
Making Clinical Simulation Mannequins Talk
Isac Cossa
1
, Guilherme Campos
2
, Pedro Sá Couto
3,4
and João Lindo
4,5
1
Higher School of Nautical Sciences, Avenida 10 de Novembro, Maputo, Mozambique
2
Dept. of Electronics, Telecom. and Informatics (DETI) / IEETA, University of Aveiro, 3810-193 Aveiro, Portugal
3
Dept. of Mathematics (DMAT) / CIDMA, University of Aveiro, 3810-193 Aveiro, Portugal
4
School of Health Sciences (ESSUA) / Clinical Simul. Centre (SIMULA), University of Aveiro, 3810-193 Aveiro, Portugal
5
Centre for Health Technology and Services Research (CINTESIS), 4200-450 Porto, Portugal
Keywords: Speech Synthesis, Pre-recording, Case Study, Glasgow Coma Scale, Consciousness, Model, Markov Chain,
Training, Instructor, Usability, Evaluation.
Abstract: This paper advocates the interest of applying speech synthesis to clinical simulation mannequins, by focussing
on a particular case study of recognised practical interest (evaluation of consciousness level based on the
Glasgow Coma Scale), chosen as a proof of concept. A response repository comprising 109 sentences was
recorded and an application was developed in Microsoft® Visual Basic® to allow configuration of the
simulation scenario, control of response generation on a low-fidelity mannequin equipped with a loudspeaker
and assessment of trainee performance. The system received very positive assessment in initial user tests on
a typical training setting.
1 INTRODUCTION
The work presented here corresponds to the first
author’s MEng dissertation project. Its main
motivation was the rapid development observed in the
fields of clinical simulation and speech synthesis.
Because of its multiple advantages from the
standpoint of training procedure flexibility and safety,
clinical simulation based on mannequins has grown
and evolved very rapidly in recent decades. It now
plays an essential role in health care professional
training programmes in virtually every field of
specialisation (Brazão et al., 2015). Commercial
mannequin models range from low-fidelity (relatively
robust and inexpensive but with hardly any automated
features – mostly used at initial training stages) to
high-fidelity (featuring complex automation but very
expensive and relatively fragile – normally reserved
for advanced courses). In any case, their
sophistication level tends to increase, as realistic
interaction with trainees is obviously the main goal.
The ability to simulate verbal communication can be
a very valuable contribution towards this goal.
According to instructors working in medical school
laboratories, trainees tend to develop a kind of
emotional attachment to clinical simulation
mannequins. Almost invariably, they name them and
engage in pretend conversations during training
sessions, as if the mannequins could follow the
procedures and chat back. Furthermore, some
crucially important clinical evaluation and diagnosis
skills are directly dependent upon verbal
communication with patients. The training settings
should help practitioners develop those skills.
Speech and language processing technologies
have also been the object of increasing research and
development interest in the past 50 years. Speech
synthesis is one of the most active fronts. Algorithms
and applications are being constantly refined in terms
of audio output quality (realism), computation time
(to afford real-time operation) and application range
(availability in multiple languages). Practical usage is
growing in every field involving human-machine
interaction, including simulation (Taylor, 2009).
The potential for integration of sound synthesis in
clinical simulation settings is largely underexplored.
Simulation mannequins incorporating speech and
other vocal sound generation systems should be more
widespread, even because upgrading low-fidelity
mannequins for this purpose is relatively easy. In
support of this position, this paper presents a pilot
study on a particular health care training application
of widely recognised usefulness.
450
Cossa, I., Campos, G., Couto, P. and Lindo, J.
Making Clinical Simulation Mannequins Talk.
DOI: 10.5220/0007571404500455
In Proceedings of the 12th Inter national Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2019), pages 450-455
ISBN: 978-989-758-353-7
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All r ights reserved

Following introductory sections devoted to
describing a typical clinical simulation scenario and
very briefly reviewing available speech synthesis
software, section 4 justifies and presents the chosen
case study. Section 5 describes the software
application developed to implement it and section 6
reports initial user evaluation tests. The final section
discusses the results and considers some future work
possibilities.
2 CLINICAL SIMULATION
Health care training based on clinical simulation
typically involves the use of two rooms. Trainees (e.g.
nursing students) take their place in one of them,
normally referred to as simulation or training room,
which contains the simulation equipment proper (e.g.
mannequin ‘patient’ lying on a hospital stretcher).
The instructor (e.g. nursing teacher) normally sits at
the control or observation room. Figure 1 shows a
typical example, with adjacent training and control
rooms, separated by a glass window. Special
‘intelligent’ glass can be used to make visual contact
unidirectional (from control room to training room
only).
Figure 1: Clinical simulation setting (UNIFAE, 2017).
Normally, training rooms are fitted with audio-
visual equipment (lighting, video cameras,
microphones…), making it possible to record the
sessions and so document trainee performance for
analysis, evaluation and debriefing – a crucial
element in the training process. Also, so long as the
equipment is controllable remotely, multiple training
rooms can be assigned to a single, non-adjacent
control room.
In addition to observing and evaluating trainee
performance, it is desirable that the instructor be able
to control the training sequence, by specifying the
condition of the ‘patient’ and her reactions to each
possible trainee action. For this purpose, simulation
mannequins tend to incorporate increasingly
sophisticated hardware and software.
3 SPEECH SYNTHESIS
Speech synthesis systems generate human vocal
sound in a given language from content specified in
written form (text file). For this reason, they are also
called Text-to-Speech (TTS) systems. As Figure 2
illustrates, they comprise two main blocks: the front-
end translates the original text into phonetic symbols;
the back-end applies digital signal processing
algorithms to generate the corresponding audio files
(Barros, 2012).
Figure 2: Block diagram of a TTS system.
TTS systems are useful in an increasing number
of applications, such as presentation and digital book
readers, disability aids and automatic messaging.
Table 1 lists some of the most popular software
packages which have been developed for speech
synthesis (Freewarenee, n.d.); (Freewareneesite,
n.d.); (Manfio, 2012); (Araújo and Silva, 2013).
Table 1: Popular TTS software.
Synthesis
method
Operating
System
Portuguese
Language
Balabolka
Phonemes
Win, Linux,
MacOS
Yes
Voice Dream
Reader
Win, MacOS
Yes
Word Flash
Reader
Win, Linux
No
Espeak
Formants
Win, Linux
Yes
Loquendo
Win, Linux,
MacOS
Yes
Festvox
UniSyn /
diphones
Linux,
FreeBSD,
Solaris
Develop.
possible
An exploratory study on the usage of these
software packages indicated that Festvox would
probably be the best option in this context, due to its
open architecture. It is designed to support
independent development, making it possible to build
new voices and libraries for different languages
Language and
text analysis
Voice
generation
Text
file
Audio
file
Phonemes
Making Clinical Simulation Mannequins Talk
451

(Black and Lenzo, 2014). Unfortunately, no libraries
were yet available for Portuguese (the target language
in this case). Developing a new library is a lengthy
process, deemed unfeasible in the available period.
The software packages for which Portuguese
language libraries were available are characterised by
a closed architecture, which makes them unsuitable
for research purposes. They seemed to be designed
for relatively undemanding end-user applications: by
and large, the available voices sounded quite artificial
and prosody could not be altered.
In spite of their more convincing voices, even the
top commercial packages lack prosody control to
model emotion and excitation in the patient’s speech.
Moreover, libraries for different languages are sold
separately, adding to their (already high) cost.
4 CASE STUDY
4.1 Selection Criteria
The development of a speech generation tool for
Portuguese based on true synthesis would not fit the
time frame of an MEng dissertation. The chosen
alternative was the development of a proof of concept
based on pre-recorded sentences. This required
finding a particular case for which reasonably
realistic ‘dialogues’ could be built from a small
repository (otherwise, it too would be unfeasible) and,
in spite of this limitation, retained relevance from the
point of view of health care training. The choice fell
on the evaluation of consciousness based on the
Glasgow Coma Scale (GCS) – more specifically, its
‘verbal response’ parameter.
4.2 Glasgow Coma Scale
The GCS (Teasdale and Jennett, 2013) is widely used
in the diagnosis and monitoring of neurologic
dysfunction. It allows quantitative evaluation of
consciousness levels (in a 3-15 point range) based on
simple criteria (Santos et al., 2013), thus providing
health care practitioners an efficient and objective
means of reporting neurological status. The score is
obtained by observation of the patient’s behaviour,
either spontaneous or in response to verbal and/or
pain stimuli. Three evaluation parameters are
considered: eye opening response (1-4 points), motor
response (1-6 points) and verbal response (1-5
points). The focus was on this last one, as it involves
dialogue with the patient. The following criteria
apply:
Oriented Response (consciousness level S5):
patients oriented in space and time, who
coherently answer questions like “What’s your
name?” or “What day is it today?”, get top marks
i.e. 5 points.
Confused Response (consciousness level S4):
patients who are able to answer the same kind of
questions, but do it in a confused way, get 4
points.
Incoherent Response (consciousness level S3):
patients whose responses are not related to the
questions (taking the previous example, that
would be the case of answers like “I’m hungry” or
“I want to go home”) get 3 points.
Incomprehensible Response (consciousness
level S2): patients who respond with moans or
sounds not forming words, get 2 points.
No Response (consciousness level S1): patients
who do not respond verbally to any stimuli get the
lowest marks i.e. 1 point.
4.3 Response Repository
Normally, evaluation of a patient takes only five or
six questions. However, taking into account all the
relevant variables regarding the patient
(consciousness state, gender, age, emotional state…),
the evaluator (trainee) and the circumstances of the
interview (date, time…), an extremely large number
of responses would be required.
Based on the long GCS training experience of one
of the authors, a core set of questions was defined,
along with a selection of responses covering the five
consciousness levels, but considering a single type of
patient (adult male) and allowing only a limited
degree of variability for each level. This selection of
responses (109 sentences in total) were recorded in a
studio and post-processed for noise filtering and
amplitude normalisation.
5 APPLICATION
DEVELOPMENT
5.1 Requirements
The envisaged training setting is as described in
section 2. There are no particular requirements
regarding the mannequin other than being equipped
HEALTHINF 2019 - 12th International Conference on Health Informatics
452
with a loudspeaker to simulate vocal communication.
A low-fidelity model is perfectly suitable. The
‘dialogue’ with the trainee should be supported by a
computer application managed at the control room.
This should allow the instructor to pre-define training
scenarios, namely by specifying the desired
behaviour of the ‘patient’. For flexibility, immediate
intervention options should also be available to
bypass pre-defined scenarios in response to
unforeseen situations. The user interface should be
graphical (GUI) and intuitive.
The trainee is expected to approach the
mannequin (following all the protocols applicable to
interaction with hospital patients) and carry out the
questioning. For the reasons presented in 4.3, the set
of questions must be strictly defined.
Response playback will be triggered upon
question identification by the instructor. This should
convey to the trainee the impression of being in
conversation with a real patient. The responses,
played back through the mannequin’s loudspeaker,
should be consistent with the scenario defined by the
instructor and the corresponding questions.
The trainee is supposed to evaluate the responses
obtained, record the corresponding GCS score and
submit a diagnosis to the instructor. The application
should assess the trainee’s performance, provide
feedback on it and assign a classification.
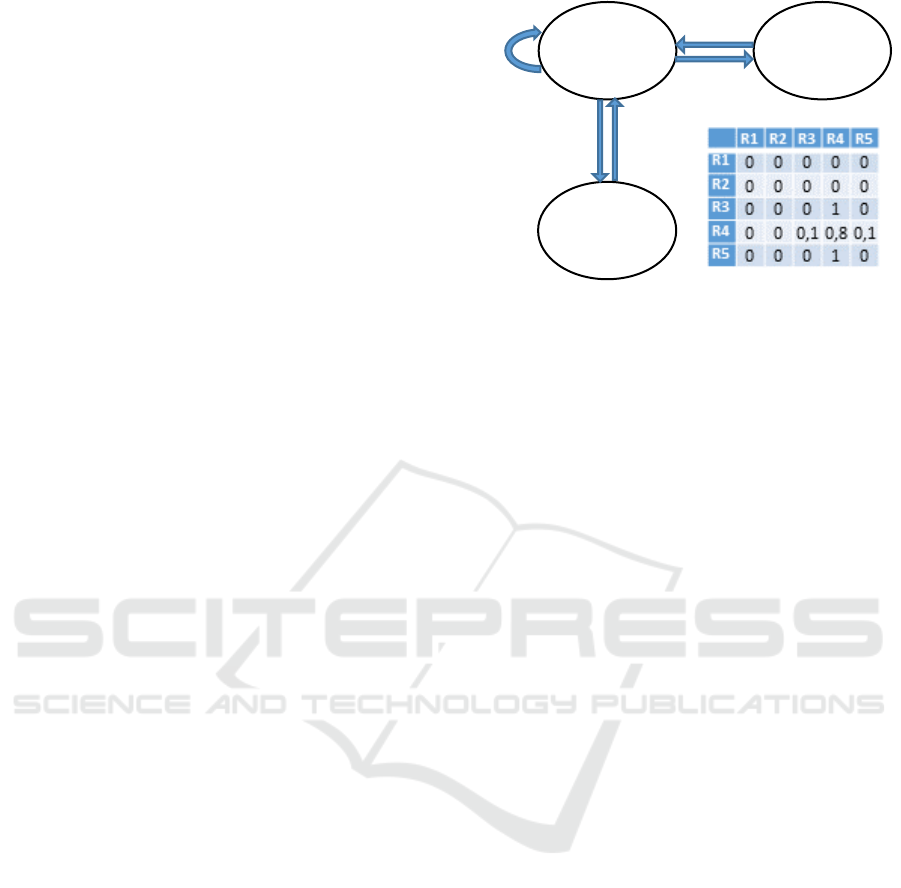
5.2 Response Generation Algorithm
In real situations, it is common to observe fluctuation
in the apparent level of consciousness (normally
between close GCS levels). Integrating that effect
into the simulation, in addition to increasing its
realism, is welcome from a training perspective, as
the correct evaluation becomes variable from
question to question. For that purpose, the response
generation algorithm developed for the mannequin
employed a probabilistic model based on Markov
chains (Childers, 1997), as illustrated in Figure 3. The
consciousness level fluctuation exhibited in the
responses is governed by transition probability
matrices, one per GCS level. These are configurable,
allowing the instructor to define any pattern of
response consciousness level, from strictly constant
to completely random.
Figure 3: Example of Markov chain response model for
consciousness level S4 allowing sporadic responses at the
levels immediately above and below, as defined by the
transition probability matrix shown.
Note it would be relatively easy to build appropriate
Markov chains to model more complex situations,
such as recovery or slow loss of consciousness.
5.3 User Interface
The application was developed in Visual Basic®. As
shown in Figure 4, its main window comprises three
panels:
Definitions: allows the instructor to enter the
configurations regarding the trainee and the
response generation mode, including the settings
of the Markov chain models described in the
previous point.
Interaction: is used to manage mannequin
responses through the identification of the
questions posed by the trainee. In automatic
mode, the algorithm chooses the response
according to the consciousness level determined
by the Markov chain model.
Evaluation: supports the analysis of the diagnosis
made by the trainee and works out her final marks
as a percentage.
6 TESTING
Initial user tests took place at one of the laboratories
of the University of Aveiro’s clinical simulation
centre (SIMULA), where a low-fidelity mannequin
was equipped with a miniature amplifier-loudspeaker
set. This was connected by bluetooth to the control
room computer, in which the application presented in
the previous section had been installed.
The tests involved seven nursing students acting
as trainees and their teacher in the instructor role. The
R4
Confused
response
R5
Oriented
response
R3
Inappropriate
response
1
1
0.1
0.1
0.8
Making Clinical Simulation Mannequins Talk
453
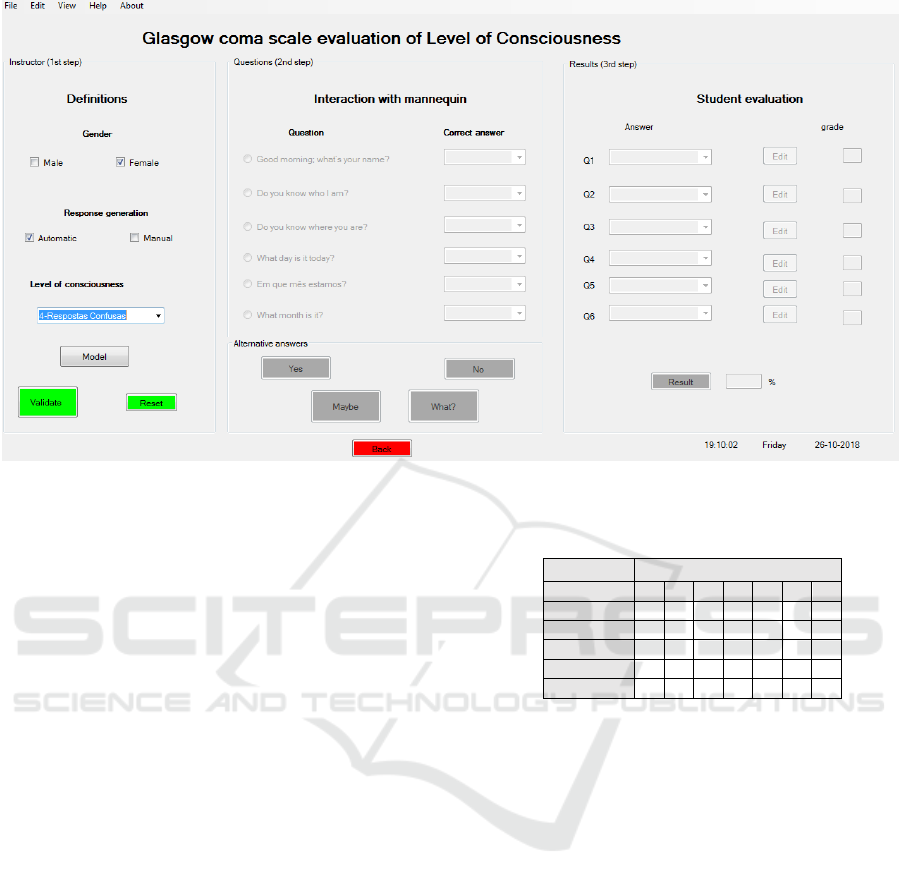
Figure 4: Application main page.
students carried out, and handed to the instructor,
their GCS consciousness level evaluations based on
a questionnaire for which a response repository had
been previously recorded, as explained in section
4.3.
At the end of the test session, the students
provided feedback by filling an evaluation form
based on the System Usability Scale (SUS)
proposed by John Brooke. They were asked to
indicate, on a range from 1 (“I totally disagree”) to
5 (“I totally agree”), to what extent they agreed with
the following statements:
1. This experience has stimulated my interest for
clinical simulation.
2. The simulation made it easier to learn the
Glasgow Coma Scale.
3. The simulation helped me develop my ability to
assess consciousness level using the GCS.
4. It was a pleasant and valuable experience.
5. Simulation mannequins equipped with speech
synthesis would be useful in several other
situations in our training course.
The resulting scores, shown in Table 2, are close
(low standard deviation) and high (total agreement
in most cases – averages between 4.57 and 5). It
should be mentioned that the lowest scores came
from a student who had missed the initial part of the
session (all the others attended the whole session).
Table 2: Assessment of the application by the trainees.
Trainee
Statement
1
2
3
4
5
6
7
1
5
5
5
4
5
5
3
2
5
5
5
5
5
5
5
3
5
5
5
5
5
5
4
4
5
5
5
4
5
5
5
5
5
5
5
5
5
5
5
7 DISCUSSION. FUTURE WORK
Although only small-scale initial tests could be
carried out, their results support the position that
incorporating vocal capabilities in simulation
mannequins can bring significant benefits in health
care training. The opinions and suggestions put
forward by the trainees in the evaluation form (an
area was reserved for that purpose) showed
enthusiasm with the experience, and interest in
repeating it with more time and a larger number of
questions. One of the suggestions was to generate
increasingly elaborate mannequin answers in the
course of the questioning. Since the GCS evaluation
protocol does not provide an opportunity for
simulating longer, more demanding dialogues, this
line of suggestions (which confirm the score
obtained for statement 5) encourage the exploration
of other application case studies. The instructor who
took part in the tests specifically suggested the area
of primary health care.
HEALTHINF 2019 - 12th International Conference on Health Informatics
454

Speech synthesis would bring obvious
advantages, since a virtually infinite set of dialogue
simulation scenarios could be programmed. That is
the main goal. However, given that prosody
manipulation is the main difficulty of speech
synthesis systems and clinical simulation
applications are especially demanding from that
point of view, this work suggests that, in some
application niches, systems based on pre-recorded
repositories may be interesting in their own right, to
the extent that they provide more realistic audio (at
least as regards prosody). This hypothetical interest
of pre-recorded speech does not hinder the
evolution to true synthesis – on the contrary, it may
constitute additional motivation for it.
In the current operation mode, the instructor
must identify the question, which demands constant
attention to the dialogue between trainee and
mannequin. It would be interesting to automate this
process and dispense (at least to a certain extent)
with instructor intervention. This would involve
equipping the mannequin with a microphone and
simulating hearing capability through the
incorporation of a question identification system
based on speech recognition.
ACKNOWLEDGMENTS
The authors wish to express their gratitude to
António Veiga, from the Dept. of Communication
and Arts (DeCA) of the University of Aveiro, for
his kind assistance with the use of DeCA’s
recording studio to build the response repository
and also to the ESSUA nursing students who agreed
to take part in the user evaluation tests.
This publication was supported by National Funds
assigned through the Foundation for Science and
Technology (FCT) to IEETA, a research unit of the
University of Aveiro, in the context of the project
UID/CEC/00127/2019.
REFERENCES
Brazão, M. L. Nóbrega, S. Correia, J. P., Silva, A., S.,
Santos, D. and Monteiro, M. H. (2015). ‘Simulação
Clínica: Uma Forma de Inovar em Saúde (Clinical
Simulation: A Way to Innovate in Health)’, Medicina
Interna, vol. 22/3 Jul-Sept: 146-155.
Taylor, P. (2009). Text-to-Speech Synthesis. Cambridge
University Press.
UNIFAE - Centro Universitário das Faculdades
Associadas de Ensino (n.d.). Laboratório de
Simulação Avançada. Retrieved November 2017
from http://www.fae.br/portal/laboratorio-de-simulac
ao-avancada/
Barros, M.J.A.S. (2012). Estudo Comparativo e Técnicas
de Geração de Sinal para a Síntese da Fala. MSc
dissertation. Faculty of Engineering of the U. of
Porto.
Freewarenee (n.d.). Sintetizadores de Fala Reconheci-
mento de Voz – Leitor de Texto. Retrieved August
2017 from http://freewarenee.weebly.com/sintetiza
dores-de-fala.html
Freewareneesite (n.d.). Software e Recursos Livres
Necessidades Especiais – Sintetizador. Retrieved
August 2017 from https:// freewareneesite.wordpress.
com/sintetizador/
Manfio, E.R. (2012). ‘Como funcionam alguns fonemas
no aplicativo Balabolka (How some phonemes in
application Balabolka works)’, Via Litterae, vol 4/2
Jul/Dec: 191-204.
Araújo, A.L.S.O. and Silva, J.S.O. (2013). ‘Educação e
tecnologia: alternativas de aplicativos facilitadores à
expressão oral para portadores de necessidades
especiais’, in 5º Simpósio Hipertexto e Tecnologias
na Educação. Retrieved November 2018 from
http://www.nehte.com.br/simposio/anais/Anais-Hipe
rtexto-2013
Black, A. W. and Lenzo, K. A. (2014). Building Synthetic
Voices (For FestVox 2.7 Edition). Retrieved
November 2018 from http://www.festvox.org/bsv/
bsv.pdf
Teasdale, G. and Jennett, B. (1974). ‘Assessment of coma
and impaired consciousness. A practical scale’.
Lancet, Jul 13;2(7872):81-4
Santos, W. C., Vancini-Campanharo, C. R., Lopes,
M.C.B.T., Okuno, M.F.P. and Batista, R.E.A. (2016).
‘Assessment of nurse’s knowledge about Glasgow
coma scale at a university hospital’. Einstein (São
Paulo), vol 14/2, Apr-Jun: 213–218.
Childers, D. G. (1997). Probability and Random
Processes: Using Matlab with Applications to
Continuous and Discrete Time Systems. Florida:
Richard D Irwin.
Making Clinical Simulation Mannequins Talk
455
