
Wellbeing Recommender System, a User-Centered Framework for
Generating a Recommender System for Healthy Aging
Jordi Torres
1a
, Meritxell Garcia
1b
, Garazi Artola
1,2 c
, Teresa Garcia-Navarro
1d
,
Isabel Amaya
1e
, Nekane Larburu
1,2 f
and Cristina Martin
1,3 g
1
Vicomtech Foundation, Basque Research and Technology Alliance (BRTA),
Mikeletegi 57, 20009 Donostia-San Sebastián, Spain
2
Biodonostia Health Research Institute (Bioengineering Area), eHealth Group, 20014 Doonstia-San Sebastián, Spain
3
Faculty of Engineering, University of Deusto, Av.Universidades, 24, 48008, Bilbao, Spain
Keywords: Healthy Aging, Recommender System, Quality of Life, Synthetic Data Generation.
Abstract: The needs of the currently aging population require new technologies to support them in order to offer them
a decent quality of life. Different interventions have been proposed in the last years to face this challenge,
where recommender systems are gaining strength. The general objective of these systems is to promote the
adoption of healthy habits among the end users, but sometimes they show limitations in the fulfilment of this
goal. To overcome these limitations, our approach offers an easy to maintain, interoperable, and personalized
recommender system capable of providing recommendations based on individuals’ daily activity data. A
methodology is presented for the generation and management of wellbeing recommendations, which are then
tested using a synthetically generated dataset that simulates a variety of user categories. With the evaluation
of this data, a technical validation is carried on to assess the performance and scalability of our developed
system.
1 INTRODUCTION
The current trend of population aging, especially in
developed countries, will pose several challenges to
our society, comprising from changes in the structure
of health and social services, as well as the financial
system and labour markets (Ahtonen, 2012).
Predictions indicate an increase of the burden of age-
related expenditures in state budgets. Increasing life
expectancy comes with a variety of changes in the
care of elderly people as we know it today, with
growing evidence that a shift from targeting
individual diseases to postponing physical
deterioration and comorbidities (Goldman et al.,
2013). Considering that the elderly population is the
group that requires the most from health services and
a
https://orcid.org/0000-0003-4818-7620
b
https://orcid.org/0000-0002-7035-3835
c
https://orcid.org/0000-0002-8194-2467
d
https://orcid.org/0000-0003-4409-0506
e
https://orcid.org/0000-0002-1073-7116
f
https://orcid.org/0000-0003-0248-7783
g
https://orcid.org/0000-0002-3919-2738
with age is affected by more comorbidities,
interventions that can lead to an improvement of
quality of life that can turn into an increase in the
healthy life-expectancy (Södergren, 2013), which is
the years that a person lives free of disability (Jagger
& Robine, 2011). In return, the burden to the health
services is reduced as the onset of disability is delayed
(Beltrán-Sánchez et al., 2015; Mehta & Myrskylä,
2017), and reduced in a shorter span of time. It is
known that this can be modified by some factors such
as health habits, among others (Fried, 2000).
In this sense, different approaches have been
carried out in the last years to promote wellbeing and
ensure healthy lives for our elderly. Among them, the
most studied approach is probably the use of
recommender systems, which have proven to be
118
Torres, J., Garcia, M., Artola, G., Garcia-Navarro, T., Amaya, I., Larburu, N. and Martin, C.
Wellbeing Recommender System, a User-Centered Framework for Generating a Recommender System for Healthy Aging.
DOI: 10.5220/0011760600003476
In Proceedings of the 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2023), pages 118-125
ISBN: 978-989-758-645-3; ISSN: 2184-4984
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
useful for this purpose (Ceron-Rios et al., 2017),
being a well-functioning form of offering tailored
health interventions (Azmi et al., 2019b; Park et al.,
2012; Sezgin & Özkan, 2013). Although some of
these systems are already in use, they present several
limitations regarding i) the need of relevant validation
studies to demonstrate their usability (Azmi et al.,
2019a; Martinho et al., 2019), ii) interoperability and
the use of standards for communication with other
clinical platforms (Hors-Fraile et al., 2018), iii) the
need of continuously updating knowledge base
(Berner & Lande, 2016), or iv) user-based
personalization (Rist et al., 2018). In view of all this,
our approach attempts to address these limitations by
presenting an interoperable, technically validated,
and multidisciplinary tool that provides personalized
recommendations to elderly users. The system is
technically validated using stochastic, synthetic data,
which allows to assess the potential benefits of the
presented tool in the target population, the elderly.
This paper presents the methodology used for the
development of our Wellbeing Recommender System
(WRS) and the assessment of its potential to aid users,
describing its components and functionalities, and
showing the steps followed for its technical validation
with synthetic data. In addition, the results and
conclusions of the approach are also presented.
2 MATERIALS AND METHODS
In this section, the methodology followed for the
generation of the dataset used for the validation of the
WRS can be found (Section 2.1), the creation and
management of the recommendations is described
(Section 2.2.1), the data evaluation process by a rule
engine is detailed (Section 2.2.2), the modelling of the
data used by the platform is explained (Section 2.2.3)
and lastly the communication protocols and standards
of the platform are detailed (Section 2.2.4. All these
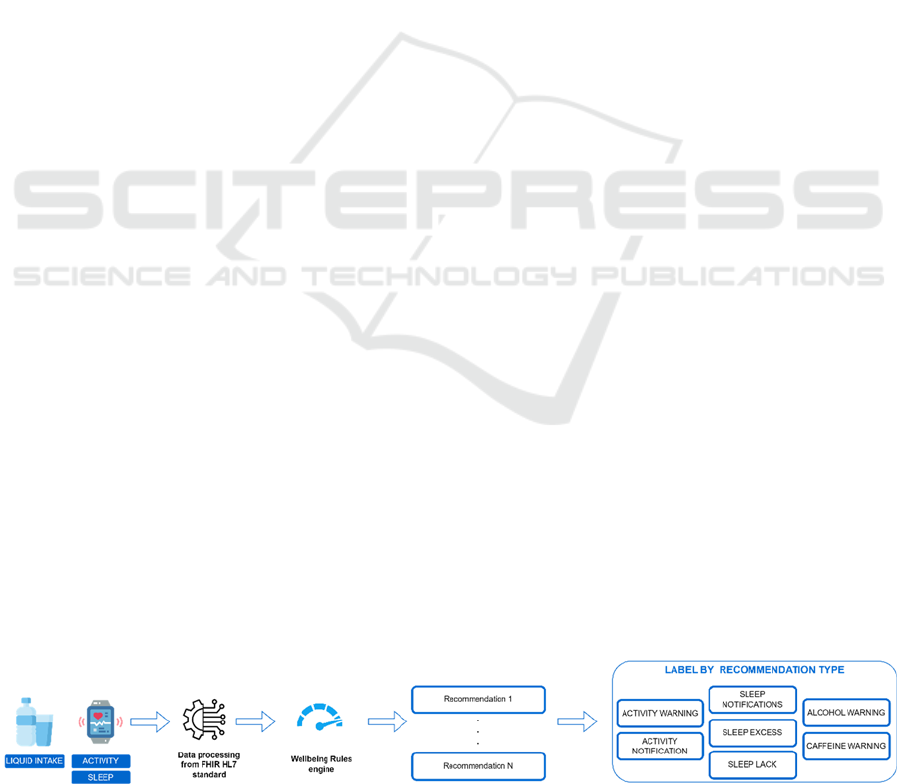
principal components and the general workflow of the
WRS are represented in the next Figure 1.
2.1 Synthetic Data Generation
In this study, we tested the WRS using a stochastic,
synthetic database named "Synthetic Database for
Recommendation System 2022 (SDRS2022)" which
simulates various user types. In subsection 2.1.1 the
methodology followed to define the categories of
users is explained, and in subsection 2.1.2 the
definition of the metrics and values that were
generated is described.
2.1.1 Elderly Population Characterization
The generated dataset simulates profiles of potential
users of the WRS. With the purpose of obtaining a
real representation of the future users, we based the
data generation on the population groupings defined
in the SHAPES project, whose aim is to build a large-
scale platform EU standardized open platform for
long-term active and healthy aging. Using the
personas method (Pérez-Montoro, 2017) eight
mutually exclusive types of personas were defined:
Active: older adults between 65-75 years old
with good health and an active lifestyle. They
can be either retired or still working and have
an active social life. Smoking, alcohol and
caffeine consumption are closely related
(Torres-Collado et al., 2018);
Chronic: older adults from 65 on that suffers
of multimorbid conditions such as diabetes and
oncological disease. Even though their
limitations, they try to maintain their autonomy
and active life (Arnautovska et al., 2018);
Musculoeskeletal: older adults that suffer
mobility difficulties. They have high risk of
falls and the fear of falling limits their daily life
activities. Sleep duration is associated with the
musculoskeletal pain (Lavigne et al., 2011).
They try to maintain their autonomy but there
is a risk of social isolation (Auais et al., 2018);
Neurodegenerative lonely elders with
memory decline, isolated from society and with
need of homecare (McCabe et al., 2014). Past
high alcohol consumption habits are related
with the prevalence of neurodegenerative
diseases (Kamal et al., 2020). Sleep patterns
become altered due to the neurodegenerative
process (Owen & Veasey, 2020);
Figure 1: Data execution workflow using the WRS.
Wellbeing Recommender System, a User-Centered Framework for Generating a Recommender System for Healthy Aging
119

Lonely: older adults socially isolated, with no
support that needs homecare assistance.
Through physical activity, they can reduce their
loneliness feeling (Pels & Kleinert, 2016),
which in turn is closely related to their sleep
quality(Jia & Yuan, 2020);
Drug dependency: older adults that have high
alcohol consumption habits. They have a high
percentage of hospitalizations and hospital
visits (Choi et al., 2015), and it is considered
that they can maintain a controlled autonomy.
Abuse of alcohol severely affects sleep
quality(Devenney et al., 2019);
Fragility: older adults over 85 years old with
high fragility suffering from falls, exhaustion
and weight loss (Scheibl et al., 2019) They are
highly dependent and need of a professional or
informal caregiver;
Deafblind: elders characterized by their
difficulties in socialising. They have a minimal
dependency condition (Bodsworth et al., 2011).
Due to their disability, can develop high
alcohol consumption habits (Fellinger et al.,
2012).
Not only were these categories defined, but also how
belonging to one of them influenced the metrics of the
study. For this, a research was done in the literature
to identify the variables and values needed to model
the categories, as detailed in the following subsection.
2.1.2 Metrics for Synthetic Users
To create stochastic, synthetic data, metrics were used
that represent the habits and lifestyle of the elderly
population. The criteria for these metrics were based
on literature related to physical activity, sleep, and
liquid intake. For physical activity, the elderly were
grouped into five age groups (65 to over 85 years old)
based on the difference in expected daily steps
(Tudor-Locke et al., 2013). For sleep data, the
literature suggests a decline in sleep duration with
aging (Faubel et al., 2009), and a range of less than 7
hours or more than 9 hours was used as a high-risk
symptom or alteration in sleep duration, respectively.
For liquid intake, the elderly tend to consume less
water as they age and in Europe, liquid intake is not
uniform due to differences in beverage categorization
(EFSA Panel on Dietetic Products, Nutrition, and
Allergies (NDA), 2010). The European Food Safety
Authority (EFSA) analyzed reports to create
reference values for liquid intake. The values were
used to make reference values for water, alcohol, and
caffeine-based beverages to monitor daily drinking
behavior and anticipate potential health problems
such as alcoholism and hypertension.
2.2 WRS Components
The WRS design is composed of the following
modules: (i) the wellbeing recommendations
manager to create and maintain the content of the
different recommendations that the system returns,
(ii) the wellbeing rule engine to generate the
personalized recommendations by evaluating user’s
data, (iii) a wellbeing ontology to keep the knowledge
representation homogeneous across the platform and
(iv) an interoperability module that transforms the
input/output data following clinical standard
communication protocols such as FHIR HL7 so that
the system can be integrated with other platforms. In
the next subsections, each component is described
more in detail.
2.2.1 Wellbeing Recommendations Manager
The recommendations included in the WRS are not
limited to a single domain; due to the possible use of
different sources that can be used to gather data, the
format used to store the recommendations in a digital
format is domain independent.
In this paper, the recommendations included are
divided into 3 groups, depending on the target that the
recommendations are associated with. These
categories are (i) liquid intake, (ii) physical activity
and (iii) sleep. For each one, specific
recommendations were defined based on agreed
criteria published and accepted in the literature (see
Section 2.1 for more details). Once identified, the
wellbeing recommendations were modelled into
several rules, which are the knowledge base used by
the rule engine described in subsection 2.2.2.
These rules are defined in a domain independent
format, so that the same representation format can be
re-used in different domains, not only the three
specified ones. Furthermore, the recommendations
can be returned in different languages, thus
broadening the potential user’s population that could
benefit from this solution. The generated
recommendations can be displayed to the end-users in
different devices (i.e., users’ phone, computer, etc),
as the communications to/from the WRS are managed
via a REST API. As a result, if an organization plans
to integrate a recommender system for its users,
employees, etc, it is possible by sending the data in a
HTTP request, as detailed in subsection 2.2.4, and
then visualize the answer as needed, either in a web,
or as notifications of a mobile application for
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
120

instance. Lastly, since recommendations may become
obsolete, or new recommendations may want to be
introduced into the system, a web-based rule
authoring tool (AT) was integrated to manage the
formalized content in a simple way by any user. This
tool was developed in (Torres et al., 2020), and was
used to first introduce the rules, and later edit them
when needed. This is a need that is critical for the
adoption of the system as the contents need to be
updated with new evidence otherwise they will
become outdated (Sim et al., 2001).
All the introduction of data was done using the
aforementioned tool, which in conjunction with the
ontology presented in subsection 2.2.3, eased the
introduction of the knowledge into the system, while
the reducing the possibility of input errors of human
origin. An example of the use of the AT for the
formalization of rules is shown in Figure 2, where the
definition of the conditions that conform are rule is
done using the interface of the AT. Individual
conditions or groups of conditions can be defined, as
well as the relation between them. In a similar way,
recommendations are introduced using the same
interfaces.
2.2.2 Wellbeing Rule Engine
The number of rules formalized in the WRS can grow
substantially over time as new content is added into
its knowledge base. As a result of it, a correct
management of the rules and its execution is crucial
to ensure the scalability of the system. As mentioned
before, the base of the WRS is the work presented in
(Torres et al., 2020), where a business rule engine
(Drools) is used to perform the mass execution of the
rules that conform the knowledge base.
Once users’ raw data is received, it is transformed
from the input FHIR message to internal JSON
instances. For liquid intake data, measurements an
aggregation by drink (i.e., water, beer, tea, juice, etc)
and by the type of the drink (alcoholic beverages,
carbonated drinks, caffeine beverages, etc). The use
of business rule engines allows the platform to
perform well, independently of the size of the
knowledge base, guaranteeing the scalability of our
system.
2.2.3 Data Model
The WRS system uses an ontology to keep its
knowledge base homogenous and easy to access for
new rule introduction. The ontology helps reduce
errors in representing the knowledge of the protocols
in rules and the information for both the conditions
and recommendations of the rules is modeled in it.
The ontology can be used by other solutions that need
the same data, as it can be accessed through a REST
API. Additionally, the information can be coded in
different languages to better fit the user's
sociolinguistic profile.
2.2.4 Interoperability
Interventions aiming to improve the habits of the
users can employ one or more component/platform to
support the patient during the intervention process.
As a result of this, the need to interchange data
between different systems becomes a necessary
feature that enhances the interoperability of the
developed platforms. In the present work, the issue of
interoperability was addressed adopting the FHIR
standard developed by HL7 for exchanging clinical
data between systems. All the interchanges of data,
both input and output requests, are done via FHIR
resources. These resources are processed by a parser
component that serializes/deserializes the data
between the FHIR and the internal formats used to
manage the users’ data.
Figure 2: Introduction of conditions using the integrated Authoring Tool.
Wellbeing Recommender System, a User-Centered Framework for Generating a Recommender System for Healthy Aging
121
Although the WRS is presented as a standalone
solution, it is designed to be capable of working in
conjunction with other components, as was the case
in the ecosystem of digital solutions developed under
the SHAPES project, where the interchange of
clinical data between the different components of the
ecosystem is done via, among others, FHIR
resources.
3 RESULTS AND DISCUSSION
With the profiles defined with the persona
methodology and the identified metrics described in
Section 2.1, a dataset of 100 subjects between 65 and
90 years of age has been created, with the following
characteristics (see Table 1).
Table 1: Statistical description of the used dataset.
Variable Mean and SD
Age (years) 78.24 ± 8.4
Gender (%)
53 (Female)
47
(
Male
)
Physical condition
14 (Active)
10 (Deafblind)
17 (Drug dependency)
12 (Musculoeskeletal)
10 (Lonely)
14 (Fragility)
16 (Chronic)
7
(
Neurode
g
enerative
)
Ste
p
s 4689.14 ± 8434.1
Sleep (hours) 6.08 ± 2.2
Water intake (ml) 1205.07 ± 1012.3
Alcohol intake (ml) 386.58 ± 195.3
Caffeine intake
(
ml
)
933.48 ± 358.5
The process of validation consisted of the
evaluation of the data by the WRS system for each
patient, the storage of the generated
recommendations, and lastly, an analysis of the
correlation between the different profiles of the
generated users and the type of the wellbeing
recommendations obtained.
As a result of the evaluation of the SDRS2022
dataset, a total of 523 recommendations were
obtained. This showed at first that the system was
capable of dealing with high amounts of data in a
reduced amount of time, but it was not easy to check
whether the recommendations obtained were related
with the different patient profiles. An aggregation of
the recommendations based on the profile of the user
that generated them was performed, grouping first the
recommendations belonging to each of the profiles
described in Section 2.1, followed by a categorization
of the rules depending on the nature of its
recommendation. The categorization was different
for each of the wellbeing recommendation categories.
In the case of the sleep recommendations, they were
grouped depending on the number of hours slept. If
the patient slept the recommended hours, it was
considered as a sleep notification, if it was not the
case, it was considered a warning, differentiating
between excess (sleep excess warning), and lack of
slept hours (sleep lack warning). A similar
categorization was done with the activity
recommendations, differentiating between
recommendations when the end-user reached
(activity_notification), and did not reach its daily step
goal (activity_warning). Lastly, in the liquid intake
case, the recommendations were grouped depending
on the class of drink, that is, recommendations
including alcoholic beverages were grouped under
alcohol warnings, and recommendations of
caffeine/theine-containing drinks such as coffee, tea
or carbonated drinks were grouped as caffeine
warnings. The obtained results regarding the
recommendation type and patient profile can be seen
in Figure 3.
The recommendations of the system reflected the
main characteristics of the user profiles, as the highest
amount of alcohol-related recommendations took
place in the Drug dependency category which also
presented over sleep disturbances and low physical
activity as described in Section 2.1. Similarly, the
Fragility users were not able to meet the daily step
target, which can be correlated with their frail
physical condition.
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
122
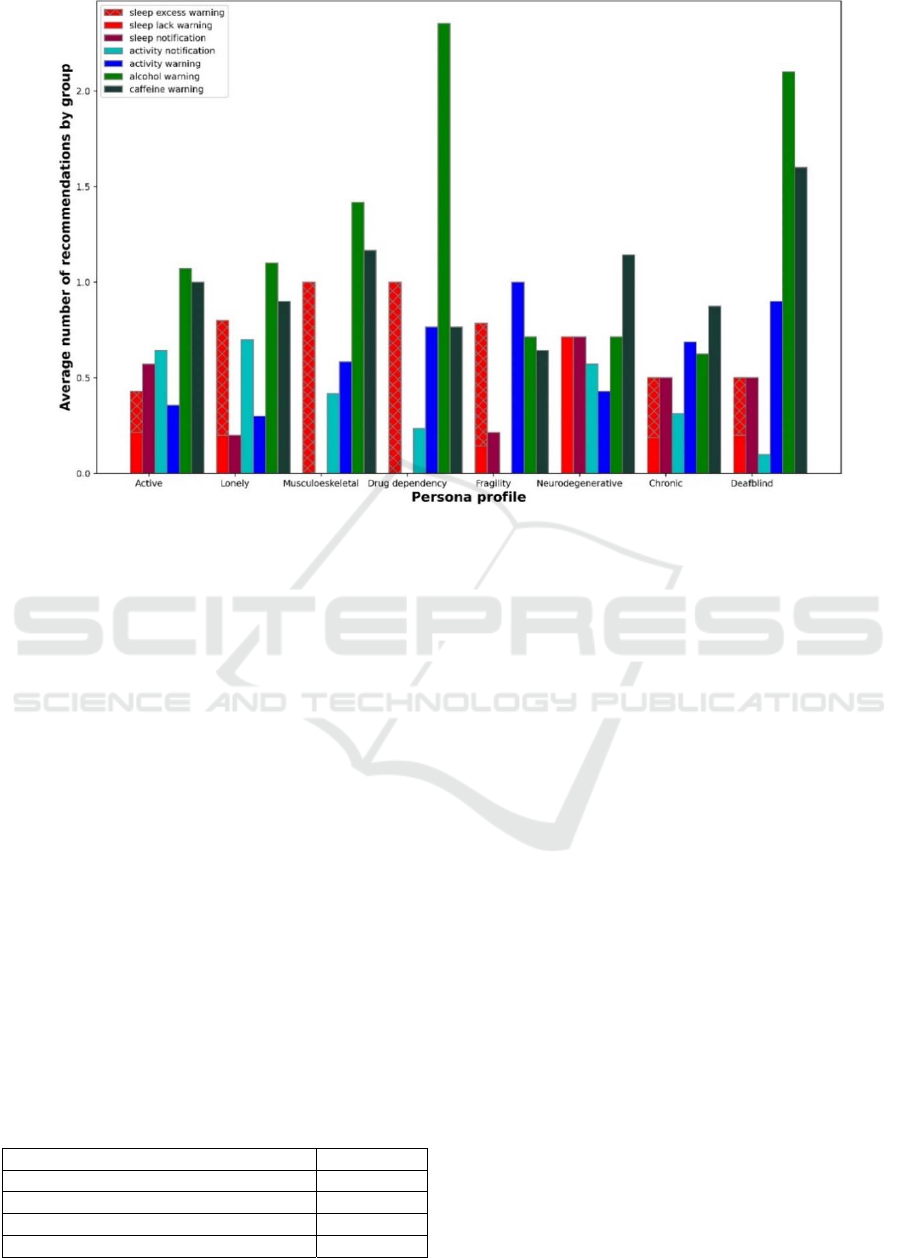
Figure 3: Average number of categorized recommendations grouped by user profile.
Other observed behaviours match Section 2.1.
Sleep disturbances are seen in the Neurodegenerative
group, high physical activity disturbances in Chronic,
and poor sleep quality in Lonely. Active,
Neurodegenerative, and Lonely groups had high
alcohol consumption. Chronic's low average
recommendations could be due to heterogeneity, and
similar recommendations for Active,
Neurodegenerative, and Lonely groups suggest a
need to improve profile modelling to prevent overlap.
Although results show that the recommendations
are in line with the habits described in Section 2.1, a
more real categorization of the patients can be done
by not limiting them to just one category, resulting in
a more accurate approximation of the WRS value.
The technical performance of the system was
evaluated by measuring the time it took to process the
SDRS2022 dataset (parse the FHIR observations,
evaluate data, and return the recommendations in
FHIR format). The evaluation was done using a PC
with 16GB of RAM and an Intel i5-9400F processor
and the results for 100 users are presented in Table 2.
Table 2: Technical characteristics of the evaluation process.
Users 100
Total observations 1500
Number of generated recommendations 523
Recommendations
/
use
r
5.23
Evaluation time (ms) 1.5
4 CONCLUSIONS
In this paper we present a rule-based recommender
system (WRS) capable of providing multidomain
wellbeing recommendations for the elderly
population. The aim of this system is to help users to
follow healthy lifestyle habits that will help them
improve their quality of life.
The WRS is integrated with a rule authoring tool
(AT) that allows for updating its knowledge base with
the latest evidence on wellbeing recommendations.
The system is designed to maintain consistency
across its knowledge base by incorporating an
ontology that defines the variables necessary for
defining wellbeing rules.
The system's value was assessed using a
synthetically generated dataset to i) test its
performance with high volumes of data and ii) ensure
proposed interventions matched various potential
end-users. Technical measurements showed the WRS
has no scalability issues as the entire evaluation of the
SDRS2022 dataset took less than two milliseconds,
including serialization/deserialization of FHIR
resources.
The potential impact of the formalized
recommendations was evaluated by analyzing the
triggered recommendations for each user profile. The
analysis showed that the formalized rules are useful
Wellbeing Recommender System, a User-Centered Framework for Generating a Recommender System for Healthy Aging
123

in providing information about users' habits.
However, the dataset used can be improved by not
limiting users to a single category and by improving
the methods of data generation to simulate more
realistic users.
Future research will develop a methodology to
analyze behavioral changes over time. The WRS
conforms to clinical standards, and new features can
be added easily to improve the impact on the end-
user’s life. The generation of synthetic data will also
be enhanced to simulate users' habits and enable
multi-category inclusion. This will allow to test the
methodology for detecting changes in behavior.
ACKNOWLEDGEMENTS
This project has received funding and clinical
professionals’ advice by gewi-Institut für
Gesundheitswirtschaft e.V. under the European
Union’s Horizon 2020 research and innovation
programme under Grant Agreement No 857159. The
funding sources had no involvement in the collection,
analysis and interpretation of data; in the writing of
the report; or in the decision to submit the article for
publication. The study complies with the current laws
of Spain and Europe. All authors declare that they
have no competing interests.
REFERENCES
Ahtonen, A. (2012). Healthy and active ageing. 4.
Arnautovska, U., O’Callaghan, F., & Hamilton, K. (2018).
Behaviour change techniques to facilitate physical
activity in older adults: What and how. Ageing and
Society, 38(12), 2590–2616.
Auais, M., French, S., Alvarado, B., Pirkle, C., Belanger,
E., & Guralnik, J. (2018). Fear of Falling Predicts
Incidence of Functional Disability 2 Years Later: A
Perspective From an International Cohort Study. The
Journals of Gerontology: Series A, 73(9), 1212–1215.
Azmi, A. K., Abdullah, N., & Emran, N. A. (2019a). A
Collaborative Filtering Recommender System Model
for Recommending Intervention to Improve Elderly
Well-being. International Journal of Advanced
Computer Science and Applications (IJACSA), 10(6),
Article 6.
Azmi, A. K., Abdullah, N., & Emran, N. A. (2019b). A
Recommender System Model for Improving Elderly
Well-Being: A Systematic Literature Review. 11, 22.
Beltrán-Sánchez, H., Soneji, S., & Crimmins, E. M. (2015).
Past, Present, and Future of Healthy Life Expectancy.
Cold Spring Harbor Perspectives in Medicine, 5(11),
a025957.
Berner, E. S., & Lande, T. J. L. (2016). Overview of
Clinical Decision Support Systems. In Clinical
Decision Support Systems (pp. 1–17). Springer, Cham.
Bodsworth, S. M., Clare, I. C. H., Simblett, S. K., &
Deafblind UK. (2011). Deafblindness and mental
health: Psychological distress and unmet need among
adults with dual sensory impairment. British Journal of
Visual Impairment, 29(1), 6–26.
Ceron-Rios, G. M., Lopez-Gutierrez, D. M., Dıaz-Agudo,
B., & Recio-Garcıa, J. A. (2017). Recommendation
System based on CBR algorithm for the Promotion of
Healthier Habits.
Choi, N., Marti, C., DiNitto, D., & Choi, B. (2015). Alcohol
Use as Risk Factors for Older Adults’ Emergency
Department Visits: A Latent Class Analysis. Western
Journal of Emergency Medicine, 16(7), 1146–1158.
Devenney, L. E., Coyle, K. B., Roth, T., & Verster, J. C.
(2019). Sleep after Heavy Alcohol Consumption and
Physical Activity Levels during Alcohol Hangover.
Journal of Clinical Medicine, 8(5), Article 5.
EFSA Panel on Dietetic Products, Nutrition, and Allergies
(NDA). (2010). Scientific Opinion on Dietary
Reference Values for water. EFSA Journal, 8(3).
Faubel, R., López-García, E., Guallar-Castillón, P.,
Graciani, A., Banegas, J. R., & Rodríguez-Artalejo, F.
(2009). Usual sleep duration and cognitive function in
older adults in Spain: Association between usual sleep
duration and cognitive function. Journal of Sleep
Research, 18(4), 427–435.
Fejer, R., & Ruhe, A. (2012). What is the prevalence of
musculoskeletal problems in the elderly population in
developed countries? A systematic critical literature
review. Chiropractic & Manual Therapies, 20(1), 31.
Fellinger, J., Holzinger, D., & Pollard, R. (2012). Mental
health of deaf people. Lancet (London, England),
379(9820), 1037–1044.
Fried, L. P. (2000). Health Promotion for Older Adults:
What Is the Potential? 26.
Goldman, D., Cutler, D., Rowe, J. W., Michaud, P.-C.,
Sullivan, J., Peneva, D., & Olshansky, S. J. (2013).
Substantial Health and Economic Returns From
Delayed Aging May Warrant a New Focus for Medical
Research. Health Affairs (Project Hope), 32(10), 1698–
1705.
Hors-Fraile, S., Rivera-Romero, O., Schneider, F.,
Fernandez-Luque, L., Luna-Perejon, F., Civit-Balcells,
A., & de Vries, H. (2018). Analyzing recommender
systems for health promotion using a multidisciplinary
taxonomy: A scoping review. International Journal of
Medical Informatics, 114, 143–155.
Jagger, C., & Robine, J.-M. (2011). Healthy Life
Expectancy. In R. G. Rogers & E. M. Crimmins (Eds.),
International Handbook of Adult Mortality (pp. 551–
568). Springer Netherlands.
Jia, G., & Yuan, P. (2020). The association between sleep
quality and loneliness in rural older individuals: A
cross-sectional study in Shandong Province, China.
BMC Geriatrics, 20(1), 180.
Kamal, H., Tan, G. C., Ibrahim, S. F., Shaikh, Mohd. F.,
Mohamed, I. N., Mohamed, R. M. P., Hamid, A. A.,
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
124

Ugusman, A., & Kumar, J. (2020). Alcohol Use
Disorder, Neurodegeneration, Alzheimer’s and
Parkinson’s Disease: Interplay Between Oxidative
Stress, Neuroimmune Response and Excitotoxicity.
Frontiers in Cellular Neuroscience, 14.
Lavigne, G. J., Nashed, A., Manzini, C., & Carra, M. C.
(2011). Does sleep differ among patients with common
musculoskeletal pain disorders? Current Rheumatology
Reports, 13(6), 535–542.
Martinho, D., Carneiro, J., Novais, P., Neves, J., Corchado,
J., & Marreiros, G. (2019). A Conceptual Approach to
Enhance the Well-Being of Elderly People. In P. Moura
Oliveira, P. Novais, & L. P. Reis (Eds.), Progress in
Artificial Intelligence (pp. 50–61). Springer
International Publishing.
McCabe, C., Dinsmore, J., Brady, A. M., Mckee, G.,
O’Donnell, S., & Prendergast, D. (2014). Using Action
Research and Peer Perspectives to Develop Technology
That Facilitates Behavioral Change and Self-
Management in COPD. International Journal of
Telemedicine and Applications, 2014, 1–10.
Mehta, N., & Myrskylä, M. (2017). The Population Health
Benefits Of A Healthy Lifestyle: Life Expectancy
Increased And Onset Of Disability Delayed. Health
Affairs, 36(8), 1495–1502.
Owen, J. E., & Veasey, S. C. (2020). Impact of sleep
disturbances on neurodegeneration: Insight from
studies in animal models. Neurobiology of Disease,
139, 104820.
Park, D. H., Kim, H. K., Choi, I. Y., & Kim, J. K. (2012).
A literature review and classification of recommender
systems research. Expert Systems with Applications,
39(11), 10059–10072.
Pels, F., & Kleinert, J. (2016). Loneliness and physical
activity: A systematic review. International Review of
Sport and Exercise Psychology, 9(1), 231–260.
Pérez-Montoro, M. (2017). Navigation design and SEO for
content-intensive websites: A guide for an efficient
digital communication. Elsevier.
Rist, T., Seiderer, A., & André, E. (2018). Providing Life-
Style-Intervention to Improve Well-Being of Elderly
People. In E. Clua, L. Roque, A. Lugmayr, & P. Tuomi
(Eds.), Entertainment Computing – ICEC 2018 (pp.
362–367). Springer International Publishing.
Scheibl, F., Farquhar, M., Buck, J., Barclay, S., Brayne, C.,
& Fleming, J. (2019). When Frail Older People
Relocate in Very Old Age, Who Makes the Decision?
Innovation in Aging, 3(4), igz030.
Sezgin, E., & Özkan, S. (2013). A systematic literature
review on Health Recommender Systems. 2013 E-
Health and Bioengineering Conference (EHB), 1–4.
Sim, I., Gorman, P., Greenes, R. A., Haynes, R. B., Kaplan,
B., Lehmann, H., & Tang, P. C. (2001). Clinical
Decision Support Systems for the Practice of Evidence-
based Medicine. Journal of the American Medical
Informatics Association
, 8(6), 527–534.
Södergren, M. (2013). Lifestyle predictors of healthy
ageing in men. Maturitas, 75(2), 113–117.
Torres, J., Artola, G., & Muro, N. (2020). A Domain-
Independent Semantically Validated Authoring Tool
for Formalizing Clinical Practice Guidelines. Studies in
Health Technology and Informatics, 270, 517–521.
Torres-Collado, L., García-de la Hera, M., Navarrete-
Muñoz, E. M., Compañ-Gabucio, L. M., Gonzalez-
Palacios, S., & Vioque, J. (2018). Coffee Drinking and
Associated Factors in an Elderly Population in Spain.
International Journal of Environmental Research and
Public Health, 15(8), Article 8.
Tudor-Locke, C., Schuna, J. M., Barreira, T. V., Mire, E.
F., Broyles, S. T., Katzmarzyk, P. T., & Johnson, W. D.
(2013). Normative Steps/Day Values for Older Adults:
NHANES 2005-2006. The Journals of Gerontology
Series A: Biological Sciences and Medical Sciences,
68(11), 1426–1432.
Wellbeing Recommender System, a User-Centered Framework for Generating a Recommender System for Healthy Aging
125
