
Effects of Quadriceps Muscle Taping Application on Quadriceps
Muscle Strength and Walking Speed in Obese Patients with Knee
Osteoarthritis
Intan Sari Maharani, Tirza Z. Tamin
Department of Physical Medicine and Rehabilitation, Dr. Cipto Mangunkusumo General Hospital, Faculty of Medicine,
University of Indonesia, Jakarta, Indonesia
intansmohan@gmail.com, tirzaediva.tamin@gmail.com
Keywords: Taping, Quadriceps Muscle Strength, Walking Speed, Obese, Knee Osteoarthritis
Abstract: Obesity is well-known as a risk factor for knee osteoarthritis (OA). In such patients, weak quadriceps
muscle and decreased walking speed are commonly found. The study aimed to prove whether taping
application on quadriceps muscle in obese patients with knee OA affects quadriceps muscle strength and
walking speed. This study is a single-blind randomized controlled trial. Subjects are overweight or grade-
1 obese, knee OA (Kellgren-Lawrence 1-3) patients with Visual Analog Scale (VAS) of 1-4 who were
admitted to our obesity clinic on August-September 2019. One group received aerobic exercise with static
cycle and taping on quadriceps muscle, while the other received the same exercise, but with sham taping.
Taping was changed regularly 2 times a week for 4 weeks. The pain scale was assessed before, regularly
according to tape changed, and at the end of the study. While, quadriceps muscle strength and walking
speed were assessed before, at 2 weeks, and the end of the study. The taping group showed significant
improvement in pain, muscle strength, and walking speed (p<0.05). Improvement in pain also found in
the sham taping group. Taping application on quadriceps muscle improves muscle strength and walking
speed in obese patients with knee OA.
1 INTRODUCTION
Obesity is a condition in which the ratio of body
weight and height exceeds the prescribed standard.
The prevalence of obesity over the past four decades
has almost tripled. In 2016, adult obesity in the
world reached around 13% (WHO, 2018). In
Indonesia, based on the 2018 Riskesdas data, the
prevalence of obesity was has grown from 14.8%
(2013) to 21.8% (2018) (Riskesdas, 2018). Based on
data from the outpatient visits to the Medical
Rehabilitation Department of Cipto Mangunkusumo
Hospital, there were 2333 patient visits to the
obesity clinic in 2018.
Excess body weight is a condition that is closely
related to an increased risk for the emergence of
osteoarthritis (OA), especially in the joints
supporting the body, such as the knee. The
excessive and repetitive burden on the knee joint as
weight support will trigger biological changes that
will cause changes in water content, proteoglycans,
and collagen in the joint cartilage (King et al, 2013).
A cohort study by Reijmen et al (2007),
showed an association between increased body
mass index (BMI) and the incidence and
progression of knee OA (Reijmen et al, 2007)
Several studies have shown that patients with knee
OA have weak lower limb muscles, especially
quadriceps muscles and this muscle weakness is
correlated with the degree of knee pain and the
level of physical disability. Quadriceps muscle
weakness has been associated with functional
disorders such as an increased risk of falls and
slower walking speeds (Tani et al, 2018).
Individuals with knee OA have weaker
quadriceps muscles and show a shorter stance phase
during walking. In walking speed, the role of the
quadriceps muscle is to control knee flexion during
weight gain while the hamstring and gastrocnemius
muscles are stationary. In conditions of quadriceps
muscle weakness, hamstring and gastrocnemius
Maharani, I. and Tamin, T.
Effects of Quadriceps Muscle Taping Application on Quadriceps Muscle Strength and Walking Speed in Obese Patients with Knee Osteoarthritis.
DOI: 10.5220/0009089202650269
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 265-269
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
265

muscle contractions may be needed to help control
the knee (Tani et al, 2018).
Walking speed is one indicator that is very
important to see a decrease in functional ability,
which is associated with increased vulnerability, and
also other disabilities. Early detection of a decrease
in functional ability is very important to improve
quality of life and reduce the level of one’s
dependence (Ferre et al, 2017). One method for
measuring walking speed is 10-meters walking test
(Graham, 2008).
Kinesiology tape (KT) is a commonly used elastic
adhesive tape, this is developed by Kenzo Kase.
Hypotheses for the effects of the use of KT include
reduced pain, muscle strength facilitation, and
inhibition, which also increased the range of joint
motion. The manufacturer claims that KT can
facilitate muscle contraction if applied from origin to
insertion. This is presumably because the
mechanism of the KT recoiling force can be
transmitted to the fascia. This force can then help the
muscle contraction if the muscle contraction and KT
have the same pull direction. Another mechanism is
that the recoil ability of KT can stimulate the skin’s
mechanical receptors. This effect will increase the
excitability of the motor unit and cause the muscle
spindle reflex if the direction of the pull matches the
direction of the muscle contraction. Kinesio taping
allows the strengthening of weakened muscles by
stimulating gamma motor neurons (Yang et al,
2018).
Tamin et al (2018), conduct a randomized
controlled trial study with 12 participants in the
intervention group and 11 participants in the control
group to find the correlation between quadriceps
muscle strength and pain improvement with
functional disability status in obese with knee OA
after taping application. All participants were given
aerobic, knee strengthening exercises, and balance
exercises for 2 sessions per week for 3 weeks. This
study suggested that correlation with functional
activities was greater in pain than quadriceps
strength (Tamin et al, 2018).
A study was held by Tani et al (2018) to evaluate
the walking speed after applying Kinesio tape on
quadriceps femoris muscle in patients with knee OA,
hows the results that applying KT facilitated muscle
activation by increasing walking speed. This is
thought to be caused by stimulation of the
proprioceptive sense, muscle spindles, and
strengthened the muscle in the affected part (Tani et
al, 2018). But this study only conducted in 3 days,
which is not enough for increasing muscle strength
theoretically (Kisner, 2002).
Therefore, this study aims to see the effect of
kinesiology tape applications to quadriceps muscle
strength and walking speed in obesity and knee
osteoarthritis patients four weeks after application.
2 METHODS
This is a single-blind randomized controlled trial
study held in August 2019 until September 2019
involving 22 patients in our outpatient obesity clinic
in the Department of Medical Rehabilitation, Cipto
Mangunkusumo National General Hospital,
Indonesia. Consecutive sampling was performed to
recruit subjects. The subjects were divided into two
groups randomly. One group (n = 11) received
aerobic exercise with static cycle and taping on
quadriceps muscle, while the other (n = 11) received
the same exercise, but with sham taping. The
inclusion criteria were as follows: (1)
overweight/obese grade 1 patients with knee
osteoarthritis KL 1-3, (2) patient age ≥ 40 years old,
(3) no history of surgery in knee, (4) not have
exercise program at least within 2 weeks, (5) no
history of neurologic disorders and unstable heart
failure, (6) ability for walking without ambulatory
aid, (7) understand the command and instruction that
given, (8) not have allergic history of using
kinesiology taping, and (9) willing to participate in
this study. Exclusion criteria applied including: (1)
Patients who had a cognitive impairment, (2) had
knee deformity (knee varus/knee valgus) ≥ 15
0
, (3)
had balance disorders, (4) had visual disorders that
were not corrected, (5) had unstable
cardiopulmonary disease, and (6) not have a
willingness to participate the study.
In the intervention group (group A), Kinesiology
Tape (Leukotape
®
K Essity) was applied with a
facilitation technique, a 40% stretch, in quadriceps
muscle based on the standard used in Obesity
polyclinic of Medical Rehabilitation Department of
Cipto Mangunkusomo Hospital. Kinesiology Tape
was applied on rectus femoris muscle in Y strip that
starts from 10 cm below anterior superior ischiatic
spine until the superior border of the patella and on
vastus medial muscle that starts from 10 cm below
intertrochanter line until the medial border of patella
with the knee flexed 45
0
for both sides of the leg.
The kinesiology tape was changed every 3 days for 4
weeks. In the sham taping group (group B),
kinesiology tape was applied horizontally on
quadriceps muscle. Aerobic exercise using a static
cycle was given for both groups. The quadriceps
strength was assessed using a hand-held
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
266

dynamometer by other clinicians. Walking speed
was measured using the 10-meter walk test with
marked in 2 meters and 8 meters. Patients walked in
comfortable speed for 2 trials, and the average speed
between 2 meters and 8 meters was calculated in m/s.
Pain scale (VAS) was assessed before, every
week according to tape changed, and at the end of
the study. While, quadriceps muscle strength and
gait speed were assessed before, at 2 weeks, and the
end of the study. The conduction of this study had
been previously approved by the Ethical Committee
of the Faculty of Medicine, Indonesia University.
The analysis was conducted using SPSS version
20.0. Statistical significance was considered to be
the value of p ≤ 0.05. Descriptive analysis was used
to calculate the mean and standard deviation. The
intergroup comparison of demographic details was
performed using independent's t-test and non-
parametric Mann-Whitney U test and for intragroup
comparison paired t-test and Wilcoxon signed-rank
test was used.
3 RESULTS
No significant differences were determined between
the groups in respect of age, body weight, body
height, BMI (Body Mass Index), and VAS pain in
the baseline values. While there were differences in
the number of types of OA grade in both groups.
Table 1: Baseline characteristics of patients.
Variable
Group A
(n=11)
Group B
(n=11)
p
Age
63.18±6.90
63.36±3.80
0.94
*
KL
grade
Grade 2
4
8
Grade 3
7
3
Bodywei
ght
61.36±5.20
63.59±8.45
0.47
*
Body
height
149.45±4.89
154.05±4.98
0.41
*
IMT
27.43±2.33
26.76±2.20
0.49
*
VAS
3.82±0.41
3.55±0.52
0.18
**
*Unpaired t-test, **Mann-Whitney U test
At two weeks and the end of the study, there
were significant differences between the group in the
improvement of quadriceps muscle strength.
Walking speed showed significant differences
between the group at the end of the study (p=0.03).
Table 3 showed a comparison within the
group in VAS, quadriceps muscle strength, and 10
MWT. VAS was significantly decreased in both
groups at 2 weeks and 4 weeks. Quadriceps muscle
strength and walking speed at 2 weeks and 4 weeks
significantly improved in group A.
4 DISCUSSIONS
In knee OA patients there is a decrease in walking
speed associated with quadriceps muscle weakness
and pain experienced on the knee when walking. A
decrease in walking speed will cause a decrease in
one’s functional abilities (Tani et al, 2018).
Many studies have researched to see the effects
of increased muscle tone after the application of
Kinesio tape. But there were no studies that have
done taping alone without exercise to see an increase
in muscle strength caused by taping application.
This raises the question of whether an increase in
muscle strength occurs due to the effect of taping
application or the effect of exercise.
A study by Tani et al, 2018, showed that taping
application in facilitation technique increase walking
speed in patients with knee OA. This study was
conducted in three days (Tani et al, 2018). Perhaps
this is caused by a decrease in pain, but not an
increase in muscle strength. Because based on
theory, improvement of muscle strength can be seen
for 2 weeks, and more real for 4 weeks of training.
In this study, there was a significant
improvement of quadriceps muscle strength and
walking speed after taping application (facilitating
technique) on quadriceps muscle in obese patients
with knee OA after 2 weeks and 4 weeks. While the
pain scale decrease in both groups. Walking speed
suggested improving because of the reduction of the
pain scale, and the increase of quadriceps muscle
strength.
The decrease in pain after KT can be attributed
to the reduction in mechanical stress on free nerve
endings within the fascia through fascia unloading.
The application of KT created convulsions on the
skin which increased the interstitial spaces between
the sheets of fascia (Added A et al,2013). The
cutaneous stretch stimulation provided by KT
interferes with the transmission of mechanical and
painful stimuli leading to pain reduction (Morris et
al, 2013).
Taping over the skin constantly stimulates
cutaneous mechanoreceptors, thus providing more
Effects of Quadriceps Muscle Taping Application on Quadriceps Muscle Strength and Walking Speed in Obese Patients with Knee
Osteoarthritis
267

sensory signals to the central nervous system for
information integration, thus facilitating contraction
of inactive muscles. Besides, reduction of motor
neuron threshold induced by cutaneous stimulation
would influence the recruitment of the motor unit,
which can facilitate muscle contraction, and
ultimately improve muscle strength (Kouhzad et
al,2014; Donec V et al, 2012).
A meta-analysis study conducted by Yam et al,
2019 concluded that kinesiotape is effective in the
population with muscle fatigue and chronic
musculoskeletal diseases, but not in the population
without disabilities. Because KT will increase blood
circulation recovery by increasing nutrient and waste
change. KT may decrease pain by gate control
theory mechanism. KT provides tactile stimulation.
This stimulation may lead to the firing of large-
diameter afferent fibers, which close the gait to pain
signals transmitted by small-diameter afferent fibers.
This stimulation then decreased muscle soreness and
musculoskeletal pain and enhances muscle strength.
KT facilitates muscle strengthening by transmitting
a pulling force to the muscle fascia. KT may
stimulate mechanoreceptors. If the direction in
which KT is pulling matches the direction of muscle
contraction, KT could enhance the muscle spindle
reflex and increase the excitability of the motor units.
If applying in the opposite direction, KT will stretch
the Golgi tendon organs and will reduce the activity
of the motor neuron. But there is an insufficient
study that researches the physiological mechanism
of KT that affects muscle contraction (Yam et al,
2019).
The limitation of this study was a small number
of recruited samples. For future studies, it is
important to look for an increased motor unit
recruitment effect by taping applications by using an
objective measurement such as electromyography.
5 CONCLUSIONS
KT is effective for increasing muscle strength and
improve walking speed in obese and knee OA
patients in 4 weeks and also reduces pain scale
immediately. This study could be applicated in
obese and knee OA patients that restricted for
exercise because of their pain.
REFERENCES
WHO. Obesity and Overweight [Internet]. 2018. World
Health Organization. Available from:
http://www.who.int/mediacentre/factsheets/fs311/en/in
dex.html.
RISKESDAS. 2018. Hasil Utama RISKESDAS 2018.
King LK., March L., Anandacoomarasamy A., 2013.
Obesity & osteoarthritis. Indian J Med Res.
Reijman M., Pols HAP., Bergink AP., Hazes JMW., Belo
JN., 2007. Body mass index associated with onset and
progression of osteoarthritis of the knee but not of the
hip: The Rotterdam Study. Ann Rheum Dis.
Tani K., Kola I., Shpata V., Dhamaj F., 2018. Evaluation
of Gait Speed after Applying Kinesio Tape on
Quadriceps Femoris Muscle in Patients with Knee
Osteoarthritis. MJMS.
Ferre X, et al., 2017. Gait Speed Measurement for Elderly
Patients with Risk of Frailty. Mobile Information
Systems.
Graham J., 2008. Assessing walking speed in clinical
research: a systematic review. J Eval Clin Pract.
Yang L., Yang J., He C., 2018. The Effect of Kinesiology
Taping on the Hemiplegic Shoulder Pain: A
Randomized Controlled Trial. Journal of Healthcare
Engineering.
Tamin TZ., 2018. Efektifitas Elastic Taping Vs Sham Vs
Kontrol Grup Terhadap Kekuatan Otot dan Fungsi
Disabilitas pada Pasien OA Dengan Obesitas.
Penelitian, Jakarta.
Kisner C., Colby LA., 2012. The Wrist and Hand. In:
Therapeutic Exercise Foundation and Techniques 6th
ed. Philadelphia: FA Davis Company.
Added A., Costa O., Fukuda TY, de Freitas DG., Salomão
EC., Monteiro RL., Costa Lda C., 2013. Efficacy of
adding the Kinesio taping method to guideline-
endorsed conventional physiotherapy in patients with
chronic nonspecific low back pain: a randomized
controlled trial. BMC Musculoskeletal Disorders.
Morris D., Jones D., Ryan H., Ryan CG., 2013. The
clinical effects of Kinesio tex taping: A systematic
review. Physiother Theory Pract.
Kouhzad H., Khademi K., Naeimi SS., Pouretezad M.,
Shokri E., Tafazoli M., Dastjerdi M., Kardooni L.,
2014. Immediate and delayed effects of forearm
Kinesio taping on grip strength. Iran Red Crescent
Med J.
Donec V., Varzaityte L., Krisciunas A., 2012. The effect
of Kinesio taping on maximal grip force and key pinch
force. Pol Ann Med.
Yam ML., Yang Z., Zee BC., Chong KC., 2019. Effects of
Kinesio tape on lower limb muscle strength, hop test,
and vertical jump performances: a meta-analysis
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
268
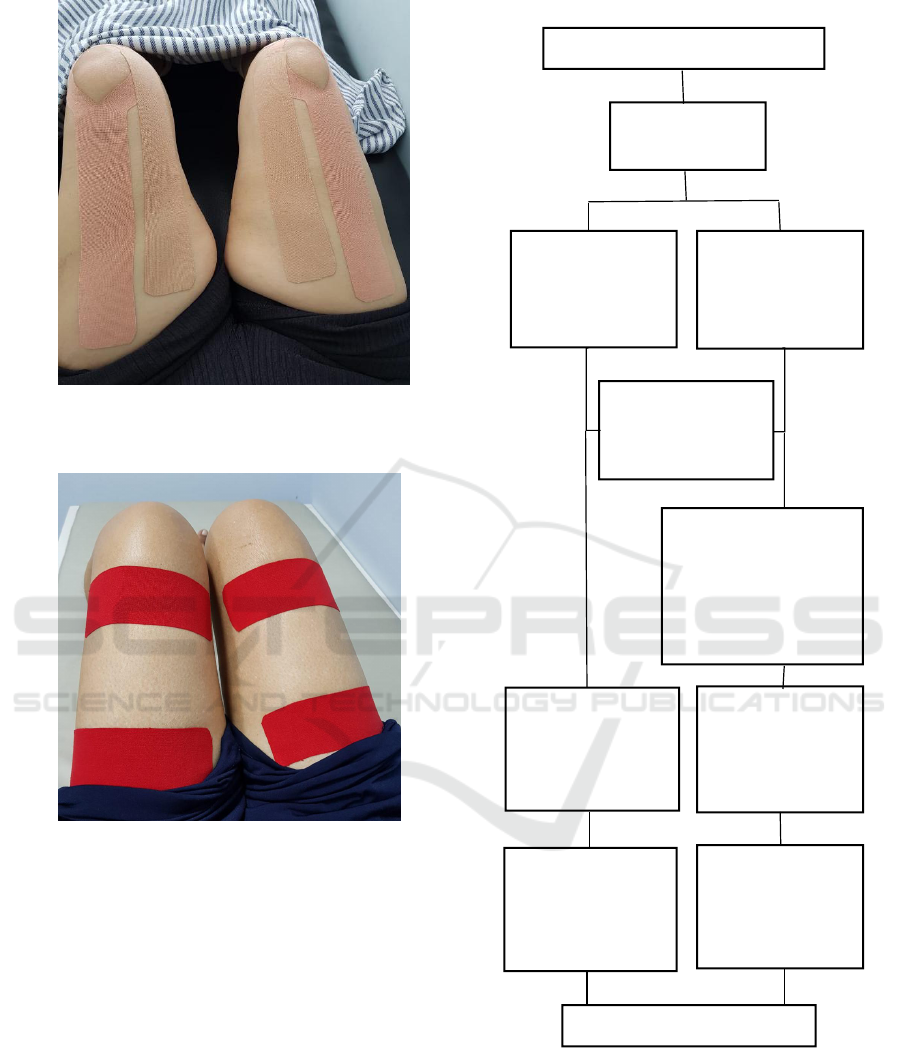
Figure 1: Kinesiology taping application in group A.
Figure 2: Kinesiology taping application in group B.
Consenting participants (n=22)
Randomization
(n=22)
Group A (n=11)
Kinesiotaping
quadriceps +
aerobic exercise
2 discontinued
treatment after 3 days
taping application
because of an adverse
event itch and rash
after taping application
Group B (n=11)
Sham taping
quadriceps +
aerobic exercise
Quadriceps
strength, walking
speed, VAS was
measured
11 patients
continued to study
after 2 weeks and
enrolled in the
second
measurement
9 patients
continued after 2
weeks and
enrolled in the
second
measurement
11 patients
continued after 4
weeks and enrolled
in the third
measurement
9 patients
continued to study
after 4 weeks and
enrolled in the
third measurement
Data were analyzed
Effects of Quadriceps Muscle Taping Application on Quadriceps Muscle Strength and Walking Speed in Obese Patients with Knee
Osteoarthritis
269
