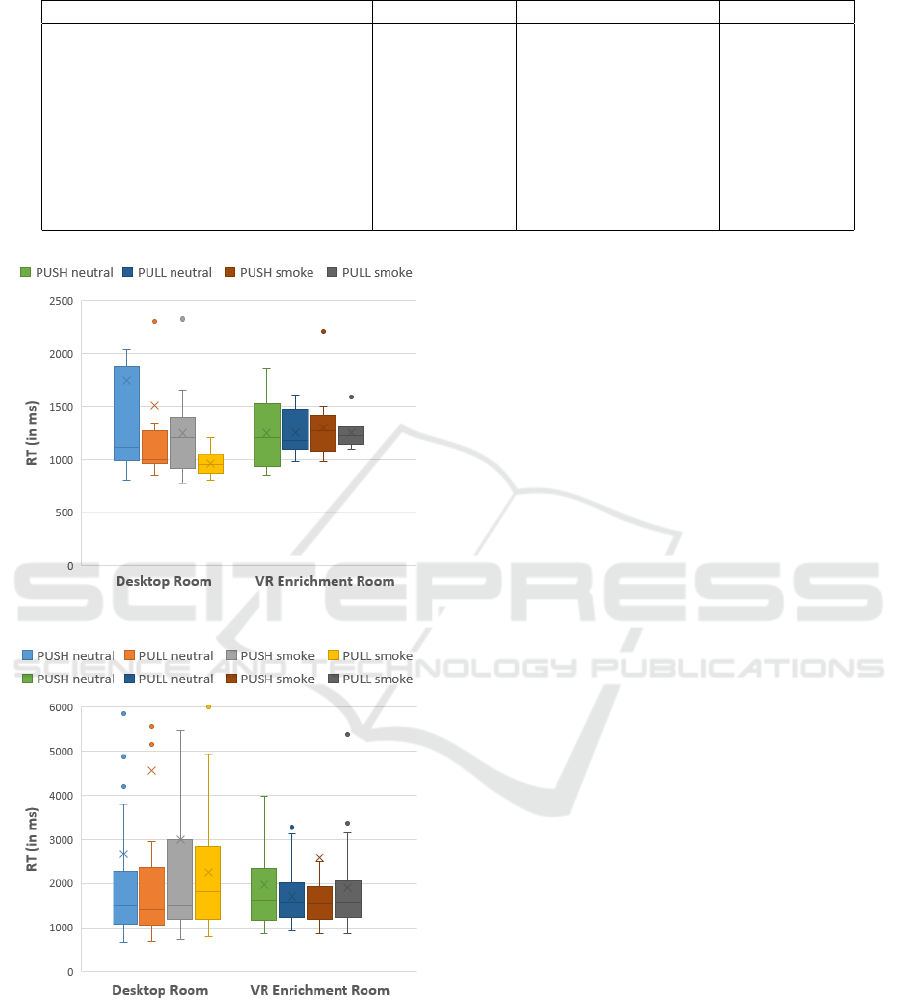
Table 1: Evaluation of RTs.
Desktop Room VR Enrichment Room Desktop AAT
median time until first contact 886 ms 851 ms /
median time until correct reaction 1416 ms 1319 ms 620 ms
mean duration of arm movement 530 ms 469 ms not necessary
Error rate smokers (%) 10 0 8
Error rate non-smokers (%) 8 6 11
Ø smoking-related bias (smokers) 256 44 25
Ø smoking-related bias (non-smokers) -312 -11 10
Ø neutral bias (smokers) 123,5 21.5 0
Ø neutral bias (non-smokers) 95 27.5 11
Figure 7: RT distribution of smokers.
Figure 8: RT distribution of non-smokers.
room. The results show that both groups were faster
in the VRER, whereby smokers were significantly
quicker to pull smoking-related stimuli in the DR (M
= 964.7,SD = 118.9) than in the VRER (M = 1252,SD
= 146.7). The lower deviation from the mean value
when pulling smoking-related stimuli also supports
the statement that smokers have a higher approach
bias for these stimuli. In addition, it is noticeable
that smokers have generally reacted faster than non-
smokers in all categories.
The evaluation of the measured RTs compared to
the DAAT can be seen in Table 1. The DAAT val-
ues refer to the study by Machulska et al. (2015) , in
which 92 smokers and 51 non-smokers participated
and responded to smoking-related vs. non-smoking-
related pictures.
Our measured RTs show that the median time
elapsed in the DR before the first contact with the
stimulus is 886 ms and 1416 ms until the correct in-
teraction with it, 530 ms were required to execute the
arm movement. The overall result of the VRER shows
that the subjects needed a median time of 851 ms un-
til the first contact and 1319 ms until the correct arm
movement, the execution took 469 ms. As expected,
due to Fitt’s Law our measured RTs are longer than
with the DAAT, where the median RT was 610 ms
until the correct reaction.
The calculated bias values are comparable with
those of the DAAT, with the exception that smok-
ers show an approach bias for neutral stimuli instead
of being neutral towards them. The bias values of
the VRER come closer to those of the desktop ATT,
as the values of the DR are much larger. Neverthe-
less, in both rooms smokers had an approach bias to-
wards smoking-related stimuli, which suggests that
those were pulled faster than they were pushed away,
whereas non-smokers had an avoidance bias towards
them. Interestingly, non-smokers had no avoidance
bias when using the DAAT, but an approach bias,
which at first would not be suspected.
The recorded data also show similarities between
the VRER and the DAAT regarding error rate, as
smokers made significantly fewer mistakes (0 % vs.
8 %) than non-smokers (6 % vs. 11 %) in these pro-
cesses. In the DR, on the other hand, more mistakes
were made in general, as smokers had an error rate of
10 % and non-smokers of 8 %.
Fighting Substance Dependency Combining AAT Therapy and Virtual Reality with Game Design Elements
35

7 CONCLUSION
On the basis of our findings, the transfer of the AAT
procedure into virtual reality is promising, and should
be pursued further, as almost all required functions
are possible in VR, except for the time measurement,
which is not sufficiently accurate due to the frame de-
pendency of the blueprints.
An added value can be recognized by using
VR and game design elements, since the evaluation
showed that the VRER was appraised more favorably
in all areas, especially considering enjoyment and
therefore motivation. The use of border colors as the
distinguishing feature also resulted in a lower error
rate. As anticipated, participants found interactions
with 3D objects more realistic, intuitive and visually
appealing, which contributed to an increased pres-
ence. The recorded data also reflect that the VRER
works better, as not only the RTs are faster, but the
VRER also shows more similarities with the DAAT
compared to the DR, especially considering the cal-
culated bias values, which are an essential part of the
AAT therapy.
The built-in game design elements were positively
received by the participants and therefore receive a le-
gitimization for implementation. Still, it had to be
examined whether the smoke effect is a disturbing
element, since the test subjects could possibly form
an association between the effect and smoking itself,
which would lead to biased results. However, the as-
sessments of the subjects lead to the conclusion that
the smoke effect could be maintained in the further
development of the project and can represent an added
value, whereby alternative particle effects should be
considered.
With regard to control, most respondents favored
the robotic hand model, as it feels more natural and in-
creases the feeling of embodiment. However, the con-
troller model was considered useful to make it easier
for beginners, as the controller is mapped in the in-
structions. It was often criticized that the thumb stick
has to be pressed repeatedly to make the next image
or object appear. Here it would make more sense for
the next stimulus to appear immediately after the pre-
vious one has been treated correctly.
For the future development of the project, a new
demonstrator, which incorporates the results of this
study, fixed the problems regarding the time measure-
ment and corrects design errors, is already in devel-
opment. Solutions suitable for therapeutic purposes,
which allow a visualization of the entire body within
the VE without interfering with the training, will be
examined. This would make the VR experience even
more realistic and pleasant, as it would improve em-
bodiment and therefore presence. In addition, this
would allow users to move more securely within the
VE. Regarding controls, the usage of the Leap Mo-
tion sensor (Leap Motion, 2018) or data gloves will be
evaluated, since hand movements can be transferred
even more faithfully to the VE. In this way, a positive
effect on embodiment can be expected.
In addition, consideration can be given to intro-
ducing gamification elements like progress bars, a
scoring system, achievements, or other elements, as
there is a significant increase in user motivation when
the context in which points or other rewards are re-
ceived is more closely related to the actions per-
formed - even if there are no stories or characters
(Dovis et al., 2012). The increased enjoyment while
playing should thereby raise the motivation to con-
tinue the therapy.
REFERENCES
Agarwal, R. and Karahanna, E. (2000). Time flies when
you’re having fun: Cognitive absorption and beliefs
about information technology usage. MIS Quarterly,
24(4):665.
Bargh, J. A. (1997). Advances in social cognition. In Wyer,
R. S., editor, The automaticity of everyday life, vol-
ume 10 of Advances in social cognition, pages 20–27.
Erlbaum, Mahwah, NJ.
Batra, A., Hoch, E., Mann, K., and Petersen, K. U. (2015).
S3-Leitlinie Screening, Diagnose und Behandlung des
sch
¨
adlichen und abh
¨
angigen Tabakkonsums. Springer
Berlin Heidelberg, Berlin, Heidelberg and s.l., 1. aufl.
2015 edition.
Boendermaker, W. J., Prins, P. J. M., and Wiers, R. W.
(2015). Cognitive bias modification for adolescents
with substance use problems–can serious games help?
Journal of behavior therapy and experimental psychi-
atry, 49(Pt A):13–20.
Chen, M. and Bargh, J. A. (2016). Consequences of au-
tomatic evaluation: Immediate behavioral predisposi-
tions to approach or avoid the stimulus. Personality
and Social Psychology Bulletin, 25(2):215–224.
Donath, C. (2017). Drogen- und suchtbericht 2017.
https://www.drogenbeauftragte.de/fileadmin/dateien-
dba/Drogenbeauftragte/Drogen
und Suchtbericht/
flipbook/DuS 2017/files/DuS 2017 download.pdf.
Last checked on Oct 31, 2017.
Dovis, S., van der Oord, S., Wiers, R. W., and Prins, P. J. M.
(2012). Can motivation normalize working mem-
ory and task persistence in children with attention-
deficit/hyperactivity disorder? the effects of money
and computer-gaming. Journal of abnormal child psy-
chology, 40(5):669–681.
duPont, P. (1995). Building complex virtual worlds without
programming. EUROGRAPHICS’95 State Of The Art
Reports, pages 61–70.
Eiler, T. J. (2018). Conception and implementation of an
application for the treatment of dependency disorders
HUCAPP 2019 - 3rd International Conference on Human Computer Interaction Theory and Applications
36

in virtual reality using gamification of the approach-
avoidance-task (aat). Master’s thesis, University of
Siegen.
Elenko, E., Underwood, L., and Zohar, D. (2015). Defining
digital medicine. Nature biotechnology, 33(5):456–
461.
Elliot, A. J. (2006). The hierarchical model of approach-
avoidance motivation. Motivation and Emotion,
30(2):111–116.
Epic Games (2017). Unreal engine features.
https://www.unrealengine.com/en-US/features.
Last checked on Oct 27, 2017.
Giraldi, G., Silva, R., and Oliveira, J. (2003). Introduction
to virtual reality. LNCC Research Report, 6.
Girard, B., Turcotte, V., Bouchard, S., and Girard, B.
(2009). Crushing virtual cigarettes reduces tobacco
addiction and treatment discontinuation. Cyberpsy-
chology & behavior : the impact of the Internet, mul-
timedia and virtual reality on behavior and society,
12(5):477–483.
Google LLC (2018). Poly: Explore the world of 3d.
https://poly.google.com/. Last checked on Mar 27,
2018.
Gorini, A., Griez, E., Petrova, A., and Riva, G. (2010). As-
sessment of the emotional responses produced by ex-
posure to real food, virtual food and photographs of
food in patients affected by eating disorders. Annals
of general psychiatry, 9:30.
Kakoschke, N., Kemps, E., and Tiggemann, M. (2017). Ap-
proach bias modification training and consumption: A
review of the literature. Addictive behaviors, 64:21–
28.
Leap Motion (2018). Leap motion: Reach
into virtual reality with your bare hands.
https://www.leapmotion.com/. Last checked on
Apr 23, 2018.
Lee, J., Lim, Y., Graham, S. J., Kim, G., Wiederhold, B. K.,
Wiederhold, M. D., Kim, I. Y., and Kim, S. I. (2004).
Nicotine craving and cue exposure therapy by using
virtual environments. Cyberpsychology & behavior
: the impact of the Internet, multimedia and virtual
reality on behavior and society, 7(6):705–713.
Lee, J. H., Ku, J., Kim, K., Kim, B., Kim, I. Y., Yang, B.-
H., Kim, S. H., Wiederhold, B. K., Wiederhold, M. D.,
Park, D.-W., Lim, Y., and Kim, S. I. (2003). Experi-
mental application of virtual reality for nicotine crav-
ing through cue exposure. Cyberpsychology & behav-
ior : the impact of the Internet, multimedia and virtual
reality on behavior and society, 6(3):275–280.
Lewin, K. (2013). Dynamic Theory of Personality - Selected
Papers. McGraw-Hill paperbacks. Read Books Ltd.
Machulska, A., Zlomuzica, A., Adolph, D., Rinck, M., and
Margraf, J. (2015). A cigarette a day keeps the goodies
away: smokers show automatic approach tendencies
for smoking–but not for food-related stimuli. PloS
one, 10(2):e0116464.
Machulska, A., Zlomuzica, A., Rinck, M., Assion, H.-J.,
and Margraf, J. (2016). Approach bias modification in
inpatient psychiatric smokers. Journal of psychiatric
research, 76:44–51.
MacLeod, C. and Mathews, A. (2012). Cognitive bias mod-
ification approaches to anxiety. Annual review of clin-
ical psychology, 8:189–217.
Marsh, A. A., Ambady, N., and Kleck, R. E. (2005). The ef-
fects of fear and anger facial expressions on approach-
and avoidance-related behaviors. Emotion (Washing-
ton, D.C.), 5(1):119–124.
Murphy, K. (2014). Cue exposure therapy: What the
future holds. https://www.rehabs.com/pro-talk-
articles/cue-exposure-therapy-what-the-future-holds/.
Last checked on Nov 11, 2017.
Pickover, C. A. and Tewksbury, S. K., editors (1994). Fron-
tiers of scientific visualization. A Wiley-Interscience
publication. Wiley, New York.
Rinck, M. and Becker, E. S. (2007). Approach and avoid-
ance in fear of spiders. Journal of behavior therapy
and experimental psychiatry, 38(2):105–120.
Sailer, M., Hense, J. U., Mayr, S. K., and Mandl, H. (2017).
How gamification motivates: An experimental study
of the effects of specific game design elements on psy-
chological need satisfaction. Computers in Human
Behavior, 69:371–380.
Schroeder, P. A., Lohmann, J., Butz, M. V., and Plewnia,
C. (2016). Behavioral bias for food reflected in hand
movements: A preliminary study with healthy sub-
jects. Cyberpsychology, behavior and social network-
ing, 19(2):120–126.
Schultze, U. (2010). Embodiment and presence in virtual
worlds: A review. Journal of Information Technology,
25(4):434–449.
Sherman, W. R. and Craig, A. B. (2003). Understand-
ing virtual reality: Interface, application, and design.
Morgan Kaufmann series in computer graphics and
geometric modeling. Morgan Kaufmann, San Fran-
cisco, CA.
Simpson, R. M., LaViola, J. J., Laidlaw, D. H., Forsberg,
A. S., and van Dam, A. (2000). Immersive vr for sci-
entific visualization: A progress report. IEEE Com-
puter Graphics and Applications, 20(6):26–52.
Slater, M., Perez-Marcos, D., Ehrsson, H. H., and Sanchez-
Vives, M. V. (2009). Inducing illusory ownership of a
virtual body. Frontiers in neuroscience, 3(2):214–220.
Tom Looman (2015). Multi-color outline post process
in unreal engine 4. http://www.tomlooman.com/
multi-color-outline-post-process-in-unreal-engine-4/.
Last checked on Mar 27, 2018.
Fighting Substance Dependency Combining AAT Therapy and Virtual Reality with Game Design Elements
37
