
A Method for Defining Edge Margin Field and Its Application
Yanjin Liu
*
, Jun Wu, Shuhui Xu and Biao Peng
Faculty of Mechanical Engineering, Qilu University of Technology (Shandong Academy of Sciences), Jinan 250353, China
Keywords:
Tumors of Liver, Incisal Edge, Margin Field, Aided Navigation.
Abstract:
Hepatectomy is one of the main treatment methods for liver tumor resection at present. However, the key
technology for accurate navigation and localization of intrahepatic tumors during surgery to achieve the
resection of hepatocellular carcinoma is still unclear. This paper is written for minimally invasive laparoscopic
liver resection of the tumor in the auxiliary navigation technology. This paper provides a method for defining
the margin field of hepatic tumor incision margins and a model system and the application of measuring the
scalpel and tumor distance. The purpose of this paper is to assist physicians in making intraoperative surgical
decisions, correct the surgical path in a timely manner and achieve a low-risk effect of minimally invasive
laparoscopic surgery.
1 INTRODUCTION
Liver cancer is one of the most common malignancies
worldwide. (Habib, 2015) Patients with early-stage
liver cancer can undergo surgical treatment such as
surgical resection, liver transplantation, and tumor
ablation, of which surgical resection is the preferred
treatment option. (Takamoto, 2019) The incidence of
liver cancer ranks sixth in the world's malignant
tumors, and the mortality rate ranks second in the
world's malignant tumors. China is a country with a
high incidence of liver cancer. According to data
released by the World Health Organization in 2015,
there are about 93 million people living with hepatitis
B virus in China, of which 1-5% of patients develop
liver cancer, new cases account for about half of the
world. Liver cancer kills about 300,000 people each
year, including 40% of the elderly. (Journal of
hepatology, 2018; Mareng, 2016; Huang, 2016; Della,
2016)
Before doing liver resection, the surgeon needs to
evaluate the residual remaining liver volume with the
help of preoperative CT liver three-dimensional
reconstruction or physician experience to prevent
excessive liver removal from causing liver failure. In
hepatectomy, the chief surgeon roughly estimates the
incision line according to the preoperative CT image,
with the surgeon's clinical experience and spatial
imagination ability, supplemented by color
ultrasound confirmation and adjustment of the cutting
line. The identification of intrahepatic duct anatomy
in the process of hepatotomy is mainly determined by
the general anatomical cognition of the ischemic line
on the hepatic surface or the clinical experience of the
surgeon to achieve anatomical hepatic resection.
Make sure that the incisional margin is not less than
one centimeter from the surface of the liver tumor.
(Moris, 2018; Yoon, 2017)
There are many effects of margin width on the
postoperative removal of hepatocellular carcinoma.
In general, complete resection of the lesion and
sufficient distance from the lesion is considered
important to ensure eradication of malignancy and to
avoid recurrence as much as possible. One centimeter
margin is sufficient for most liver cancer patients, but
for those who can tolerate a wide range of liver
resection, two centimeter margin can helps to reduce
tumor recurrence.
As we all know, the current difficulty of
laparoscopic liver tumor resection is that: first of all,
most of the ultrasound localization is used to perceive
the two-dimensional image information of the tumor
in the liver, but the depth information of the tumor
cannot be determined. And the surgeon in the
operation cannot accurately determine the relative
position relationship between the tumor and the blood
vessel due to the lack of three-dimensional
information inside the liver. The above two
difficulties may lead to the surgeon removing excess
liver or incomplete tumor cutting so that there is no
guarantee of optimal trajectory to remove the liver
Liu, Y., Wu, J., Xu, S. and Peng, B.
A Method for Defining Edge Margin Field and Its Application.
DOI: 10.5220/0012020500003633
In Proceedings of the 4th International Conference on Biotechnology and Biomedicine (ICBB 2022), pages 325-328
ISBN: 978-989-758-637-8
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
325

tumor. It increasing the risk of surgery and prolonging
the operation time.
Aiming at the problems of high surgical risk and
long surgical time during liver tumor resection in
existing techniques, this paper proposes a method for
establishing a marginal field model for tumor
resection and the application of measuring the
distance between scalpel and tumor during liver
resection surgery.
2 SOFTWARE AND METHODS
FOR 3D RECONSTRUCTION
OF DICOM IMAGING DATA
2.1 Software
Design and simulation of 3D virtual liver surgery
based on CT scan data, the 64-row thin layer scanning
dataset of the patient's abdominal liver was collected.
In this paper, Mimics software developed by the
Belgian company Materialise was used for three-
dimensional reconstruction of the liver, intrahepatic
tumors and their intrahepatic blood vessels.
2.2
The Basic Steps of Modeling
Medical Image Processing Software
Mimics
DICOM data read: We first imported a standard
Dicom3.0 format image file formed from more than
400 CT scans of the patient's abdomen into Mimics
software. After receiving the command, the software
will automatically generate coronal and sagittal
images based on the cross-sectional images, which
are shown separately in Fig. 1.
Threshold profile extraction and three-
dimensional reconstruction: Due to the different CT
values of different tissues, the CT difference between
the corresponding tissues and organs themselves is
small and the difference with other surrounding
tissues and organs is large, so that use the threshold
setting tool in the toolbar to set the corresponding
threshold to segment the image. Mimics will split all
the pixels extracted under a template called Mask, and
Mimics will provide a series of editing and
modification operations for this template to extract
and refine the required tissues and organs. By editing
the template, we can do 3D modeling to achieve the
transformation from a 2D image to a 3D solid, as
shown in the lower right corner of Fig. 1. (Mi, 2021)
Figure 1: Three-dimensional images reconstructed after the patient CT was imported into Mimics.
3 A METHOD FOR DEFINING
THE MARGIN FIELD OF
HEPATIC TUMOR INCISION
MARGINS
3.1 Define the Method
The envelope is a convex surface that tightens the
tumor. After the threshold segmentation extraction of
the intra-abdominal tumor by Mimics software, the
model of the tumor is exported, and the contour of the
outer surface of the tumor is known to be uneven, and
the surface of the concave area on the tumor surface
is first obtained by the convex surface of the tumor
surface algorithm to obtain a convex surface model of
the tight enveloping tumor, and the convex surface
obtained by smoothing it is the envelope surface of
the tumor, as shown in Figure 2(a).
Then, a point A is randomly selected on the
envelope surface, the crossing point A is the tangent
plane Σ of the envelope surface, and the straight line
segment perpendicular to the tangent plane Σ is the
ICBB 2022 - International Conference on Biotechnology and Biomedicine
326

normal segment at a certain point A on the envelope
surface. By analogy, taking all the points on the tumor
envelope as the starting point, each point on the
envelope surface is made perpendicular to the normal
segment of the tangent plane Σi at the point, the length
of the normal segment is set as 1cm per unit length,
and finally a new convex surface composed of the end
point of the unit length normal segment is obtained,
so that the new convex surface is defined as a tangent
edge surface 1cm away from the tumor outer network,
and its principle is regarded as the uniform expansion
deformation of the tumor model. In summary, the
outward expansion deformation is based on all the
points on the envelope surface, and the convex
surface that expands and deforms by 1 cm is defined
as the tangent edge surface of the tumor. The distance
from any point on the cut edge surface to the tumor
should be no less than 1 cm, as shown in Fig. 2(a).
Finally, based on the envelope surface isometric
expansion to obtain a plurality of convex surfaces,
consisting of a plurality of progressively deformed
and expanded convex surfaces of the field, we define
it as the margin field of the tumor, wherein the
interval between each surface of the margin field is 1
cm, as shown in Figure 2 (b), the distance from the
above-mentioned cut edge surface to the tumor
surface contour is 1 cm, the cut edge surface is the
tumor 1 cm margin field.
(a) (b) (c)
Figure 2: The outer contour surface, envelope surface, and marginal field of the tumor.
3.2 Distance Calculation Application
Between Scalpel and Tumor Based
on Margin Margin Field
In the future minimally invasive liver tumor resection,
robot technology will be continuously introduced for
the requirements of accurate removal of liver tumors,
and under the motion simulation model based on
robot surgical action, the definition and visualization
of the margin field provide the robot with distance
parameters to know the distance d of the scalpel and
the tumor boundary. According to the distance
between the margin field and the envelope surface, it
is named, as shown in Fig. 2(c). Such as 1cm margin
field, 2cm margin field and 3cm margin field, etc.
Assuming that the scalpel head is located between the
2cm to 3cm margin field in the simulation model of
robot motion, it is obvious that the distance from the
scalpel head to the tumor is 2 to 3cm. In summary, the
definition of marginal field can be used in future
robotic minimally invasive surgery to measure the
distance between the scalpel and the intrahepatic
tumor, providing auxiliary guidance for physicians
when removing the tumor during surgery, and
avoiding the risk of surgery caused by the scalpel
touching the tumor.
3.3
Establishment System for Marginal
Fields
Fig. 3 Further provides an establishing module for
tumor margin margin field, comprising: establishing
module 1, determining module 2, envelope creation
module 3 and determining module 4. Wherein, the
establishment of module 1 for obtaining the patient's
imaging data, through the three-dimensional
reconstruction of the body data to obtain a model of
the relative position relationship between the tissues;
judgment module 2, for calling the relative position
information between the tumor and other tissues to
determine the resectability of the tumor, if yes
(intrahepatic tumor has resectability), into the
envelope creation module 3, if not, end; the envelope
creation module is used to establish an envelope
surface according to the external contour information
of the tumor surface, the envelope surface is the
convex envelope of the tumor; determine module 4, It
is used to determine the tumor 1 cm margin and
margin
field based on the envelope surface of the
A Method for Defining Edge Margin Field and Its Application
327
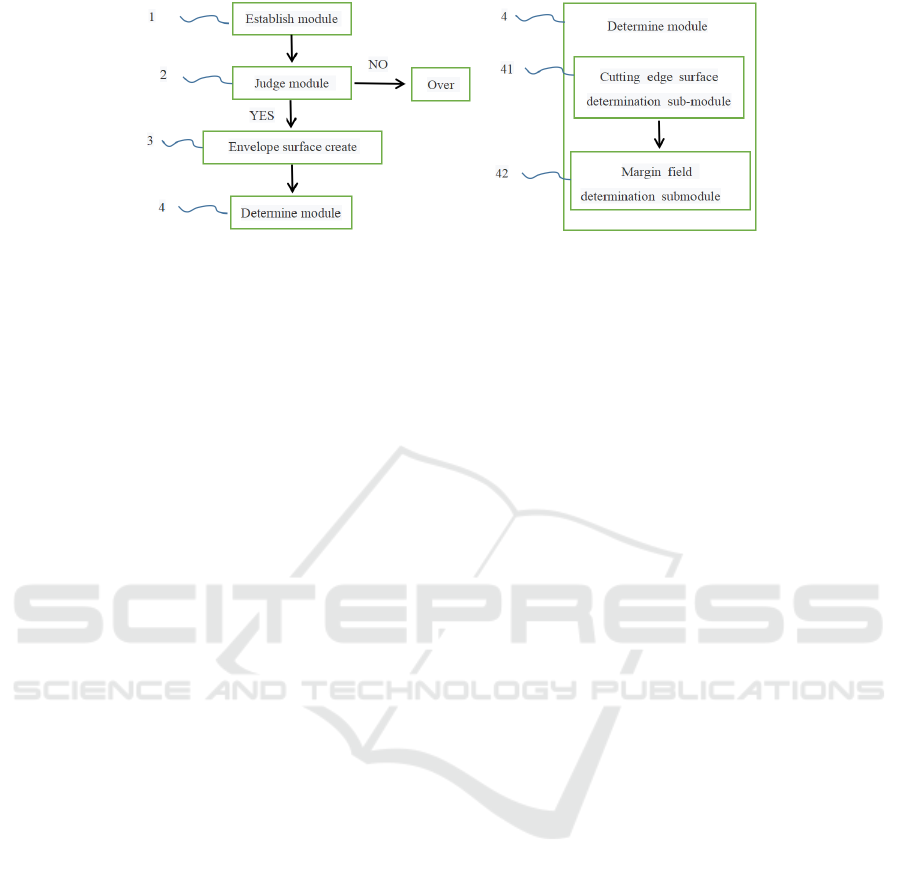
Figure 3: The overall structure diagram of the system for the establishment of tumor margin field.
tumor. According to the model established by the
system, the situation of intrahepatic tumors in the
human body is effectively simulated, and then
according to the location relationship between tumors
and intrahepatic blood vessels in the liver, a
reasonable anatomical direction is selected to
determine how to achieve complete resection of
tumors with the purpose of minimizing liver damage.
4 CONCLUSION
In this paper, we first elaborate on the global impact
of liver cancer incidence and the limitations of
treatment strategies and surgical treatment options,
and then propose the establishment method and
distance measurement application of a tumor excision
margin field model for the reasons why it is difficult
to know the depth of intrahepatic tumor information,
resulting in greater surgical risk and long surgical
time.
This paper analyzes the three-dimensional
reconstruction process of CT body data of Mimics
software, and it can be seen that Mimics can well
display the corresponding three-dimensional anatomy
of the human body, so that doctors can make detailed,
reasonable and accurate disease diagnosis; this paper
also provides a definition method and establishment
system of tumor margin margin field; finally
describes the application of tumor margin margin
field to measure the distance between scalpel and
tumor in future robotic minimally invasive surgery,
based on the scalpel in real time positioning feedback
information in the three-dimensional model. In this
way, it assists physicians in making intraoperative
decisions, can change the surgical path in time, and
finally achieves accurate resection of lesion areas in
robot-assisted liver tumor resection and achieves low-
risk surgical results.
ACKNOWLEDGMENTS
This research was supported by the Natural Science
Foundation of Shandong Province (Application No.
ZR202109280010).
REFERENCES
Della Corte C, Triolo M, Iavarone M, Sangiovanni A. Early
diagnosis of liver cancer: an appraisal of international
recommendations and future perspectives. Liver Int
2016; 36:166-76.
EASL Clinical Practice Guidelines: Management of
hepatocellular carcinoma. Journal of hepatology2018;
69: 182-236.
Habib A, Desai K, Hickey R, et al. Locoregional therapy of
hepatocellular carcinoma [J]. Clin Liver Dis, 2015,
19(2): 401-420.
Huang YQ, Lu X, Min H, Wu QQ, Shi XT, Bian KQ, Zou
XP. Green tea and liver Cancer risk: A meta-analysis of
prospective cohort studies in Asian populations.
Nutrition2016; 32: 3-8.
Marengo A, Rosso C, Bugianesi E.Liver Cancer:
Connections with Obesity, Fatty Liver, and Cirrhosis.
AnnuRevMed 2016; 67: 103-17.
Mi Meng; Huang Dongning; Yang Kaixing. Treatment of
extra-articular scapular fractures with assistance of 3D
reconstruction measurements with Mimics software
2021; 23(8): 688-693.
Moris D, Vernadakis S. Laparoscopic Hepatectomy for
Hepatocellular Carcinoma: The Opportunities, the
Challenges, and the Limitations. Annals of surgery
2018; 268: e16.
Takamoto T, Makuuchi M. Precision surgery for primary
liver cancer [J]. Cancer Biol Med, 2019,16(3):475-485.
Yoon YI, Kim KH, Kang SH, Kim WJ, Shin MH, Lee SK,
et al. Pure Laparoscopic Versus Open Right
Hepatectomy for Hepatocellular Carcinoma in Patients
with Cirrhosis: A Propensity Score Matched Analysis.
Annals of surgery 2017; 265:856-863.
ICBB 2022 - International Conference on Biotechnology and Biomedicine
328
