
Health Scores for Generating Health-Respecting Shift Plans by Means of
an Expert System from the Perspective of Care Organisations
Damian Kutzias
a
, Sandra Frings
b
, Stefan Strunck
c
and Petra Gaugisch
d
Fraunhofer IAO, Fraunhofer Institute for Industrial Engineering IAO, Germany
fi
Keywords:
Shift Planning, Health Score, Digitalisation, Care Organisations, Care Worker, Expert System,
Health-Respecting Shift Plan.
Abstract:
The care section is an essential part of our society as well as our everyday life. It is also a section which
suffers from staff shortage. Even though the job itself is not the problem, the shortage is related to shift-related
below-average working conditions. This work focuses on health-related aspects of shift planning in order to
provide insights which can assist in improving the situation of care workers. To this end, a literature and law
analysis was followed by interviews to collect, aggregate and extend health-related rules for the shift planning
process. A list of derived rules from practice is presented in addition to a discussion of previous insights from
literature. Based on these rules, a publicly available software demonstrator was implemented for sensitisation
and to show how a health-focused shift plan generation could look like. The basis for shift plan evaluation
is a health score definition, which takes into account the number of shifts and weighted rule violations. The
demonstrator was also used on shift plan data covering several years, resulting in insights about rule violations
from practice.
1 INTRODUCTION
In the discussion about the shortage of skilled care
workers and the ensuring nursing care in Germany,
the stressful working conditions in the care sector are
coming to the fore. High physical and psychological
demands, high work density combined with too lit-
tle time for nursing activities, frequent overtime and
changes in shift plans as well as little room for ma-
noeuvre at work characterise the everyday life of the
care staff. This resulted in a high rate of sick leave,
high fluctuation in the care staff and reductions of
working hours. The low attractiveness of the care sec-
tor is not the result of dissatisfaction with the job it-
self, but rather the demotivating working conditions
(Rohwer et al., 2021; Rothgang et al., 2020).
The BKK Health Report of 2022 shows that em-
ployees in elderly care were absent due to illness for
an average of 33.2 days. On average, this is 15 days
more than the average of all employees in Germany
with 18.2 sick days per employee (Knieps and Pfaff,
2022).
a
https://orcid.org/0000-0002-9114-3132
b
https://orcid.org/0000-0002-9639-6948
c
https://orcid.org/0000-0001-6673-1904
d
https://orcid.org/0000-0003-0195-8328
Other studies, such as the AOK-Bundesverband
(AOK-Bundesverband, 2023) or the Tech-
nikerkrankenkasse (TK Die Techniker, 2023),
confirm this trend. This vicious circle of high sick-
ness rates and increasing staff shortages resulted in
increasing workload for the remaining care staff. The
recovery phase during the non-working time is often
interrupted because care workers have to step in for
colleagues at short notice (Herrmann and Woodruff,
2019).
According to the BKK study mentioned above,
44.2 percent of geriatric care workers said that they
are currently only partially or not at all able to cope
with the higher demands of their job. This proportion
is almost twice as high as in other professions, where
it is 24.6 percent. One out of four care employees
are considering changing employers within the next
two years. More than one in five people are thinking
about giving up their profession completely (Knieps
and Pfaff, 2022). To break this vicious cycle, strategic
measures are required that aim to improve working
conditions as well as to support employees through
health-respecting shift plans.
According to the DGB Good Work Index of 2018,
69 percent of care staff work in shifts, 82 percent on
weekends, 17 percent in the night shift and 54 percent
Kutzias, D., Frings, S., Strunck, S. and Gaugisch, P.
Health Scores for Generating Health-Respecting Shift Plans by Means of an Expert System from the Perspective of Care Organisations.
DOI: 10.5220/0012557200003699
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2024), pages 121-131
ISBN: 978-989-758-700-9; ISSN: 2184-4984
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
121

in the evening shift (Schmucker, 2019). Studies show
that shift work can be stressful for both health and so-
cial life (Hirschwald et al., 2020; Jacobs et al., 2019;
Strauß et al., 2021).
Shift planning in care facilities is a tool for
scheduling staff. It has a significant impact on the
quality of patient care, the job satisfaction of care
staff and the efficiency of the facility. In addition, the
shift plans document compliance with laws, accident
prevention regulations and collective agreements, etc.
(Birkenfeld, 2000). The challenge for those persons
creating shift plans lies in taking into account the in-
terests of residents and the employees of the facility
itself. Residents demand a consistent quality of care
as well as flexibility in the provision of care.
Software applications have supported the design
of shift plans for many years. Today’s software for
shift planning is usually integrated into a software
suite used in the care domain. For care work, digital
support is particularly important for documentation as
well as planning of resources (Daum, 2022). A recent
study found out, that the majority (89 percent) of the
surveyed care organisations stated that care schedul-
ing/shift planning is predominantly performed digi-
tally (Daum, 2022). One major challenge with shift
planning is the volatility of the work - a challenge
which can be reduced with software supported solu-
tions. These systems can offer a spontaneous visu-
alisation of the consequences of a planning decision
by showing time accounts, staffing information and
information regarding rest times and other legal or er-
gonomic criteria. Shift planning can be supported to
a lesser or greater automation extent (Kubek et al.,
2020), whereat the software usually offers the option
for managing profiles for each employee/care staff
member that stores availability and personal prefer-
ences.
Planning software is usually able to show vio-
lation of relevant rules, usually predominantly law-
based rules. Due to the fact, that the systems already
stores huge sets of data regarding personnel and their
shift plans, this data could be used to extract infor-
mation regarding the “quality” of a shift plan seen as
a whole as well as on employee level. The quality
can be measured with different aspects in mind. This
work focuses on health-related quality measures, tak-
ing into account rules derived from law, science and
interviews.
The contributions of this work are as follows:
health-related rules for shift planning are presented
and discussed in three categories, extending law-
based and established rules by recommendations de-
rived from interviews. In addition, a health score is
introduced as a health-based measurement for shift
plans. Last, but not least, a demonstrator is presented
which shows an implementation of the discussed con-
cepts, emphasising the importance of visualisation of
relevant aspects. This demonstrator was also used on
data coming from practice covering several years of
shift plans providing useful insights.
The remainder of this work is structured as fol-
lows: section 2 describes the methodology of this
paper. section 3 presents the professional basis of
health-related aspects which are used for the technical
demonstrator described in section 4. Finally, section 5
comes with a conclusion and future work.
2 METHODOLOGY
The underlying research questions of the presented
work are the following two:
1. What health-related factors are relevant for the
preparation of shift plans?
2. How can the health-related factors for shift plans
be utilised (by technical means) to improve the
well-being of the care staff in care organisations?
A mixed-method approach was chosen, which in-
cluded literature research, qualitative surveys and ele-
ments from prototyping. The literature study accord-
ing to the method vom Brocke (vom Brocke et al.,
2009) started with a research on the applicable le-
gal regulations in the field of shift plans. Relevant
national and international labour laws and regula-
tions that deal with health aspects in relation to shift
plans were examined. In parallel, occupational sci-
ence sources and recommendations were evaluated in
order to create a comprehensive basis for the further
research steps.
Following this literature review, a qualitative ap-
proach was chosen to systematically answer the re-
search questions. The research method is made up of
the following steps:
1. Semi-standardised interviews were conducted to
determine the approach the persons responsible
for shift scheduling were taking and to identify the
requirements for shift planing from the staff. This
allowed for comprehensive data collection and in-
clusion of the practice perspective.
2. The interviews also included questions about cur-
rent technical support for service planning. This
helped to understand existing software solutions
and their use in the context of the care sector.
3. A detailed analysis of non-digital shift plans from
practice provided by care organisations was car-
ried out to identify further criteria for shift plan-
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
122

ning and fulfilment of the health aspects men-
tioned by the interview partners.
4. The findings were reflected with the interviewees
to ensure that the requirements and factors identi-
fied meet the needs of the practice.
5. A set of rules was formulated based on the find-
ings from the interviews, from the review of non-
digital shift plans and from the legal regulations
found in the literature review. These rule sets were
to serve as a basis for the development of the soft-
ware demonstrator that can transparently present
the health aspects in shift plans.
6. Common shift plan applications were examined
and discussions were held with manufacturers of
shift plan software in order to get to know relevant
functions and find out to what extent shift plan
design is already supported by automation and the
use of artificial intelligence (AI).
7. Criteria, requirements, rules and minimum func-
tionality for a demonstrator were fixed.
8. Based on this, a prototype demonstrator was then
specified and developed according to the pro-
totyping method by Pomberger (Pomberger and
Weinreich, 1994).
9. The result is a software demonstrator as a proof
of concept for sensitisation and motivation, which
analyses the aspects of healthy working within
shift plans and displays rule violations both in
a detailed and summarised manner as a global
“health score".
10. For a qualitative evaluation, V1.0 of the demon-
strator was presented to care experts, care organ-
isations and software manufacturers in online ap-
pointments and feedback was received.
11. Based on the feedback, V2.0 of the demonstrator
was developed and deployed as a public available
online tool for dissemination of the results.
3 HEALTH-RESPECTING
PERSPECTIVES
As already described, employees demand reliability,
a fair workload, individualisation and personal flex-
ibility. The facility itself expects compliance with
the personnel budget, economical use of working
hours, quality management and minimum legal re-
quirements, as well as minimal planning effort (Her-
rmann and Woodruff, 2019). Due to the importance
of duty scheduling in terms of keeping employees
healthy and in the care context additional of shift
work, framework conditions are recommended and in
some cases regulated by law. The most relevant as-
pects are presented in the following subsections. They
provide the basis for health-respecting shift plans and
are utilised by the technical implementation in sec-
tion 4.
3.1 Rules Derived from Laws
The legal framework for the organisation of working
time is of great importance for the protection of em-
ployees’ working conditions and for ensuring a bal-
anced relationship between work and rest. German
law is the focus of this subsection due to the fact, that
the context of our work is the German care sector and
that all of our interview partners and data providers
are from Germany. The most important law in this
respect is the Working Time Act (Arbeitszeitgesetz -
ArbZG) (Bundesministerium der Justiz, 2020). Ac-
cording to § 1 the purpose of the law is to ensure
the safety and health protection of workers. It limits
working time in Germany to eight hours per working
day. An extension to up to ten hours is permitted un-
der certain conditions. Employees may work a max-
imum of 48 hours per week. However, a 30-minute
rest break must be granted after six hours of work at
the latest, unless the total working time is less than
nine hours. If the working time exceeds nine hours,
it is 45 minutes. The rest break can be divided into
sections of at least 15 minutes each. In addition to
rest breaks, the law provides for a daily rest period of
eleven hours. This means that there must be at least
eleven hours between two work assignments. Special
provisions apply to night work. Night work within
the meaning of the Act is work that is predominantly
performed between 23.00 and 6.00 o’clock.
With regard to a limit on consecutive working
days, the German law does not provide for an explicit
maximum limit. The limit is set by other provisions,
such as Sundays off, and was limited by the Euro-
pean Court of Justice to a maximum of 12 consecu-
tive working days (Court of Justice of the European
Union, 2017).
Working time arrangements in the care sector are
particularly affected by exemptions in the law. Col-
lective agreements may go even further. For example,
it is possible to reduce the rest period to ten hours.
The laws in Germany and the other member states
of the EU are directly influenced by the European
Parliament and Council. In the Council Directive
2003/88/EC (European Union, 2003), the EU de-
fines minimum requirements for the organisation of
working time, including minimum periods of daily
rest, weekly rest and annual leave, breaks, maximum
Health Scores for Generating Health-Respecting Shift Plans by Means of an Expert System from the Perspective of Care Organisations
123

weekly working time, and certain aspects of night
work, shift work, and patterns of work. Regarding
rest time the directive states that every worker is enti-
tled to a minimum daily rest period of 11 consecutive
hours per 24-hour period. A maximum average work-
ing time of 48 hours per week, including overtime is
also specified. The directives remain unspecific re-
garding breaks and refers to agreements between the
employers and employees or by national legislation.
In the USA, the Fair Labor Standards Act (FLSA)
is the federal law that regulates working hours (U.S.
Department of Labor, nd). According to the FLSA,
employees must receive at least the minimum wage
and may not be employed for more than 40 hours in
a week without receiving at least one and a half times
their regular pay rate for any hours worked over 40.
There is no federal or state law on limits to the length
of the working week, but the FLSA creates a finan-
cial disincentive to longer working hours by requiring
time and a half pay for employees working more than
40 hours in a week.
3.2 Rules Derived from Official
Recommendations from Authorities
In addition to the various legal requirements, there are
other scientifically based recommendations for work-
ing and rest times, breaks and shift work coming from
official authorities. In Germany, it is stipulated by law
that reliable scientific findings must be taken into ac-
count when dealing with working hours (§ 6 (1) Ar-
bZG) (Bundesministerium der Justiz, 2020).
With regard to working hours, a working time
of 8 hours is generally recommended (BAuA, 2016).
However, splitting shifts into two separated, shorter
shifts with a long break, which is usually not spend at
the workplace, between the two shifts, should also be
avoided (Beermann et al., 2019). Consecutive work-
ing days should also be limited, and a rest day should
be planned after 5 days (Beermann et al., 2019),
whereby individual interspersed rest days should be
avoided (BAuA, 2021) to ensure recovery (Wong
et al., 2019).
With regard to the shift work required in car-
ing, labour science recommends a forward respective
clockwise rotating shift sequence. This means that a
phase of early shifts should be followed by a phase
of late shifts, then night shifts and finally days off,
whereby the number of night shifts should be a maxi-
mum of 3 nights (Burgess, 2007; BAuA, 2016).
Other recommendations do not directly address
working time and shift planning, but concern the han-
dling of the shift plans or the organisation of avail-
able staff. Occupational science findings emphasise
the design of a better shift work. In addition to rec-
ommendations on the lengths of shifts, the rotation
from early to late and night shifts as well as the shift
sequence, the regularity and predictability of work-
ing hours are emphasised (Knauth and Hornberger,
1997; DGAUM, 2020; BGW, 2006). Especially the
plans should be predictable and plannable in order
to improve the work-life balance (Beermann et al.,
2019). Insufficient predictability of work and leisure
time leads to increased subjective health complaints
and increased dissatisfaction with own working time
arrangements (Engel et al., 2014). In this context, a
health-promoting shift plan plays an important role.
A shift plan that is based on science recommendations
and putting the needs of the employees can have a
positive impact in their satisfaction, mental and phys-
ical health, and the quality of care. A very important
aspect is the absence of changes at short notice, which
also has been confirmed to be a success criterion when
recruiting and retaining employees (Gaugisch et al.,
2017). There is no uniform opinion on the appropri-
ate lead time a shift plan should be developed and pro-
vided to the staff. Guidelines in other countries were
only found in isolated cases; the Formula Retail Em-
ployee Rights Ordinances in San Francisco, for ex-
ample, stipulate a binding two week advance notice
of work performance for certain companies (City and
County of San Francisco, 2015).
3.3 Rules Derived from Other Sources
and Interviews
In addition to the legal framework and official recom-
mendations, there is further literature on guidelines
for the design of shift plans.
A shift plan is used to regulate both the staffing
requirements and the actual deployment of staff in
care facilities. It is intended to ensure that the work-
flow is efficient, of high quality and satisfactory for
both the persons being cared for and the care worker
(Birkenfeld, 2000). Care workers have clear expec-
tations of an effective shift plan, which can be clas-
sified into the categories of reliability and planning
security, fairness, individualisation and personal flex-
ibility (Herrmann and Woodruff, 2019). In terms of
reliability and planning security, they expect, for ex-
ample, punctual closing time, regular weekends off
every 14 days and an early announcement of the shift
plan. A well-designed shift plan should also be able
to accommodate staff absences without people having
to fill in for sick colleagues at short notice or having
to work on non-working days.
In a study by the German Professional Associa-
tion for Nursing Professions (DBfK, 2019) the staff
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
124

also demand sufficient staff to adequately cover the
workload and that it should be binding at least four
weeks in advance.
In addition, the integration of buffers for short-
term staff absences is important in order to maintain
the quality of patient care. The reliability of the shift
plan is crucial and it is desirable to take individual
preferences into account.
In a collection of good practices (BGW, 2006),
measures were identified that elderly care facilities
implement with regard to labour logistics. With refer-
ence to duty scheduling, the establishment of a pool
of temporary staff is mentioned in order to ensure the
aforementioned reliability of the shift plan and to re-
duce the need to call staff in from off duty. Here too,
early provision of the plan (4 weeks) is discussed,
although in the interviews conducted as part of the
project, organisations even aim for 6 weeks in ad-
vance. In terms of shift planning, the facilities are
aiming to reduce work peaks and avoid split shifts.
In order to supplement these aspects from litera-
ture, interviews with shift planners were conducted
as part of this work. In the interviews, it was fre-
quently mentioned that employees’ wishes are con-
sidered when planning shifts. It has been confirmed
that this leads to greater acceptance of the sched-
ules and increases satisfaction. There is limited aca-
demic research specifically on the impact of consid-
ering employee wishes in shift planning on employee
health. However, there is research that suggests that
flexible work arrangements, which can include shift
scheduling, can have positive impacts on employee
well-being and health. For example, a comprehen-
sive review of shift working nurses concluded that
factors including control over shift patterns are cru-
cial factors in achieving work-life balance (Dall’Ora
and Dahlgren, 2020). Care workers want that the shift
plan takes their individual time needs into considera-
tion, for example a shift plan that can be integrated
into their rhythm of life (Herrmann and Woodruff,
2019; Kubek et al., 2019; Schmucker, 2019).
Some of these aspects were simply confirmed by
the conducted interview of us, but there were also ad-
ditional aspects and also relevant conflicts arise. Of
such conflict is that some employees’ wishes contra-
dict official recommendations or even legal require-
ments. For example, employees occurred in the inter-
views who work more than 3 days in a row at night in
order to have more time off afterwards. Others prefer
to work longer shifts (e. g. 10 hours) in order to have
more time off afterwards. This creates a conflict, at
least between the finding that taking wishes into ac-
count increases satisfaction, but according to current
findings the work is more stressful as a result.
In the interviews, various groups of people in their
organisations were identified for whom special con-
ditions and facilities apply. Employees with chil-
dren get more flexibility in the start and end times of
their shifts, which are adapted to school and childcare
times. For employees whose partners also work shifts,
their own working hours are adapted to their partner’s
so that working hours are as similar as possible and
free time can be spent together. Older employees are
offered shorter shifts or, if their working time account
allows, more consecutive days off.
In terms of other organisational aspects, full-time
employees tend to be given longer shifts to ensure
days off. For this reason, full-time employees are of-
ten scheduled first in the shift plan. Part-time employ-
ees are therefore often given slightly shorter shifts. A
special feature applies to the planning of holidays: an
attempt is made to schedule either an early shift be-
fore a desired holiday, or a late shift after the holiday,
or even a whole day off is scheduled to extend the
holiday.
The full list of health-related rules based on
employee-wishes for shift planning derived from the
conducted interviews is given in the following:
■
Early duty should be preferred on last working
days before holidays, if possible.
■
Late shifts should be preferred on first working
days after holidays, if possible.
■
Part-time workers have shorter shifts.
■
Full-time workers have longer shifts.
■
Free days are appended to holidays, if possible.
■
Shift plans of partners should be respected.
■
Times of day care centres and schools are re-
spected for care workers with (small) children.
■
Older care workers have shorter shifts.
■
Older care workers have preference consecutive
free days.
■
Shift plans should plan with net time, i. e. their
working time minus holiday times, training times,
and other predictable peculiarities.
■
Holiday planning can be finalised in December of
the last year.
■
A certain amount of wishes is respected per
month, if possible (e. g. two per month).
■
Individual needs are respected such as certain
times to bring children to their sport locations.
■
Wishes about night shifts are respected in particu-
lar.
■
Wishes can be registered until the 15th of the pre-
vious month.
Health Scores for Generating Health-Respecting Shift Plans by Means of an Expert System from the Perspective of Care Organisations
125

In practice, it usually is not possible to respect all
rules, especially when considering a multitude of in-
dividual living conditions and wishes. But trying to
respect the needs of the care workers as good as pos-
sible is both, expected and valued by the concerned
care workers.
In terms of reliability, the planers have paid par-
ticular attention to outage management. For example,
one organisation has a buffer of day workers who are
willing to cover night shifts. In addition to pools of
temporary staff, there are also resource services that
can be called upon at short notice. And finally: Stand-
ing in is usually rewarded with attractive compensa-
tion, such as an extra weekend off. The full list of
outage rules derived from our interviews is as follows:
■
Part-time workers are preferred for standing in.
■
Care workers which stand in often get a fair com-
pensation, e. g. additional free weekends.
■
There should be a reasonable amount of buffer
care workers for night shifts.
■
When organising buffers, the level of training
should be taken into account.
■
A resource service should be used for structured
outage management, i. e. care workers which
check whether they are needed or not at the be-
ginning of the day. If not, they get a compensa-
tion for staying ready, e. g. one hour of work time
noted.
3.4 Stakeholders and Their Interests
After investigating the health-related factors of shift
planning (research question 1, cf. section 2), the ques-
tion arises how these insights can be utilised (research
question 2). With already numerous law-based rules,
it is unrealistic that planners can respect the multi-
tude of health-related rules manually in a reasonable
amount of time. Therefore, the target is a software
support in form of an extension of the already used
planning tools. To this end, a software demonstrator
was implemented (cf. section 4) for sensitisation of
the main stakeholders, i. e. care workers as the most
affected group of persons, planners as those having to
create the shift plans with various requirements, em-
ployee representative committees as those, caring for
the fulfilment of many requirements to shift plans, and
last, but not least, software providers as those which
have the basis to implement the means to bring the
insights of this work to practice.
This last subsection is about the two stakeholder
groups which are most probably the main users of the
potential software support, i. e. planners during gener-
ation and employee representative committees (such
as work councils) as verifying instances. The demon-
strator was designed having these two user groups in
mind.
The works councils have a right of co-
determination with regard to duty scheduling in Ger-
many (Bundesministerium der Justiz, 2022). They
pursue various interests with regard to duty schedul-
ing, with the aim of creating a balanced and fair work-
ing environment. A central concern is to promote
the work-life balance of employees by carefully or-
ganising working hours. In doing so, the representa-
tive office emphasises compliance with working time
laws and collectively agreed provisions. Another fo-
cus is on protecting the health of employees. Duty
scheduling should be designed in such a way that suf-
ficient breaks and appropriate rest periods are taken
into account in order to avoid overwork. At the same
time, the employee representatives are committed to
involving employees in the duty scheduling process
in order to better take their needs and preferences into
account. Representation also aims to distribute the
workload fairly and ensure that employees’ qualifi-
cations and competences are appropriately taken into
account. This is not just about avoiding overwork,
but also about promoting efficient work performance.
The employee representatives are in favour of flexi-
bility in duty scheduling to make it easier to combine
work and family life. The introduction of flexible
working time models plays a key role here. Trans-
parency and open communication between employer
and employees are further key concerns in order to
recognise and resolve potential problems at an early
stage. Overall, the employee representatives strive for
balanced duty scheduling that not only fulfils opera-
tional requirements but also focuses on the needs of
employees.
Planning shifts is a major challenge for the mid-
dle care management, as it requires them to take into
account individual wishes, staffing requirements and
compliance with legal, collective bargaining and er-
gonomic standards. In the "Game of Roster" project
(GamOR), a digital collaborative shift planning sys-
tem was developed for care workers that motivates
employees to participate in the shift planning process
(Kubek et al., 2020). In the requirements analysis,
shift planners complained above all about the amount
of time it takes to create shift plans. Those responsi-
ble for duty scheduling are regularly confronted with
several conflicting objectives when it comes to tak-
ing into account legal and economic requirements, er-
gonomic findings and individual wishes. In addition,
economic requirements to plan shifts with only a min-
imum number of staff and the high sickness rate of
employees lead to time-consuming shift plan changes
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
126

at short notice (Kubek et al., 2019). Therefore, it is
helpful for the shift planner to be provided with all
information in a clear and transparent manner. This
includes information on where legal requirements or
requirements found in scientific sources on healthy
working. The plan could then be adapted and the up-
dated result could be showed immediately.
Another added value for the planners is, that with
a tool support for rules and wishes, they have concrete
data about the care workers which can not only be
used to ensure fairness, but also to communicate on a
solid basis.
With these use cases and target groups in mind,
a technical software demonstrator was developed,
which is the subject of the following section.
4 DEMONSTRATOR FOR
HEALTH-RESPECTING SHIFT
PLANNING
The sheer number of different rules makes it ex-
tremely difficult to respect them all as a human plan-
ner during shift plan generation. Even though shift
plan generation by means of a planning software has
become standard (cf. section 1) over the last years, the
majority of such tools provide assistance, but hardly
any automation to their users (Petrovic, 2019). Given
the assisted process of shift plan generation, trans-
parent visualisation of rules and their compliance be-
comes an important feature of these assisting systems,
since otherwise their users have to care about rule
compliance, manually check them during the genera-
tion process, or check in the end and adapt an already
finished shift plan again when compliance problems
are found.
Unfortunately, existing tools only provide assis-
tance regarding a small amount of the rules described
in section 3. Usually, the rules given by law are
mainly covered, the others not. This may be because
software in this area rarely profits from developed
models and methods (Petrovic, 2019).
With the goal of sensitisation by showing what can
be done and how it can be implemented, a techni-
cal software demonstrator was developed. This sec-
tion presents this demonstrator to show how health-
related rules beyond laws could be implemented and
visualised during the process of shift plan generation.
The demonstrator is freely available in the internet
(Kutzias et al., 2022).
4.1 Rule Violations and Health Score
When going beyond the law-based rules, it becomes
unrealistic to always fulfil all different rules all the
time for all care workers. This has been confirmed by
the conducted interviews, the literature (cf. section 1)
and the analysed data from practice. In such a situ-
ation, a measure of quality for evaluation and com-
parison of different shift plan time intervals can help
the responsible persons to keep track of the quality of
their shift plans during generation.
Different rules can differ heavily in relevance.
Therefore, a simple count of rule violations, which
cannot grasp such differences, is not the best measure.
In addition, some rules can conflict and also their rel-
evance can be based on individual preferences. Par-
ents, for example, might optimise their time together
with their children at the cost of ignoring other health-
related aspects. Time with the children can also be a
health-relevant factor, which can also heavily affect
the well-being of a human (Milkie et al., 2010).
Whereas a total count of (weighted) rule viola-
tions is interesting information, the relation of vio-
lations and the amount of work might be even more
helpful. Even on a per-person level, this might be very
important, e. g. for part-time care workers. Based on
these considerations, the following requirements for
such a measure were derived:
1. Violations should be relative to the amount of
work performed.
2. Rules should have a configurable relevance.
3. Individual preferences should be respected.
4. The measure should be intuitively understandable
and comparable.
A concrete measure - namely "health score" - is
proposed to be able to compare shift plans regarding
their health-related quality based on the four require-
ments mentioned above. The basis is the number of
shifts defining the maximum number of quality points
which is achievable (Requirement 1). For all occur-
ring violations, the penalty points are summed up re-
specting possible differences depending on the care
worker for which the violations occur (Requirement
2 and Requirement 3). Based on these two values, a
ratio is used to calculate a value between 0 and 100
to indicate the quality of the shift plans (Requirement
4). In the following, a more detailed and formal defi-
nition of this value, the health score, is given.
Definition 1 (Health Score). Let S be the set of shifts
in the corresponding shift plan, C the set of avail-
able care workers and V the set of violations with
c
v
∈ C the corresponding care worker for each vio-
lation v ∈ V and p : V ×C → N
0
the function assign-
Health Scores for Generating Health-Respecting Shift Plans by Means of an Expert System from the Perspective of Care Organisations
127
ing the penalty to a violation in combination with a
concrete care worker. w is a constant weight for the
shifts, which can be fixed for application. Then the
health score HS is defined as:
HS = max
0, 100 ·
|S| · w −
∑
v∈V
p(v, c
v
)
|S| · w
Since the penalty points are flexible, it is no re-
striction to fix a constant weight of points per shift.
This constant weight value should simply be chosen
high enough for the desired possible relation of the
different rules (as long as staying with integers) and
granularity of the violation point definition. Since
the sum of penalties can exceed the number of maxi-
mum points, a minimum of 0 is set by using the max-
imum function, so that the desired interval of [0, 100]
is achieved.
4.2 Technical Implementation
To show how health-respecting shift plan generation
can look like, a technical demonstrator was devel-
oped. It consists of the following main functionali-
ties: a calendar for shift plan generation, care worker
management with master data, a configurable rule set
for health score calculation, a measurement engine
for shift plan evaluation and health score calculation,
and a visualisation of rule violations and the health
score. This subsection gives a concise description of
the demonstrator and its implementation of the previ-
ously mentioned aspects.
Web technologies were used to provide an easy
Internet access: the server back-end was implemented
using Node.js with express as the webserver. On the
front-end side, jQuery and jQuery UI were the main
frameworks for implementation.
Since it is meant to be a demonstrator, not a soft-
ware product for sale, some restrictions were made:
■
Only a subset of identified rules were imple-
mented.
■
Only single source violations were visualised di-
rectly in the calendar.
■
Due to data protection reasons, fictional data was
used for public show cases.
■
For simplicity, rule configuration is made on shift
plan instead of care worker level.
The health score was implemented with w = 15
resulting in a maximum number of 15 times the num-
ber of shifts. Due to the rule configuration handling,
violation penalties are calculated per rule type.
For the available care workers, master data is re-
spected such as date of birth, hours per week, level
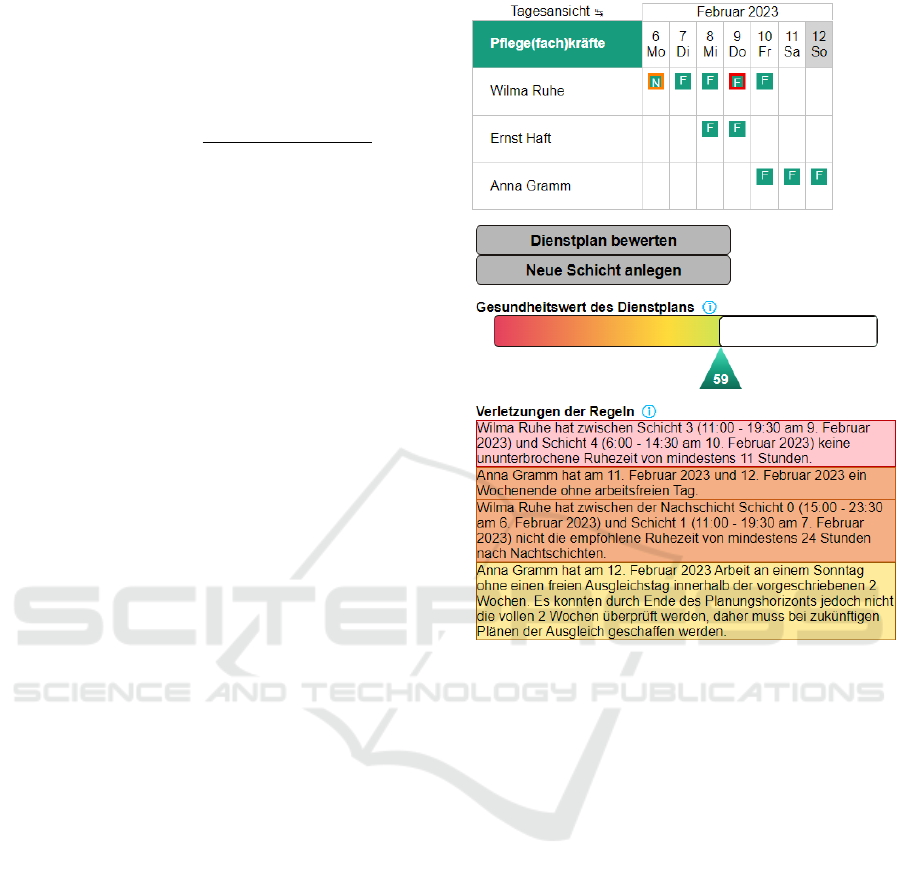
Figure 1: A small sample shift plan in the demonstrator
for one week with several rule violations. Red is used for
law rule violations, orange is used for official recommenda-
tion rule violations and yellow for unofficial rule violations.
This sample sums up to a health score of 59, indicated by
both, by the number under the bar and the filling of the bar.
of training, several pregnancy-related data, and law-
based special permissions for youth work. For per-
formance reasons, rule checking is not done automat-
ically on each and every change in the shift plan, but
on button click: the shift plan is sent to the server
which calculates rule violations and sends them back.
These rule violations are then visualised in the calen-
dar, in a percentage-based filled bar with the health
score and a list of all violations given beneath the bar.
A sample of the demonstrator with an already checked
shift plan with three care workers and a time interval
of one week can be seen in Figure 1.
In addition to the online functionalities, a module
was implemented for automatic processing of larger
data sets for analysing real data. This module is not
part of the online demonstrator to avoid contract data
processing issues. It was used for analysing data cov-
ering several years coming from practice using the
same rule set and code as the online demonstrator
uses.
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
128

4.3 Rules and Violation Visualisation
When rules are implemented in software, questions
about the user interface and the presentation arise.
Immediate visual feedback is only possible by live
evaluation and presentation. In addition, it is advis-
able to visualise rule violations as close as possible to
the shifts and care workers related to the violations,
to enable planners to efficiently locate violations and
react to it.
To be able to visualise rule violations inside a
planning tool with a calendar, different rules were
grouped by their relevant time intervals in the follow-
ing way:
■
Single Source Violations: Violations caused
within a single work shift are the most simple
class and can be visualised by highlighting the re-
lated shift or day. An example for this can be seen
in Figure 2.
■
Multi Source Violations: Violations caused
across several shifts or days can, for example, be
visualised by overarching visual elements for con-
secutive elements such as a coloured overlay bar
for a few days or by simply highlighting all single
elements, presenting their unity by changing the
highlighting of all of them on hovering over one
of them.
■
Long Interval Violations: Violations which are
related to days and shifts with large time differ-
ences are hard to visualise in a calendar. One pos-
sibility, for example, would be by highlighting the
care worker or some kind of list next to the plan-
ning area.
A concrete delimitation between multi source vi-
olations and long interval violations was intentionally
not defined, since the meaningfulness of such a def-
inition might depend on the concrete use case and
software. It could be meaningful to define it simply
by consecutiveness, a number of days between the
earliest and the latest (e. g. seven), or count every-
thing exceeding the boundaries of the current month
as a long interval violation. The last definition would
be meaningful, since many enterprises generate their
shift plans in a monthly fashion according to the gath-
ered shift plan data and the conducted interviews.
This results in calendar views showing single months
in many planning tools.
4.4 Analysis of Historical Shift Plan
Data
According to the methodology described in section 2,
the demonstrator was used for sensitisation and col-
Figure 2: An example for the visualisation of a single source
violation. The leftmost cell represents a single day with a
shift without any violations, the second left represents a day
with a shift with a single source violation and on the right
the same cell is shown with a hovering effect. A block in
a cell representing a day with an "F" denotes an early shift
that day.
lecting feedback from providers of shift planning
software and users from care organisations. Espe-
cially, the the care organisations which assisted as
providers of shift planning data from practice re-
ceived a demonstration in conjunction within the last
interview-session.
A data set covering several years was evaluated
for investigating trends over several years using the
example of one care organisation. Four years of shift
plan data (September 2018 to October 2022) was re-
ceived. Data from planned as well as actual shifts
from 53 care workers was analysed using the demon-
strator. Surprisingly, the differences between planned
and actual shifts showed a comparably small amount
of differences in rule violations. However, there was
a relevant amount of rule violations overall. On the
positive side, it was shown that the health score was
trending upwards, i. e. the overall amount of rule vio-
lations decreased over time, starting with round about
40 going up and staying around 90 over the last two
years. On the other hand, several health-related rules
had an upwards trend in the amount of related viola-
tions as described in the following:
■
Required free compensation days for work on
Sundays within the following two weeks had an
upwards trend in violations ending with roughly
0.36 violations per care worker per month.
■
The recommendation that at least one day should
be free of work on weekends was often violated
with an upwards trend ending at 2.32 violations
per care worker per month.
■
The recommendation that not more than five days
per week should be used for work had an upwards
trend in violations ending with 1.53 violations per
care worker per month.
When analysing the average rule violations per
care worker per month, it was observed that individual
care workers had up to a factor of five times as many
violations as the average of all care workers. Even
though the cause is not confirmed, it may be due to
the "yes-person" character of those care workers.
These insights affirmed what has been stated in
Health Scores for Generating Health-Respecting Shift Plans by Means of an Expert System from the Perspective of Care Organisations
129

the literature several times: the working conditions
in the care sector have much room for improvement.
The care organisations were surprised by several of
the numbers and trends in the feedback discussions,
especially about the individual persons with drastic
violation peaks.
The analysis of data from practice gave insights
about possible reasons for problems of the health
sector such as the sickness rate and dissatisfaction
of many care workers. These insights in combina-
tion with the used techniques (health-related rules,
health score, visualisation during shift plan genera-
tion) could be utilised by commercial software tools
to balance the health related aspects in practice to
achieve more fair and healthy work conditions.
5 CONCLUSION AND FUTURE
WORK
Shift planning was analysed regarding health-related
aspects. In addition to existing law-based rules and
official recommendations, further recommendations
were derived from interviews with care workers. The
majority of different rules is far from being respected
in practice and often there are large balancing issues
between different care workers, as both, the inter-
views and the analysis of several years of shift plan
data show. To be able to measure shift plans with re-
spect to these health-related rules, a health score was
formally defined.
In order to prepare the next step by sensitising and
showing how it can be done, a software demonstra-
tor was developed as a publicly available web-tool,
which implements many of the discussed rules and
shows how they could be utilised by or being inte-
grated into software planning tools. The demonstrator
received a lot good feedback during the feedback ses-
sions with the interview partners, showing the need
of the planners in practice. Software providers were
more reserved, but also interested.
Besides bringing the health-related rules to soft-
ware planning tools and making the shift planning
process more fair and transparent, further interesting
research and development steps were considered.
Given the challenge of shift planning with a mul-
titude of different (health-related) rules to consider, a
next logical step would be to (partially) automate the
process of shift plan generation. Since the general
problem of generating optimal shift plans with given
restrictions is too hard to reliably compute optimal so-
lutions, at least with the current state-of-the-art (it is
an NP-hard problem (Aickelin and Dowsland, 2000)),
approximations are the main way to solve the prob-
lem. AI can be utilised to calculate such approxima-
tions. For this step to be done, a large amount of his-
torical data is likely to be required. Given the amount
of rule violations in practice, current data should not
be used in an unlabelled way if the health-related as-
pect is to be respected, i. e., for given shift plans, a
quality measure either as a number or clear category
is needed. Such data is hard to acquire, since usu-
ally, hardly anyone cares about rating past shift plans.
The proposed health score presented in this work is
a quality measure which could be used for providing
such a rating by automatically processing past shift
plans, but it depends on making the decisions about
the configurable weights in a generic manner. Further
research on this end could help to automate the shift
plan generation process.
Additionally, more simple local automation steps
could be implemented such as searching for possible
local swaps and offering them to the planners, but this
limited approach cannot guarantee to provide valid lo-
cal solutions, if none exists. Nevertheless, using such
an approach with comparison of local swaps (for ex-
ample, using the health score), a suggestion system
can be implemented to assist in doing fast adaptions.
Such a system would especially be meaningful for re-
quired short-term-adaptions, possibly caused by sick-
nesses of care workers.
ACKNOWLEDGEMENTS
The acquisition of the used data as well as the im-
plementation of the demonstrator were performed
within the German project »Regionales Zukunftszen-
trum „pulsnetz.de - gesund arbeiten”« funded by the
Federal Ministry of Labour and Social Affairs.
REFERENCES
Aickelin, U. and Dowsland, K. A. (2000). Exploiting
problem structure in a genetic algorithm approach to
a nurse rostering problem. Journal of Scheduling,
3(3):139–153.
AOK-Bundesverband (26.04.2023). Krankenstand in der
Pflege: Anstieg um mehr als 44 Prozent in elf Jahren.
BAuA (2016). Handbuch zur Handbuch Gefährdungs-
beurteilung „Arbeitszeit“. Bundesanstalt für Ar-
beitsschutz und Arbeitsmedizin (BAuA).
BAuA (2021). Handbuch Gefährdungsbeurteilung - Teil 2:
10 Arbeitszeitgestaltung. Bundesanstalt für Arbeitss-
chutz und Arbeitsmedizin (BAuA).
Beermann, B., Backhaus, N., Tisch, A., and Brenscheidt,
F. (2019). Arbeitswissenschaftliche Erkenntnisse
zu Arbeitszeit und gesundheitlichen Auswirkungen.
baua: Fokus.
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
130

BGW (2006). al.i.d.a - Arbeitslogistik in der stationären
Altenpflege - Projektabschlussbericht.
Birkenfeld, R. (2000). ABC der Dienstplangestaltung: Ar-
beitszeitflexibilität und neue Arbeitszeitmodelle im
Gesundheitswesen.
Bundesministerium der Justiz (2022). Betriebsverfassungs-
gesetz.
Bundesministerium der Justiz (22.12.2020). Arbeitszeitge-
setz: ArbZG.
Burgess, P. A. (2007). Optimal shift duration and sequence:
recommended approach for short-term emergency re-
sponse activations for public health and emergency
management. American Journal of Public Health, 97
Suppl 1(Suppl 1):S88–92.
City and County of San Francisco (2015). Formula Retail
Employee Rights Ordinances.
Court of Justice of the European Union (2017). The weekly
rest period for workers does not necessarily have to
be granted the day following six consecutive working
days: Press Release No 115/17 to Case C-306/16.
Dall’Ora, C. and Dahlgren, A. (2020). Shift work in nurs-
ing: closing the knowledge gaps and advancing inno-
vation in practice. International journal of nursing
studies, 112:103743.
Daum, M. (2022). Die Digitalisierung der Pflege in
Deutschland: Status quo, digitale Transformation und
Auswirkungen auf Arbeit, Beschäftigte und Quali-
fizierung. DAA-Stiftung Bildung und Beruf, Ham-
burg.
DBfK (2019). Ergebnisse einer Online-Umfrage zum ‚Di-
enstplan‘.
DGAUM (2020). Leitlinie "Gesundheitliche Aspekte und
Gestaltung von Nacht- und Schichtarbeit.
Engel, C., Hornberger, S., and Kauffeld, S. (2014). Organ-
isationale Rahmenbedingungen und Beanspruchun-
gen im Kontext einer Schichtmodellumstellung nach
arbeitswissenschaftlichen Empfehlungen — Spielen
Anforderungen, Ressourcen und Personenmerkmale
eine Rolle? Zeitschrift für Arbeitswissenschaft,
68(2):78–88.
European Union (2003). Directive 2003/88/EC of The Eu-
ropean Parliament and of The Council. Official Jour-
nal of the European Union.
Gaugisch, P., Risch, B., Strunck, S., and Willmann, R.
(2017). Pflegepersonalsurvey - Arbeitgeberattraktiv-
ität und Führungsmotivation in der Altenhilfe.
Herrmann, L. and Woodruff, C. (2019). Dienstplanung im
Stationären Pflegedienst: Methoden, Tools und Fall-
beispiele. Gabler, Wiesbaden.
Hirschwald, B., Nold, A., Bochmann, F., Heitmann, T.,
and Sun, Y. (2020). Chronotyp, Arbeitszeit und Ar-
beitssicherheit. Zentralblatt für Arbeitsmedizin, Ar-
beitsschutz und Ergonomie, 70(5):207–214.
Jacobs, K., Kuhlmey, A., Greß, S., Klauber, J., and
Schwinger, A., editors (2019). Mehr Personal in
der Langzeitpflege - aber woher?, volume 2019 of
Springer eBook Collection. Springer, Berlin, Heidel-
berg.
Knauth, P. and Hornberger, S. (1997). Schichtarbeit
und Nachtarbeit: Probleme, Formen, Empfehlungen.
Bayer. Staatsministerium f. Arbeit u. Sozialordnung,
Familie, Frauen u. Gesundheit, München, 4 edition.
Knieps, F. and Pfaff, H., editors (2022). Pflegefall Pflege?,
volume 2022 of BKK Gesundheitsreport. MWV
Medizinisch Wissenschaftliche Verlagsgesellschaft,
Berlin.
Kubek, V., Blaudszun-Lahm, A., Velten, S., Schroeder,
R., Schlicker, N., Uhde, A., and Dörler, U. (2019).
Stärkung von Selbstorganisation und Autonomie der
Beschäftigten in der Pflege durch eine digitalisierte
kollaborative Dienstplanung. In Bosse, C. K. and
Zink, K. J., editors, Arbeit 4.0 im Mittelstand, pages
337–357. Springer Gabler, Berlin, Heidelberg.
Kubek, V., Velten, S., Eierdanz, F., and Blaudszun-Lahm,
A. (2020). Digitalisierung in der Pflege: Zur Unter-
stützung einer besseren Arbeitsorganisation. Springer
Berlin Heidelberg, Berlin, Heidelberg.
Kutzias, D., Frings, S., Strunck, S., and Gaugisch, P. (2022).
pulsnetz Demonstrator: https://pulsnetz-demo.
iao.fraunhofer.de.
Milkie, M. A., Kendig, S. M., Nomaguchi, K. M., and
Denny, K. E. (2010). Time With Children, Children’s
Well–Being, and Work–Family Balance Among Em-
ployed Parents. Journal of Marriage and Family,
72(5):1329–1343.
Petrovic, S. (2019). “You have to get wet to learn how to
swim” applied to bridging the gap between research
into personnel scheduling and its implementation in
practice. Annals of Operations Research, 275(1):161–
179.
Pomberger, G. and Weinreich, R. (1994). The role of proto-
typing in software development.
Rohwer, E., Mojtahedzadeh, N., Harth, V., and Mache, S.
(2021). Stressoren, Stresserleben und Stressfolgen
von Pflegekräften im ambulanten und stationären Set-
ting in Deutschland. Zentralblatt für Arbeitsmedizin,
Arbeitsschutz und Ergonomie, 71(1):38–43.
Rothgang, H., Müller, R., and Preuß, B. (2020). BARMER
Pflegereport 2020: Belastungen der Pflegekräfte und
ihre Folgen, volume Band 26 of Schriftenreihe zur
Gesundheitsanalyse. BARMER, Berlin.
Schmucker, R. (2019). Arbeitsbedingungen in Pflege-
berufen: Ergebnisse einer Sonderauswertung der
Beschäftigtenbefragung zum DGB-Index Gute Arbeit.
In Jacobs, K., Kuhlmey, A., Greß, S., Klauber, J.,
and Schwinger, A., editors, Mehr Personal in der
Langzeitpflege - aber woher?, Springer eBook Collec-
tion, pages 50–59. Springer, Berlin, Heidelberg.
Strauß, R., Tisch, A., Vieten, L., and Wehrmann, J. (2021).
Hohe Anforderungen, wenig Ressourcen: Arbeit-
szeiten in der Alten- und Krankenpflege.
TK Die Techniker (11.05.2023). Zum Internationalen Tag
der Pflegenden: Krankenstand bei Pflegekräften auf
Rekordhoch.
U.S. Department of Labor (n.d.). Wages and the Fair Labor
Standards Act.
vom Brocke, J., Simons, A., Niehaves, B., Riemer, K., Plat-
tfaut, R., and Cleven, A. (2009). Reconstructing the
giant: On the importance of rigour in documenting the
literature search process. 17th European Conference
on Information Systems (ECIS).
Wong, I. S., Popkin, S., and Folkard, S. (2019). Work-
ing Time Society consensus statements: A multi-level
approach to managing occupational sleep-related fa-
tigue. Industrial health, 57(2):228–244.
Health Scores for Generating Health-Respecting Shift Plans by Means of an Expert System from the Perspective of Care Organisations
131
