
Characterization of Telemedicine Patients to Discover Patient
Journeys Using Process Mining
Matías Cornejo T.
1a
, Sebastián Valderrama
2b
and Eric Rojas C.
3,4 c
1
Faculty of Medicine, Universidad de Chile, Santiago, Chile
2
Department of Internal Medicina, School of Medicine, Pontificia Universidad Católica de Chile, 7820436, Santiago, Chile
3
Institute for Biological and Medical Engineering, Schools of Engineering, Medicine and Biological Sciences, Pontificia
Universidad Católica de Chile, Santiago, Chile
4
Department of Clinical Laboratories, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile
Keywords: Telemedicine, Patient Journey, Patient Profile, Process Mining.
Abstract: Process mining has established itself as a highly valuable tool in healthcare and demonstrated its effectiveness
in process discovery, compliance verification and workflow optimization across a variety of clinical settings.
However, its application in the analysis of telemedicine medical care has not been explored in depth. The
present paper introduces the first stage of the research “Improving the patient journey in telemedicine using
process mining” which aims to optimize the care process in telemedicine. In this initial stage, the
characterization of patients who utilize this model of care in a hospital network in Chile between 2020 and
2023 is conducted. Accordingly, statistical information from the Red de Salud UC-Christus healthcare
network is used to determine the most frequent characteristics of patients in socio-demographic, health-
insurance and clinical terms. Profiles of typical patients who have received treatment via telemedicine will
then be constructed. The preliminary results presented herein will serve as a basis for selecting the type(s) of
patients who are of particular interest to institutional authorities. In the latter stages of the project, information
from the electronic clinical records of the selected patient profiles will be used to build event logs and thereby
construct patient journeys through process mining.
1 INTRODUCTION
Telemedicine has become an important tool with
which to bring healthcare closer to the general
population (World Health Organization [WHO],
2019; Welsh, 2002). Its use has reduced care costs,
improved clinical outcomes and increased user
satisfaction (Manocchia, 2020). Moreover, the
COVID-19 pandemic has given rise to significant
interest in this type of care and has, moreover,
become a public health necessity (Zheng Wong et al.,
2021). Therefore, a more in-depth analysis of its
implementation is required in order to ensure that
health system users continue to receive quality care.
Data science has been an extremely useful
resource in the study of new implementations in
medicine. One of these is process mining, which has
a
https://orcid.org/0009-0005-2905-1842
b
https://orcid.org/0000-0003-3913-6661
c
https://orcid.org/0000-0002-2570-1861
proven to be highly effective in several lines of
research. Therefore, the present study proposes the
use of this discipline in the construction of the patient
journey with telemedicine. This first stage of the
project focuses on the characterization of
telemedicine patients in a private hospital network in
Chile, with the aim of determining the most
appropriate patients to whom this novel technique can
be applied.
This paper first outlines the background of the
topic and the current context of telemedicine in Chile,
in Section 2. Section 3 introduces the objective of this
first stage of the research. Section 4 details the
methodology used in the analysis of the available
information and the subsequent construction of the
patient profiles by the private hospital network.
Section 5 discusses the results obtained. Finally,
T., M., Valderrama, S. and C., E.
Characterization of Telemedicine Patients to Discover Patient Journeys Using Process Mining.
DOI: 10.5220/0012460300003657
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 723-730
ISBN: 978-989-758-688-0; ISSN: 2184-4305
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
723

section 6 presents a brief conclusion of the results and
the possible future implications of these findings.
2 BACKGROUND
2.1 Telemedicine
Telehealth encompasses a wide range of tools that use
telecommunication systems for medical purposes
(Welsh, 2002). Among these tools, telemedicine is
defined as the use of information and communication
technologies for the exchange of valid information to
ensure diagnosis, treatment and prevention of
diseases (WHO, 2019).
The use of telemedicine has multiple benefits,
with Mendoza-Alonso et al. (2021) listing these as:
saving time and money, reducing patient absences,
improving health outcomes, decreasing the likelihood
of infections, offering personalized care, and
lowering costs for providers and insurers. However,
the same authors state that telemedicine still faces
certain challenges regarding its correct
implementation, particularly in terms of access to
stable communication networks that are necessary for
its appropriate implementation.
The COVID-19 pandemic had such a profound
impact on the global healthcare system that it
prompted a growth in demand for remote medical
care around the world (Zheng Wong et al., 2021).
With that in mind, telemedicine has been effective in
increasing access to health and medical information
for both patients and physicians since its inception
(WHO, 2019). Chile has been no exception to this
reality, and the Chilean State has set several related
objectives, including to decongest health systems,
improve access to health services, and address the
main challenges involved in implementing this model
(Universidad de Desarrollo [UDD] et al., 2020). In
addition, certain strategies have been proposed to
bring telemedicine closer to the population (Centro
Nacional de Sistemas de Información en Salud
[CENS], 2022). These include guidelines, protocols
and laws that have expanded their use in health
services. (UDD et al., 2020; Mendoza-Alonzo et al.,
2021; Chilean Law No. 21.541, 2023).
2.2 Patient Trajectories
The patient journey is defined as the time series of
encounters with healthcare facilities, healthcare
professionals, a hospital unit or a home health agency
(Beleffi et al., 2020). The patient journey study has
been used as a tool to assess patient satisfaction with
the care process, clinical outcomes, and even to
ensure patient safety during a hospital stay.
Several tools can be used to describe the patient
journey, one of which is process mining (Andrews et
al., 2020; Dahlin et al., 2019, Abo-Hamad, 2018).
Process mining is the bridge between traditional
model-based process analysis and contemporary data
analysis techniques, such as data mining and machine
learning (van der Aalst, 2016). Unlike other process
modeling tools, process mining uses data as empirical
evidence to build process models. It enables
institutions to optimize their workflows from
different perspectives. This is achieved through three
core activities that lie at the heart of process mining:
discovery, conformance checking, and optimization
(van der Aalst, 2016).
To perform these tasks, process mining needs an
event log as its means of input (van de Aalst, 2016).
The event log corresponds to a table that stores data
related to the activities performed in a single process.
The information stored in this table must contain at
least a case ID, the name of the activity and a
timestamp (van der Aalst, 2016). This information
allows for the activities performed for a process to be
traced in each of the cases. In this way, a process
diagram of the workflow of the institution in question
can then be constructed (Imran et al., 2022; Kratsch,
2021).
Process mining has been applied in distinct
industries and has achieved positive results across the
board (Ito et al., 2020). The healthcare sphere has
been no exception, and several studies have
demonstrated the benefits of its use in the medical
field (Kusuma et al., 2021). In particular, the review
conducted by Rojas et al. (2016) demonstrates the
utility of this technique in healthcare. The healthcare
system benefits from the application of process
mining because clinical practice requires a detailed
record of the activities performed by healthcare
personnel on the patient. Additionally, electronic
clinical records facilitate the traceability of events
(Rojas et al., 2016, Kusuma et al., 2021). Crucially,
the information contained within electronic clinical
records can be used to build event logs for process
mining (Arias et al., 2020, Munoz-Gama et al., 2022).
A particular use of process mining in healthcare is
its ability to discover the patient journey throughout
the care process (Andrews et al., 2020; Dahlin et al.,
2019, Abo-Hamad, 2018). Event logs help to identify
the steps patients follow through the different
departments of a hospital (Yang & Su, 2014; Rojas et
al., 2017). Patient pathway analysis allows
inefficiencies in the system to be uncovered (Sulis et
al., 2022) so that institutions can take steps to improve
HEALTHINF 2024 - 17th International Conference on Health Informatics
724

their use of resources and increase patient safety and
satisfaction (Sulis, 2022; Munoz-Gama et al., 2022).
Although data science is widely used in healthcare
(Su et al., 2022; Sarriegi, 2021; Liu, 2020), few
studies have investigated the use of process mining in
telemedicine (Kampeera, 2023; Corallo et al., 2021).
This is important because process mining is quite
flexible and can be adapted to different environments,
taking advantage of the data available for workflow
analysis (van der Aalst, 2016). It therefore has
tremendous potential to analyze the patient journey
and help to identify patterns that facilitate a more in-
depth understanding of that journey.
With that in mind, this project aims to use process
mining to construct the telemedicine patient journey,
and subsequently compare this trajectory with that of
patients who receive face-to-face treatment. The
objective is to determine whether telemedicine is
equivalent to the traditional care model with respect
to clinical and administrative aspects of the care
process.
In this first stage of the project, the data contained
in the information system of a private hospital
network will be analyzed to characterize the patients
who have received medical and non-medical care via
telemedicine. To undertake this characterization,
socio-demographic (sex, age, area of residence),
health insurance (publicly or privately financed) and
clinical (medical specialty) aspects will be
considered.
3 OBJECTIVES
The objectives of the present study are to characterize
the patients who receive telemedicine care according
to their socio-demographic realities and the medical
specialty sought via this model, to subsequently
discover patient journeys using process mining.
The purpose is to determine the benefits and
drawbacks of using process mining in the analysis of
patient trajectories in different clinical settings,
particularly in telemedicine and face-to-face care.
4 METHODOLOGY
First, an exploration of the available information will
be carried out to identify the types of patients who
choose either telemedicine or face-to-face care. For
the present study, the patient database of the Red de
Salud UC-Christus network in Santiago de Chile will
be used. In particular, the commercial database of the
Red de Salud UC-Christus network is analyzed,
which contains not only socio-demographic
information on patients, but also data regarding the
clinical specialties in which this model of care is
available, in addition to the type of financing the
institution receives from these patients. The use of
anonymized data has the approval of Scientific
Ethical Committee of Health Sciences of the
Pontificia Universidad Católica de Chile.
Second, the most relevant patient characteristics
will be defined. Specifically, analysis will be
undertaken of sex, age, district and region of
residence, financing, number of patients and number
of consultations for each of the health specialties that
provide telemedicine care.
Third, the characteristics will be explored
according to the interest of the clinical experts of the
Red de Salud UC-Christus network. First, the total
number of patients and consultations undertaken will
be made for both sexes between 1
st
June 2020 and 1
st
June 2023. Subsequently, a similar analysis will be
conducted over three one-year periods. The number
of patients and consultations related to each of the
specialties accessed during the three years will then
undergo analysis. The place of residence of the
patients will also be considered for all specialties.
Once this information has been aggregated, the
patient profiles related to the telemedicine model will
be created. To do so, the most frequently attending
sex will be analyzed first, followed by their most
likely place of residence (the most common district),
the most demanded specialty, and finally the most
commonly used type of health insurance. Analysis of
the other sex will then take place according to the
same order. Subsequently, a profile will be devised
which considers the second and third most common
place of residence. This characterization will help to
provide a more in-depth understanding of the
population that chooses the telemedicine model of
care, to focus the subsequent phases of the project on
more precise data.
Finally, the criteria with which to determine the
type of patient whose journey is to be discovered will
be defined. Clinical and administrative characteristics
of interest to clinical experts will be considered, as
well as institutional interests related to the growth of
the Red de Salud UC-Christus network.
In future research, a quality control of the data
extracted from the electronic clinical records of the
healthcare institution will be performed, followed by
the construction of the necessary event log to model
the patient journey through process mining.
Subsequently, process discovery algorithms will be
applied to this event log to obtain the patient journey.
Characterization of Telemedicine Patients to Discover Patient Journeys Using Process Mining
725
In the final analysis, the patient journeys obtained in
the previous step will be compared, in conjunction
with clinical experts, who will guide the work
according to the requirements of the institution’s
medical team.
5 RESULTS
5.1 Characterization
The present study analyzed data related to patients
from the Red de Salud UC-Christus network who
received telemedicine care during the three-year
period studied, from 1
st
June 2020 to 1
st
June 2023.
The data was obtained from the commercial statistics
belonging to the hospital network, which includes
information on age, sex, place of residence, health
insurance, number of patients, number of
consultations and specialties.
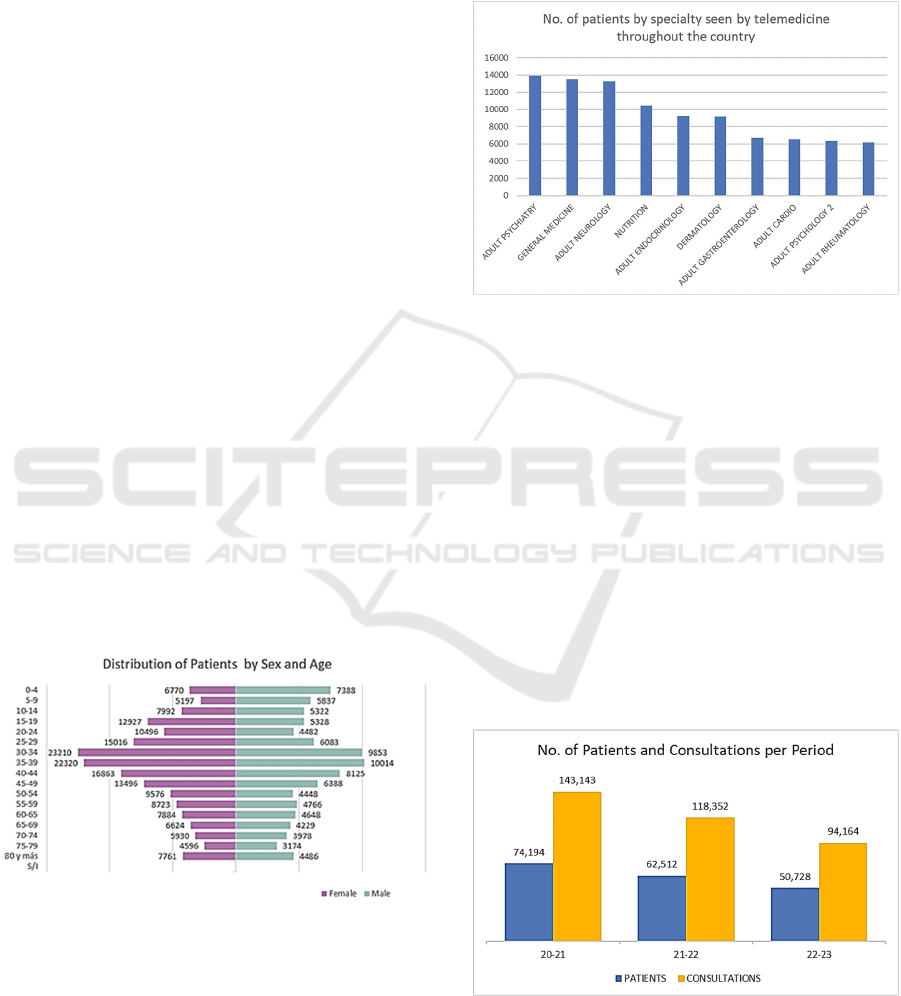
A total of 152,422 patients and 354,660
consultations were obtained, of which 52.6% of
patients are female and 30.8% are male, with the
remainder failing to disclose information on their sex.
The average age of the patients is 39.3 years for
females and 38.4 years for males. Figure 1 shows the
distribution of patients by sex and age.
Regarding medical specialties, 92 were analyzed
in total. The most sought specialties were adult
psychiatry, general medicine, and adult neurology,
with more than 13,000 patients accessing each one
during the three-year period studied. Figure 2 shows
the top ten specialties in terms of overall patient
numbers.
Figure 1: Distribution by sex and age of patients using
telemedicine in the Red de Salud UC-Christus network
between 1
st
June 2020 and 1
st
June 2023. Patients from the
30-40 age range are the most active users of telemedicine.
Regarding the geographical location of the
patients, it was found that of the 16 regions that
constitute Chile, the Metropolitan Region accounted
for 62.5% of all telemedicine care recieved, followed
by the Los Lagos Region with 8.3%. No other region
accounts for more than 8.3% of the national total. The
municipalities with the highest number of
consultations were Santiago, Las Condes, Ñuñoa and
Antofagasta.
Figure 2: No. of patients accessing each specialty across the
country between 1
st
June 2020 and 1
st
June 2023, in relation
to the ten most commonly accessed specialities.
Regarding distribution within the regions, it was
found that the population that uses the Red de Salud
UC-Christus network telemedicine the most lives in
the largest cities and that the number of patients
decreases in more peripheral areas near those cities.
For example, in the metropolitan region, which has
62% of the patients, most of them are in the city of
Santiago, where the UC-Christus Network is located,
while the outlying cities have fewer patients.
In addition, the data was analyzed over three 12-
month periods in order to observe the evolving
behavior of patients as the COVID-19 pandemic
progressed. Specifically, the following periods were
determined: 1
st
June 2020 to 31
st
May 2021 (20-21);
Figure 3: Number of patients and consultations for the 20-
21, 21-22 and 22-23 periods. A gradual drop in both
parameters is observed year-on-year.
HEALTHINF 2024 - 17th International Conference on Health Informatics
726
1
st
June 2021 to 31
st
May 2022 (21-22); and 1
st
June
2022 to 1
st
June 2023 (22-23). Figure 3 shows the
decrease in patients and consultations in the periods
described. The number of patients is shown in blue
and the number of consultations in yellow. The
number of patients decreased by 11.7% between 20-
21 and 21-22, and by 22.6% between 21-22 and 22-
23. Furthermore, consultations fell by 17.3% between
20-21 and 21-22 and by 20.43% between 21-22 and
22-23.
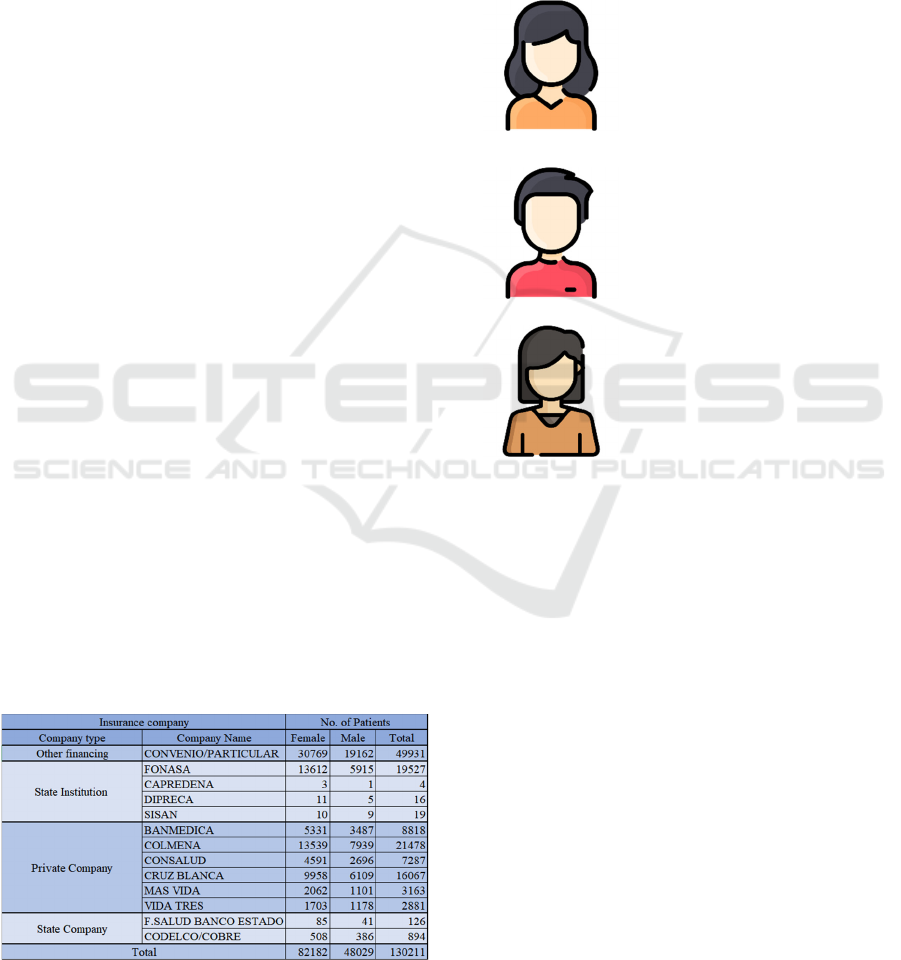
Subsequently, patients were analyzed according
to their sex and type of health insurance scheme held.
Chilean healthcare operates with a mixed financing
system that includes privately financed and
administered companies (the majority of insurers),
privately financed State-owned companies, and
public institutions with mixed public-private
contributions and State administration. Table 1 shows
the number of patients by sex for each type of
insurance held in the period 2020-2023. Note that the
discrepancy between the number of patients listed in
Table 1 compared to the number listed on the
healthcare network’s general database is due to the
fact this more detailed data is not necessarily
available for all patients.
The largest single group of patients (49,931, or
38.35%) financed their telemedicine care through
‘Other financing’, i.e., by means of another type of
insurance or private payment. The second largest
group of patients are beneficiaries of Fonasa, the main
public insurance provider in the country (19,527
patients), representing 15.00%. Private financing
reaches 45.84% (59,694 patients) and only one type
exceeds the total number of Fonasa patients
(Colmena). State-owned companies constituted only
1,020 patients, representing just 0.78%.
Table 1: Number and sex of patients who received
telemedicine care in the Red de Salud UC-Christus network
between 1
st
June 2020 and 1
st
June 2023 by health insurance
type.
5.2 Patient Profiles
This data can then be utilized to compile profiles of
patients who receive telemedicine care from the
hospital network. The patient profile consists of the
characteristics most likely to be found in any patient
of the healthcare institution, and considers each
characteristic as the most common for each profile,
based on sex and geographic location:
Sex: Female
Approximate age: 35-39 years old
Residence: Santiago,
Metropolitan Region
Specialty: Psychiatry
Financing: Convenio/Particular
(Medical contract/Private)
Sex: Male
Approximate age: 34-38 years old
Residence: Las Condes,
Metropolitan Region
Specialty: General Medicine
Financing: Convenio/Particular
(Medical contract/Private)
Sex: Female
Approximate age: 35-39 years old
Residence: Viña del Mar,
Valparaiso Region
Specialty: Neurology
Financing: Fonasa
The methodology proposed for data analysis and
patient profiling can be replicated in other institutions
with detailed socio-demographic information such as
that presented in this article.
5.3 Preparing Event Logs to Discover
Project Trajectories
To prepare the event logs, it is necessary to determine
the minimum data characteristics that will be
required. As described by van der Aalst (2016), event
logs store activity information, including case
identification data, activity identification and a
timestamp that allows for the differentiation of each
activity in the flow and ensures the traceability of
activities.
In conjunction with the clinical experts, the most
relevant profiles will be selected. Subsequently, the
event data stored in the electronic clinical record of
the Red de Salud UC-Christus network will be
extracted. To reiterate, the electronic clinical register
already functions based on a structure that allows
users to identify the minimum requirements for the
Characterization of Telemedicine Patients to Discover Patient Journeys Using Process Mining
727

construction of an event log. Table 2 provides an
example of what an event log would look like for the
patients.
Table 2: Example of an event log with clinical data.
Case ID Activity Timestamp Doctor
001 First consultation 2020/06/03 12:05:54 Dr Q.
002 Laboratory test 2021/10/05 11:58:06 Dr M.
004 Radiology test 2020/08/06 15:26:34 Dr Q.
001 Referral to specialty 2021/25/06 14:15:23 Dr L.
003 2nd consultation 2022/04/12 16:03:56 Dr X.
004 Referral to specialty 2020/08/07 15:06:05 Dr Q.
6 DISCUSSION
Preliminary results show that a diverse population of
patients is accessing telemedicine care from the Red
de Salud UC-Christus network. Yet, it is possible to
identify common characteristics that increase the
likelihood of finding one type of patient profile over
another. For example, the typical telemedicine patient
in the network is generally an adult, lives in the
Metropolitan Region, and is most likely female. In
addition, the data demonstrates that this typical
telemedicine patient finances their care privately.
The main specialties requested in telemedicine are
psychiatry, neurology and nutrition, which may be
due to the fact that these types of consultations are
easier to adapt to telemedicine than those requiring
physical analysis. However, the field of general
medicine is noteworthy because it represents the
second most requested type of consultation, in terms
of total number of patients. This is explained by the
fact that patients first consult in general medicine and
are then referred to a specialist.
When analyzing the geographic location of the
patients, it is observed that they are mainly
concentrated in large cities. This can be explained by
the fact that cities have larger populations than small
and remote towns. However, it is worth deliberating
whether the goal of telemedicine to bring healthcare
systems closer to remote populations is still being
met, as evidence shows that people with better access
to healthcare are those who use this model of care the
most.
When analyzing the number of patients and
consultations by period, an increasing drop in the
number of patients and consultations year-on-year
can be observed. There are two possible explanations
for this phenomenon: first, the end of the COVID-19
pandemic has resulted in patients preferring face-to-
face care once more; and second, patients have
decided to seek care in other healthcare centers.
Either way, greater amounts of data are required to
identify the reasons for the drop in patient numbers.
Since the patient profiles compiled in the present
study are based on statistics from the healthcare
institution rather than the electronic health record, a
more in-depth analysis is required to develop a more
detailed profile of users of the health services
provided by this hospital network. However, the
characterizations herein will allow clinical experts to
be consulted on a selection of the patient profiles that
are of particular interest to them and the healthcare
provider itself.
Another limitation of this project is that the study
is carried out in a single health institution. However,
the methodology proposed for the characterization
can be used in other centers that have this type of
registry. This allows for a multicenter comparison of
the results.
It should be noted that in the development of this
research, challenges related to data quality will arise.
To address this issue, the guidelines set out in
ISO/IEC 25012 will be followed and the relevance of
all data will be discussed with clinical experts.
In addition, it should be mentioned that, when
dealing with personal data, the correct use of sensitive
information will have to be considered to keep the
identity and integrity of users protected. In this same
sense, anonymized data will be used with the
approval of the Scientific Ethical Committee of
Health Sciences of the Pontificia Universidad
Católica de Chile.
Another challenge is that the data will not allow
traceability of events. This will be addressed by
working directly with the administrators of the
information systems to ensure that the time stamp of
each event is included.
7 CONCLUSIONS AND FUTURE
WORK
These preliminary results provide an improved
understanding of the universe of patients who use the
telemedicine service provided by the Red de Salud
UC-Christus network. Moving forward, it will be
possible to conduct a more rigorous analysis of how
telemedicine care is implemented across the network.
Such analysis will give rise to greater clarity on the
requirements needed to build an event log with which
to identify patient journeys.
Future efforts will involve a more thorough
analysis to establish an event log for identifying
patient journeys. Further work includes a literature
HEALTHINF 2024 - 17th International Conference on Health Informatics
728

review for additional patient characterization
methods, a study on the pros and cons of using
process mining in telemedicine research and
extracting patient data for journey discovery. The
subsequent comparison of telemedicine and face-to-
face care journeys aims to identify differences across
patient types, specialties, and diagnoses, offering
insights for improvement and informed decision-
making in patient care.
ACKNOWLEDGEMENTS
We thank the Red de Salud UC-Christus for their
collaboration in the execution of this project. We
thank the Universidad de Chile and the Pontificia
Universidad Católica de Chile for their support to this
research and the academia. Additionally, we thank
FONDECYT for their support of this research and
their ongoing assistance to the scientists of Chile.
This project is part of the FONDECYT
project #11230708 “Improving the Patient Journey in
Telemedicine using Process Mining”.
REFERENCES
World Health Organization. (2019). Recommendations on
Digital Interventions for Health System Strengthening
1
st
edition. WHO.
Welsh, T. (2002). Organizational structure of telehealth
care: an examination of four types of telemedicine
systems four types of telemedicine systems. PhD diss.,
University of Tennessee.
Manocchia, A. (2020). Telehealth: Enhancing Care through
Technology. Rode Island Medical Journal, 103(1), 18-
20. pubmed.ncbi.nlm.nih.gov/32013298
Mark Yu Zheng Wong, Dinesh Visva Gunasekeran, Simon
Nusinovici, Charumathi Sabanayagam, Khung Keong
Yeo, Ching-Yu Cheng, and Yih-Chung Tham. (2021).
Telehealth demand trends during the covid19 pandemic
in the top 50 most affected countries: Infodemiological
evaluation. Journal of Medical Internet Research
Public Health and Surveillance, 7(2):e24445, 2021
Universidad del Desarrollo, Universidad de Concepción, &
UC. Davis Chile Life Sciences Innovation Center.
(2020). Fundamentos para los Lineamientos para el
Desarrollo de la Telemedicina y Telesalud en Chile (2°
Edición)[PDF]. Extracted on October 19
th
, 2023 from
lineamientostelesalud.cl/2021/01/segunda-edicion-de-
los-fundamentospara-los-lineamientos-para-la-
telemedicina-y-telesalud-en-chile
Centro Nacional de Sistemas de Información en Salud.
(2022) Propuesta Colaborativa para Implementar la
Telemedicina en Chile [PDF]. Extracted on October
19
th
, 2023, from https://cens.cl/wp-
content/uploads/2022/07/Propuesta-Telemedicina-
jul2022.pdf
Mendoza-Alonzo, P., Mendoza-Alonzo, J. (2021).
Telemedicine: expected challenges in Chile based on
the experience in the United States during the
pandemic. Revista Médica de Chile, 149(8).
Modifica la normativa que indica para autorizar a los
Prestadores de Salud a efectuar atenciones mediante
Telemedicina. Ley N° 21.541. March 3
rd
, 2023 (Chile).
van der Aalst, W. (2016). Data Science in Action. In:
Process Mining. Springer, Berlin, Heidelberg.
Imran, M., Maizatul, I., Hamid, S., Nizam, M. (2022).
Complex Process Modeling in Process Mining: A
Systematic Review. IEEE Access. 10.
Kratsch, W. (2021). Data-driven Management of
Interconnected Business Processes - Contributions to
Predictive and Prescriptive Process Mining. EPub
Bayeruth. epub.uni-bayreuth.de/id/eprint/5329/
Ito, S., Vymětal, D., & Šperka, R. (2020). Process mining
approach to formal business process modelling and
verification: a case study. Journal of Modelling in
Management, 16(2), 602-622.
Rojas, E., Munoz-Gama, J., Sepulveda, M., Capurro, D.
(2016). Process mining in healthcare: A literature
review. Journal of Biomedical Informatics 61.224–236.
Kusuma, G. P., Kurniati, A. P., Rojas, E., Mcinerney, C.,
Gale, C. P., & Johnson, O. A. (2021). Process Mining
of Disease Trajectories: A Literature Review. IOS
Press eBooks.
Arias, M., Rojas, E., Aguirre, S., Cornejo, F., Munoz-
Gama, J., Sepúlveda, M., Capurro, D. Mapping the
Patient’s Journey in Healthcare through Process
Mining. Int. J. Environ. Res. Public Health 2020, 17.
Munoz-Gama, J., Martin, N. D., Fernandez-Llatas, C.,
Johnson, O. A., Sepúlveda, M., . . . Zerbato, F. (2022).
Process mining for healthcare: Characteristics and
challenges. Journal of Biomedical Informatics, 127,
103994.
Yang, W., & Su, Q. (2014). Process mining for clinical
pathway: Literature review and future directions.
(2014). In 11th International Conference on Service
Systems and Service Management (ICSSSM), Beijing,
China, 2014, pp. 1-5.
Rojas, E., Sepúlveda, M., Munoz-Gama, J., Capurro, D.,
Traver, V., Fernandez-Llatas, C. (2017). Question-
Drive Methodology for Analyzing Emergency Room
Processes Using Process Mining. Applied Science,
7(3):302.
Guzzo, A., Rullo, A., & Vocaturo, E. (2022). Process
mining applications in the healthcare domain: A
comprehensive review. Wiley Interdisciplinary
Reviews: Data Mining and Knowledge Discovery,
12(2), e1442.
Erdogan, T. and Tarhan, A., Systematic Mapping of
Process Mining Studies in Healthcare, IEEE Access, 6,
pp. 24543-24567, 2018.
Rinner, C.; Helm, E.; Dunkl, R.; Kittler, H.; Rinderle-Ma,
S. (2018). Process Mining and Conformance Checking
of Long Running Processes in the Context of
Characterization of Telemedicine Patients to Discover Patient Journeys Using Process Mining
729

Melanoma Surveillance. International Journal of
Environmental Research and Public Health, 15, 2809.
Andrews R, Wynn MT, Vallmuur K, ter Hofstede AHM,
Bosley E. (2020). A Comparative Process Mining
Analysis of Road Trauma Patient Pathways.
International Journal of Environmental Research and
Public Health. 17(10):3426.
Dahlin S, Eriksson H, Raharjo H. (2019). Process Mining
for Quality Improv: Propositions for Practice and
Research. Quality Management in Health Care.
28(1):8-14.
Abo-Hamad W. (2018) Patient Pathways Discovery and
Analysis Using Process Mining Techniques: An
Emergency Department Case Study. In: Cappanera, P.,
Li, J., Matta, A., Sahin, E., Vandaele, N., Visintin, F.
(eds) Health Care Systems Engineering. ICHCSE 2017.
Springer Proceedings in Mathematics & Statistics, vol
210. Springer, Cham.
Beleffi, E., Mosconi, P., & Sheridan, S. E. (2020). The
patient journey. Springer eBooks (pp. 117-127).
Sulis, E., Amantea, I. A., Aldinucci, M., Boella, G.,
Marinello, R., Grosso, M., Platter, P., & Ambrosini, S.
(2022). An ambient assisted living architecture for
hospital at home coupled with a process-oriented
perspective. Journal of Ambient Intelligence and
Humanized Computing.
Su, J., Zhang, Y., Ke, Q., Su, J., & Yang, Q. (2022).
Mobilizing artificial intelligence to cardiac
telerehabilitation. Reviews in Cardiovascular
Medicine, 23(2), 045.
Sarriegi, J. K., Beristain, A., Sánchez, R. H., Graña, M.,
Rebescher, K. M., … Konstantinidis, E. I. (2021).
COLAEVA: Visual Analytics and Data Mining Web-
Based Tool for Virtual Coaching of Older Adult
Populations. Sensors, 21(23), 7991.
Liu, J., Zhang, W., Jiang, X., & Zhou, Y. (2020). Data
Mining of the Reviews from Online Private Doctors.
Telemedicine Journal and E-health, 26(9), 1157-1166.
Extraído de:doi.org/10.1089/tmj.2019.0159
Kampeera, W. (2023). The implementation of telemedicine
to reduce doctor visits in the social medicine clinic at
Hatyai hospital. Journal of the Thai Medical Informatic
Association, 9(1), 42-51.
Angelo Corallo, Mariangela Lazoi, Roberto Paiano, and
Fabrizio Striani. (2021). Application of Process Mining
in Teleconsultation Healthcare: Case study of Puglia
Hospital. In Proceedings of the 10th International
Conference on Information Systems and Technologies
(ICIST '20). Association for Computing Machinery,
New York, NY, USA, Article 32, 1–13.
International Organization for Standardization. (2008).
Software engineering -- Software product Quality
Requirements and Evaluation (SQuaRE) -- Data quality
model (ISO/IEC Standard No. 25012). Retrieved from
https://www.iso.org/standard/35736.html
HEALTHINF 2024 - 17th International Conference on Health Informatics
730
