
Health Information Systems for Clients with Mild Intellectual and
Developmental Disability: A Framework
Muneef Alshammari
1
, Owen Doody
3
and Ita Richardson
1,2,4
1
Lero-The Irish Software Research Centre, University of Limerick, Ireland
2
Department of Computer Science and Information Systems, University of Limerick, Limerick, Ireland
3
Department of Nursing and Midwifery, University of Limerick, Limerick, Ireland
4
Aging Research Centre, HRI-Health Research Institute, University of Limerick, Limerick, Ireland
Keywords: Intellectual and Developmental Disability, Client Engagement, Person-centred Care, Gamification in
Healthcare, Information-Motivation-Behavioral Skills Model (IMB), Person-Centred Health Information
Framework (PCHI).
Abstract: Persons with intellectual and developmental disability (IDD) remain among the most vulnerable members of
society and frequently face numerous barriers accessing healthcare services. Following our recent literature
review identifying needs for persons with IDD, we propose that frameworks can be useful to identify the key
components of person-centred health information. These will ultimately support the building of relevant
Health Information Systems. This paper presents the initial development and content of the Person-Centred
Health Information framework (PCHI) developed to support persons with mild IDD. PCHI is based on the
Information-Motivation-Behavioral skills (IMB) model and its use in the design and development of Health
Information Systems has the potential to improve health access and outcomes for persons with mild IDD.
1 INTRODUCTION
Due to the recent unprecedented advances in software
and technology, Health Information Systems (HIS)
worldwide are undergoing innovative
transformations. HIS refers to the interaction between
people, process and technology to support operations
and management in delivering essential information
to improve the quality of healthcare service
(Almunawar and Anshari, 2012). HIS should not be a
separate and independent component of the health
system and should be designed according to the
service delivery system with patients/clients in mind.
HIS have the potential to deliver collaborative
person-centred care delivery across the continuum of
care.
The concept of person-centred care has been
increasingly advocated in healthcare. Additionally,
person-centred care is important for healthcare
services, eliciting insights from patients/clients which
foster improved working partnerships, thus providing
healthcare services that better meet consumer needs
(Delaney, 2018). However, person-centred care can
give a subjective lived-experience perspective of
IDD.
Persons with intellectual and developmental
disability (IDD) represent one of the major disability
groups in the developed world. IDD is defined and
characterized by significant limitations both in
intellectual functioning (reasoning, learning,
problem-solving) and in adaptive behaviours which
relate to everyday social and practical skills.
Internationally, IDD currently affects around 1% of
the population in high income countries and 2% in
low and middle income countries (Maulik et al,
2011). For persons with mild IDD, difficulties in
processing complex domain-specific statements,
understanding healthcare information content and
complying with treatment plans are common.
Supporting persons involves supporting the person to
fulfil basic needs, such as managing self-care and
self-advocacy. Thus, the opportunity for persons to
make choices are important to their quality of life.
When developing HIS to support person-centred
healthcare for use by persons with mild IDD,
researchers and developers must account for their
specific requirements.
New technologies are continuously being
adopted in healthcare services. Additionally,
developments in HIS have facilitated more effective
Alshammari, M., Doody, O. and Richardson, I.
Health Information Systems for Clients with Mild Intellectual and Developmental Disability: A Framework.
DOI: 10.5220/0008966801250132
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 125-132
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
125

approaches to healthcare activities and increased ease
of accessibility for vulnerable individuals (Bechtel
and Ness, 2010). Modern HIS improves service
quality in the healthcare service sector in general and
in clinical treatment in particular, enhancing client
safety (Rahimi, 2018). As a vulnerable grouping,
further research is required regarding the use of
technology to support persons with mild IDD,
examining topics such as access to and effectiveness
of healthcare services. This paper aims to address this
by outlining a framework for person-centred health
information for persons with mild IDD. The
proposed framework extends the existing
Information-Motivation-Behavioral (IMB) skills
model to include engagement and communication,
with a view to supporting and improving clients’ self-
care management and quality of life. Utilising this
framework will inform and support the development
and design of future HIS systems for persons with
mild IDD. Through drawing attention to HIS design
and accessibility, adherence to existing HIS standards
for users with IDD can be promoted. Additionally,
researchers can be encouraged to develop new
interaction strategies to address the issues related to
HIS design and usability for persons with IDD.
1.1 Research Question
As increasing attention is drawn to health disparities
across the general population, data also demonstrates
that clients with IDD experience even greater health
inequalities (Kirschner et al., 2007). Beyond the
realm of healthcare services, the general population
routinely utilizes technology to obtain information
and perform everyday tasks at a click of a button.
However, most health care systems have been
conspicuously slow to develop information system
tools of comparable functionality for persons with
mild IDD (Krist and Woolf, 2011). Therefore, this
paper considers the central research question:
Which conceptual framework for person-centred
health information can support the development
of HIS for clients with mild IDD?
The question is addressed by:
• Reviewing academic literature to identify
frameworks which have been used successfully in
various support provision areas;
• Developing and presenting a framework which
can be used to support HIS development for
persons with mild IDD.
2 LITERATURE REVIEW
Our recent literature review (Alshammari, et al.,
2018), identified six main barriers to the use and
access of health information which are experienced
by persons with mild IDD: (a) communication skill,
(b) client engagement and satisfaction, (c)
training/education for persons with IDD, (d) attitude
and knowledge of healthcare professionals, (e)
persons with IDD being excluded from health
promotion and research, and (f) quality of accessing
healthcare services. In this paper we are particularly
interested in working towards the elimination of
barriers to communication and engagement, and, in
providing more details regarding the experience of
persons with IDD when accessing health
information. Furthermore, we describe relevant
literature examining the accessibility of HIS for
persons with mild IDD.
2.1 Barriers to Communication
It is estimated that 50% to 90% of persons with IDD
experience a significant range of communicative
challenges (Baker et al., 2010). It therefore follows
that communication plays a key role in the
formulation and adoption of any person-centred
health information framework for persons with mild
IDD. In our previous paper, we identified that
persons with mild IDD struggle to understand
information from their healthcare professionals or
they themselves are not able to effectively
communicate their thoughts or needs regarding their
health condition (Alshammari et al., 2018). In
addition, other studies (Chou, 2012, Mustika et al.,
2014) identify that children with IDD can develop the
ability to communicate and learn using such
technology. Persons with mild IDD and their carers
expect healthcare professionals to communicate well,
both in terms of how they conduct information
provision and their service relationships.
Communication is an important dimension which can
have a positive effect not only on a person's self-
management of their healthcare, but also on
additional factors including socio-demographic
characteristics and a person’s health literacy (Santana
and Feeny, 2014). The increasing complexity of care
pathways arising from the growing numbers of
persons with mild IDD who experience chronic
illness further increases the communication demands
facing healthcare professionals. Unfortunately, such
complexities also raise the likelihood of problems and
errors, while resolving these problems rests more and
more on sophisticated forms of communication
HEALTHINF 2020 - 13th International Conference on Health Informatics
126

(Iedema and Manidis, 2013). Well-developed HIS
can provide solutions to communication barriers, thus
enhancing the patient-centredness aspect of
healthcare systems.
2.2 Barriers of Engagement
Due to communication barriers, it is difficult for
persons with mild IDD to engage with the health
system. For example, during clinical consultations,
the communication is often directly between the
health professional and the carer - consequently, the
person with mild IDD is left out of the conversation.
To address this enhanced engagement for persons
with mild IDD offers a promising pathway towards
both better quality and more efficient care. This, in
turn, should improve overall population health.
Persons with mild IDD need the encouragement and
support to be more confident and involved in their
personal healthcare decision-making process, as
those who are engaged as decision-makers in this way
have been shown to be healthier and achieve better
outcomes (Chinn, 2017). Thus, personal engagement
in healthcare management has the potential to
contribute to better health outcomes, and HIS have an
important role to play in supporting this engagement.
It is important that the barriers of engagement are
properly considered during HIS development and
solutions devised to address the key barriers for
persons with mild IDD.
2.3 IDD and HIS
Existing literature exploring HIS often focuses on
assistive technology and these studies touch on topics
related to the using mobile technology such as
increasing self-discovery and an increasing
confidence in technology use (Chmiliar and Anton,
2015, Burke, 2017).
However, there are few studies on HIS for persons
with IDD. The literature available on this topic
mainly relates to hospital passports which some
studies refer to as hand-held health records (HHHRs),
logbooks, health passports or health diaries.
Northway et al. (2017) presented a review of
hospital passport use in the UK for persons with IDD.
In their review, they found that some health passports
lack primary care information as well as a level of
communication which supports expression and
understanding. However, this does not necessarily
speak to the level of HIS technology because they
were not considering a technological intervention. In
addition, Nguyen et al. (2014) highlighted the use and
benefit of hospital passports for persons with IDD,
reporting that hospital passports could increase
health-related knowledge and awareness of personal
health issues for long-term healthcare activity.
Conversely while their review is not explicitly for
HIS technology content, they offer health passports
as a solution for the improvement of hospital records
and as a means to support persons with IDD in the
long-term. Thereby, this would enhance knowledge
and provide an awareness of personal health issues.
3 RESEARCH METHOD
Following a literature review (Alshammari et al.,
2018) to identify and discuss the barriers to access
health information , a review of existing models and
frameworks used and acknowledged to improve
health outcomes for persons with mild IDD was
undertaken.
This iterative process involved a series of
systematic steps (see Figure 1) and led to the
development of person-centred health information
framework. The process included a mapping of
existing conceptual frameworks and models against
person-centred health care requirements. Identifying
similarities and matching elements of each existing
framework was an important step and confirmed the
strong relationship between health information and
person-centred care. The Information-Motivation-
Behavioral (IMB) skills model was identified as a
starting point for building a conceptual framework for
person-centred health information for persons with
mild IDD. In actual fact, the IMB model emphasizes
that people who are well-informed and motivated are
likely to engage in activities that enhance knowledge
and skills needed to perform focused behaviour,
which allows them to obtain better health outcomes
(Athilingam et al., 2017). In doing this, we developed
the concepts of barriers to engagement and barriers to
communication, and conceptualized them within the
IMB skills model. The framework that we present
here, the Person-Centred Health Information (PCHI)
framework for persons with mild IDD, is its first
iteration.
Health Information Systems for Clients with Mild Intellectual and Developmental Disability: A Framework
127

Figure 1: Processes used to develop Person-Centred Health Information framework (PCHI).
3.1 Information-Motivation-Behavioural
Skills Model
The IMB framework demonstrates that, while
information is a prerequisite for changing behaviour,
information in and of itself is insufficient to achieve
this change (Osborn et al., 2010). As a general social
psychological conceptualization for understanding
and promoting health-related behaviour, it purports
that persons who are well-informed and motivated are
likely to engage in activities which enhance the
knowledge and skills needed to perform focused
behaviour, and, in turn, are enabled to enjoy better
health benefits (Fisher et al., 2003). The IMB model
has three constructs: (1) information, (2) motivation,
and (3) behavioural skills (Sabaté, 2003) and has been
empirically validated across a number of diverse
populations and health promotion behaviours.
While IMB is recognized as a credible model, a
literature review conducted by Alshammari et al.
(2018) identified a significant gap in knowledge for
developing HIS. Thereby, considering the barrier to
communication and engagement that must be
considered when developing HIS for persons with
mild IDD, we modified the IMB skills model to
address these barriers. Within HIS, the accuracy of
information is not sufficient as an output for persons
with mild IDD to support the management of their
personal healthcare. Communication and
engagement are equally important and must be
included in any framework supporting HIS
development. Our proposed Person-Centred Health
Information Framework (PCHI) offers an extended
version of the IMB model.
3.2 Person-Centred Health
Information Framework (PCHI)
Version 1
Figure 2 presents the PCHI framework for persons
with mild IDD and variables not previously included
in IMB are indicated by dotted lines. The inclusion
of both engagement (Athilingam et al., 2017) and
communication (de Jong et al., 2014) are essential as
they have a direct bearing on health outcome.
Moreover, the model proposes that communication
and engagement factors may indirectly influence
health outcome by means of behaviour change. In
addition, the communication element may indirectly
influence the health outcome via motivation.
Engagement may also exert an indirect influence on
health outcome through an understanding of health
information and a stronger involvement with the
healthcare professionals. This first iteration of PCHI
has six components as described in the following
sections.
3.2.1
Health Information
The simplest function of personal health records is to
store information which may be entered by the person
and can include hyperlinks to useful resources. Some
personal health records personalise information for
the individual and would incorporate motivational
messages to help the person take action to confront
HEALTHINF 2020 - 13th International Conference on Health Informatics
128

challenges, such as weight loss. When presenting
health information to persons with mild IDD, we need
to consider how they can process and use information.
Therefore, the use of simple vocabulary or pictorial
language which can be understood by persons with
mild IDD could be implemented. This type of
information is likely to be most effective both at the
outset of care and in subsequent maintenance, and
needs to include accurate information about available
treatment(s) (Rivet, 2011). Additional information
can also include health promotion advice and facts
about preventive behaviour.
3.2.2
Motivation
In the past decade, there is a wide range of
recreational software applications intended to
promote various aspects of health-care, from simply
helping people adhere to an activity schedule, get
fitter, or to deal with the day-to-day care of chronic
illnesses. Furthermore, the application of
gamification is popular in physical health domains
such as physical fitness, diet, and managing chronic
illnesses (Werbach and Hunter, 2012). As motivation
is at the heart of sustained behaviour change, games
are deemed to be among the most powerful
motivational tools (Deterding, 2015), and can be
applied to many fields (Zichermann and
Cunningham, 2011). The utilization of gamification
in health-related contexts is growing. Many solutions
are intended to promote wellness and consequently
reduce the potential negative outcomes associated
with unhealthier or risky behaviours (Institute of
Medicine, 2001). For Deterding et al., (2011),
“gamification is about making use of the underlying
principles of gaming and applying them to any non-
game activity”. Moreover, according to Zichermann
and Cunningham (2011) gamification is “the process
of game-thinking and game mechanics to engage
users and solve problems, these definitions that
unites concepts such: as serious games, advergaming,
and games-for-change into a cohesive worldview
that’s informed by the latest research into behavioral
psychology and the success of social games.”
Games are broadly acknowledged as having the
capability to expand persons' motivation. As
indicated by the Federation of American Scientists,
there are numerous elements which make a game
motivating, a fuller understanding of which can aid
the application of gamification in training (Sitra et al.,
2017). Persons with IDD have demonstrated a strong
interest in video games (Mazurek et al., 2015) and
those who are undertaking research into autism have
also been increasingly interested in examining the
effects of video game use. Consequently, many
researchers have focused on developing applications
of game technology for improving social and
behavioural outcomes in persons with IDD (Durkin,
2010, Ern, 2014).
3.2.3
Engagement
Having persons with mild IDD become active
participants in their healthcare is recognized as a
crucial component of high-quality healthcare
services, particularly in the treatment of chronic
illnesses (Hale et al., 2011). Engagement, as shown
in the PCHI, will encourage developers to consider
the use of HIS in terms of their personal health record
to enable data and information sharing between
persons with mild IDD and their healthcare
professionals. Thus, this also has the capacity to
motivate persons with mild IDD. Motivation such as
gamification can also be used to support engagement,
as games are frameworks which are purpose-built for
both enjoyment and engagement (Johnson et al.,
2016).
3.2.4
Communication
This element of the framework focuses on effective
communication between healthcare professionals
and persons with mild IDD. Major goals within the
category of communication from a HIS perspective
are to facilitate easier access for persons with mild
IDD to their health professionals, thereby reducing
reliance on telephone or potentially unsecured email
systems, encouraging persons with IDD to
communicate using their own words, and
empowering them to interact directly with their
personal medical record. We propose that the
communication construct within PCHI could
enhance the communication channel between
persons with IDD and healthcare professionals
through meaningful involvement of all parties in the
care process. The challenge for persons with IDD is
in reframing healthcare professionals as partners who
offer advice and identifying approaches which enable
them to take responsibility for their health and
wellbeing, such as engaging in self-managing
behaviours (Santana and Feeny, 2014).
Health Information Systems for Clients with Mild Intellectual and Developmental Disability: A Framework
129
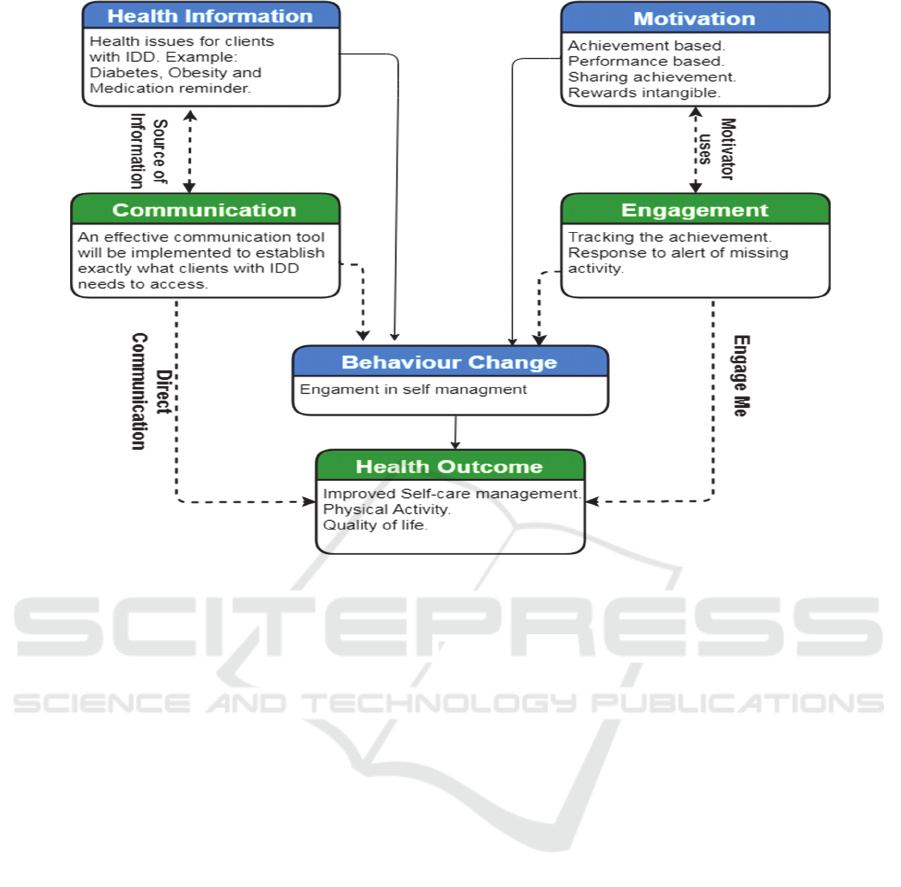
Figure 2: The Person-Centred Health Information Framework (PCHI) version 1.
3.2.5 Behaviour Change
As shown in the PCHI framework, both increased
motivation and the provision of health information
could encourage persons with IDD to change
behaviour. This would support the implementation of
a PCHI framework-based intervention because they
are person-centered and goal-oriented. Several
conceptual models of health behaviour change
describe the factors influencing behavioural
performance across disease contexts, with the
ultimate goal of informing health promotion
interventions (Elder et al., 1999).
Fundamentally, our framework asserts that
persons with mild IDD who are well informed and
motivated are likely to engage in activities that
enhance knowledge and the skills needed to perform
focused and relevant behaviour. Allowing persons
with IDD to reap greater health benefits.
3.2.6
Health Outcome
At a general level, our framework emphasizes that
undertaking positive health behaviour is a function of
the extent to which individuals are well-informed,
motivated, engaged and enabled to communicate.
This will then enable the instigation of behavioural
change, either personally or in conjunction with their
carer. To ensure that persons with mild IDD are not
disenfranchised by the growing number of HIS, their
requirements need to be considered in the
development and design of such systems. PCHI
provides a framework to support and inform such HIS
developments. However, it must be recognised that
persons with IDD may need further support from their
carers and friends, which technology cannot provide,
but may be able to influence.
4
DISCUSSION
In the general population, it is reported that people
who directly communicate health concerns to their
healthcare professionals have a greater degree of
influence on the health outcome. In the interests of
the individual and of equality and inclusion, this
should also be the case for persons with mild IDD. It
is an important behaviour in the healthcare context
because information without accessibility cannot
have any impact on their health unless it is consumed
by persons with IDD. This paper has identified a set
of framework components that should be considered
during HIS developments. This framework can be
used to guide HIS design with the intention of
improving the health outcome for persons with IDD.
HEALTHINF 2020 - 13th International Conference on Health Informatics
130

To this end, we have scoped the parameters of a
design framework, PCHI, incorporating elements
derived from the literature and a previously existing
model, the IMB skills model. The value of this
framework is that it enables us to proactively identify
and understand person-centred HIS design for
persons with mild IDD. Studies in the field of IDD
highlight the benefits of person-centred health
information from both the individual and
organizational perspectives. The PCHI framework
proposes that communication and engagement are
additional intrinsic elements not previously included
in such frameworks. As indicated through the IMB
skills model, this need has not been identified for the
general population. Our paper focuses on a specific
population - persons with mild IDD, and has
highlighted communication and engagement as a
specific need for this population group. Indeed, it is
possible that other specific populations such as those
with dementia or older persons have similar
requirements, but this is not within the scope of this
paper. Design and development of HIS which
consider and include the elements from PCHI can
contribute to better health outcomes for persons with
mild IDD. Our future work will involve the
development of a prototype HIS through the
involvement of persons with mild IDD. Furthermore,
we will test it with a diverse population within a range
of settings.
5 CONCLUSION
There is currently a crucial unmet need for PCHI
targeted person-centered interventions that are easy to
use by persons with IDD who experience cognitive
difficulties and lack social support. The World
Health Organization Report on Disability
recommended the development of a person-centred
framework for assessing people rendered vulnerable
through issues of disability (World Health
Organization, 2015). Such a framework can be useful
for identifying specific health needs and challenges,
assisting the decision-making for persons with mild
IDD and their caregivers. This work commences that
development. Considerable work remains to be done
in terms of HIS development, implementation and
evaluation. Healthcare professionals and family
caregivers are critical partners in the plan for persons
with mild IDD. As reliance on technology grows, we
need to consider other elements which could be
included in PCHI. There is more to be learned about
the effect of person-centred health information on a
person’s health outcomes, and we may need to
consider, for example, safety and quality of care.
Today, more than ever, HIS can play a pivotal role in
enabling persons with mild IDD to become more
independent and capable as they engage in their own
healthcare process.
ACKNOWLEDGMENTS
This work was funded by college of Public Health and
Health informatics, University of Hail. It has been
partially supported by the Science Foundation Ireland
grant 13/RC/2094, co-funded under the European
Regional Development Fund through the Southern &
Eastern Regional Operational Programme to Lero -
the Irish Software Research Centre (www.lero.ie).
REFERENCES
Almunawar, M. N. and M. Anshari (2012). "Health
information systems (HIS): Concept and technology."
arXiv preprint arXiv:1203.3923.
Alshammari, M., Doody, O., & Richardson, I. (2018, June).
Barriers to the Access and use of Health Information by
Individuals with Intellectual and Developmental
Disability IDD: A Review of the Literature. In 2018
IEEE International Conference on Healthcare
Informatics (ICHI) (pp. 294-298). IEEE.
Athilingam, P., Jenkins, B., Johansson, M., & Labrador, M.
(2017). A Mobile Health Intervention to Improve Self-
Care in Patients With Heart Failure: Pilot Randomized
Control Trial. JMIR Cardio, 1(2), e3.
Baker, V., Oldnall, L., Birkett, E., McCluskey, G., &
Morris, J. (2010). Adults with learning disabilities
(ALD) Royal College of Speech and Language
Therapists position paper. London: RCSLT.
Bechtel, C. and D. L. Ness (2010). "If you build it, will they
come? Designing truly patient-centered health care."
Health Affairs 29(5): 914-920.
Burke, S. M. (2017). "The Use of Technology by
Adolescents With Intellectual and Developmental
Disabilities." Journal of pediatric nursing 37: 134.
Chinn, D. (2017). "Review of interventions to enhance the
health communication of people with intellectual
disabilities: A communicative health literacy
perspective." Journal of applied research in intellectual
disabilities 30(2): 345-359.
Chmiliar, L. and C. Anton (2015). "The iPad as a mobile
assistive technology device." Journal of Assistive
Technologies 9(3): 127-135.
Chou, D. (2012). "Health IT and patient safety: building
safer systems for better care." Jama 308(21): 2282-
2282.
de Jong, C. C., Ros, W. J., & Schrijvers, G. (2014). The
effects on health behavior and health outcomes of
Internet-based asynchronous communication between
Health Information Systems for Clients with Mild Intellectual and Developmental Disability: A Framework
131

health providers and patients with a chronic condition:
a systematic review. Journal of medical Internet
research, 16(1), e19.
Deterding, S. (2015). "The lens of intrinsic skill atoms: A
method for gameful design." Human–Computer
Interaction 30(3-4): 294-335.
Deterding, S., Dixon, D., Khaled, R., & Nacke, L. (2011,
September). From game design elements to
gamefulness: defining gamification. In Proceedings of
the 15th international academic MindTrek conference:
Envisioning future media environments (pp. 9-15).
ACM.
Durkin, K. (2010). "Videogames and young people with
developmental disorders." Review of General
Psychology 14(2): 122.
Elder, J. P., Ayala, G. X., & Harris, S. (1999). Theories and
intervention approaches to health-behavior change in
primary care. American journal of preventive medicine,
17(4), 275-284.
Ern, A. M. (2014). The use of gamification and serious
games within interventions for children with autism
spectrum disorder, University of Twente.
Fisher, W. A., Fisher, J. D., & Harman, J. (2003). The
information-motivation-behavioral skills model: A
general social psychological approach to understanding
and promoting health behavior. Social psychological
foundations of health and illness, 82, 106.
Hale, L. A., Trip, H. T., Whitehead, L., & Conder, J. (2011).
Self‐management abilities of diabetes in people with an
intellectual disability living in New Zealand. Journal of
Policy and Practice in Intellectual Disabilities, 8(4),
223-230.
Iedema, R. and M. Manidis (2013). "Patient-clinician
communication: An overview of relevant research and
policy literatures."
Institute of Medicine, A. (2001). "Crossing the quality
chasm: a new health system for the 21st century."
Washington, DC.
Jo Delaney, L. (2018). "Patient-centred care as an approach
to improving health care in Australia." Collegian 25(1):
119-123.
Johnson, D., Deterding, S., Kuhn, K. A., Staneva, A.,
Stoyanov, S., & Hides, L. (2016). Gamification for
health and wellbeing: A systematic review of the
literature. Internet interventions, 6, 89-106.
Kirschner, K. L., Breslin, M. L., & Iezzoni, L. I. (2007).
Structural impairments that limit access to health care
for patients with disabilities. Jama, 297(10), 1121-
1125.
Krist, A. H. and S. H. Woolf (2011). "A vision for patient-
centered health information systems." Jama 305(3):
300-301.
Maulik, P. K., Mascarenhas, M. N., Mathers, C. D., Dua,
T., & Saxena, S. (2011). Prevalence of intellectual
disability: a meta-analysis of population-based studies.
Research in developmental disabilities, 32(2), 419-436.
Mazurek, M. O., Engelhardt, C. R., & Clark, K. E. (2015).
Video games from the perspective of adults with autism
spectrum disorder. Computers in Human Behavior, 51,
122-130.
Mustika, M., Te Kao, C., Cheng, C. Y., Heh, J. S., Lin, C.
S., & Tsai, Y. S. (2014, July). A Multimedia Distance
Language Assessment System for Preschoolers with
Autism Spectrum Disorder: A System Design. In 2014
7th International Conference on Ubi-Media Computing
and Workshops (pp. 319-321). IEEE.
Nguyen, M., Lennox, N., & Ware, R. (2014). Hand‐held
health records for individuals with intellectual
disability: a systematic review. Journal of Intellectual
Disability Research, 58(12), 1172-1178.
Northway, R., Rees, S., Davies, M., & Williams, S. (2017).
Hospital passports, patient safety and person‐centred
care: A review of documents currently used for people
with intellectual disabilities in the UK. Journal of
clinical nursing, 26(23-24), 5160-5168.
Organization, W. H. (2015). World report on ageing and
health, World Health Organization.
Osborn, C. Y., Rivet Amico, K., Fisher, W. A., Egede, L.
E., & Fisher, J. D. (2010). An information-motivation-
behavioral skills analysis of diet and exercise behavior
in Puerto Ricans with diabetes. Journal of health
psychology, 15(8), 1201-1213.
Rahimi, B., Nadri, H., Afshar, H. L., & Timpka, T (2018).
"A systematic review of the technology acceptance
model in health informatics." Applied clinical
informatics 9(03): 604-634.
Rivet Amico, K. (2011). "A situated-Information
Motivation Behavioral Skills Model of Care Initiation
and Maintenance (sIMB-CIM): an IMB model based
approach to understanding and intervening in
engagement in care for chronic medical conditions."
Journal of health psychology 16(7): 1071-1081.
Sabaté, E. (2003). Adherence to long-term therapies:
evidence for action, World Health Organization.
Santana, M.-J. and D. Feeny (2014). "Framework to assess
the effects of using patient-reported outcome measures
in chronic care management." Quality of Life Research
23(5): 1505-1513.
Sitra, O., Katsigiannakis, V., Karagiannidis, C., &
Mavropoulou, S. (2017). The effect of badges on the
engagement of students with special educational needs:
A case study. Education and Information Technologies,
22(6), 3037-3046.
Werbach, K. and D. Hunter (2012). For the win: How game
thinking can revolutionize your business, Wharton
Digital Press.
Zichermann, G. and C. Cunningham (2011). Gamification
by design: Implementing game mechanics in web and
mobile apps, " O'Reilly Media, Inc.".
HEALTHINF 2020 - 13th International Conference on Health Informatics
132
