
Intervention on Marital Satisfaction
for Wives of People with Schizophrenia
Novita Sari
1,2
. Sofia Retnowati
2
1
Psychology Department of Medicine Faculty, Universitas Syiah Kuala, Indonesia
2
Department of Psychology, Universitas Gadjah Mada, Indonesia
Keywords: Burden, Caregiver, Marital Satisfaction, Schizophrenia.
Abstract: Schizophrenia is characterized by profound disruption in cognition, emotions and behavior. Family
members as the primary caregiver for caring People with Schizophrenia (PWS). For PWS who have been
married, their couple has significant role. The couple of PWS experiences stress that results in burden of
caregiving. Wives of PWS have a higher burden than husbands of PWS. Burdened with an overabundance
of caregiving influences the marital dissatisfaction. This study aimed to analyze whether the intervention is
able to reduce the caregiving burden thereby increasing marital satisfaction for wives of PWS. The research
method used was single-case research experimental method with A-B-A design. The respondents was 3
(three) wives of PWS. All respondents experienced the burden decreasing after participating the
intervention. As their burden decreased, they experienced an increase in marital satisfaction. The results
indicated that the intervention was able to reduce caregiving burden so that it improved marital satisfaction
for wives of PWS.
1 INTRODUCTION
Schizophrenia is a severe disorder that can occur at
approximately seven per thousand of the adults’
population, mostly in age range of 15-35 years
(World Health Organization [WHO], 2013). The
average of 1% world population experience
Schizophrenia with onset on the teenage or early
adulthood phase. Schizophrenia is characterized by
profound disruption in cognition, emotions and
behavior. Symptoms are typically divided into
positive and negative symptoms. The positive
symptoms are those that appear to reflect an excess
or distortion of normal function, such as
hallucinations and delusions, whereas negative
symptoms are those that appear to reflect a
diminution or loss of normal function, such as
apathy, unusual emotional response, non-socialize,
reduced performance, and rarely speak (Maslim,
2001).
Caregiver plays the crucial role in supporting the
recovery of people with mental illness. The care
quality directly has effect on functioning of them
(Raj, Shiri, and Jangam, 2019). Family has a
significant role in caregiving for People with
Schizophrenia (PWS) (Hailemariam, 2015). For
PWS who have been married, their couple has
significant role (Shah, Wadoo, & Latoo, 2010). The
family member who become the caregiver for people
with mental illness reported there are numerous
challenges which affected to their life quality, such
as absence from work, financial problem, experience
a lot of negative emotion, lack of time to enjoy the
life and social problem (Hailemariam, 2015).
Most of family members who take a role as
caregiver of schizophrenia have the caregiver burden
in severe level. None of them has normal level of
caregiver burden (Hailemariam, 2015). Caregiver
burden is defined as a multidimensional response to
the negative appraisal and perceived stress due to the
care of people with mental disorders (Kim, Chang,
Rose, and Kim, 2012). It consists of two categories
which are objective and subjective burden (Schene,
Tessler, and Gamache, 1994). Objective burden is an
observable effects on caregiving, such as financial
problem, whereas subjective burden focuses on the
psychological stresses that can be reflected by
symptoms of anxieties, depression and low levels of
subjective welfare (Idstad, Ask, and Tambs, 2010).
276
Sari, N. and Retnowati, S.
Intervention on Marital Satisfaction for Wives of People with Schizophrenia.
DOI: 10.5220/0009447802760283
In Proceedings of the 1st International Conference on Psychology (ICPsy 2019), pages 276-283
ISBN: 978-989-758-448-0
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Wives of PWS experience in both of burden
categories (Idstad, et al., 2010). The most identified
aspect is burden to wives of PWS that is “anxiety
toward future”. The dominated aspect which become
the main attention is “accepting the sorrow and
grief” (Rose, 2011). They feel confused in order to
get interaction with PWS effectively (Mizuno,
Takataya, Kamizawa, Sakai and Yamazaki, 2012;
Rose, 2012). The wives of PWS express the negative
emotions, such as helplessness due to multiple roles
in family results in caregiving of husband, children
education, financial (Pashapu, et al, 2014). They also
experience the anxiety of her husband’s behavior
that will be inherited to their children (Mizuno, et
al., 2012).
The burdened spouses affect to marital
relationships such as extra marital affair and sexual
problem. The wives of PWS express negative
appraisal of caregiving and have negative
perceptions toward their marital life (Pashapu, et al.,
2014). Positive behavior is able to affects the marital
satisfaction directly, that is the acceptance of spouse,
whereas negative behavior is able to decreases the
marital satisfaction, such as blaming and criticizing
the spouse (Canel, 2013). More than that, lack of
spouse’s participation in marital relationship is the
result of mental illness which decreasing the marital
satisfaction (Diana, Sukarlan, and Pohan, 2012).
Marital satisfaction indicated by commitment to
continue the marriage, mutual respect, mutual
support, and mutual trust, openness, accepts the
partner conditions, doing activities together,
expressing the emotion and low levels stress of
marriage (Canel, 2013; Nimtz, 2011).
Based on Crisis Theory with ABC-X model
developed by Hill, high burden in caregiving
influence marital dissatisfaction (Madanian, Mansor,
and Omar, 2012). Crisis Theory explains how
couples react to stressful events. This models
consists of stressful events (A), the ability of
families to face stressful events (B), individual
appraisal of stressful events (C), and combined as a
determinant of the outcomes (X). Interaction of A-
B-C can contribute to the condition of marriage (X).
Lack of understanding about Schizophrenia,
communication skills, problem solving, stress
management, and lack of social support become
factor (B). Burdened with an overabundance of
caregiving as a result of individual appraisal of
caregiving becomes factor (C). Interaction of factor
A-B-C can influence the marital dissatisfaction (X).
Providing interventions can change the factor (B)
and (C), so that marital satisfaction may be increased
(X).
Based on previous research and PWS wives’
needs, the researchers compiled “Bangkit Program”
as an intervention for wives of PWS. The
researchers chose the name ”Bangkit Program”
because the word 'Bangkit' in Bahasa Indonesia has
several meanings, such as increasing awareness,
changing the passivity towards a more active and
motivating self to get starting a recovery process.
The term itself was cover the whole process of
recovery and giving motivational significance
(Subandi, 2006). “Bangkit Program” consists of
four (4) sessions: (1) Psychoeducation about
Schizophrenia; (2) Effective Communication Skills
Sessions; (3) Problem Solving Skills Session; and
(4) Stress Management Sessions (in “Bangkit
Program” named by being a Tough Spouse).
2 LITERATURE REVIEW
2.1 Caregiver Burden
Caregiver is a person who handle the responsibility
toward person who has mental illness problem,
therefore the caregiver is unable to have productivity
for a long term. Caregiver burden has a narrow
perspective comparing with family burden (Schene
et al., 1994). Caregiver burden involves emotional
loss due to process of caregiving, shameful feeling,
and the severe burden, financial problem, role and
lifestyle changing (Budd, Oles & Hughes, 1998).
People who are struggling with severe mental
illness, such as schizophrenia often bring out the
high level of stress and perceived burden in
caregiver (Sartorius, Leff, Lopez-Ibor, Maj, and
Okasha, 2005).
Caregiver burden consists of two dimensions that
are objective and subjective burden (Schene et al.,
1994). Objective burden is able to be observed and
measured by other people and consists measurable
effects on household, such as routine depending
which affected by caregiving, financial struggle,
whereas subjective burden is apperception of people
towards the effect of caring, such as guilty feeling
and anxiety about future (Mantovani, et al.,2016;
Schene et al., 1994).
2.2 Marital Satisfaction
Satisfaction identified as a level of a person to
express happiness and satisfaction to couple
(Harway, 2005). Marital satisfaction is how the
couple’s feeling toward her/himself, partner, and
her/ his marriage subjectively and relatively
Intervention on Marital Satisfaction for Wives of People with Schizophrenia
277

consistent (Bradbury, Fincham, & Beach, 2000).
Marital satisfaction formed by the interaction quality
between couples. Happiness toward her/ his
relationship with partner, her/ his feeling toward the
marriage, and the perception about marriage is a
factor affecting phase of marriage satisfaction. The
concept of marital satisfaction is unstable and
changeable constructed. The changing of
relationship quality and quantity are the main factor
which able to decrease the phase of marital
satisfaction (Canel, 2013). According to Oslon-
Siggg & Oslon (2011) there are 10 aspects of marital
satisfaction, they are communication, conflict
resolution, couple’s lifestyle and habit, financial
management, spending leisure time together,
affection and sexuality, friends and family, children
and caregiving, role equality, religions.
2.3 Schizophrenia
Schizophrenia is severe disorder characterized by
some symptoms which is related to severe disruption
in life function (Sartorius, et al, 2005). The
symptoms of schizophrenia disorder are disruption
in several crucial aspect, such as mind, perception,
intention, motoric behavioral, feeling or emotion,
and life functioning. The symptoms of schizophrenia
consists of 3 categories that are positive symptom,
negative symptom, and disorganization. Positive
symptom includes overwhelming and distortion,
such as hallucination and dilution. Whereas,
negative symptom consist of deficit behavioral, such
as avolition, alogia, blunted affect, anhedonia, and
asociality while disorganization is also known as
formal thinking disorder refers to a problem in
organization variety of thoughts and talking
(Davison, Neale and Kring, 2004).
3 RESEARCH METHOD
3.1 Respondent
Three wives were involved as respondent in this
(JM, NN, and SR). Researchers recruited them
through various institutions in Yogyakarta-
Indoensia, such as Community Health Centers
(Puskesmas) in Sleman-Yogyakarta, Indonesian
Schizophrenia Caring Community (Komunitas
Peduli Skizofrenia Indonesia), Puri Nirmala
Hospital, and Regional General Hospital Grhasia.
The inclusion criteria of the study are: (1) Being the
primary spouse for her husband who suffered
schizophrenia; (2) Live together with her husband
who had Schizophrenia; (3) Speak in Bahasa
Indonesian fluently; (4) Write and read well. Here is
the identities of survey respondents: fraud habit.
Table 1: Respondent’s Background.
Factors Respondent
JM
Respondent
NN
Responde
nt SR
Age 54 years old 55 years old 43 years
old
Education Elementary
School
Bachelor Junior
High
School
Etnic Java Java Java
Number of
Child(ren)
1 child 3 children 2 children
Occupatio
n
Farmer Housewife Labor
Month
income
< Rp
1.000.000
> Rp
2.500.000
< Rp
1.000.000
Duration
of Caring
17 years 5 years 18 years
Present
Husband’s
Job
farmer Pansion Jobless
3.2 Design and Data Analysis
This study used an experimental method to a single
case (Single-Case Research Design) aimed to test
the effect of an intervention by comparing the
different conditions on the same respondents
periodically (Kazdin, 1982). Single-Case Research
Designs used are A-B-A design.
The data was obtained for this study were
analyzed using descriptive and quantitative analysis
by using visual inspection based on score calculation
of burden and marital satisfaction. This visual
analysis aimed to evaluate the consistency of
“Bangkit Program” effect by comparing multiple
conditions (A-B-A). It is presented in graphs.
Descriptive analysis was obtained from
observations, interviews, and daily report book
during the research process. It aimed to get an
overview of in-depth study on the effect of each
respondent.
3.3 Measurement
The instruments used in this study were: (1) Burden
Scale modified from Rismarini (2013); (2) Marital
Satisfaction Scale (Fowers & Olson, 1993) which
has been modified; (3) Daily report book consists of
the events and feelings description of the
respondents from day to day and 25 items of
ICPsy 2019 - International Conference on Psychology
278
caregiving burden based on three aspects of Zarit,
Reever & Bach-Peterson Theory (Utami, 2011) and
it is intended as a self-monitoring; (4) “Bangkit
Program” Modules: and (5) Booklet containing
materials of “Bangkit Program”.
3.4 Experimental Procedures
Before presenting “Bangkit Program”,
researchers conducted a trial module by two
steps: (1) Professional judgment by
psychologists about the module content; and (2)
trial module of “Bangkit Program” for a wife
of PWS who has the same criteria as the study
respondents. Enforcement of trial module was
intended that “Bangkit Program”
implementation will be run in accordance with
“Bangkit Program” module procedures. After
conducting trial module, researchers made some
revisions so that when the entire research the
procedure of “Bangkit Program” can be
applied fully.
After conducting module trial, then
researcher carried out the research through three
(3) phases, namely baseline 1 phase (A
1
), the
intervention phase (B) and baseline 2 phase
(A
2
). In the baseline 1 phase (A
1
) researchers
did not provide any treatment to the respondent.
Respondents were asked to complete a daily
diary on this phase. After that, researchers
checked the daily report book, interviewed and
observed the respondent. In the end of baseline
1 phase (A
1
), researchers asked respondents to
fill out a pre-test of burden scale and marital
satisfaction scale.
Researchers provide “Bangkit Program” in
intervention phase (B). “Bangkit Program”
materials was delivered by a pschyologist as
facilitator in “Bangkit Program” training.
During the intervention phase (B), the
respondents were asked to fill in daily report
book every day. Then in the end of “Bangkit
Program” training, respondents were asked to
fill out a post-test of marital satisfaction scale
and burden scale. While Baseline 2 Phase (A
2
)
is for withdrawing “Bangkit Program”
intervention. Respondents were also asked to
complete daily report book. In the end of
baseline 2 phase (A
2
), researchers provided
follow-up test of burden scale and marital
satisfaction scale to respondents.
4 RESULT
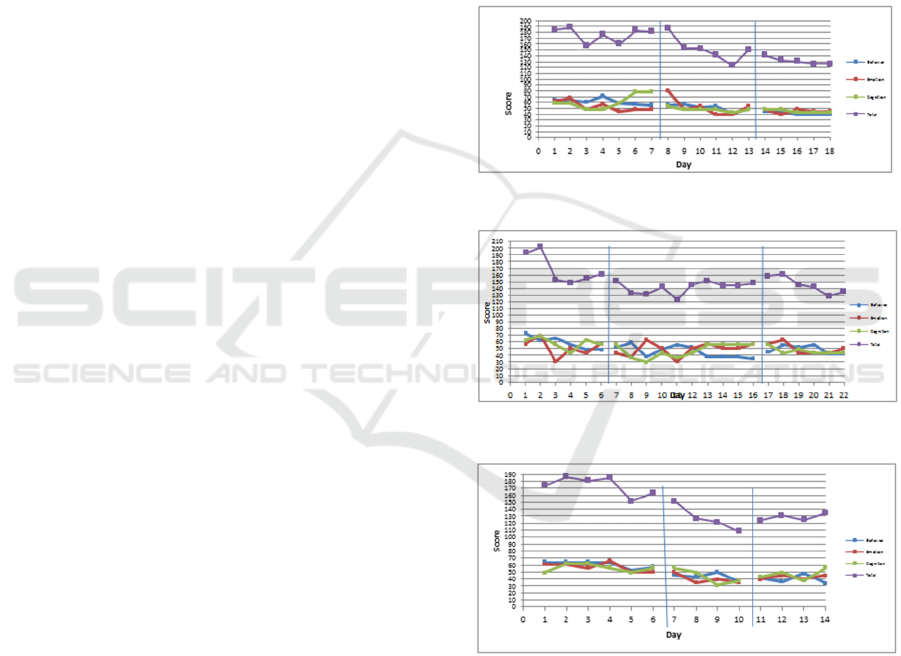
4.1 Burden Level based on Daily
Report Book
Three respondents’ caregiving burden decreased.
Figure 1, Figure 2, and Figure 3 is the score obtained
by the respondents’ burden based on daily report
book:
Figure 1: Burden Score of Respondent JM.
Figure 2: Burden Score of Respondent NN.
Figure 3: Burden Score of Respondent SR.
Based on mean of burden of respondent JM
(Figure 4), NN (Figure 5), and SR (Figure 6), all of
them experienced a decrease in burden at
intervention phase (B) and baseline 2 phase (A
2
) as
compared to baseline 1 (A
1
).
Intervention on Marital Satisfaction for Wives of People with Schizophrenia
279
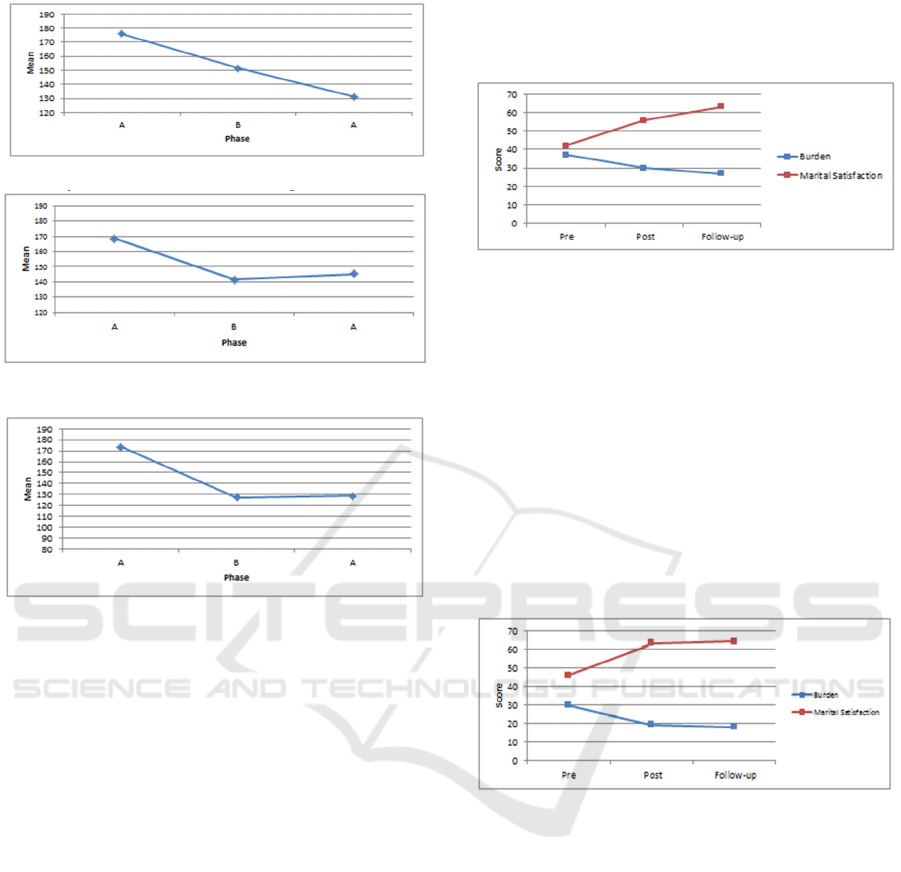
Figure 4: Mean of Burden of Respondent JM.
Figure 5: Mean of Burden of Respondent NN.
Figure 6: Mean of Burden of Respondent SR.
Mean of burden of respondent JM in baseline 1
phase (A
1
) was X,¯ = 175.82 (SD = 12.26),
intervention phase (B) was X,¯ = 151, 46 (SD =
21.28) and baseline phase 2 phase (A
2
) was X,¯ =
131.06 (SD = 2.62). Respondent NN had mean of
burden in baseline 1 phase (A
1
) was X,¯ = 168.78
(SD = 22.5), intervention phase (B) was X,¯ =
141.53 (SD = 9.48), and baseline 2 phase (A
2
) was
X,¯ = 145.31 (SD = 12.96). Respondent SR had
mean of burden in baseline 1 phase (A
1
) was X,¯ =
173.35 (SD = 13.53), intervention phase (B) was
X,¯ = 127.09 (SD = 17.9), and baseline 2 phase (A
2
)
was X,¯ = 128.7 (SD = 4.91).
4.2 Burden and Marital Satisfaction
According to mean of burden on daily report book
and Burden Scale indicated that respondent JM
experienced decreasing burden level, both at post-
test and follow-up test. The decrease in burden
levels was followed by an increase in marital
satisfaction scores of respondents JM. The increase
in marital satisfaction scores in post-test by 15
points, whereas at follow-up by 22 points from pre-
test scores (Figure 7). It indicated that “Bangkit
Program” could reduce the caregiving burden, so
that marital satisfaction increased. The effect of
“Bangkit Program” persisted until the follow-up
period.
Figure 7: Burden and Marital Satisfaction of Respondent
JM.
Based on Burden Scale, respondent NN’s burden
scores decreased during post-test by 11 points and
follow-up by 12 points. The decrease in burden
score influenced marital satisfaction scores (Figure
8). The marital satisfaction scores increased
consistently from post-test to follow-up test. Marital
satisfaction score increased singnificantly by 17
points at post-test, while at follow-up increased by
18 points. Thus, “Bangkit Program” could reduce
the caregiving burden, so that marital satisfaction
increased in respondent NN. The effects of “Bangkit
Program” persisted in respondent NN.
Figure 8: Burden and Marital Satisfaction of Respondent
NN.
The decrease caregiving burden score and the
increase marital satisfaction were not only
experienced by respondent JM and NN, but also
respondent SR. Based on respondent SR’s Burden
Scale, its scores significantly decrease in post-test by
14 points and follow-up test by 15 points. The
decrease in caregiving burden was followed by an
increase in marital satisfaction scores. According to
post-test measurement, respondent SR had increased
by 6 points. Similarly, the follow-up measurement of
marital satisfaction increased significantly by 17
points.
ICPsy 2019 - International Conference on Psychology
280

Figure 9: Burden and Marital Satisfaction of Respondent
SR.
Based on the visual analysis of 3 (three)
respondents above, it could be concluded that
“Bangkit Program” could reduce the caregiving
burden, so that marital satisfaction increased on
wives of PWS. “Bangkit Program” had long-term
effects in all respondents.
4.3 Effectiveness of “Bangkit
Program” Intervention
Respondent JM
Before getting “Bangkit Program”
intervention, respondent JM believed that her
husband got a disease because of being spelled
by her stepmother, so that she did not seek
medical treatment for him. After getting an
explanation of Schizophrenia in Session 1:
psychoeducation, he had begun to realize that
her husband was having psychiatric disorders
because the schizophrenia symptoms are
exactly the same as that of her husband. At the
end of the first session, she intended to seek
immediate medical treatment for her husband.
Based on Figure 1, respondent JM’s emotion
aspect scores increased when the first session
(on day 8). It is caused by a deep concern about
the future husband, feeling sad, guilty, and
ashamed.
Respondent JM had another benefit of
“Bangkit Program”, that is ability to
communicate with neighbors. She began to
explain about schizophrenia to neighborhood,
so that they were able to understand the
circumstances of her husband and not isolate
him from society. By understanding of
schizophrenia and communication skills with
the neighborhood around, appearing behavioral
changes in the society, such as they paid
attention to respondent JM and her husband
condition, offer transportation assistance when
respondent JM intended to bring her husband
to the hospital, and got no fear anymore to
interact with JM’s husband.
Respondent NN
Before getting “Bangkit Program”, respondent
NN often overlook her condition and very
focused on her husband's condition so that he
left a lot of outside activities. After the
“Bangkit Program” intervention, respondent
NN realized that she also needs entertainments
and activities that can make her happy.
Previously NN pinched her husband when she
asked him to take a bath, eating, or sleeping.
This condition happens because NN felt
annoyed, tired and impatient with her
husband's behavior. Instead, after joining
“Bangkit Program” she realized that her
behavior like that couldn’t support the recovery
for her husband. Nowadays if she have started
feel tired, upset, or disappointed, she will
practice the relaxation that has been taught at
each session of “Bangkit Program”.
NN stated that she accepted her husband's
condition sincerely, but she felt sadness,
disappointment, and helplessness. In follow-up
session of “Bangkit Program” respondent NN
reported that her feeling right now is getting
better, just before she could not noticed her
husband’s improvement because of her sadness
and helplessness. Nowadays no matter how
small the change is shown by her husband,
responden NN appreciates it, such as her
husband is able to eat the cake without
respondent NN’s help, laughing while
watching comedy on television, and so on.
Respondent SR
SR Respondents showed some positive
behavior change in caregiving after getting
“Bangkit Program”. Based on observations
and interviews in baseline 1 phase, respondent
SR often do not care and avoid her husband.
Otherwise, after getting “Bangkit Program”
intervention, respondent SR gave caring and
communicate effectively to her husband. In
addition, respondent SR also began to make a
joke with her husband after she got “Bangkit
Program” intervention. These conditions
indicated that by decreasing caregiving burden,
respondent SR get better interaction with her
husband (PWS), so that marital satisfaction
increased.
5 DISCUSSION
This study uses a single case design, so that the
causal correlation between intervention and behavior
change can be explained deeper. Respondents have
Intervention on Marital Satisfaction for Wives of People with Schizophrenia
281

different characteristic based on education, duration
of caring, and economic conditions. In addition,
these differences among respondents can enrich the
wealth of knowledge.
All three respondents who involved in study
showed sadness and sorrow accept experienced. This
condition should be a concern in the intervention
process. That is dominant aspect that should be the
center of attention for researchers that receive
sadness and grief. It shows the attitude of despair
and helplessness wrapped in words that can be
accepted by society (Rose, 2011).
The experience most occurred in PWS couple
focuses on finance, future, exhausted, isolated, and
workload beyond (Mizuno, et al., 2012).
Respondent NN has slightly on financial problem
because her husband has retirement benefits that can
fulfill the needs of the family. Nonetheless
respondent NN felt isolated, tired, and have a high
workload, whom taking care of the husband, such as
help eating, drinking, defecating and, bathing her
husband. Whereas, the burden experienced by
respondent JM and SR is greater in financial
problems. They did not need to take care of her
husband (PWS) as done by NN because their
husbands are already independent. But the difficulty
in financial situation made them frustrated and tired,
to be worked hard to meet the needs of family, while
their husband's physical condition were good but do
not able to help the family finances. These
conditions made negative feelings in both
respondent JM and SR against her husband, such as
angry, upset, and disappointed.
For wives of PWS, social support plays a very
important role to reduce the caregiving burden
(Robinson, Rodhers, & Butterworth, 2008). It is also
experienced by all respondents. When they were
able to ask the help from others, it made
opportunities for their husbands (PWS) to get
support from various parties. Communication skill,
seek help from others and problem solving were
taught in the “Bangkit Program” to the respondents
of this study can decrease the caregiving burden.
The burden experienced by all respondents causes
decreased marital satisfaction (Fitzpatrick & Haase,
2010; Madanian, et al., 2013). When the
respondents’ burden decreased, they made positive
interactions and acceptance of a husband. It resulted
in increased marital satisfaction. Higher stress and
burden level, then lower marital satisfaction (Canel,
2013). Therefore, all respondents who received the
intervention “Bangkit Program” got marital
satisfaction increased significantly due to the
decreasing caregiver burden.
6 CONCLUSION
Based on the results of this study indicate that all
three respondents whose caregiving burden had
decreased significantly after interventions of
“Bangkit Program”. As the burden decrease, the
marital satisfaction increased. There is no
differences in reduction of burden based on the
duration of taking care, economic status and level of
education. Thus, “Bangkit Program” can be applied
to wives of PWS with various levels of education,
economic status, and duration of care for the
reduction the caregiving burden. Hypothesis of this
study is accepted that “Bangkit Program” can
reduce the caregiving burden so that marital
satisfaction increased.
Based on the implementation of this study, the
research put forward several recommendations for
further research, they are: (1) additional media other
than the booklet can help respondents understand the
material better, such as using video; (2) “Bangkit
Program” materials delivering can be adjusted to
respondents understanding level; (3) Module of
psycho-education sessions can be conducted in two
sessions, so that the respondent can dig deeper
knowledge about schizophrenia and had a longer
time to reveal the experiences (sharing) during the
accompaniment process.
REFERENCES
Bradbury, T., Fincham, F., & Beach, S. (2000). Research
on the Nature and Determinants of Marital
Satisfaction: A Decade in Review. Journal of Marriage
and the Family, Vol. 62 (4) , 964-980.
Budd R.J., Oles G, & Hughes I,C. (1998). The
Relationship Between Coping Style and Burden in the
Carers of Relatives with Schizophrenia. Acta
Psychiatrica Scandinavica. Vol. 98 (4). 304-9.
Canel, A. (2013). The Development of the Marital
Satisfaction Scale. Education Sciences; Theory &
Practice. Vol 13 .
Davison, G.C, Neale, J.M and Kring, A.M. 2004.
Psikologi Abnormal. Jakarta: PT Raja Grafindo.
Diana, C., Sukarlan, A., & Pohan, L. (2012). Hubungan
antara Caregiver Strain dan Kepuasan Pernikahan pada
Istri Sebagai Spouse Caregiver dari Penderita Stroke.
INSAN, Vol. 14 (3) , 171-178.
Fitzpatrick, K., & Haase, T. (2010). Marital Satisfcation
and Resilience in Caregivers of Spouses With
Dementia. Clinical Gerontologist Vol. 33 , 165-180.
ICPsy 2019 - International Conference on Psychology
282

Fowers, B., & Olson, D. (1993). ENRICH Marital
Satisfaction Scale: A Brief Research and Clinical Tool.
Journal of Family Psychology Vol. 7 (2) , 176-185.
Hailemariam, K.W. (2015). The Psychological Distress,
Subjective Burden and Affiliate Stigma among
Caregiver of People with Mental Illness in Amanuel
Specialized Mental Hospital. American Journal of
Applied Psychology. Vol (4 (2), 35-49.
Harway, M. (2005). Handbook of Couple Therapy. New
Jersey: John Willey & Sons.
Idstad, M., Ask, H., & Tambs, K. (2010). Mental Disorder
and Caregiver Burden in Spouse: the Nord-Trondelag
health Study. BMC Public Health Vol 10, 516.
Kazdin, A.E. (1989). Single-Case Research Designs:
Methods for Clinical and Applied Settings. New York:
Oxford University Press.
Kim, H., Chang, M., Rose, K., & Kim, S. (2012).
Predictors of Caregiver Burden in Caregivers of
Individuals with Dementia. Journal of Advanced
Nursing Vol. 68 (4) , 846-855.
Madanian, L, Shafeq, S.M, & Omar, A.H. (2013). Marital
Satisfaction of Iranian Female Student in Malaysia: a
Qualitattive Study. Social and Behavioral Sciences,
Vol. 84, 987-993.
Maslim, R. (Ed.). (2001). Buku Saku: Diagnosis
Gangguan Jiwa. Jakarta: Bagian Ilmu Kedokteran Jiwa
FK Unika Atma jaya.
Mizuno, E., Takataya, K., Kamizawa, N., Sakai, I., &
Yamazaki, y. (2012). Female Families' Experiences of
Caring for Persons with Schizophrenia. Archieves of
Psychiatric Nursing , 1-10.
Nimtz, M. A. (2011). Satisfaction and Contributing
Factors in Satisfying Long Term Marriage: A
Phenomenological Study. Liberty University.
Olson-Sigg, A., & Olson, D. (2011). PREPARE/ENRICH
Program for Premarital and Maried Couples. Case
Studies in Couple Therapy , 1-12.
Pashapu, D.R., Hamza, A., Chandra, P.S., & Marimuthu.
(2014). Qualitative Study on the mArital Needs of
Couples with a Spouse Living with Schizophrenia in
India. IJRSI. Vol. 1(1). 5-11.
Raj, E.A., Shiri, S and Jangam, K.V. (2019). Subjective
Birden, Psychological Distress, and Perceived Social
Support Among Caregivers of Person with
Schizophrenia. Indian Journal of Social Psychiatry.
Rismarini, N.A. (2013). Hubungan Antara Beban Fisik,
Beban Psikologis, dan Esktraversi dengan
Penyesuaian pada Family Caregiver Pasien
Skizofrenia. Yogyakarta: Fakultas Psikologi
Universitas Gadjah Mada.
Robinson, E., Rodhers, B., & Butterworth, P. (2008).
Family Relationship and Mental Illness Impact and
Service Responses. Australian Family Relationships
Clearinghouse No.4 .
Rose, L., Mallinson, R., & Gerson, L. (2011). Mastery,
Burden, and Areas of Concern Among Family
Caregivers of Mentally Ill Person. Archieves of
Psychiatric Nursing Vol. 20 (1), 41-51.
Sartorius, N., Leff, J., Lopez-Ibor, J.J., Maj, M., &
Okasha, A. (2005). Families and Mental Disorder:
From Burden to Empowerment. England: John Wiley
& Sons
Shah, A., Wadoo, O., & Latoo, J. (2010). Psychological
Distress in Carers of People with Mental Disorder.
British Journal of Medical Practitioners, Vol 3 (3)
.
Schene A.H., Tessler R.C., Gamache G.M. (1994).
Instruments Measuring Family or Caregiver Burden in
Severe Mental Illness. Social Psychiatry and
Psychiatric Epidemiol. Vol. 29 (5), 228-240.
Subandi, (2006). Psychocultural Dimension of recovery
from First Episode Psychosis in Java. Department of
Psychiatry School of Medicine, Faculty of Health
Sciences. Adelaide: The University of Adelaide.
Utami, W. (2011). Hubungan Antara Pengetahuan
Tentang Skizofrenia dan Stretegi Koping dengan
Beban Psikologis pada Family Caregiver Orang
dengan Skizofrenia. Yogyakarta: Universitas Gadjah
Mada.
WHO. (2013). Schizophrenia. Retrieved 6 7, 2013, from
World Health Organization: http://www.who.int
Intervention on Marital Satisfaction for Wives of People with Schizophrenia
283
