
A Methodology Based on Quality Gates for Certifiable AI in Medicine:
Towards a Reliable Application of Metrics in Machine Learning
Miriam Elia
a
and Bernhard Bauer
b
Faculty of Applied Computer Science, University of Augsburg, Germany
(miriam.elia, bernhard.bauer)@informatik.uni-augsburg.de
Keywords:
Certifiable AI, Quality Management, Machine Learning, Healthcare, Metrics, Deep Learning, Performance
Evaluation, Algorithm Auditing.
Abstract:
As of now, intelligent technologies experience a rapid growth. For a reliable adoption of those new and
powerful systems into day-to-day life, especially with respect to high-risk settings such as medicine, technical
means to realize legal requirements correctly, are indispensible. Our proposed methodology comprises an
approach to translate such partly more abstract concepts into concrete instructions - it is based on Quality
Gates along the intelligent system’s complete life cycle, which are composed of use-case adapted Criteria
that need to be addressed with respect to certification. Also, the underlying philosophy regarding stakeholder
inclusion, domain embedding and risk analysis is illustrated. In the present paper, the Quality Gate Metrics is
outlined for the application of machine learning performance metrics focused on binary classification.
1 INTRODUCTION
Thanks to astonishing results, the adoption of AI in
medicine is moving more and more into the center of
attention. Many requirements for a conscious integra-
tion of the new technology, especially regarding high-
risk contexts, have been published. Recently, the EU
released its AI Act that stands as a legislative guide-
line (European Commission, 2021). However, tech-
nical means to realize these requirements in medicine
are yet to be developed and standardized. In addi-
tion, ”[t]he healthcare application field introduces re-
quirements and potential pitfalls that are not imme-
diately obvious from the ’general data science’ view-
point” (Jussi, 2021, 1). Challenges regarding the de-
sired adoption of this complex technology into clini-
cal day-to-day life are partly based on the necessity of
comprehensive Machine Learning (ML) knowledge
to accurately evaluate the system. The present work
is part of our approach towards a generic and cus-
tomizable methodology - introduced in this paper and
based on Quality Gates (QG) - that comprises exist-
ing research on the development of ML models for
Certifiable AI in Medicine into guidelines for devel-
opers and auditing offices, while paying special atten-
tion to end-user perspectives, the inclusion of domain
a
https://orcid.org/0000-0001-6253-230X
b
https://orcid.org/0000-0002-7931-1105
knowledge and risk analysis. The focus lies on defin-
ing general guidelines towards metrics selection for a
comprehensive evaluation of the ML model, adapted
to the respective medical context. Section 2 explains
the current legal situation regarding intelligent medi-
cal devices with respect to software quality manage-
ment and metrics for ML in healthcare. In section
3, our methodology’s basic concepts are introduced,
while section 4 specializes on the QG Metrics and
presents guidelines for a reliable selection, adapted
to the medical context. Finally, section 5 summarizes
the present work and derives open research questions.
2 RELATED WORK
Functional & Safety Standards: Since 2021, an
updated version of the Medical Device Regulation
(MDR) is in place that guarantees the Conformit
´
e Eu-
rop
´
eenne (CE), i.e. conformity with ”[...] EU safety,
health and environmental protection requirements, as
well as with norms set by the International Orga-
nization for Standardization (ISO)” (Ben-Menahem,
2020, 1). ISO does not perform certification activities
itself, but provides internationally accepted norms, as
DIN EN ISO 9001:2015-11 for process-oriented qual-
ity management systems, or ISO 13485 for medical
devices, for instance. Another important concept is
safety, i.e. protecting the user from potentially harm-
486
Elia, M. and Bauer, B.
A Methodology Based on Quality Gates for Certifiable AI in Medicine: Towards a Reliable Application of Metrics in Machine Learning.
DOI: 10.5220/0012121300003538
In Proceedings of the 18th International Conference on Software Technologies (ICSOFT 2023), pages 486-493
ISBN: 978-989-758-665-1; ISSN: 2184-2833
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

ful behavior of the software. Functional requirements
are summarized under IEC 61508, while DIN EN
IEC 60601 and DIN EN IEC 62304 specifically fo-
cus on medical devices. Moreover, Safety Integrity
Levels 0 − 4 (SIL), i.e. ”[...] classification levels
indicating safety requirements in safety-critical sys-
tems”(Papadopoulos, 2010, 1) are assigned.
Certification & Medical AI: As of now, the EU
AI Act is on everyone’s mind, aiming to form the
”[...] legislation for a coordinated European approach
on the human and ethical implications of AI” (Eu-
ropean Commission, 2021, 2). This document de-
fines the foundation of AI-based devices in the EU, its
philosophy is summarized in (European Commission,
2020), and discussed in further detail with respect to
medicine in (Schneeberger, 2020). Currently, the cer-
tification process for high-risk medical devices is con-
ducted by an independent authority, i.e. notified bod-
ies. (Ben-Menahem, 2020, 1-3) However, currently,
they are not equipped to implement all incoming de-
mands, which could lead to a scarcity of medical de-
vices in the EU (European Commission, 2023, 2-4).
For a comprehensive impact analysis regarding the
new MDR regulations for risk classes, clinical eval-
uation, post-market surveillance and notified bodies,
refer to (Niemiec, 2022). Current challenges for AI
in healthcare are mainly centered around black box
models that are able to perform complex tasks, but
whose inner workings are incomprehensible for hu-
man stakeholders. This could lead to an incorrect ap-
plication of developed models in the clinical context,
”[...] due to methodological flaws and/or underlying
biases” (Roberts, 2021, 1), for instance. In (Muller,
2021) generally applicable principles regarding AI in
medicine that could form a solid baseline for technical
design decisions, are summarized.
Quality Gates & Metrics: A QG is a concept derived
from software quality management, and could be de-
fined as ”[...] an objective quality assurance gate,
that is, a verification procedure, performed either
by independent reviewers or by automated scripts”
(Paula F., 2006, 34). Their most basic function-
ing consists of summarizing important criteria regard-
ing specific outcomes that are generated at differ-
ent points during the software development life cycle
(Flohr, 2008, 245). A means of defining criteria for
virtual QGs for manufacturing use cases is presented
in (Filz, 2020, 8ff), but could be adapted to medi-
cal contents, since they are based on the inclusion
of domain knowledge. A thorough and comprehen-
sive understanding of the respectively conveyed infor-
mation is indispensable for ML performance metrics
interpretation, especially in medicine, but not nec-
essarily guaranteed (Hicks, 2022, 1). For instance,
a very common metric for classification tasks is the
Receiver Operating Characteristic Area under the
Curve (ROC AUC). It is used as primary evaluation
metric in popular bench marking tools hosted e.g. on
Grand-challenge.org, like the STOIC
1
challenge for
3D computer tomography classification of COVID-19
infected lungs (Boulogne, 2023), for instance. Their
metrics selection is based on (Reinke, 2021), accord-
ing to which ROC AUC and its prominent opposition
Precision-Recall AUC (PR AUC) both reflect data im-
balance (Reinke, 2021, 43ff.). However, there is an
ongoing discussion whether or not ROC AUC reflects
imbalanced data sets, which is a very common case
in medicine (Davis, 2006; Saito, 2015). Also, pub-
lished paper and bench-marking tools tend to display
disagreement regarding the consistent application of
both metrics for an empirical analysis (Ribeiro, 2020;
Strodthoff, 2020). This inconsistency enforces the ne-
cessity to standardize valid approaches.
3 METHODOLOGY BASED ON
QUALITY GATES
Our proposed methodology’s main objective is to
”make auditing simple”, and thus provide concrete in-
structions for the domain-adapted realization of spe-
cific legislative requirements in the context of Certifi-
able AI in medicine, while respecting different stake-
holder’s needs and specific design decisions’ risks. In
the long term, such findings could be adapted in a
(partially) automated manner to the complete appli-
cation’s life cycle through adapted frameworks and
templates for a comprehensive documentation of de-
sign decisions. In general, the conceptual foundation
is based on the definition of scientifically substanti-
ated Criteria for QGs along the complete life cycle of
the intelligent software. To the best of our knowledge,
a similar adaptation of QGs and ML-certification in
healthcare has not yet been published. Attributed
to the variety of different ML methods for different
medicinal use cases that compose of different data
types and tuning objectives, the concrete realization
of Criteria should be adapted respectively. Struc-
tural similarities from a technical viewpoint between
use cases should suffice to generalize applied meth-
ods, as in (Strodthoff, 2020, 3) where metrics from
multi-label protein discovery were adapted to ECG-
classification.
General Structure of Quality Gates: In figure 1 the
high-level QG’s hierarchy adapted to ML-processes
is depicted: QG Data ensures a clean and informa-
1
https://stoic2021.grand-challenge.org/
A Methodology Based on Quality Gates for Certifiable AI in Medicine: Towards a Reliable Application of Metrics in Machine Learning
487
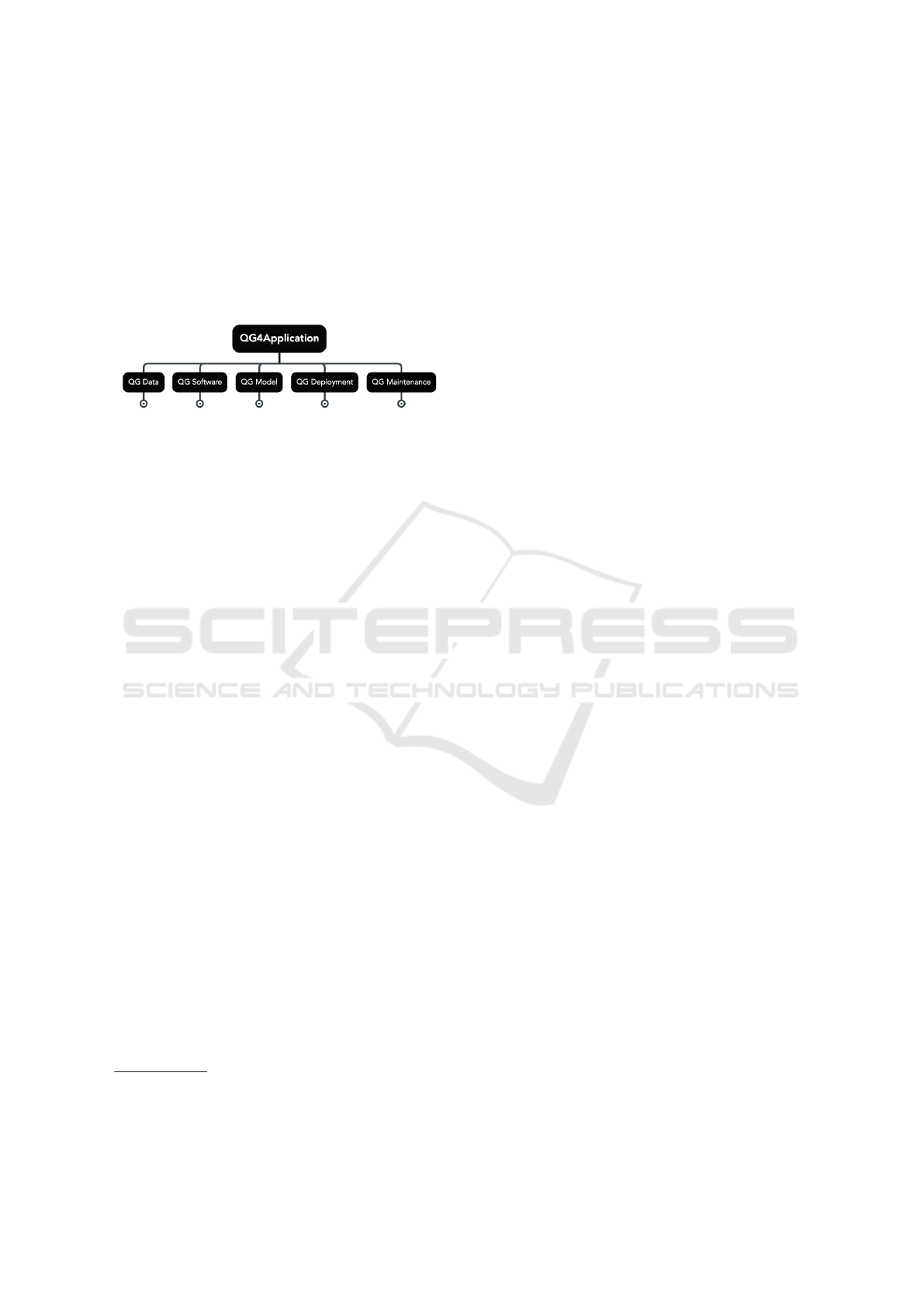
tive data set that is ready for model training, QG Soft-
ware guarantees overall compliance with software en-
gineering requirements, QG Model delivers a trans-
parent algorithm that has been thoroughly assessed,
QG Deployment assures a seamless rollout, while
QG Maintenance ensures regular monitoring, which
could include physician training in the medical sec-
tor Only in combination, the whole QG4Application
is evaluated.
2
Figure 1: High-Level Quality Gates.
The process-steps depicted in figure 1 represent
basic ML-development and should be audited for all
levels of risk regarding intelligent applications, refer
to (Koshiyama, 2021, 3), where five similar stages of
development are defined for ML algorithm auditing in
general, or (Oala, 2021, 2) where the authors present
a concept for healthcare-specific algorithm auditing.
3.1 Basic Concepts
The following definitions comprise our presented
methodology’s conceptual foundation, and are partly
derived from traditional software quality assessment.
In (Koshiyama, 2021), the authors propose Explain-
ability, Robustness, Fairness, and Privacy as audit-
ing verticals, which form an important component of
Algorithm Audit research (Koshiyama, 2021, 2-3).
Our ”auditing verticals” are intended as guidelines of
thought when defining QG Criteria that should have
been analyzed by the responsible party for the respec-
tive process step(s). Within our context, fundamen-
tal requirements for trustworthy, and thus certifiable
AI, such as fairness, privacy, and robustness (Euro-
pean Commission, 2020), are addressed via a pro-
found Risk Analysis.
Quality Gate: Significant milestone or decision point
during the creation of a ML-based software that, in
a body, serve as a quality guideline to assess the
software‘s compliance with EU-legislation regarding
Certifiable AI in medicine. Project-specific Criteria
are evaluated against pre-defined desired Criteria for
the particular use case. Based on the degree of their
fulfilment, Gatekeepers decide the project’s level of
compliance, which might lead to re-working some
2
Our proposed methodology focuses on the ML part of
the complete medical device, thus, Software Engineering-
specific information is only mentioned marginally.
QGs. QGs might be optional or weighted differently
regarding their impact. (Flohr, 2008)
Scope: Each QG has access to specific project-based
resources or outcomes that are measured by the re-
spective Gatekeeper. Its Scope includes other QG’s
outcomes. QGs are arranged in a tree-structure, with
growing Scope from more project-specific leaf-QGs
to more abstract root-QGs. The highest level of Scope
covers QGs for Data, Software and Model Develop-
ment, as well as Application Deployment and Mainte-
nance.
Criteria: Basis for QG-evaluation by the Gatekeeper.
Concrete and use case specific requirements with
growing level of abstractness following the Scope
from leaf to root. Should be adapted to the specific
use case if necessary. (Flohr, 2008)
Gatekeeper: Measures the fulfillment of each QG re-
garding its decision Scope depending on the point in
time of the application life cycle. It compares pre-
defined, desired Criteria with the actual project’s out-
comes and decides to what extend the system is in
compliance. (Flohr, 2008)
Scoring System: It comprises multiple indexes, with
the Compliance Index as central part, i.e. the ”main
index” that comprises the complete application’s eval-
uation in a single number. Its calculation comprises
other indexes and the Gatekeeper’s results. For in-
stance, QG Data could be evaluated as stand-alone or
embedded within the application’s assessment.
Explainability: Since XAI has become a very popu-
lar field of research, its inclusion during the ML-based
application’s life cycle is addressed separately: we
follow a similar philosophy, as in (European Commis-
sion, 2020), where XAI contributes to the requirement
Transparency, through providing a pool of methods,
that help to ”[...] explain both the technical processes
of the AI system and the reasoning behind the deci-
sions or predictions that the AI system makes” (Eu-
ropean Commission, 2020, 14). Thus, depending on
the respective process step, the application of XAI
can have various forms and objectives in support of
realizing other Criteria, rather than being the cen-
ter of an evaluation: a developer might use LIME to
assess the model’s performance regarding learnt fea-
tures (Ribeiro, 2016) to achieve robustness, while a
physician requires a humanly readable explanation.
3.2 Quality Gates in the Application’s
Life Cycle
Following ISO guidelines, the aforementioned high-
level QGs are illustrated as processes during the soft-
ware’s life cycle in figure 2: Data Management and
all its sub processes, followed by Model Develop-
ICSOFT 2023 - 18th International Conference on Software Technologies
488

ment and Software Engineering, and is concluded
with the Application’s Deployment, and Maintenance
in the real world. Our suggested methodology aims
to assist development teams in form of the inclu-
sion of Domain Knowledge, or communication of
QG Inter-Dependencies based on previous/following
QG outcomes during the application’s life cycle with
the objective to design the application in a way that
Stakeholder’s needs are fulfilled and possible Risks
mitigated. Also, the auditor will find scientifically
grounded guidelines for ML quality assessment tai-
lored to specific groups of medical use cases thanks
to our methodology’s customizability.
Figure 2: Quality Gates during the ML Life Cycle.
Regarding our proposed methodology’s applica-
tion, it should be considered, that ”[a]lthough these
stages appear static and self-containing, in practice
they interact in a dynamic fashion, not following a lin-
ear progression but a series of loops [...]”(Koshiyama,
2021, 3). This may include multiple iterations of the
presented processes, starting during development and
before certification, while continuing afterwards. For
auditing, only a static version of a particular model
with its respective data can be assessed, and each
modification or re-training automatically requires a
new audit
3
.
3.2.1 Overall Guidelines
Generally, we defined four guidelines as necessary
lines of thought for the definition of QG-Criteria,
with the objective to unify common ML-concepts in
support of different stakeholders involved during the
ML-based software’s life cycle. Thus, regarding ML
for medicine, special focus is placed on the inclusion
of Stakeholders, while paying special attention to a
thorough impact Risk Analysis in the real world. Also
benefits of the inclusion of Domain Knowledge are
evaluated, and Inter-Dependencies regarding differ-
ent QGs’ outcomes considered.
Stakeholder: Considering all Stakeholder needs
from a technical point of view enhances the imple-
mentation of a successful application that fulfills its
3
For instance, mirroring the Digital Twin concept from
the industry, a static Real-World Twin could be deployed in
the application and dynamically updated, while its twin is
continuously optimized, including new data.
intended purpose. The most obvious include Devel-
oper and Domain Experts from a medical background
who participate in the software’s development, the
Auditor who is responsible to ensure product compli-
ance with legislation, and finally the User, i.e. medic-
inal personnel and patients, who will one day work
with the system. Thus, interdisciplinary teams are ad-
vised to be considered standard during the complete
development process.
Risk Analysis: The application-wide Risk Analysis
is realized by the mapping of conducted analysis with
differing and specific aims into indexes. Examples in-
clude uncertainty estimation, fairness, privacy, trans-
parency, robustness and sustainability.
Inter-Dependency: This guideline is methodology-
specific and refers to communicating result-based rec-
ommendations between QGs. An example for an
Inter-QG-Dependency is the recommendation of ad-
equate metrics based on the QG Data’s analysis and
clinical objective of the project, or the effects of QG
Pesudo- /Anonymization on included meta data as ad-
ditional features.
Domain Knowledge: Especially in medicine, the in-
clusion of domain- and use case-specific knowledge
is indispensable for efficiently training and accurately
evaluating the ML-model, since AI-based software
for healthcare is primarily designed to enhance clini-
cal treatment and patient care. Thus, the inclusion of
use-case specific domain knowledge should be con-
sidered, when designing Criteria for leaf-QGs.
3.2.2 Data
The proposed QG Data comprises the processes
Source Selection, General Preparation, and ML
Preparation, and is illustrated in figure 3. When
defining the data set composition, a high distribution
in data sources is desired, in favor of the algorithm’s
quality. Further, raw data needs to be analyzed, e.g.
with respect to data type, and possibly collected meta
data, as well as cleaned from missing values or er-
rors. Then, especially in healthcare, data pseudo- or
anonymization is likely to be required. In a final step,
since the data is intended to serve as basis for training
a ML algorithm, samples need to be annotated cor-
rectly, as well as the resulting label and feature distri-
butions analyzed.
Figure 3: Quality Gates for Data Set Generation.
Bias: Biased data sets propagate their inherent distri-
butions through model training into the application’s
A Methodology Based on Quality Gates for Certifiable AI in Medicine: Towards a Reliable Application of Metrics in Machine Learning
489
real world context, which could lead to incorrect and
unfair predictions. Thus, the implementation of mea-
surements to detect and reduce bias is important for
the assessment of the Fairness requirement (Euro-
pean Commission, 2020, 6). Bias analysis is relevant
for multiple process steps, especially for QG Data and
QG Model, but also in retrospect during QG Deploy-
ment and QG Maintenance. Within our methodology,
such methods are summarized in form of a Bias Index
for Risk Analysis. Other interesting, and promising ar-
eas of research that are potentially interesting for ML
data set preparation in medicine include synthetic data
and multi-modal approaches (MacEachern, 2021).
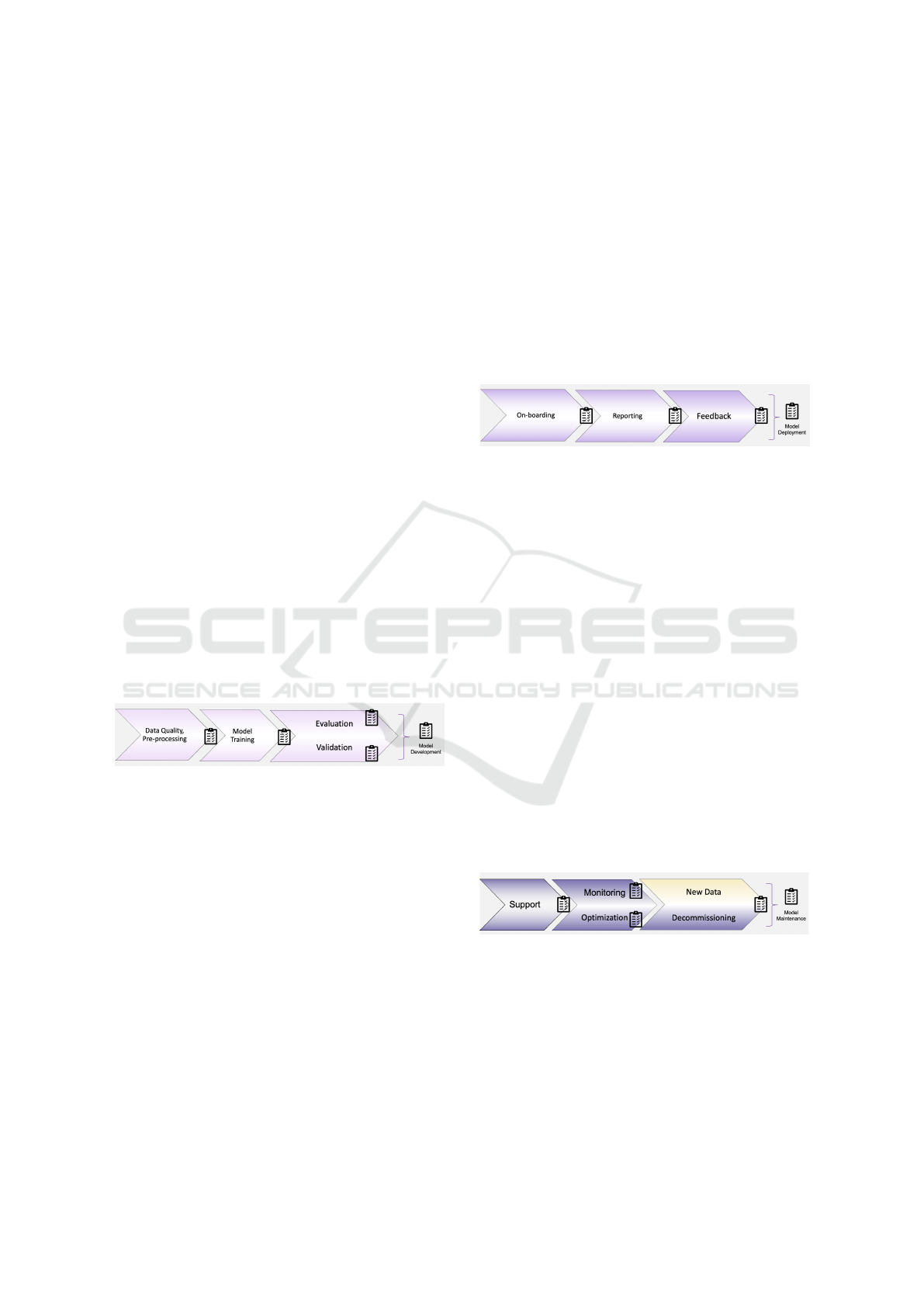
3.2.3 Model
The presented QG Model is divided into four sub
processes, Data Quality and Pre-processing, Model
Training, Evaluation, and Validation, as depicted in
figure 4. Depending on design decisions regarding the
model’s architecture or training objectives, different
pre-processing steps should be considered and eval-
uated against domain-specific requirements. During
model training, optimized hyper-parameters are cal-
culated, and different architectures compared on train
and validation set, while considering data set specific
information from the previous QG Data, like class
imbalance, for instance. The final test set is applied
for evaluating the algorithm’s generalization perfor-
mance by means of domain-embedded and meaning-
fully interpreted metrics.
Figure 4: Quality Gates during Model Development.
The extent to which this mostly development-
specific information is relevant to present a compre-
hensive view of the model’s behavior for auditing is
yet to be defined. However, information included for
QG Validation like XAI methods that could help to
evaluate the model from a different viewpoint, by un-
covering wrong patterns learnt or to test the model’s
robustness through adversarial analysis, for instance
(Ribeiro, 2016), are important information to assess
the system’s overall performance.
3.2.4 Deployment
Other important steps during the application’s life cy-
cle, are its deployment and maintenance in the real
world. Regarding healthcare-specific requirements
however, in our proposed methodology those two
inter-related processes are regarded separately. QG
Deployment is divided into three sub processes On-
boarding, Reporting and Feedback, as illustrated in
figure 5. Especially in a clinical setting, a close co-
operation between the human user, and the intelli-
gent system is evident, which requires a thorough
on-boarding phase to support a conscious utilization
of the ML-based device. For instance, an appropri-
ate XAI-method could be integrated to analyze model
predictions from an additional perspective, but whose
interpretation might need further explanations to be
humanly interpretable. Refer to (Henry, 2022) for an
analysis of physician and intelligent system coopera-
tion.
Figure 5: Quality Gates for Deployment.
A valid approach towards achieving a conscious
application is educating medical personnel about AI’s
benefits and risks, as well as necessary basic ML
knowledge, depending on their respective degree of
interest, i.e. only application or also development of
such systems. Other important considerations for this
phase include approaches on monitoring the model’s
behavior in the real world, as well as concepts to
transmit and integrate user feedback.
3.2.5 Maintenance
The outlined QG Maintenance is divided into four sub
processes, Support, Monitoring, Optimization, and
Decommissioning or New Data, as depicted in figure
6. This phase is closely related to the previously de-
fined QG Deployment, and partly continues relevant
processes. Besides offering user support and train-
ing as necessary, as well as repeatedly monitoring the
model’s real-world performance, algorithm optimiza-
tion is another important process that should be pur-
sued in parallel, while optionally including new data.
Figure 6: Quality Gates during Maintenance.
These steps are repeated until the application’s de-
commissioning, which should be organized in detail
to assure a smooth continuation in the respective real-
world setting. The intended tendency is to closely ob-
serve the model after its first deployment, and contin-
uously re-assess, but with an increasing distance be-
tween iterations, in alignment with MDR regulations
(Ben-Menahem, 2020, 3).
ICSOFT 2023 - 18th International Conference on Software Technologies
490

4 QUALITY GATE: METRICS
For a reliable model training and performance eval-
uation within its application context, adequate met-
rics need to be selected, since their interpretation is
not comparable for different tasks with varying ob-
jectives and data distributions (Strodthoff, 2020, 6).
QG Metrics is also relevant after deployment, for
maintenance, and to measure clinical success. These
multiple points of reference for QG Metrics require
a thorough documentation of all relevant decisions,
their interpretation should be domain-embedded and
translated for multiple stakeholders, at best from early
development on. However, its results are to be in-
terpreted in combination with Indexes relevant for
Risk Analysis. This section first introduces a gen-
eral overview of machine learning metrics for the
most common binary classification problems, refer
to (M
¨
uller, 2022) for metrics in image segmentation.
In a next step, healthcare-specific challenges that af-
fect metrics interpretation are highlighted. Finally,
solid guidelines for a reliable definition of Criteria
for QG Metrics in the broader picture of certifiable AI
in medicine are outlined, while addressing domain-
specific challenges.
4.1 Metrics for Healthcare
In general, a combination of metrics is necessary for
a comprehensive view on the model’s performance
- no single metric reflects on all desired capabili-
ties (Kelly, 2019, 3). Thus, preliminary material dis-
playing the model’s prediction versus true labels for
instance, could provide necessary insights to better
evaluate the model, for reasonable prediction thresh-
olds, and to enhance the global understanding of ap-
plied performance metrics. Regarding metrics as a
body, two foundational perspectives could be defined
to evaluate model performance depending on the ac-
cessible artifacts. Another perspective on ML evalu-
ation that is not part of this research comprises statis-
tical analysis of the model’s architecture and its com-
ponents, as in (Martin, 2021).
Classification: Following this strategy, the model’s
performance on different classes is measured based
on the confusion matrix (Jussi, 2021, 5). Further, this
approach is based on Thresholding to categorize pre-
dictions in either true or false. Their applicability,
including the most widely used ones such as Accu-
racy
4
, Recall, Specificity, Precision or F1-score, as
well as common pitfalls regarding incorrect perfor-
4
Accuracy is a poor measure for imbalanced data sets,
and should be replaced by Balanced Accuracy (Jussi, 2021,
5-7).
mance measuring in current research, has been thor-
oughly studied in (Hicks, 2022).
Ranking: The Ranking-perspective is based on the
real valued function learned by the model that returns
its confidence, thus accessing the model is necessary.
Further, this approach is a threshold-independent per-
formance measurement, includes metrics like ROC
AUC (Zhang, 2014, 1822), and could also be referred
to for threshold optimization.
4.2 Guidelines for Metrics Application
As a general rule, each selected metric should be ac-
companied by Additional Material that exactly docu-
ments its interpretation within the real-world medical
context, since measuring clinical efficacy is not trivial
(Kelly, 2019, 3). For this purpose, a comprehensive
understanding of the underlying data is indispensable,
as these represent the link to reality. However, clinical
data usually is distributed, heterogeneous and high-
dimensional, and multiple sources might first need to
be fused following some medical reasoning to rep-
resent meaningful input for the ML model (Muller,
2021, 120), which can be an elaborate process. Thus,
”[t]he development of quality recommendations and
standards for training data sets has to be a community-
driven effort of many diverse stakeholders” (Muller,
2021, 120), since high-quality data sets play a crucial
factor regarding model performance.
Standards: Some metrics are not symmetric, i.e. the
definition which class is positive 1 or negative 0 im-
pacts their outcome and is not interchangeable (Hicks,
2022, 3). A standardized definition marking the dis-
ease as the positive class, while healthy samples are
defined as the negative class is reasonable for bi-
nary classification in healthcare, as proposed in (Jussi,
2021, 9) for instance. Also, the inconsistency regard-
ing metrics selection in general should be addressed
by defining a standardized metrics collection for au-
diting different ML use cases, like e.g. image clas-
sification, in addition to ”[p]eer-reviewed randomised
controlled trials as an evidence gold standard” (Kelly,
2019, 2f.) that accurately measure possible risks and
clinical success. The need for further standardization
is becoming more prevalent with respect to auditing,
and could be realized by the standardized inclusion of
a certain metrics combination within popular imple-
mentation frameworks.
Bench-Marking: For classifier comparison, bench-
marking trained models within different areas of
medicine are important to establish a generally ac-
cepted performance base line. However, careful con-
sideration is necessary, since some metrics behave
differently, depending on the data collection process
A Methodology Based on Quality Gates for Certifiable AI in Medicine: Towards a Reliable Application of Metrics in Machine Learning
491

and its resulting diversity (Jussi, 2021, 5). For of-
ficial bench-marking, either independent real-world
test sets that are publicly unavailable should be cre-
ated (Kelly, 2019, 3), or, another approach are simula-
tion studies based on synthetic data (Friedrich, 2022,
3). Additionally, platforms that provide the necessary
infrastructure are required.
Imbalanced Data: As mentioned, imbalanced data
is a very common case for medical data. Thus, stake-
holders are expected to be aware of this situation and
select and interpret metrics accordingly. In contrast to
sensitivity and specificity, positive and negative pre-
dictive value (PPV/NPV) are ”[...] influenced by the
ratio of disease and healthy cases that happen to be in
the test set” (Jussi, 2021, 5), for instance.
5
Metrics Calculation: Careful considerations are
obligatory while designing training and validation
versus test data sets, since they are required to be in-
dependent for a bias-reduced evaluation and stratified
for class-imbalance. Other popular methods for the
data pipeline setup during the development process,
like cross validation and bootstrapping, are discussed
in (Jussi, 2021, 9-12) in great detail, referencing im-
portant settings that might need to be audited differ-
ently for certification.
Performance Optimization: To select optimal hy-
perparameters, it is crucial to optimize with respect
to the same error measure for comparison (Jussi,
2021, 13), which should be embedded and understood
within its medical application area. From a developer
perspective, the metric that will be monitored during
training for methods like early stopping or learning
rate reduction should be defined carefully.
Domain Embedding: Domain embedded evaluation
approaches are expected to be the most resourceful
approaches and should be considered as standard for
medicine, since the intelligent application’s real per-
formance is to be measured and understood regard-
ing its real-world impact (Kelly, 2019, 3). Luckily,
”[m]any fields of biomedicine have published their
own guidelines on how to evaluate machine learning
algorithms [...]” (Jussi, 2021, 9).
Generalizability: Due a high variation in clinical
data, achieving a reliable generalizability is challeng-
ing but important. A possible solution could include
on-site model training to sharpen a pre-trained model
towards its specific application context. Further, clin-
ical assessment requires independent and diverse test
sets that are capable to measure such abstracts con-
cepts, see Risk Analysis. (Kelly, 2019, 4)
5
PPV is equal to precision for binary classification
(Jussi, 2021, 6).
5 CONCLUSION
The present work outlines an approach to translate
legislation regarding medical AI applications into
concrete technical guidelines illustrated for metrics in
healthcare. First, the basic concept comprising our
proposed methodology is explained in detail, as well
as the current situation regarding certification and
software quality management for medical AI. Like-
wise, the philosophy underlying our methodology is
outlined while paying special attention to all stake-
holders from the beginning, is highlighted. Also, au-
diting should include all stakeholders’ perspectives:
the ML-developers’, health experts’ and/or patients’
view of the intelligent application. Further, current
ambiguities regarding metrics selection that demand
for auditing in medicine to create/retrace commonly
accepted concepts to their origins for repeated (re-
)evaluation, are addressed. Finally, guidelines for Cri-
teria definition(s) that comprise QG Metrics are pro-
posed. As of now, we are working on a project in the
ECG domain for multi-label classification that will be
published as a use case for the proposed approach to-
wards a reliable metrics application.
Our suggested methodology is one possible ap-
proach to realize algorithm auditing, and current re-
search should continue to develop standardized com-
pilations for specific ML use cases in favor of the au-
diting process. Thanks to the multitude and diversity
of such use cases, this is not a trivial approach, and the
present paper ventures a first attempt to design a com-
prehensive methodology, presented in more detail for
a reasonable selection process for ML performance
metrics. To address all existing medical use cases, ex-
tensive further research is required, possibly follow-
ing a mixture of newly proposed technical guidelines,
as in (Oala, 2021; Jussi, 2021).
Another principal question that should be further
analyzed is to what extend open-sourcing should be
made obligatory, since a monopoly on such power-
ful technologies is questionable. An important part of
the outlined methodology includes indexes for Risk
Analysis that are designed to evaluate more abstract
but indispensible concepts such as transparency or
robustness. Further research should consider addi-
tional indexes that contribute to a more sound vue
d’ensemble of the whole model’s performance and
compliance with legislation, as well as develop tech-
nical realizations for relevant points during the soft-
ware life cycle. While developing such concepts, it
might be future-oriented to consider their generaliz-
ability towards bench-marking different artifacts like
data sets or models, which the presented Scoring Sys-
tem might be suitable for. Another crucial aspect, that
ICSOFT 2023 - 18th International Conference on Software Technologies
492

could be included in standard auditing of intelligent
medical devices, is measuring metrics or other com-
ponents via statistical tools such as standard devia-
tion and confidence intervals, refer to (Jussi, 2021)
for more information.
ACKNOWLEDGEMENTS
This work was partially funded by the German Fed-
eral Ministry of Education and Research (BMBF) un-
der reference number 031L9196B.
REFERENCES
Ben-Menahem, S. M., e. a. (2020). How the new european
regulation on medical devices will affect innovation.
Nature Biomedical Engineering, 4(6):585–590.
Boulogne, L. H., e. a. (2023). The stoic2021 covid-19 ai
challenge: Applying reusable training methodologies
to private data. Manuscript submitted for publication.
Davis, J., e. a. (2006). The relationship between precision-
recall and roc curves. In Proceedings of the 23rd In-
ternational Conference on Machine Learning, ICML
’06, page 233–240, New York, NY, USA. Association
for Computing Machinery.
European Commission, D.-G. f. C. N. C. . T. (2020). The
Assessment List for Trustworthy Artificial Intelligence
(ALTAI) for self assessment. Publications Office.
European Commission, D.-G. f. C. N. C. . T. (2021). Reg-
ulation of the european parliament and of the council
laying down harmonised rules on artificial intelligence
(artificial intelligence act) and amending certain union
legislative acts.
European Commission, D.-G. f. H. . F. S. (2023). Proposal
for a regulation of the european parliament and of the
council amending regulations (eu) 2017/745 and (eu)
2017/746 as regards the transitional provisions for cer-
tain medical devices and in vitro diagnostic medical
devices (text with eea relevance.).
Filz, M., e. a. (2020). Virtual quality gates in manufacturing
systems: Framework, implementation and potential.
Journal of Manufacturing and Materials Processing,
4.
Flohr, T. (2008). Defining suitable criteria for quality gates.
In Software Process and Product Measurement, pages
245–256, Berlin, Heidelberg. Springer Berlin Heidel-
berg.
Friedrich, S., e. a. (2022). On the role of benchmarking data
sets and simulations in method comparison studies.
Henry, K. E., e. a. (2022). Human-machine teaming is
key to AI adoption: clinicians’ experiences with a
deployed machine learning system. NPJ Digit Med,
5(1):97.
Hicks, S. A., e. a. (2022). On evaluation metrics for medi-
cal applications of artificial intelligence. Scientific Re-
ports, 12(1):5979.
Jussi, T., e. a. (2021). Evaluation of machine learning algo-
rithms for health and wellness applications: A tutorial.
Computers in Biology and Medicine, 132:104324.
Kelly, C. J., e. a. (2019). Key challenges for delivering clini-
cal impact with artificial intelligence. BMC Medicine,
17(1):195.
Koshiyama, A., e. a. (2021). Towards algorithm auditing:
A survey on managing legal, ethical and technologi-
cal risks of ai, ml and associated algorithms. SSRN
Electronic Journal.
MacEachern, S. J., e. a. (2021). Machine learning for pre-
cision medicine. Genome, 64(4):416–425.
Martin, C. H, e. a. (2021). Predicting trends in the qual-
ity of state-of-the-art neural networks without access
to training or testing data. Nature Communications,
12(1):4122.
M
¨
uller, D., e. a. (2022). Towards a guideline for evalu-
ation metrics in medical image segmentation. BMC
Research Notes, 15(1):210.
Muller, H., e. a. (2021). The ten commandments of ethical
medical ai. Computer, 54(07):119–123.
Niemiec, E. (2022). Will the EU medical device regulation
help to improve the safety and performance of medical
AI devices? Digit Health, 8:20552076221089079.
Oala, L., e. a. (2021). Machine learning for health: Al-
gorithm auditing & quality control. J Med Syst,
45(12):105.
Papadopoulos, Y., e. a. (2010). Automatic allocation of
safety integrity levels. pages 7–10.
Paula F., W. P. (2006). Quality gates in use-case driven
development. In Proceedings of the 2006 Interna-
tional Workshop on Software Quality, WoSQ ’06,
page 33–38, New York, NY, USA. Association for
Computing Machinery.
Reinke, A., e. a. (2021). Common limitations of image pro-
cessing metrics: A picture story.
Ribeiro, A. H., e. a. (2020). Automatic diagnosis of the
12-lead ECG using a deep neural network. Nature
Communications, 11(1).
Ribeiro, M. T., e. a. (2016). ”why should i trust you?”:
Explaining the predictions of any classifier.
Roberts, M., e. a. (2021). Common pitfalls and recommen-
dations for using machine learning to detect and prog-
nosticate for covid-19 using chest radiographs and ct
scans. Nature Machine Intelligence, 3(3):199–217.
Saito, T., e. a. (2015). The precision-recall plot is more
informative than the roc plot when evaluating bi-
nary classifiers on imbalanced datasets. PLOS ONE,
10(3):1–21.
Schneeberger, D., e. a. (2020). The european legal frame-
work for medical ai. In Machine Learning and Knowl-
edge Extraction, pages 209–226, Cham. Springer In-
ternational Publishing.
Strodthoff, N., e. a. (2020). Deep learning for ecg analysis:
Benchmarks and insights from ptb-xl.
Zhang, M., e. a. (2014). A review on multi-label learning al-
gorithms. IEEE Transactions on Knowledge and Data
Engineering, 26(8):1819–1837.
A Methodology Based on Quality Gates for Certifiable AI in Medicine: Towards a Reliable Application of Metrics in Machine Learning
493
