
Resolving Differences of Opinion between Medical Experts: A Case
Study with the IS-DELPHI System
Derek Sleeman
1
, Kiril Kostadinov
1
, Laura Moss
1,2
and Malcolm Sim
2
1
Computing Science Department, The University of Aberdeen, AB24 3FX, U.K.
2
Academic Unit of Anaesthesia, Pain and Critical Care, School of Medicine, University of Glasgow, G31 2ER, U.K.
Keywords: Expertize Capture, Clinical Decision Support Systems, Inconsistencies, Negotiations, DELPHI-approach,
Refinement, Cognitive Informatics, Medical Informatics, Pattern Recognition and Machine Learning.
Abstract : Knowledge intensive clinical systems, as well as machine learning algorithms, have become more widely
used over the last decade or so. These systems often need access to sizable labelled datasets which could be
more useful if their instances are accurately labelled / annotated. A variety of approaches, including statistical
ones, have been used to label instances. In this paper, we discuss the use of domain experts, in this case
clinicians, to perform this task. Here we recognize that even highly rated domain experts can have differences
of opinion on certain instances; we discuss a system inspired by the Delphi approaches which helps experts
resolve their differences of opinion on classification tasks. The focus of this paper is the IS-DELPHI tool
which we have implemented to address the labelling issue; we report its use in a medical domain in a study
involving 12 Intensive Care Unit clinicians. The several pairs of experts initially disagreed on the
classification of 11 instances but as a result of using IS-DELPHI all those disagreements were resolved. From
participant feedback (questionnaires), we have concluded that the medical experts understood the task and
were comfortable with the functionality provided by IS-DELPHI. We plan to further enhance the system’s
capabilities and usability, and then use IS-DELPHI, which is a domain independent tool, in a number of
further medical domains.
1 INTRODUCTION AND
LITERATURE REVIEW
Knowledge intensive systems are pervasive across a
wide range of industries (e.g. industrial, healthcare,
automotive) and applications (e.g. expert systems,
tutoring systems, adaptive interfaces). These systems
often require domain knowledge which can then be
exploited to address a range of tasks. Knowledge
acquisition is the process of acquiring knowledge for
subsequent use in knowledge intensive systems. One
method to perform knowledge acquisition is through
direct interaction with domain experts.
Experts’ judgements are highly regarded,
accurate, and can be characterized by: “employing
more effective strategies than others; perceiving
meaning in patterns that others do not notice; form
rich mental models of situations to support sense
making and anticipatory thinking; have extensive and
highly organised domain knowledge; and are
intrinsically motivated to work on hard problems that
stretch their capabilities”, (Klein et al, 2017).
However, there are a wide range of challenges
faced in the elicitation of knowledge from experts in
order to acquire accurate and useful knowledge,
(Shadbolt & Smart, 2015). In this paper we focus on
differences which may be found between experts’
performance during a knowledge acquisition task.
Although highly regarded, a domain expert may still
display errors or inconsistencies in their performance.
Cognitive biases (e.g. in deterministic and non-
deterministic reasoning, (Tversky & Kahneman,
1974)) have been shown to occur in expert reasoning,
(Fischhoff, 1989). Other conditions in which a
domain expert’s performance can be affected include:
experts can ‘gloss over’ information i.e. miss surface
detail and overlook features; context dependence
within a domain i.e. without contextual-enabling
information, experts may be more limited in their
abilities; and inflexibility i.e. experts can have
problems adapting, for example, to (significant)
changes in basic domain concepts, (Chi, 2006). In
dealing with uncertain scenarios, such as in the
medical domain, people, including experts, often
66
Sleeman, D., Kostadinov, K., Moss, L. and Sim, M.
Resolving Differences of Opinion between Medical Experts: A Case Study with the IS-DELPHI System.
DOI: 10.5220/0008922000660076
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 66-76
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

make mistakes as they deviate from decision theory.
1
Although we have described how an expert’s
performance may be negatively affected, it is
suggested that the observed effect is smaller than in
non-experts, (Shields et al, 1987). Further, in some
cases, biases can be considered as useful components
of expertise; at least this is the perspective of the
naturalistic decision-making movement, (Klein et al,
1986).
Several knowledge elicitation tools have been
developed to help overcome some of the challenges
faced during knowledge elicitation. Of particular
interest to the work reported here are approaches
which help experts detect and resolve differences
when performing a task. One way to address the
problem of differing opinions between experts is to
perform a Delphi exercise during which perceived
differences between experts are resolved through
several rounds of discussions, (Murry & Hammons,
1995). Other methods to enable consensus with group
decisions, include the Analytical Hierarchy Process,
(Saaty, 2008) and the Nominal Group Technique,
(Dunnette et al, 1963).
Software tools have been developed to help
support such activities. Open Source ACH is a freely
available implementation of the Analysis of
Competing Hypotheses (ACH) method
2
. In the tool, a
table (or matrix) is displayed with hypotheses
presented in columns and evidence presented in rows.
Each piece of evidence (a row) is then compared with
each of the hypotheses (columns) and a level of
consistency is noted. Aengenheyster et al, 2017
provide a survey of electronic “real-time delphi” tools
with a focus on the following tools: Risk Assessment
and Horizon Scanning (RAHS)
3
, eDelfoi
4
, Global
Futures Intelligence System (GFIS)
5
, and Surveylet
6
.
The aim of these tools is largely to manage and
conduct experiments using the Delphi process (e.g. by
providing tools to create electronic questionnaires).
For a detailed summary of other computerized tools
which support group decision making see
(Fjermestad & Hiltz, 1998). (On the other hand, we
believe, IS-DELPHI is unique in creating visual
displays of differences which in turn suggest changes
that can lead to expert agreement.)
So far, the approaches and tools discussed largely
support experts developing a consensus on whether
they agree on propositions (e.g. “The use of
1
Namely, the principles of how to achieve optimum
outcomes when reasoning or making decisions under
uncertainty.
2
http://competinghypotheses.org/
3
www.rahs-bundeswehr.de
antibiotics is set to increase over the next 5 years”).
In a Delphi approach, this is achieved through
repeated rounds until a pre-determined level of
agreement has been reached. However, such group
exercises often appear disjoint from the context of
knowledge application, and further may not allow
sufficient investigation of various opinions.
Supporting electronic tools provide limited
functionality for experts to justify their opinion (i.e.
to offer insights into how or why they formed their
opinion) or to directly discuss points of disagreement
with other expert participants. Tools which support
other types of knowledge elicitation, such as
procedural knowledge or classification, are
effectively lacking. For example, Open Source ACH
provides collaborative features which help experts
identify the basis of a disagreement, but it is limited
to hypothesis generation and identification of
supporting evidence (e.g. in intelligence gathering).
In this paper we describe a tool, IS-DELPHI,
which is loosely based on the Delphi approach, but
has been designed to support the development of an
expert consensus on the performance of classification
tasks rather than propositional statements. Further, to
enhance the likelihood of achieving consensus during
such problem-solving tasks, the facility for experts to
discuss how they have classified an entity is included
as an integral part of this tool.
The rest of the paper is organized as follows:
section 2 summarizes the IS-DELPHI system which
supports experts as they discuss differences with
fellow experts; section 3 gives an overview of IS-
DELPHI’s functionality; section 4 reports a case
study; section 5 discusses the results of that study; and
section 6 discusses future work.
2 RESOLVING DIFFERENCES OF
OPINION BETWEEN FELLOW
EXPERTS: THE IS-DELPHI
PROJECT
The focus of our group’s approach has been to see if
experts, given suitable tools, are themselves able to
detect, and in some cases, resolve inconsistencies. In
an earlier (medical) study, we asked clinicians to
annotate a series of time-points indicating which class
4
www.edelfoi.fi
5
www.themp.org
6
https://calibrum.com/
Resolving Differences of Opinion between Medical Experts: A Case Study with the IS-DELPHI System
67

each instance, in their view, belonged to. (These
classes were intended to capture the ICU patient’s
overall physiological state.) In that study we mentioned
the set of 5 classifications we thought should be used
and asked each expert to annotate the set of instances
independently. Once these annotations were available,
we used a system we had implemented called
INSIGHT (Sleeman et al, 2012) to compare a
particular expert’s annotations with those of a rule-set
produced by a senior clinician from that group. This
tool allowed the several experts to achieve agreement
between their annotations and a ruleset in several ways;
namely they could modify an instance’s annotation, or
they could revise the ruleset. At the heart of this system
was a Confusion Matrix which showed the expert
when the annotations produced by the single expert and
their (evolving) ruleset agreed. Where there was
agreement, that instance would appear in one of the
diagonal cells; if there was disagreement then it would
appear in an off-diagonal cell. Quite good agreements
were obtained based on 3 experts, (Sleeman et al,
2012). To progress further we held a Delphi-style
session with 3 medical experts and analysts who acted
as enablers. The result of this session was a ruleset,
approved by the 3-experts, which did provide better
agreement than the individual rulesets, but we noted
that inconsistencies (still) existed between the
“common” ruleset and the annotations produced by the
individual experts who had taken part in producing the
common ruleset
7
, (Sleeman et al, 2012). These
experiences led us to consider holding sessions
between pairs of clinicians where they had annotated
a number of instances differently, to see if it might be
possible for these differences to be resolved – or
perhaps for individuals to clearly explain why they
were not prepared to change their annotations. That is,
we decided it would be useful to carry out a series of
Delphi-style interactions between pairs of experts.
Subsequently, we have developed the IS-DELPHI
web-based system which attempts to carry out
programmatically, the negotiation stage discussed
above when it is presented with 2 sets of annotations of
a common set of instances produced earlier by pairs of
experts. The investigators need to review the sets of
annotations and decide which pairs of experts might
find it useful to have Delphi-style dialogues
/discussions. (Clearly, if a pair of experts produced
identical annotations it would not be helpful for them
to “meet”.)
3 OVERVIEW OF THE
IS-DELPH SYSTEM
The system provides facilities for the administrator(s)
to set up studies between pairs of experts, and secondly
provides facilities for pairs of experts to view their
differences and attempt to resolve them. These
functionalities are described in sections 3.1 and 3.2
respectively.
3.1 Facilities Provided for the
Administration / Setting-up of
Studies
There are 3 main functionalities provided here,
Figure 1: This shows a typical Confusion Matrix displayed by IS_DELPHI which reflects the annotations made by 2 users.
7
Subsequently we used Bayesian models to represent the
annotation processes of each expert, and we discovered, in
this formulism, there were distinct differences between the
several expert models, and further that, occasionally, each
expert failed to accurately apply their distinct model,
(Rogers et al, 2013). (The later corresponding to what
psychologists refer to as “slips”.)
HEALTHINF 2020 - 13th International Conference on Health Informatics
68
namely: displaying a list of active users, and the
registration of new users; creating new projects and
uploading the corresponding annotated datasets; and
creating new studies between existing (registered)
users and their already uploaded annotated datasets.
Additional functionalities allow the administrator to
archive the annotated CSV files produced by the
experts, to download log files, and to terminate
sessions etc. For more details see, (Sleeman &
Kostadinov, 2019).
3.2 Facilities Provided to Enable
Experts to Explore and Resolve
Their Differences
There are 3 main groups of facilities available here,
namely:
Accessing IS-DELPHI
8
, logging in to an existing
account using your password.
Studies: Pressing this TAB, lists all the studies
which the user is currently involved in, shows the
name of your partner(s), and provides a ‘view’
button which allows you to see the state of the
Confusion Matrix of each active study. Figure 1
shows a screenshot of a typical Confusion Matrix.
Ability to revise your annotations and to leave
associated comments. This is a significant topic and
is described in some detail in the rest of this section.
The Confusion Matrix in Figure 1 is quite sparse as the
2 experts have only used “D” and “E” annotations. The
cells on the diagonal indicate agreement between the 2
sets of annotations, whereas off-diagonal cells show
disagreements. (Note, the active user’s annotations are
indexed through the rows of the table, while the other
expert’s annotations are indexed though the columns.)
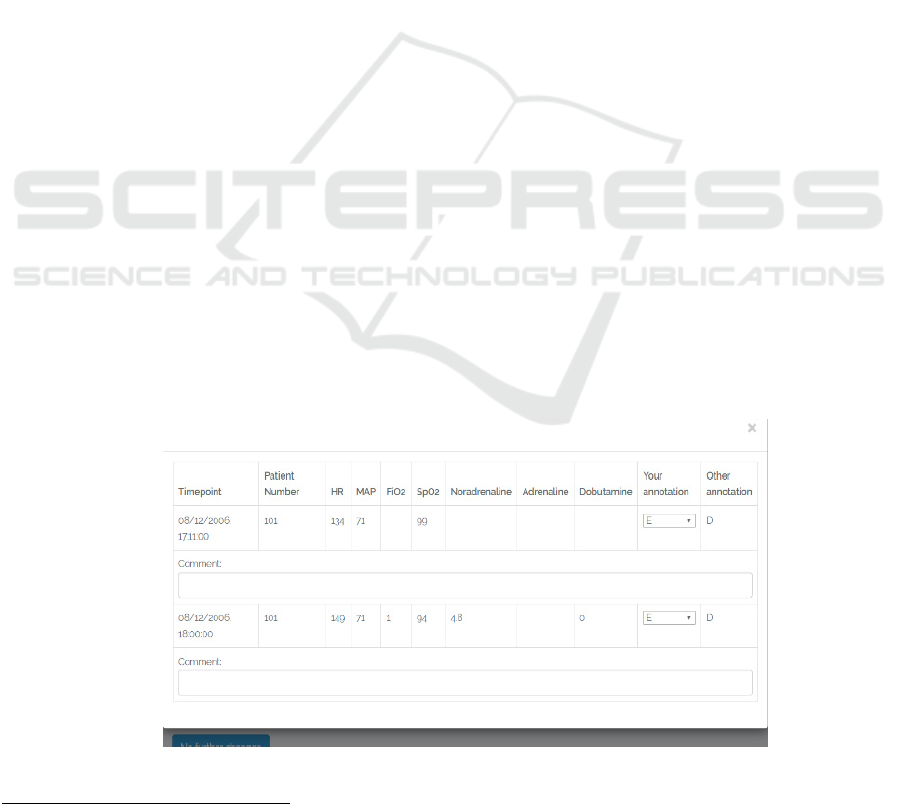
If a user clicks on any cell, the system opens another
window at the top of the screen which displays all the
time-points in that cell. Figure 2 shows the cell where
User 1 (the active user) has annotated both instances as
Es – and the other expert has annotated them as Ds.
User 1 (the active user) is then able to change his
annotation if he wishes (using the drop-down menu
shown in Figure 2). In fact the user is able to make as
many changes as he wishes to this cell. In general, as
there are several cells where the experts disagree, the
active user can change the annotations associated with
each of these. In the initial implementation, we only
allowed a user to add a comment to a cell after an
annotation had been changed. Once the user has
reported all the annotations and comments they wish to
make, then they can press the ’submit changes’ button
which then transfers control of the study to their
partner. (As only one partner at a time has the ability to
modify annotations), The system then sends the partner
an email telling them that they can now access the
system and make changes to the annotations if they
wish. In fact before the system gives control to the
other partner it asks the currently active user one
further question – namely “Have you made all the
changes to your annotations, which you think, are
necessary?” As mentioned above, the ability to make
changes to annotations and add comments then passes
to the partner, who can then make such changes if they
wish or they too can indicate, by pressing the “NO
FURTHER CHANGES” button, that they are satisfied
that no further changes are necessary. Note the system
only closes a study if both users press the “NO
FURTHER CHANGES” button in 2 consecutive
interactive
sessions. Again, for more details see
(Sleeman & Kostadinov, 2019).
Figure 2: This shows details of an off-diagonal cell – where the 2 experts disagree on the annotation.
8
http://intelsys-abdn.org.uk
Resolving Differences of Opinion between Medical Experts: A Case Study with the IS-DELPHI System
69

4 CASE STUDY
As noted earlier, we have developed a scoring system
which captures the overall state of a patient in the
Intensive Care Unit (ICU PSS), and can be used, unlike
APACHE, at any point in a patient’s ICU stay,
(Sleeman et al, 2012). The score uses commonly
available physiological and pharmacological data and
aims to take into account the amount of support the
patient is receiving. That is, a patient with a “normal
blood pressure” but receiving large quantities of
inotropes, would not be classified the same as a patient
with a “normal blood pressure” but no
pharmacological support. By means of a sophisticated
rule base the scoring system summarises the overall
state of the patient from A to E. Where the “A” level
represents a relatively well patient on minimal, or no
physiological and / or pharmacological support, who
may be ready for transfer to a ward or a high
dependency unit. On the other hand, “E” represents a
patient who is extremely sick requiring considerable
physiological and / or pharmacological support. “C”
represents a patient who is somewhere in the middle
i.e. moderately unwell and receiving some
physiological and / or pharmacological support.
The case study was run as 2 parts: firstly, the pilot
study was run with 4 participants
9
. Results from the
questionnaires and observations from the analysts (DS
and KK) were used to enhance the system and some
aspects of the documentation, and then a “full” study
was run with 12 ICU clinicians at the Consultant or
Senior Registrar levels. The overall structure of both
studies was the same, namely:
Each participant was asked to annotate
independently an identical set of 60 time-points for
ICU patients (these had the same form as the
clinicians see regularly in the ICU) as one of 5
categories. The participants added their annotations
to a spreadsheet. (So, this information was captured
on-line.)
The analysts then reviewed these responses, and
selected pairs of experts who replied differently to
a number of time-points. (In the pilot this selection
was done “manually”; for the “Full” study we used
software to help make these selections.)
Use of the IS-DELPHI system: the system
administrator then registered the various experts
and loaded their annotated files to the system.
Further, they set up a series of “studies” each of
9
2 ICU specialists and 1 trainee anaesthetist took part in
this study, and to complete a pair one of the analysts (DS)
also participated. DS used the definitions defined by experts
which involved a pair of experts identified in the
previous step.
Although, IS-DELPHI has been designed as a web-
based system, in the pilot study, the participants were
asked to come to a central laboratory in the Queen
Elizabeth University Hospital complex (Glasgow) so
that the investigators could better monitor the
interactions between the participants.
4.1 Results of the Pilot Study
The comments below are based on feedback contained
in the questionnaires returned and more specifically by
a detailed report provided by the medical author of this
paper (MS) who was also a participant in the pilot
study:
Various enhancements to the user interface were
suggested, so the expert can clearly indicate when
they had completed revising the annotations
associated with a particular cell.
Comment facility: As noted above (section 3.2) the
initial implementation of the system only allowed a
user to add a comment once an annotation had been
changed. This expert argued that it should be
possible to add comments about a time-point before
a change is made. Indeed, he argued that this
facility should be much more flexible – including
allowing an expert to view, in a separate window, a
complete interaction (annotations and comments)
between the 2 experts – where each interaction is
time-stamped.
A significant discovery was that some browsers
were not communicating effectively with IS-
DELPHI which resulted in some annotation
changes and comments not being recorded by the
system.
We determined which browsers were causing
problems, and then blacklisted these in the User
manual. Secondly, the various system changes
suggested were considered by the analysts and the
majority were implemented before the full study was
undertaken.
4.2 The Full Study
As noted in section 4, 12 ICU specialists were involved
in the full study which took essentially the same form
as that noted above for the pilot project (namely,
annotation of a common set of instances, selection of
in the earlier ICU PSS study with INSIGHT, (Sleeman et
al, 2012) as his “crib”.
HEALTHINF 2020 - 13th International Conference on Health Informatics
70

pairs of experts to resolve their differences, and use
of IS-DELPHI by these pairs.)
4.2.1 Selecting Pairs of Experts Who Might
Usefully Use the IS-DELPHI System to
(Attempt to) Resolve Their Differences
As noted above, this study was run with 12 experts
who were asked to annotate an identical set of 60
instances. To select appropriate pairs, the Python-
based COMPARE program firstly creates a table
which shows the number of agreements /
disagreements between each of the pairs i.e. (P1 P2),
(P1 P3) … (P1 P12), (P2 P3), (P2 P4)… (P2 P12) ..
(P11 P12). (Matching Criterion-1: 2 Annotations are
considered different if they are 1 or more ICU PSS
categories apart.) Note too that P3 did not return any
annotations which in turn means that only 5 groups
can be formed. This information is shown in Table 1
where we report the number of instances on which the
pairs of annotations are different with respect to the
current matching criterion. For example (P1, P2)
reports 34 disagreements which means there are 26
(60 – 34) agreements. The average number of
differences shown in this table is 31.69 with a SD of
9.35; with those figures becoming 27.80 and 4.60
respectively when P11, who seems to be an “outlier”,
is removed from the calculation.
The next step was to select pairs of experts who
would work together to resolve their differences.
Here, the algorithm chose 5 pairs which gave overall
the smallest number of instances to be considered,
provided that each pair contained at least the
minimum number of instances specified (2 in this
study) where this value is passed to the COMPARE
algorithm as the threshold parameter. And of course
each instance selected, complies with the current
Semantic Matching criterion. (Clearly, we are not
interested in selecting pairs, which have no
differences, as in such cases the experts would have
nothing to discuss in IS-DELPHI.) Given that there
are a relatively small number of participants in this
study, it would have been possible to select these
pairs “manually”. However, as the process is
somewhat time-consuming and error-prone, we
decided to add further functionality to the
COMPARE program to make these selections. This
selection process is based on a maximum weighted
matching algorithm, (Galil, 1986) which attempts to
minimize the number of items in all the chosen pairs,
with the added constraint, noted above, that each pair
must contain at least 2 instances. The pairs chosen
by COMPARE for this study are highlighted in
Table-1.
The number of instances selected, by
COMPARE, were considered too large for the expert-
pairs to process (using IS-DELPHI), and so we
decided to investigate the number of instances where
the semantic differences are 2 or more ICU PSS
categories apart. (Matching criterion-2). In this
scenario, (A C) (A D) (A E) (B D) (B E) (C E) and
the reversed forms would be reported but (A B) (B A)
(B C) (C B) etc would not be. When this criterion
was applied the number of disagreements between the
pairs of experts, reported by the COMPARE system,
reduced quite considerably as shown in Table 2. The
average number of differences shown in this table is
7.00 with a SD of 9.59; with those figures becoming
2.76 and 2.99 respectively when P11, who seems to
be an “outlier”, is removed from the calculation.
Again the COMPARE system selected pairs of
experts who have 2 or more time-points. For
example,
in Table-2 the pair of experts (P1, P2) are
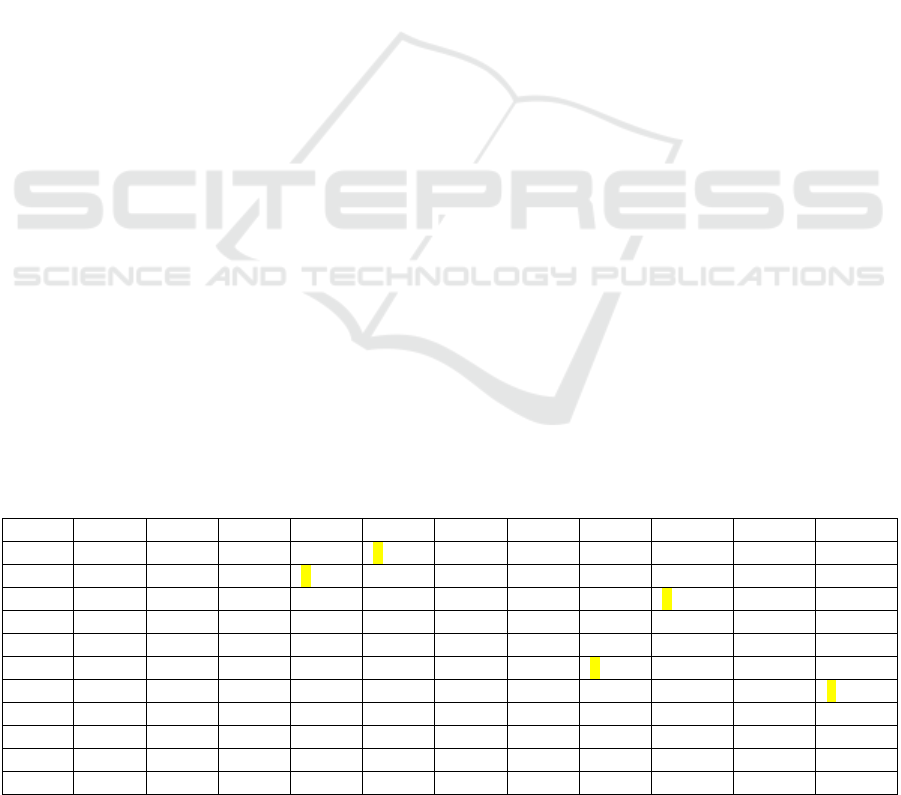
Table 1: Number of Disagreements (Using current criteria). The selected pairs are highlighted in YELLOW; note P11 is not
assigned to a pair because there are an odd number of participants – also this person does seem to be an outlier. Pn indicates
the nth Participant in this study.
P1 P2 P4 P5 P6 P7 P8 P9 P10 P11 P12
P1 - 34 24 28 23 22 31 29 32 49 23
P2 - 25 20 31 37 27 32 27 52 36
P4 - 21 26 30 25 28 25 50 22
P5 - 33 34 26 23 34 49 34
P6 - 2628342747 19
P7 - 26273050 28
P8 - 19 32 49 26
P9 -3152 30
P10 - 50 26
P11 - 44
P12 -
Resolving Differences of Opinion between Medical Experts: A Case Study with the IS-DELPHI System
71
shown as having 3 instances which have a “semantic
difference” of at least 2 classes between their
annotations. (It is not uncommon, in this domain, for
annotations produced by 2 experts to differ by one
category.) The pairs highlighted in Table-2 were
selected by the algorithm, namely: (P1 P6) (P2 P5),
(P4 P10), (P7 P9) & (P8 P12); it is only possible to
form 5 groups; P11 was excluded by the criteria we
have used for pair selection. Moreover, looking at the
“raw” data it would appear that P11 is, anyway,
somewhat of an outlier when compared to the rest of
this group. (In future studies, once the general
approach has been shown to be workable, we might
decide to include “outliers” like P11 to see if this
approach would work with pairs of experts which
have a substantial number of differences. Also see
section 6.)
The COMPARE system has 3 parameters,
namely: whether unlabelled classes are to be handled,
the minimum “semantic” distance between 2
annotations for them to be considered not to match,
and the minimum number of instances to be
considered by each pair of experts. Note, the
algorithm reports the number of mismatches, not
matches, found.
4.2.2 Use of the IS-DELPHI System
The instructions to the participants in this study
recommended that they consider time-points where
the annotations provided by the experts, are 2 ICU
PSS classes different, as differences of just one class
apart are not uncommon. (The experts could, of
course, choose to consider any of the time-points
contained in the confusion matrix.)
The various changes made and comments
recorded by each of the experts participating in a
particular study are recorded by the system in a log
file which is unique to each study. Each interaction is
time-stamped, and the system also effectively records
when the “active” user changes and when a study is
closed. These log files are discussed in some detail in
section 4.3.
4.3 Results of the Full Study
The critical issue to be decided was whether IS-
DELPHI was able to help these experts resolve their
differences. Table 3 indicates strongly that this is
indeed the case, and reports that from the 5 pairs there
were 11 time-points where the 2 experts disagreed
initially by 2 ICU PSS classes in their annotations,
and after using the system 7 of these were fully
resolved. Moreover, in the remaining 4 instances the
differences were reduced to just 1 ICU PSS class
which we had suggested in the documentation given
to the study participants, in this domain, could be
considered to be effectively equivalent. Further, there
were no instances in which neither expert made a
change.
We have also carried out a more fine-grained
analysis which investigates how these changes were
achieved – i.e. was an agreement achieved by just a
single expert making a 2-step change or did both
experts make 1-step changes? Of the 7 time-points
where full agreement was achieved we note that 3
were achieved by a single expert making a “big”
change, and the other 4 were achieved by both experts
each making a smaller change. And of course, in the
case of the 4 time-points where the final difference
was 1 ICU PSS class, just one of the experts made a
smaller change of 1 semantic class.
Table 2: The selected pairs are highlighted in YELLOW; note P11 is not assigned to a pair (because there are an odd number
of participants – also this person does seem to be an outlier). (NB Matching criterion-2 has been used here, and each selected
pair must have at least 2 instances.) Pn indicates the nth Participant in this study.
P1 P2 P4 P5 P6 P7 P8 P9 P10 P11 P12
P1 - 3 0 1 20126 26 1
P2 - 0 2 3 8 4 10 11 30 1
P4 - 0 10113 27 0
P5 - 33119 22 1
P6 - 1144 23 0
P7 -224 31 0
P8 - 0 10 24 2
P9 -8 23 3
P10 - 31 4
P11 - 24
P12 -
HEALTHINF 2020 - 13th International Conference on Health Informatics
72
4.3.1 Analysis of Time-points Which Only
Differ by One Semantic (ICU PSS)
Class
Below we give a summary of the number of such
instances which were presented to each pair and the
number which each pair processed:
F1: There were 21 instances of this type, of which
8 annotations were amended by just 1 expert.
F2: There were 18 instances of this type, none of
which were amended by either expert.
F3: There were 22 instances of this type, of which
10 annotations were amended by the first expert
and 11 by the other expert. The annotation of the
remaining instance was not changed but one expert
left several comments about it.
F4: There were 25 instances of this type, of which
11 annotations were amended by one expert and
none by the other expert.
F5: There were 24 instances of this type, of which
4 annotations were amended by just one expert who
also left a comment explaining why he was not
changing a further annotation. The second expert
made no changes or comments.
4.3.2 Analysis of the Actual Interactions
Which Occurred between Experts
When using IS-DELPHI
As noted above (section 3.2) the first implementation
of IS-DELPHI used in the Pilot Study, only allowed
experts to make a comment after they had changed an
annotation. The feedback from the Pilot Study was that
this is far too restrictive, so we amended the system to
allow either comments, or a change of annotation, or
both to be made at each stage of the interaction. This
seems to have been a very valuable enhancement to the
system, as the types of interactions we have seen in the
full study are certainly much more flexible than the
first system supported, and can be summarized as the
expert user:
Only modifies the actual annotation(s) - no
comments provided
Makes change to an annotation and adds a
comment in the same interaction (in either order).
Comments precede changes (these are given in
different interactions)
Changes precede comments (these are also given in
different interactions)
There are many examples of these different
“styles” of interactions in the log files collected from
the 5 pairs of experts during this study. Figure 3 gives
an excerpt of the interactions between experts P02 and
P05 which includes several of these types of
interactions – particularly the one which has changes
of annotation and comments occurring in the same
interaction. In this study, the 2 experts in fact resolved
differences in their initial annotations for both TP-45
and TP-59. However to make the interaction easier to
follow we have only included interactions which
discuss TP-45; also we edited the dialogue a little to
remove several typos etc. It is also important to know
that P02’s initial annotation of this time-point was an
“E” and P05’s was a “C”. What’s interesting about the
interaction is that both experts summarize the “case” as
they see it, allude to the reasons why they gave the
initial annotations they did, and then discuss issues
raised by their partner which is making them
reconsider their initial annotations. With this instance
(TP-45), the final interactions of both experts was to
propose a compromise classification of “D”, hence
achieving full agreement on this time-point.
4.3.3 Feedback from the Participants in the
Full Study
Stage 1: The questionnaire posed the following
questions:
1. I understood the overall approach of the IS-
DELPHI project. (Rating scale where 1 is very
unclear, and 10 is absolutely clear):
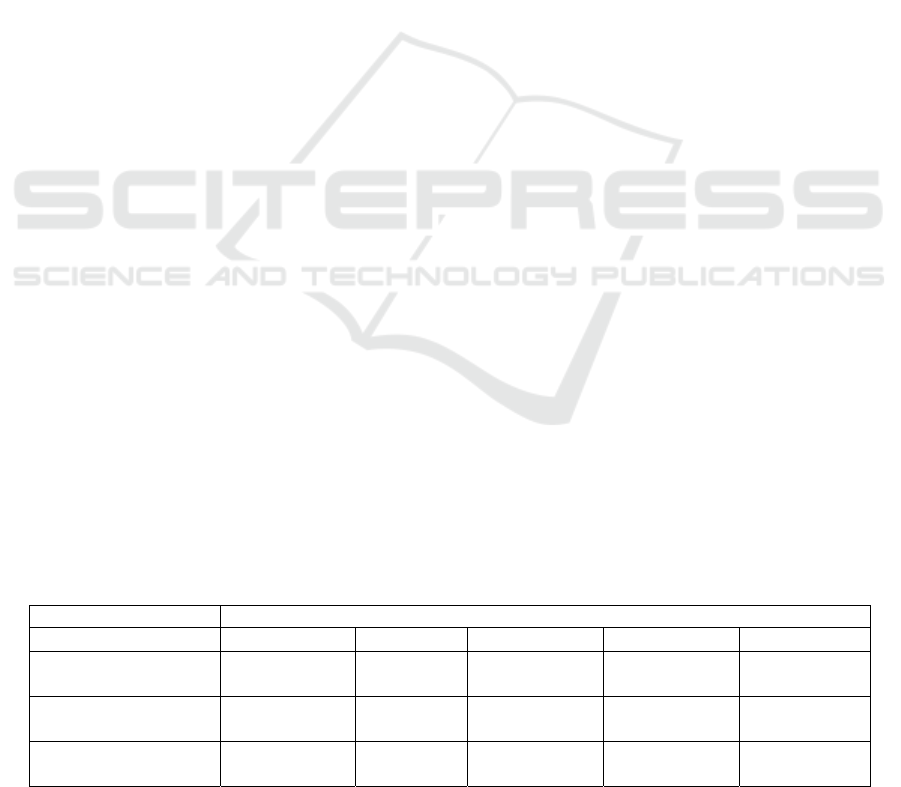
Table 3: Across the 5 pairs there were 11 instances where the initial annotations of the 2 experts differed by ICU PSS 2 classes.
The results show the agreement after each pair has used the IS_DELPHI system.
Pairs
F1 F2 F3 F4 F5
First Time-Point Full
a
g
reemen
t
Full
a
g
reemen
t
Full
a
g
reemen
t
1 class
differen
t
1 class
differen
t
Second Time-Point 1 class
differen
t
Full
a
g
reemen
t
Full
a
g
reemen
t
Full
a
g
reemen
t
1 class
differen
t
Third Time-Point - - Full
a
g
reemen
t
--
Resolving Differences of Opinion between Medical Experts: A Case Study with the IS-DELPHI System
73

2. I understood what I was required to do in Phase 1
of the IS-DELPHI project. (Rating scale where 1 is
very unclear, and 10 is absolutely clear):
Where the results are: Q1, Mean 9.00, standard
deviation (SD) 1.26; Q2, Mean 9.18, SD 1.33. NB
There were 11 participants; one expert completed
neither the annotations nor the questionnaire.
The participants were also asked to make
suggestions about the study. The following comments
were received:
2 comments about details of units for the
vasopressors
A question about FiO2 and whether it applied to
ventilated / unventilated patients.
“Very interesting and thought provoking study.”
Stage 2: This questionnaire posed the following
questions:
1. I understood the overall approach of the IS-
DELPHI project. (Rating scale where 1 is very
unclear, and 10 is absolutely clear):
2. I understood what I was required to do in Phase 2
of the IS-DELPHI project. (Rating scale where 1
is very unclear, and 10 is absolutely clear):
3. The section of the user manual for domain experts
was clear. (Rating scale where 1 is very unclear,
and 10 is absolutely clear):
Where the results were: Q1, Mean 8.40, SD 0.84;
Q2, Mean 8.00, SD 0.94; Q3, Mean: 7.10, SD 1.10.
NB Only 10 people (5 pairs) took part in this phase.
The participants were also asked to make
suggestions about the study. Only 2 comments were
received:
“..I think the screen shots need to be clearer.
There is a lot of explanation which is good but is
a lot to take in and is quicker/easier to understand
by practicing live. Perhaps earlier reference to
opening up a version to look at and play with
could help.”
“It was clear enough. Didn’t need to refer too
carefully to the manual, though my partner did.”
Figure 3: This gives an excerpt of an interaction, captured by IS_DELPHI, between experts P02 and P05. This dialogue has
been slightly revised with typos etc removed. In the complete session they also discussed a further time-point on which they
initially disagreed, but for ease of presentation those comments have been removed – just leaving a discussion of a single
time-point (TP-45).
[2019-05-30 15:03:51] Expert P02 left a comment on timepoint TP-45 [PN-7465: 2017-
10-07 15:00:00]
1
: "Low oxygen saturations on maximum FiO2, quite fast heart rate with
low/normal BP"
[2019-05-30 15:20:02] Expert P05 left comment on timepoint TP-45: "Agreed, but not
obviously needing CVS support. The picture I have is of a struggling respiratory
failure patient requiring intubation. MAP of 58 might hint at impending CVS
compromise but in absence of other data (e.g. CRT) hard to assume"
[2019-05-30 15:28:11] Expert P02 left comment on timepoint TP-45: "I agree that is
probably the most likely picture though this could be the situation in an intubated
patient. Given the absence of inotrope/vasopressor requirement happy to change to
D."
[2019-05-30 15:30:52] Expert P05 left comment on timepoint TP-45: "Agree. D seems
fair given both our ‘angles’."
[2019-05-30 15:31:38] Expert P02 changed evaluation on timepoint TP-45 from E to D.
No comment was provided.
[2019-05-30 15:35:12] Expert P05 Changed evaluation on timepoint TP-45 from C to D.
Comment: "Okay, agreed to go to D."
. . . . . . . . . . . . . . . . . . . . . . .
[2019-05-30 20:59:07] Expert P02 indicated that they have no further changes.
[2019-05-31 14:20:17] Expert P05 indicated that they have no further changes.
The study ends.
HEALTHINF 2020 - 13th International Conference on Health Informatics
74

5 DISCUSSION
In this paper we have described and illustrated the use
of the IS-DELPHI tool, which has been designed to
support the development of consensus between pairs
of experts when solving common classification tasks.
We believe that the provision of a facility which
allows experts to discuss their several approaches to
common tasks, has greatly contributed to the tool’s
effectiveness.
IS-DELPHI has been evaluated in a study with
medical domain experts. The results of the full study
show that the 5 pairs of clinicians were able to make
considerable progress in agreeing on (common)
annotations. In 7 out of the 11 instances, they
achieved full agreement on the final annotations, and
in 4 further instances reduced the differences between
their annotations from 2 ICU PSS classes different to
just 1 (which, we’d noted, in this domain, is
commonly accepted as a match.) Our analysis of the
interactions / dialogues between the several experts
suggests that IS-DELPHI has elicited useful
dialogues between the pairs of experts which has
facilitated them reaching agreements on their revised
annotations, (see Figure 3).
Further, we note that 4 out of the 5 pairs of experts
also “processed” time-points which were only 1 ICU
PSS class apart, something which was not specified
in the study instructions. For instance, pair F3 instead
of revising just the annotations associated with the 3
time-points whose ICU PSS classes were 2 semantic
classes apart, actually made changes to 24 time-points
(21 of which were just 1 semantic class apart). This
suggests that many of the participants, understood the
tasks well, and secondly, were quite comfortable with
the functionality provided by IS-DELPHI.
Additionally, questionnaires from both phases
suggest that the majority of the participants
understood the task to be performed, and were happy
with the instructions for both phases of the study and
with the user manual provided. We have noticed that
the lowest mean score and the greatest spread was for
question 3 about the effectiveness of the manual.
From studying the logs the analysts determined that
some users were unclear how to terminate sessions.
In summary, we suggest that the IS-DELPHI
system has a useful role to play in the important
Knowledge Acquisition process; we have shown in
this study that it enables clinical experts to discuss
and often resolve their differences, so ensuring that
the resulting medical knowledge is more consistent.
6 FURTHER WORK
Following this successful case study, we are now
planning a number of additional activities including:
a) Other studies: a larger study based on ICU
datasets, further medical domains and in other
disciplines such as Management.
b) Adding a feature to process the experts
comments / justifications with Natural Language
and Argumentation Techniques.
c) Store more complex multi-stage comments /
justifications.
d) Extend the criteria which the system uses to
select pairs of experts, to include pairs with a
larger number of differences.
e) IS_DELPHI has focused on tasks where the
experts classify the various instances. We plan to
investigate whether the system could be extended
to also address further problem-solving
approaches, e.g., planning.
f) Systems developments (archive log files, the
export and import of the expert-refined CSV
files, and address the several system
enhancements mentioned in section 5.)
g) Create a video showing how to use the system,
which will either supplement or replace the
current user manual.
ACKNOWLEDGMENTS
We are grateful to the following colleagues from the
QEUH (Glasgow) for taking part as experts in this
study (2 in the pilot and the remainder in the full
study): Dr. Russell Allan, Dr. Richard Appleton, Dr
Aporva Ballal, Dr. Matthew Baynham, Dr. Euan
Black, Dr. Andrew Cadamy, Dr. Alan Davidson, Dr
Robert Hart, Dr. Louise Hartley, Dr. Andy Mackay,
Dr. Johnny Millar, Dr. Peter Stenhouse, and Dr.
Laura Strachan.
IS-DELPHI was implemented by Kiril
Kostadinov with financial support from the
University of Aberdeen Development Trust. Helpful
discussions with Professor Wamberto Vasconcelos
(Computing Science Dept., The University,
Aberdeen) and Dr. Martin Shaw (Clinical Physics
Department, Glasgow Royal Infirmary).
REFERENCES
Aengenheyster, S., Kerstin Cuhls, Lars Gerhold, Maria
Heiskanen-Schüttler, Jana Huck, Monika Muszynska,
Resolving Differences of Opinion between Medical Experts: A Case Study with the IS-DELPHI System
75

Real-Time Delphi in practice — A comparative
analysis of existing software-based tools,
Technological Forecasting and Social Change,
Volume 118, 2017, Pages 15-27.
Chi, M.T.H. Two Approaches to the Study of Experts’
Characteristics. In: The Cambridge Handbook of
Expertise and Expert Performance. Ericsson, K.A.,
Charness, N., Feltovich, P.J., Hoffman, R. (Eds)
Cambridge University Press. 2006.
Dunnette, M.D., Campbell, J.D., and Jaastad, K. The effect
of group participation on brainstorming effectiveness
for two industrial samples. Journal of Applied
Psychology, XLVII pg 30-37. 1963.
Fischhoff, B. “Eliciting Knowledge for Analytical
Representation,” IEEE Trans. Systems, Man, and
Cybernetics, vol. 19, no. 3, 1989, pp. 448–461.
Fjermestad, J., Hiltz, S.R. An assessment of group support
systems experimental research: methodology and
results. Journal of Management Information Systems.
Vol 15. Issue 3 (December 1998).
Galil, Z., Efficient algorithms for finding maximum
matching in graphs, ACM Computing Surveys, 1986.
Klein, G., R. Calderwood, and A. Clinton-Cirocco. Rapid
Decision Making on the Fire Ground, Proc. Human
Factors and Ergonomics Soc. Ann. Meeting, vol. 30,
no. 6, 1986, pp. 576–580.
Klein, G., Shneiderman, B., Hoffman, R.R. and Ford, K.M.
(2017, November/December). Why expertise matters:
A response to the challenges. IEEE: Intelligent Systems,
pp. 67-73.
Murry, J., J. Hammons, "Delphi a versatile methodology
for conducting qualitative research", Rev. Higher
Educ., vol. 18, no. 4, pp. 423-436, 1995.
Rogers, S., Derek Sleeman, & John Kinsella. Investigating
the disagreement between clinicians’ ratings of patients
in ICUs. IEEE Journal of Biomedical and Health
Informatics 17.4 (2013): 843-852.
Saaty, T.L. Decision making with the analytic hierarchy
process. International Journal of Services Sciences,
Vol 1, No 1. 2008.
Shadbolt, N. R., & Smart, P. R. (2015) Knowledge
Elicitation. In J. R. Wilson & S. Sharples (Eds.),
Evaluation of Human Work (4th ed.). CRC Press, Boca
Raton, Florida, USA.
Shields, MD., Solomon, I., and Waller, W.S. “Effects of
Alternative Sample Space Representations on the
Accuracy of Auditors’ Uncertainty Judgments,”
Accounting, Organizations, and Society, vol. 12, no. 4,
1987, pp. 375–385.
Sleeman, D., & Kiril Kostadinov (2019). IS-DELPHI User
Guide, Technical report, Department of Computing
Science, The University of Aberdeen.
Sleeman, D., Moss, L., Aitken, A., Hughes, M., Sim, M.,
Kinsella, J. Detecting and Resolving Inconsistencies
between Domain Experts' Different Perspectives on
(Classification) Tasks. Artificial Intelligence in
Medicine, 2012 Jun;55(2):71-86.
Tversky, A., & D. Kahneman, D. Judgement under
Uncertainty: Heuristics and Biases. Science, vol. 185,
Sept. 1974, pp. 1124–1131.
HEALTHINF 2020 - 13th International Conference on Health Informatics
76
