
Methodology of Toxicometric Evaluation
of Acute Poisonings
A.I. Iskandarov
1
a
and B. Eshmuratov
2
b
1
Ministry of Health of the Republic of Uzbekistan
,
Tashkent, Uzbekistan
2
Department of Forensic Medicine, Tashkent Medical Academy, Tashkent, Uzbekistan
Keywords: Toxicometry, Chemical Illness, Factor and Cluster Analysis, Concentration Thresholds, Toxicokinetics.
Abstract: This article introduces a novel methodological framework for evaluating acute chemical illness, facilitating
the identification of the primary impact of toxic agents on homeostasis. This approach enables tailored
detoxification strategies and supports a rigorously justified forensic medical evaluation of the severity of
chemical injuries and their postmortem diagnosis. By offering insights into the direction of toxic agent effects,
this methodology contributes to more effective management of chemical trauma cases. It enhances our ability
to provide targeted medical interventions and ensures a comprehensive understanding of the pathological
processes involved, thereby advancing forensic medicine practices in this domain.
1 INTRODUCTION
Chemical pollution poses a significant threat to
human life and the environment globally, including in
Uzbekistan, driven by extensive chemical production,
international trade, and widespread use in various
sectors. With over 7 million chemical substances
synthesized and approximately 70 thousand in daily
use, the potential consequences of this pollution are
vast and unpredictable. Public health protection from
chemical pollution receives insufficient attention in
environmental programs, despite humans being both
perpetrators and primary victims of environmental
disasters. Biomonitoring for acute human poisoning
could provide valuable insights into environmental
conditions, yet the country lacks adequate measures
and interdepartmental coordination for prevention.
Responsibility for chemical product safety falls on the
Ministry of Health's sanitary and epidemiological
service, primarily focused on setting maximum
allowable concentrations (MACs) and production
control. However, during emergencies, human
exposure often far exceeds MACs, necessitating the
development of acute toxicity passports. This study
aims to devise a new methodological approach for
assessing acute poisonings, leveraging real clinical
a
https://orcid.org/0009-0008-0110-1221
b
https://orcid.org/0009-0002-1787-4399
and morphological data from forensic medicine
centres.
2 MATERIALS & METHODS
The material for the research consisted of 252 cases
of acute poisonings with the most common industrial,
household toxins, and medications. The study
employed multidimensional statistical analysis
methods: factor, cluster, nonlinear regression
analyses, and a probit graph of the "poison
concentration-effect" relationship.
3 RESULTS & DISCUSSION
Below is the methodological rationale and examples
of toxicometric assessment of industrial, household,
and medicinal products. The use of toxicometric
(quantitative) assessment of chemical illness in
forensic medicine is proposed for the first time by the
author of this investigation.
In the first section, "Passports for the acute
toxicity of a chemical compound," an assessment of
the risk of death for victims is provided across the
1608
Iskandarov, A. and Eshmuratov, B.
Methodology of Toxicometric Evaluation of Acute Poisonings.
DOI: 10.5220/0012987800003882
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 2nd Pamir Transboundary Conference for Sustainable Societies (PAMIR-2 2023), pages 1608-1612
ISBN: 978-989-758-723-8
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
entire range of recorded concentrations of toxins in
the blood. For this purpose, the "probit analysis"
method is used (Fig. 1).
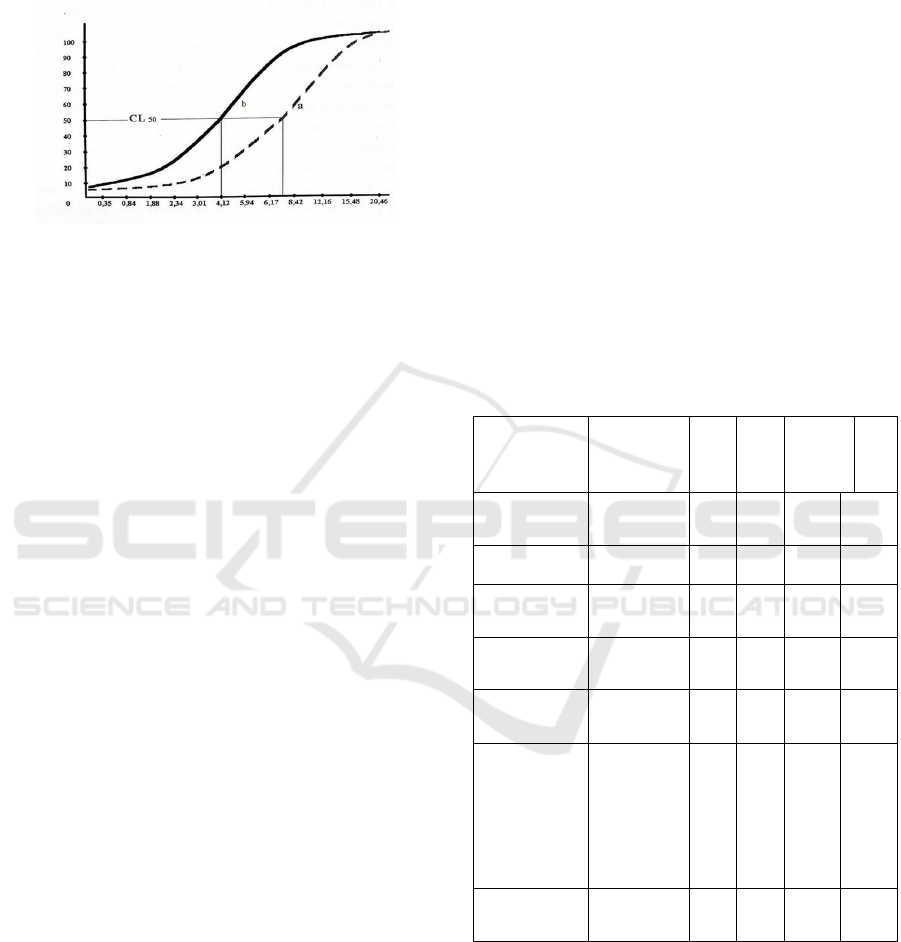
Figure 1. Probit graph of the "free hemoglobin
concentration-effect" relationship in acute poisonings with
acetic acid. On the abscissa axis - the logarithm of
intravascular hemolysis level, on the ordinate axis - the
percentage of the risk of death.
In a typical case, the probit plot of the "concentration
of poison-effect" relationship has an S-shaped form.
The lower flat portion of the graph (or its lower
asymptote) corresponds to poison concentrations
where the initial magnitude of chemical injury does
not exceed the limits of the physiological defense of
the organism, and the outcome of poisoning is always
favorable. This level is denoted as CL0 - the
maximum tolerable concentration of poison. It is
characterized by the onset of acute clinical symptoms
of poisoning and can be labeled as the threshold for
acute poisoning.
The next ascending portion of the graphical curve
corresponds to concentrations where the outcome of
poisoning is uncertain, and the risk of death
exponentially increases with the rise in poison content
in the blood. Within these concentrations, the
organism is in a critical state, and the treatment
outcome largely depends on the organization of
intensive detoxification therapy. When assessing the
critical condition of the organism, the mean lethal
concentration of poison in the blood (CL50) can be
used as an objective criterion. From a forensic
perspective, this level of poison in the blood is
considered life-threatening, and the data from
poisoning are regarded as severe bodily injuries
(harm to health) dangerous to life.
Having reached a certain limit, and regardless of
further increases in the concentration of the toxic
agent, the probit plot curve returns to a horizontal
position. This segment (upper asymptote)
corresponds to CL100 - the absolutely lethal
concentration of poison or a life-incompatible
chemical injury.
Thus, the analysis of the "concentration of poison-
effect" relationship is a valuable tool in studying the
quantitative aspects of the relationship between the
absorbed dose of a chemical substance and the nature
of the overall response of the organism. From the
perspective of this relationship, the crisis of
homeostasis should be characterized as an unstable,
transitional state between the two only possible polar
outcomes of poisoning - recovery and death.
Using such normative graphs, an objective
prognosis of the outcome can be provided even at the
very beginning of a chemical injury. In accordance
with the risk of death, priority service can be ensured
for the most severely affected contingent in mass
chemical disasters. The results of the toxicometric
assessment of the risk of death in acute poisonings
with industrial, household poisons, and
pharmaceuticals are presented in Table 1.
Table 1. Results of toxicometric assessment of mortality
risk in acute poisonings with industrial, household toxins,
and medicinal preparations.
Name of
Poison
Toxicomet
ric
Parameters
Ch0 Ch2
5
Ch5
0
Ch75 Ch10
0
1 2 3 4 5 6
Dichloroetha
ne (
μg
/k
g
)
2,76 8,31 14,6
3
19,20 26,44
Carbofos
(
μg
/k
g
)
0,3 176 1,04 1,92 3,03
Chlorophos
(
μg
/k
g
0,21 1,22 3,81 6,41 8,51
Acetic Acid
(free
hemoglobin
in blood
plasma,
μg
/k
g
)
1,48 5,62 10,8
4
16,80 33,88
Phenobarbit
al (
μg
/k
g
)
16,0 38,1
5
66,6
9
151,3
4
215,7
2
Critical condition is not only a specific form of
disturbances in the body's vital functions but also a
distinct phase in the course of a pathological process.
Unfortunately, in the majority of contemporary
studies, the dynamics of mortality risk in poisonings
are not considered. However, this indicator is no less
important as a criterion for the danger of a chemical
compound than the poison level in the blood. Figure
2 presents graphs of survival probabilities for patients
Methodology of Toxicometric Evaluation of Acute Poisonings
1609
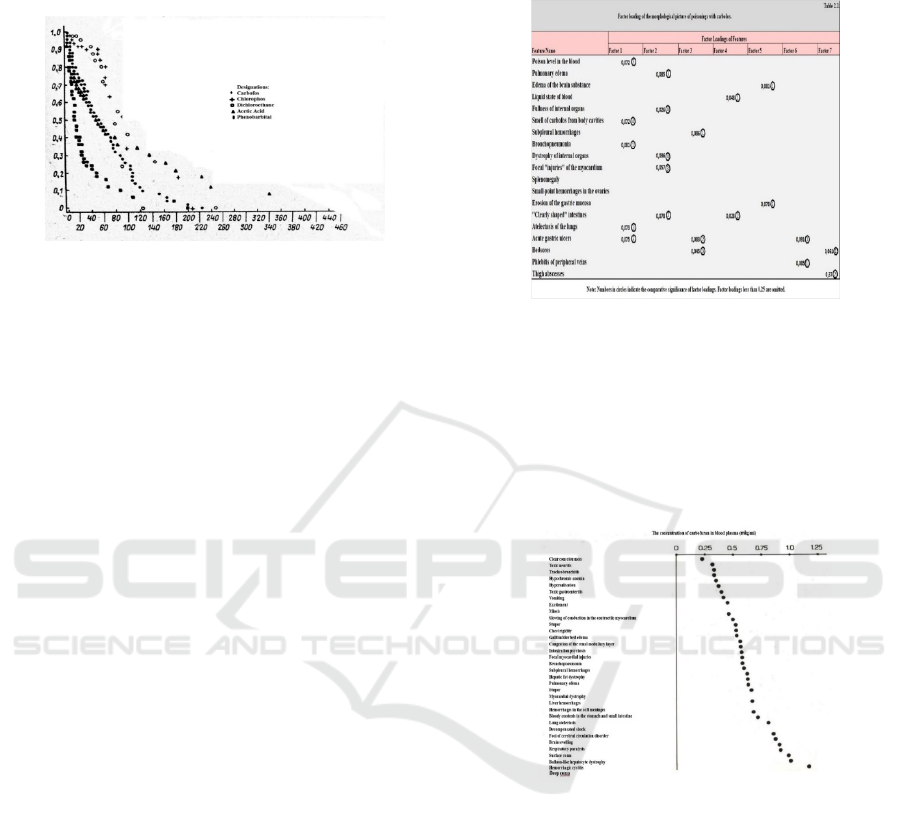
at each moment in time during adverse outcomes of
various chemical diseases (Fig. 2).
Figure 2. Duration of life for victims in adverse outcomes
of acute poisonings. On the ordinate axis - the probability
of survival at time T; on the abscissa axis - time (hours).
This indicator is obtained using a computer when
determining the reliability function in a special
mathematical model by D.R. Cox.
Upon scrutinizing the graphs, it's evident that the
survival likelihood declines rapidly within the initial
hours of dichloroethane poisonings, whereas with
acetic acid or carbofos, homeostasis reliability
diminishes less drastically, allowing the dying
process to extend up to 120-200 hours.
Conversely, irreversible effects in phenobarbital
poisoning manifest relatively late, typically after
severe pulmonary complications set in, such as
pneumonia. Thus, based on mortality intensity,
dichloroethane merits classification as an extremely
hazardous substance, while carbofos and acetic acid
qualify as highly toxic, and phenobarbital as
moderately toxic poisons. This classification
becomes pivotal for patient triage during mass
poisonings.
In the study of acute poisonings, discerning
between the direct impact of the poison and the body's
response poses a crucial challenge. The specificity of
subsequent clinical symptoms and morphological
changes remains largely unexplored, impeding
informed pathogenetic treatment and expert
assessment of illness severity and postmortem
diagnosis.
To address this complexity, factor analysis
emerges as a methodologically sound approach,
enabling the identification of interdependent features
and their correlation with the overall reaction of the
organism.
By delineating the significance of each feature
within the studied process, factor analysis provides
invaluable insights into the pathological mechanisms
underlying acute poisonings, exemplified by the
clinical-morphological profile of organophosphorus
compound poisoning.Table 2. Factor structure of the
clinical and morphological picture of poisonings with
carbofos.
It is known that chemical substances affect the cells of
tissues and organs only when their concentration exceeds a
threshold. Thus, if clinical and morphological signs of
poisonings are arranged according to the magnitude of their
concentration thresholds (as depicted in Fig. 3, using acetic
acid poisoning as an example), they will be grouped based
on the resistance of each tissue to the specific toxic
substance.
Figure 3. Concentration thresholds for the main clinical and
morphological signs of poisonings with the mentioned toxic
substance.
As indicated in the presented table, the critical
phase of chemical poisoning is characterized by the
greatest clinical diversity. Its distinctive feature is the
involvement in the pathological process of tissues,
organs, and systems to which the selective action of
the poison does not directly extend. With the help of
this program, it is possible to establish a typical
clinical-morphological picture of poisonings for any
specific magnitude of chemical trauma based on the
degree of hemoglobinemia. Conversely, based on the
nature of clinical and morphological changes, one can
deduce the highest concentration of the toxic
substance.
PAMIR-2 2023 - The Second Pamir Transboundary Conference for Sustainable Societies- | PAMIR
1610
Ultimately, the outcome of acute poisonings depends on
whether the body can eliminate the absorbed dose of the
poison. Therefore, in our comprehensive problem, special
attention is paid to studying the kinetics of poisons in the
blood. For each type of chemical substance, we have
developed normative toxicokinetic graphs using a computer
program we created. Leading parameters of this process
have been determined: the elimination rate constant and the
half-life period of the poison in the blood. These parameters
should be considered fundamental in monitoring the
resuscitation period of acute poisonings, allowing forensic
experts to assess the correctness of the treatments
administered (Table 3).
Table 3 Comparative Characteristics of the Toxicokinetics
of Organophosphorus Insecticides
Name of
the Poison
n Initial
level of
poison in
the blood
(μg/kg)
Eliminatio
n rate
constant of
the poison
(Ke)
Half-life
of the
poison in
the blood
(T1/2)
Maximum
duration of
the
toxicogeni
c phase
(hours)
Carbofos 150 0,15±0,0
6
35 19,8
0
7
2
Chloropho
s
100 1,70±0,2
5
39 17,7
6
5
3
Foxim 107 0,87±0,0
5
37 18,7
5
6
6
THM-3 69 1,02±0,1
5
23 30,1
3
9
8
Metafos 50 0,96±0,1
2
43 16,1
1
5
0
It is always advisable to study the course of chemical illness
from two perspectives: what the poison does to the
organism and how the organism itself affects the
biotransformation of the poison. Our research results have
shown that toxic coma, exotic shock, and several other
critical states of the organism can significantly prolong the
duration of poison circulation in the blood. This
circumstance needs be taken into account by forensic
experts when organs are removed from corpses for forensic-
chemical examinations.
The body's response to its damage is not an instantaneous
reaction but a process unfolding over time through specific
phases of interacting factors. In chemical illness, where the
sequence of toxic effects is, to a certain extent, a
consequence of the distribution and biotransformation of
poisons in the organism, the analysis of this process is
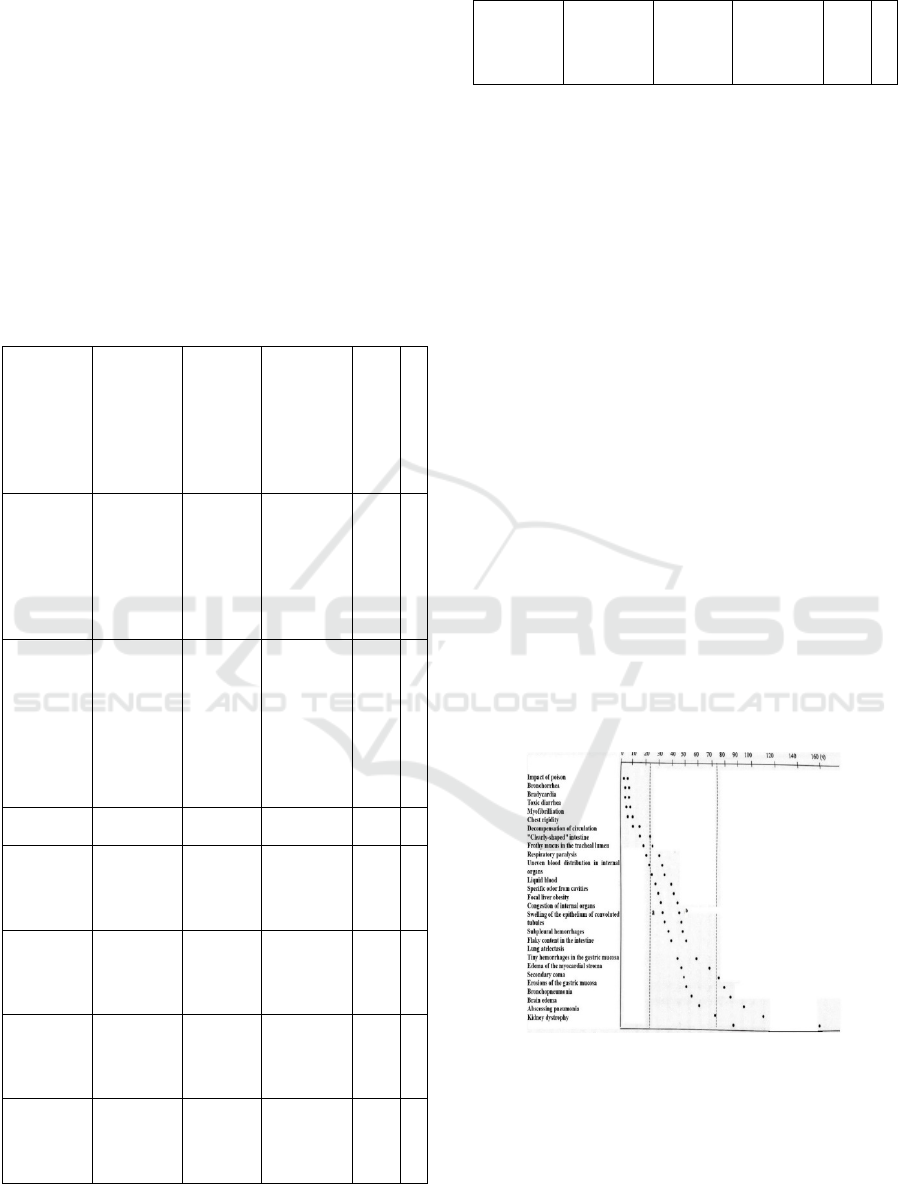
particularly relevant. Figure 4 presents the toxicodynamics
of the clinical and morphological manifestations of acute
poisonings with сhlorophos and сarbofos.
The pathogenetic connection that effectively exists between
different types of toxic effects is expressed in their
sequence. From the perspective of the dynamics of
poisoning, each preceding stage of chemical illness
prepares and shapes the subsequent one. Therefore, as a risk
factor for bronchopneumonia in this poisoning, all
preceding toxic effects and syndromes, especially
bronchorrhea, chest rigidity, and artificial ventilation of the
lungs (AVL), should be considered.
Figure 4. Toxicodynamics of the clinical and morphological
picture of poisonings with сarbofos and сhlorophos.
Before our research in clinical and forensic toxicology, the
study of critical conditions in poisonings was typically
fragmented. For the first time, we proposed the use of
multidimensional statistical analysis in synthesizing the
entire complex of chemical illness (Fig. 5).
Methodology of Toxicometric Evaluation of Acute Poisonings
1611

Figure 5. Structural portrait of acute phenobarbital
poisoning.
This figure demonstrates the structural portrait of acute
poisonings with phenobarbital obtained through the cluster
analysis method. This picture is presented as a graph, where
the vertices represent clinical-morphological and
laboratory-functional features of chemical illness, and the
connecting edges reflect the direction and inter-system
connections. In addition, the arrangement of features is
ranked according to their influence (level of proximity) on
the outcome of the illness. In other words, the upper part of
the graph contains features that dominate in the mechanism
of thanatogenesis (respiratory paralysis, pneumonia, etc.),
while the lower part of the graph concentrates indicators
that do not have a significant impact on the outcome of
poisoning.
4 CONCLUSION
The implementation of toxicometric assessment in
acute chemical illness offers valuable insights into the
primary effects of toxic substances on homeostasis,
facilitating tailored resuscitation interventions and
scientifically informed expert evaluations of illness
severity and post-mortem diagnoses. However,
addressing the complexities of medical care in acute
poisonings, particularly during mass disasters,
necessitates innovative solutions such as intelligent
computer systems. The sheer volume and diversity of
chemical illnesses make comprehensive physician
training in pathogenesis, clinical manifestations, and
treatment virtually unattainable. Consequently, the
development and deployment of such computer-
based programs are imperative for enhancing medical
response capabilities. Moving forward, collaboration
with institutions like the Research Institute of Clinical
and Experimental Lethal would be vital for advancing
research and implementing practical solutions to
improve outcomes in cases of acute chemical
poisoning.
REFERENCES
Berezhnoy R.V. (1984). Forensic Toxicological Studies
and Prospects for Their Development. Forensic
Medical Examination, 1, 17-20.
Gorbunov T.I. (1975). Some Issues of Intensive Therapy in
Acute Poisonings. Anesthesiology, Resuscitation, and
Intensive Care, Saransk, 309-315.
Dagaev V.N. (1984). Toxicokinetics of Some Poisons
Depending on the Severity of Chemical Trauma.
Intensive Therapy of Acute Toxicoses, Moscow, 26-30.
Egorov A.N., Krivovich K.I. (2008). Intensive Therapy in
Acute Poisonings Accompanied by Exotoxic Shock.
Current Problems of Anesthesiology and Resuscitation,
Dushanbe, 175-177.
Zagryadskaya A.P. (1977). Forensic Medical Examination
of Poisonings. Gorky.
Iskandarov A.I. (1992). Forensic Toxicometry and
Thanatogenesis of Acute Poisonings with Toxic
Industrial Chemicals. Author's Abstract of the Doctoral
Dissertation in Medical Sciences, Moscow.
Komarov F.I., Rapoport S.I. (1988). Chronomedicine –
Achievements and Tasks. Therapeutic Archives, 18(8),
12-17
Luzhnikov E.A. (1982). Clinical Toxicology. Moscow:
Medicine, 368.
Principles and Methods of Assessing the Toxicity of
Chemical Substances. (1991). WHO, Moscow:
Medicine, 312.
Tomilin V.V. (1982). Current State and Directions for the
Further Development of Forensic Toxicology. The 2nd
All-Union Congress of Forensic Medical Experts,
Moscow, 351-355.
Ostapenko Y.N., Matveev S.B. (2001). Epidemiology and
Medical Aid at Acute Poisoning in Russia. Preegl Lek,
58(4), 293-296.
Pivovarov G.N. (2000). Erroneous Diagnosis of
Myocardial Infarction in Acid Poisoning. Lik. Sprava,
Sep.(6), 83-84.
Su M. Nelson, L. (2001). Massive Necrosis of the
Gastrointestinal Tract After Ingestion of Acid. Y. Surg,
Oct., 167(16), 708.
Verstaeten S.M. (1992). Acute Respiratory Poisoning Due
to Concentrated Sulfuric Acid. Acta Tubete Pnevmol.
Belg, Jan-Art. 63(1), 122-126.
Weintraub B.A. (1997). A Total Case of Acid Ingestion.
Chicago, USA, Oct., 23(5), 413.
Zamir O., Hold G. et.al. (1985). Corrosive Injury to the
Stomach Due to Acid Ingestion. Am Y. Surg, Mar;
51(3), 170-173.
PAMIR-2 2023 - The Second Pamir Transboundary Conference for Sustainable Societies- | PAMIR
1612
