
Linear Analysis of National Life Expectancy
Huijia Wang
XJTLU Wisdom Lake Academy of Pharmacy, China
Keywords: Life Expectancies, Linear Regression, Generalized Linear Model, Regression Diagnosis.
Abstract: Life expectancy is the most important indicator to measure the population’s health status. It is also a
comprehensive indicator to measure a country’s economic and social development and medical and health
service level. It is affected by biological factors, environmental factors, lifestyle, and medical and healthcare
systems. This study aims to explore how the national life expectation changes and the differences in regions
and potential health care systems. The given dataset and related data are for human development reports.
There are 185 countries considered in this study. Besides regional factors, many variables affect life
expectancy, such as Total fertility rate (FERTILITY), Health expenditure per capita (HEALTHEXPEND),
Public expenditure on education (PUBLICEDUCATION) and so on. In this paper, we developed a simple
linear model and a multiple regression model using stepwise regression to explore which potential variables
have a more significant effect on life expectancy and test the feasibility and plausibility of the model. We
find that region, fertility, health care costs, and public expenditure on education significantly affect national
life expectancy. Finally, we developed generalized linear models with different linkage functions for
comparison and further analysis.
1 INTRODUCTION
The average life expectancy of the population is an
indicator to measure the level of economic
development and medical and health services of a
society. Two aspects restrict the length of life
expectancy. On the one hand, social and economic
conditions and health care levels limit people’s life
spans, so the length of life span varies significantly
in different societies and periods. On the other hand,
due to personal differences in physique, genetic
factors, and living conditions, the length of life of
each person also varies greatly. With the
improvement of the modern medical system, the
health care system has gradually become an
essential indicator of life expectancy (Feynman,
1963). Virtually every person, corporation, and
government have their perspective on health care;
These different perspectives result in a wide variety
of systems for managing health care (Dirac, 1953).
Comparing different health care systems helps us
learn about approvals other than our own, which
helps us make better decisions in designing
improved systems (Frees, 1993).
An assessment of the poverty, production, and
environmental challenges in CARICOM countries
showed that scientists had examined the current
human development experience of CARICOM
countries, focusing on the interrelated challenges of
poverty, production, and environment, which
showed that development remained unbalanced.
Therefore, the national medical and health services
may not be guaranteed accordingly (Lima, 2020).
And in some remote and barren countries, the health
care system is not perfect. The Brazilian National
Cancer Institute (INCA) periodically publishes
cancer incidence estimates of the nineteen main
cancer sites in Brazil (Perry, 2020). And this report
aims to explore how the national life expectancy
changes and differs in regions and potential health
care systems through R studio.
2 DATA PREPROCESSING
Who is doing health care right? Health care
decisions are made at the individual, corporate and
government levels. Virtually every person,
corporation and government have their own
perspective on health care; these different
perspectives result in a wide variety of systems for
managing health care. Comparing different health
Wang, H.
Linear Analysis of National Life Expectancy.
DOI: 10.5220/0012040700003620
In Proceedings of the 4th International Conference on Economic Management and Model Engineering (ICEMME 2022), pages 617-623
ISBN: 978-989-758-636-1
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
617

care systems help us learn about approaches other
than our own, which in turn help us make better
decisions in designing improved systems.
Here, we consider health care systems from n =
185 countries throughout the world from the
UNLifeExpectancy.csv for National Life
Expectancies from the following website:
https://instruction.bus.wisc.edu/jfrees/jfreesbook
s/Regression%20Modeling/BookWebDec2010/data.
html.
The data is concerned with human development
reports. We see https://hdr.undp.org/en/data for
more details. The details are included in Table 1
below.
Table 1: Data description.
Variable Number of Obs Missing Description
REGION 0 Categorical variable for region of the world
COUNTRY 0 The name of the country
LIFEEXP 0 Life expectancy at birth, in years
ILLITERATE 14 Adult illiteracy rate, % aged 15 and older
POP 1 2005 population, in millions
FERTILITY 4 Total fertility rate, births per woman
PRIVATEHEALTH 1 2004 Private expenditure on health, % of GDP
PUBLICEDUCATION 28 Public expenditure on education, % of GDP
HEALTHEXPEND 5 2004 Health expenditure per capita, PPP in USD
BIRTHATTEND 7 Births attended by skilled health personnel (%)
PHYSICIAN 3 Physicians per 100,000 people
SMOKING 88 Prevalence of smoking, (male) % of adults
RESEARCHERS 95 Researchers in R & D, per million people
GDP 7 Gross domestic product, in billions of USD
FEMALEBOSS 87 Legislators, senior officials and managers, % female
As a measure of the quality of care, we use
LIFEEXP, the life expectancy at birth. There are
185 countries consider in this study, not all countries
provided information for each variable. Data not
available are noted under the column “NA”. The
descriptive statistics are included in Table 2 below.
Table 2: Descriptive statistics.
mean sd 0% 50% 100% n NA
LIFEEXP 67.050811 11.081747 40.5 71.0 82.3 185 0
ILLITERATE 17.688304 19.862690 0.2 10.1 76.4 171 14
POP 35.357609 131.698363 0.1 7.8 1313.0 184 1
FERTILITY 3.189503 1.707809 0.9 2.7 7.5 181 4
PRIVATEHEALTH 2.517391 1.329662 0.3 2.4 8.5 184 1
PUBLICEDUCATION 4.694904 2.046379 0.6 4.6 13.4 157 28
HEALTHEXPEND 718.005556 1037.012073 15.0 297.5 6096.0 180 5
BIRTHATTEND 78.252809 26.420077 6.0 92.0 100.0 178 7
PHYSICIAN 146.076923 138.553078 2.0 107.5 591.0 182 3
SMOKING 35.092784 14.399857 6.0 32.0 68.0 97 88
RESEARCHERS 2034.655556 4942.933272 15.0 848.0 45454.0 90 95
GDP 247.551124 1055.692710 0.1 14.2 12416.5 178 7
FEMALEBOSS 29.071429 11.709763 2.0 30.0 58.0 98 87
We conduct the following exploratory analysis
concerning the distribution of LIFEEXP and
determine if we may do some transformation so as
to symmetrize the distribution. First, we use the
histogram to see the distribution of the variable in
Figure1. It can be seen from the histogram that this
ICEMME 2022 - The International Conference on Economic Management and Model Engineering
618
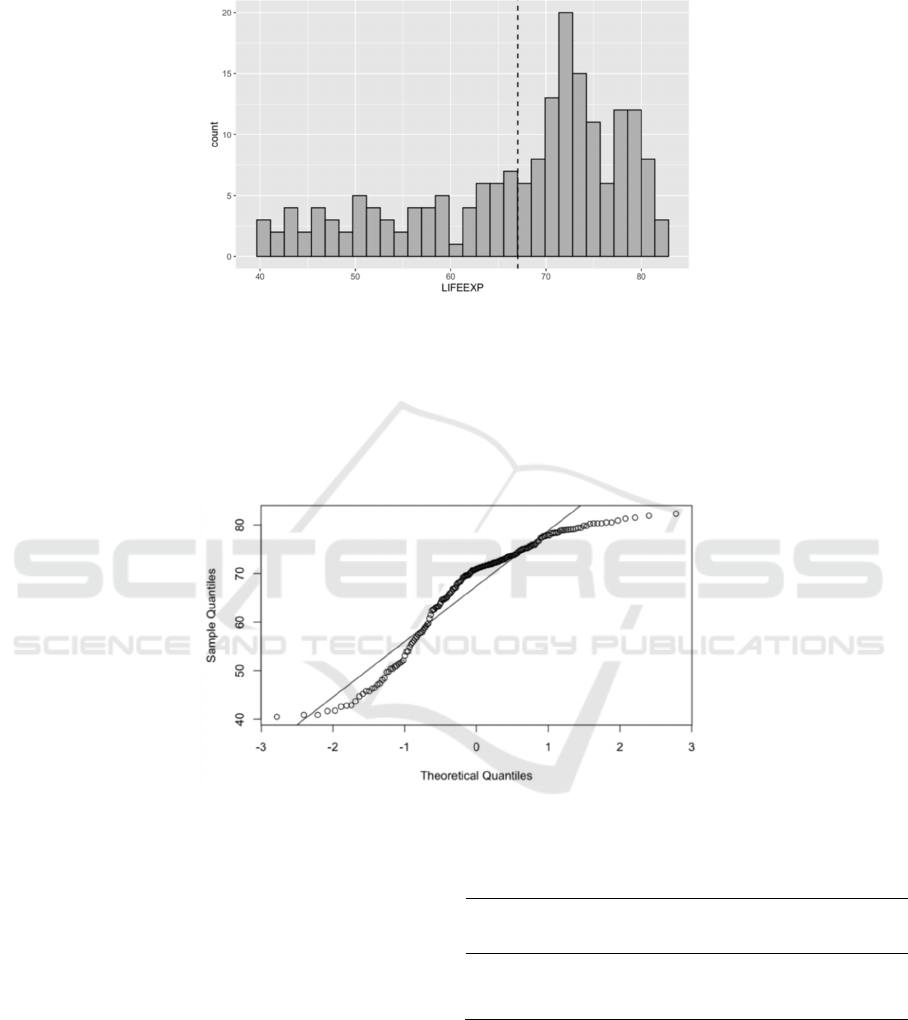
variable has no obvious symmetrical trend and
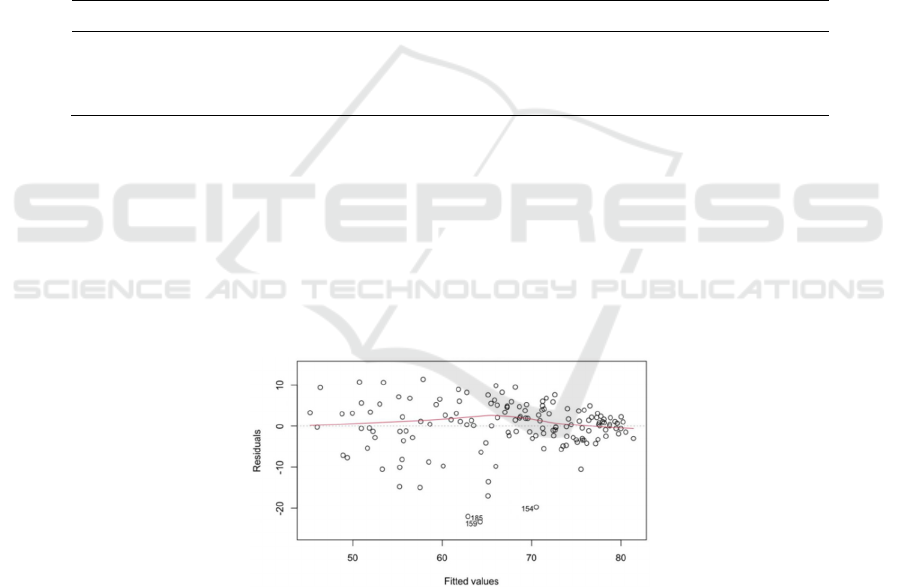
cannot be considered as normal distribution. Then
we further use the QQ plot to test in Figure2.
Figure 1: Histogram of LIFRRXP.
When viewing them, the histogram appears to be
skewed to the left. The QQ plot indicates a serious
departure from normality. If we take a natural log
transformation and examine the distribution of this
transformed variable when viewing them, the
transformation still does little to symmetrize the
distribution. It can also be seen from the correlation
matrix that the FERTILITY variable has a strong
correlation with LIFEEXP, and the value in the
correlation coefficient matrix is the largest, so we
can consider establishing a simple linear model of
these two variables.
Figure 2: QQplot of LIFRRXP
3 MODEL ANALYSIS
3.1 A simple Linear Model of Life
Expectancy
We continue the analysis by examining the relation
between y = LIFEEXP and x = FERTILITY. Fit a
linear regression model of LIFEEXP by
FERTILITY. The results are shown as follows.
Table3. Simple linear model regression results
Estimate Std.
Error
t value Pr(>|t|)
(Intercept) 83.7381 1.0439 80.22 <2e-16
FERTILITY -5.2735 0.2887 -18.27 <2e-16
Through observation, we found that p-value <
2.2e-16, so fertility variables have a significant
impact on life expectancy. The obtained linear
model formula is as follows.
LIFEEXP 𝛽
ˆ
𝛽
ˆ
𝐹𝐸𝑅𝑇𝐼𝐿𝐼𝑇𝑌
5.2735𝐹𝐸𝑅𝑇𝐼𝐿𝐼𝑇𝑌 83.7381
(1)
Linear Analysis of National Life Expectancy
619
3.2 A Multiple Linear Regression
Model of Life Expectancy
After considering establishing a simple univariate
linear model, we will consider using the basic
multivariate linear regression model. According to
the analysis and observation of the missing values of
the data, we found that the variables
RESEARCHERS, SMOKING, and FEMALEBOSS
have many missing values, so these columns of
variable values should be deleted when establishing
the model.
And we can find that the means and standard
deviations of the HEALTHEXPEND variable and
the GDP variable in the data set are large, more than
several hundred times those of the other variables.
At this point, we should consider a log-transformed
form. Taking logarithms of the variables in the
linear regression model can reduce the absolute
differences between the data and the effect of
individual extreme values.
Then we use the filtered variables to establish a
multivariate linear model. However, not every
variable in the model has significant meaning, so we
need to carry out stepwise regression to further
screen and analyze. From the results of stepwise
regression that after two rounds of regression, the
variable FERTILITY, PUBLICEDUCATION, and
lnHEALTH are significant in the model. So next we
consider fitting the regression model with these
three variables. The result is in Table4 as follows.
Table 4: Multiple regression model results.
Estimate Std. Error t value Pr(>|t|)
(
Interce
p
t
)
60.7626 4.5865 13.248 < 2e-16
lnHEALTH 3.2777 0.5864 5.589 1.09e-07
PUBLICEDUCATION -0.5341 0.2549 -2.095 0.0379
FERTILITY -3.2220 0.4934 -6.531 1.02e-09
As we expected in Table3, each variable is
significant in the model. The expression of the
established multivariate linear model is as follows.
LIFEEXP
β
β
lnHEALTH
β
PUBLICEDUCATION
β
FERTILIT
Y
(2)
60.7626 3.278lnHEALTH
0.534PUBLICEDUCATION
3.222FERTILIT
Y
Also we can do diagnosis plots with this model.
The results are in Figure3, Figure4, Figure5,
Figure6. It shows that most assumptions on the
linear models are consistent with the data
information.
Figure 3: Residuals vs Fitted.
ICEMME 2022 - The International Conference on Economic Management and Model Engineering
620
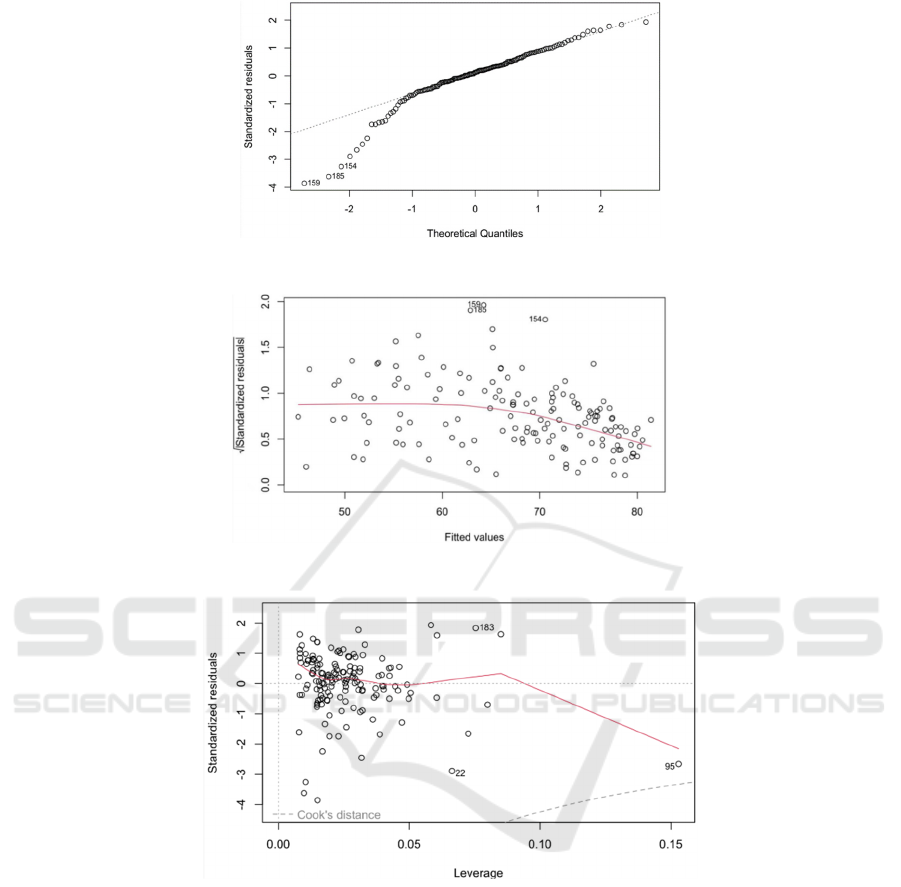
Figure 4: Normal QQplot.
Figure 5: Scale-Location.
Figure 6: Residuals vs Leverage.
Specifically, we conclude the following:
1.First, the standardized residuals have no
apparent trend in its fitted values. Thus, the
heteroscedasticity of the response variable is not
significantly shown.
2. Second, we see that the normality of the
residuals seems acceptable according to the normal
QQ plot, besides the 154th,159th and 185th
observations. Since the empirical quantile based on
normal distribution is fairly close to the theoretical
quantile.
3.Finally, we can see that there is no correlation
between the residual series and prices. Therefore,
the independence assumption seems to be
acceptable.
3.3 Model Improvement and Variable
Selection
The study in the previous section shows that
national life expectancy is significantly associated
with the total fertility rate, public expenditure on
education, and 2004 health expenditure per capita.
As we want to explore how the national life
expectancy changes and differs in regions and
Linear Analysis of National Life Expectancy
621
potential health care systems, in this section we will
add the region variable to the model.
Then we added the categorical variable REGION
to the initial model and again performed stepwise
regression to filter the new model. From the results,
we found that FERTILITY, REGION,
PHYSICIAN, PUBLICEDUCATION and
lnHEALTH have a significant impact.
We take the Variance Inflation Factor to check if
there is any obvious collinearity. As we know the
larger VIF implies high correlation between the
independent variable and the remaining variables. It
means that different combinations of the covariates
may lead to the same fitted values, which is
therefore mainly a problem for interpretation rather
than prediction, and cause numerical problems
during the fitting process. For this model, variable
PHYSICIAN has a VIF of 2.60. and a maximum
correlation of 70.1% with the other variables.
Therefore, the removal of this variable could be
considered for the model.
Then we fit a regression model using three
explanatory variables, FERTILITY,
PUBLICEDUCATION, and lnHEALTH, as well as
the categorical variable REGION. The result is in
Table5.
Table 5: Multiple regression model results (add REGION).
Estimate Std. Error t value Pr(>|t|)
(Intercept) 61.4123 64.3493 14.120 < 2e-16
PUBLICEDUCATION -0.5492 0.2416 -2.273 0.0245
lnHEALTH 3.8136 0.5702 6.688 4.58e-10
FERTILITY -3.0003 0.4705 -6.376 2.28e-09
REGION -0.8802 0.2100 -4.191 4.80e-05
All variables are significant in this model. And
the expression of the established multivariate linear
model is as follows.
LIFEEXP β
β
lnHEALTH β
PUBLICEDUCATION β
FERTILITY β
REGION
61.4123 3.8136 lnHEALTH 0.5492 PUB 3.000FER 0.880REGION
(3)
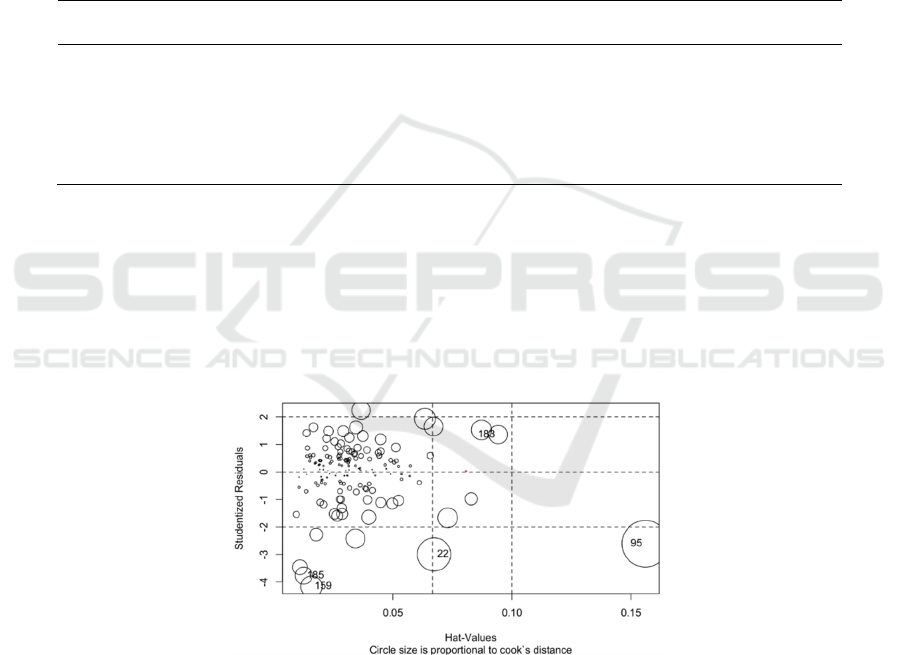
Clearly, this model explains the data very well.
The coefficient of determination is 73% and each
variable has a significant impact on life expectancy.
We also can use Cook’s distance to further draw the
influence diagram to observe some outliers in Figure
7.
Figure 7: Influence Plot.
3.4 Modeling and Screening of
Generalized Linear Models
The generalized linear model is an extension of the
linear model and establishes the relationship
between the mathematical expectation of the
response variable and a linear combination of
predictor variables through a linkage function. It is
characterized by the fact that the natural measure of
the data is not forcibly altered and the data can have
a non-linear and non-constant variance structure. It
is a development of the linear model in the study of
non-normal distributions of response values and the
concise and direct linear transformation of non-
linear models.
ICEMME 2022 - The International Conference on Economic Management and Model Engineering
622

In this problem, we can also consider the
modelling of generalised linear models. We use
different link functions and families to build the
corresponding models and thus compare them to
obtain the best model. Because the join function
involves a logarithmic link function, the
HEALTHEXPEND variable is not treated
logarithmically in this question.
Do the glm LIFEEXP and
PUBLICEDUCATION+HEALTHEXPEND+FERT
ILITY+REGION. The result is in Table6 below.
Table 6: Results of generalized linear model.
EDM
g(μ)
𝛽
^
𝛽
^
𝛽
^
𝛽
^
AIC
Gaussian Identity -0.451 0.004 -4.246 -1.369 950.2
Gamma Identity -0.608 0.005 -4.043 -1.531 982.9
Inverse Gaussian Identity -0.699 0.005 -3.928 -1.625 1004
Gaussian Log -5.092 e-03 5.255 e-05 -7.115 e-02 -2.012 e-02 954.4
Gamma Log -7.395 e-03 6.002 e-05 -6.988 e-02 -2.269 e-02 985.6
Inverse Gaussian Log -8.779 e-03 6.465 e-05 -6.884 e-02 -2.416 e-02 1006
Then we can find the gaussian response with
identity function seems most appropriate, since both
regression parameters are significant for modelling
LIFEXP, and the AIC is the smallest among all the
models.
Interestingly, we know that the Gaussian
distribution is approximated as a normal
distribution. That said, if we use the above variables
to build a linear model, a multivariate linear model
might work better than a generalised linear model,
as not every variable is suitable for modelling using
a logarithmic link function. Whether there is a more
appropriate generalised linear model deserves
further research and investigation.
4 CONCLUSION AND
DISCUSSION
In this paper, we first conducted a descriptive
analysis of the data, observing the missing value
characteristics of some variables. The correlation
matrix of the data was then derived, and a simple
linear model was developed and analyzed for the
most highly correlated variables. We then built a
multiple regression model using stepwise regression
to explore which potential variables had a more
significant effect on life expectancy and test the
model’s feasibility and plausibility. After analyzing
this model, we added the region variable, a
categorical variable with significantly different
means across regions. After building a new model
using stepwise regression, we found that region,
fertility rate, healthcare costs, and public education
expenditure significantly affected national life
expectancy. Finally, generalized linear models with
different link functions were developed for
comparison and further analysis.
However, this article still has some
shortcomings, such as the treatment of the selection
of variables by deleting columns with many missing
values. It is worth further debating how to
supplement the missing values. As well as in the
generalized linear model, there is no better choice of
linking function, and the form of the link function
still needs further determination. Finally, I believe
that the established multivariate linear model R
2
can
still be further improved, and in the future, we may
conduct further research.
REFERENCES
Dirac P. (1953) The lorentz transformation and absolute
time. Physica, 19:888–896.
https://doi.org/10.1016/S0031-8914(53)8009 9-6
Feynman R, Vernon F. (1963) The theory of a general
quantum system interacting with a linear dissipative
system. Annals of Physics, 24:118–173.
https://doi.org/10.1006/aphy.2000.6017
Frees E. (1993) Regression modeling with actuarial and
financial applications. Cambridge University Press,
London. https://doi.org/10.1017/CBO9780511814372
Lima M, Siqueira H, Moura A, Hora E, Brito H, Marques
A, et al. (2020) Temporal trend of cancer mortality in
a Brazilian state with a medium Human Development
Index (1980–2018). Sci Rep. 10(1):213-284.
https://doi.org/10.1038/s41598-020-78381-4
Perry K. (2020) Structuralism and Human Development:
A Seamless Marriage? An Assessment of Poverty,
Production and Environmental Challenges in
CARICOM Countries. International Journal of
Political Economy.49(3):222–242.
https://doi.org/10.1080/08911916. 2020.1824735
Linear Analysis of National Life Expectancy
623
