
Adoption of Digital Health Technologies in Supported Living Services
Peter Elimian
1
, Ceyda Kiyak
2a
and Deniz Cetinkaya
1b
1
Department of Computing and Informatics, Bournemouth University, Poole, U.K.
2
School of Psychology, University of East Anglia, Norwich, U.K.
Keywords: Supported Living Service, Health Technology, Health Care, Medication Reminders.
Abstract: The adoption of digital health technologies in supported living services has shown great potential to
revolutionise the quality of support offered to service users who are predominantly adults with learning
disabilities and mental health conditions. Despite these potential benefits, the adoption of these technologies
in supported living services remains at a low level. Therefore, this study aimed to address this gap by
investigating the factors influencing the adoption of digital health technologies in supported living services.
The research employed a mixed-method approach, conducting a case study in two local supported living
services with a sample size of six participants, three from each service. Analysis of the collected data, utilizing
both descriptive statistics and thematic approaches, revealed that 83.3% of participants acknowledged
widespread acceptance of digital health technologies in the services. Notably, 66.7% highlighted the
prevalence of health monitoring and assistive technology devices, including blood pressure monitors, blood
glucose monitors, mobility scooters, and virtual assistants. Participants attributed the positive adoption
environment to facilitation factors such as enhanced funding, training initiatives, and organizational support.
Furthermore, most participants emphasized the essential need for a medication reminder app, expressing a
preference for an easy-to-use and user-friendly design.
1 INTRODUCTION
Adopting Digital Health Technologies (DHT) in adult
social care services can revolutionise care delivery for
residents and improve their quality of living (CQC,
2022). DHT aims to improve health and care services
as well as health systems (NIHR, 2022). One crucial
aspect where DHT has shown significant impact is
supported living services, which accommodates and
provides some level of care and support to people
with learning disabilities and mental health
conditions (NHS, 2021). Similarly, adopting care
technology in supported living services can promote
independence of the residents and reduce care
packages, which would eventually result in
considerable cuts in cost for the operators. As digital
health technologies become more accessible, there is
a growing interest in their potential to enhance the
quality of care and promote overall health and
wellness. However, despite the potential benefits,
there are also challenges to adopting these
a
https://orcid.org/0000-0002-9218-2248
b
https://orcid.org/0000-0002-1047-0685
technologies. The National Health Service in the UK
(NHS) Digital (NHS Digital, 2022) stated that
digitally excluded people have higher risks of being
left out of health and social care services.
Consequently, there is a need for further research to
understand the factors that influence the adoption of
DHT in supported living services and to identify
strategies for successful implementation.
Supported living housing is a service or scheme
that provides individuals with disabilities, or mental
health needs the opportunity to live as independently
as possible in their own homes or shared living spaces
with appropriate support (NHS, 2021). People who
live in supported living accommodations are called
service users. According to Health and Care
Professional Council (HCPC) (HCPC, 2018), a
service user is anyone receiving the care or support of
a professional registered with HCPC. Also, supported
living accommodation involves a housing service
which comes along with supervised support or care.
Although there is a close relationship between care
homes and supported living housing, one of the
Elimian, P., Kiyak, C. and Cetinkaya, D.
Adoption of Digital Health Technologies in Supported Living Services.
DOI: 10.5220/0012631300003699
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2024), pages 181-189
ISBN: 978-989-758-700-9; ISSN: 2184-4984
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
181

primary differences is that supported housing aims to
promote residents’ independence. According to NHS
(2021), supported living services suit service users
who want to avoid living in residential care.
DHT refer to a range of devices and applications,
such as mobile health apps, wearable devices, and
telehealth systems, that use digital technology to
support healthcare delivery and improve health
outcomes (NIHR, 2022). Despite the digital
transformation agenda suggested by the NHS, which
advised all health and social care providers to adopt
the use of digital platforms and technology in service
delivery, the level of adoption of DHT in supported
living services is still at a low level, especially in the
aspect of medication management.
The purpose of this study is to explore ways that
will ease the adoption of DHT in supported living
services by analysing the use of DHT in supported
living settings and examining the case studies to
identify barriers, facilitators and impact factors. The
two main research questions addressed in this study
are: 1) “What are the guidelines for adopting digital
health technologies in supported living services?” and
2) “How can the adoption of digital health
technologies enhance the quality of care in supported
living services?”.
The scope of this research covers only the
supported living services in Bournemouth in the UK,
with specific consideration of two services used as
case studies. The supported living accommodation
considered for this study is the supported living
housing for adults with learning disabilities and
mental health diagnoses. This study focuses on
adopting DHT in supported living services from the
perspective of the support team, mainly the service
managers and support workers.
This paper is organised into seven sections. This
section presents an introduction to the problem
domain and overview of the study. Section 2 presents
the literature review and Section 3 provides the
research methodology employed. Section 4 presents
the data analysis and results. Section 5 proposes a
sample system design for a medication reminder
mobile application to be used in supported living
services. Section 6 and Section 7 present the
evaluation of the study and conclusions respectively.
2 LITERATURE REVIEW
2.1 Use of DHT in Social Care
Adopting digital health technologies has several
benefits to users and the health and social care
system, which became very visible during the
COVID-19 pandemic (NIHR, 2022). The use of DHT
has shown evidence during the pandemic, of giving
more people access to healthcare, improving health
outcomes of users, and increasing the quality of
health and social care system by rapid decongesting
of hospitals (GOV.UK, 2022b). One of the examples
of DHT adopted in the UK is telecare, e.g., the use of
digital devices such as personal alarms and
monitoring systems in adult social care to help
majority of residents manage risk and promote safety.
The use of telehealth gained wide acceptance during
the COVID-19 pandemic, with the NHS launching a
video consultation service using video enhanced app
like Zoom to reduce the risk of infection via physical
contact (Hutchings & Morris, 2022; CQC, 2022).
The remarkable growth in the use of DHT in the
UK has introduced technology-enabled care (TEC),
which is the harmonisation of telecare, telemedicine,
m-Health, and eHealth services (NHS, 2022). The
convergence of these services produces an integrated
care system that will improve the quality of care
delivered in health and social care. According to
GOV.UK report (2022a), the digital transformation of
health and social care is a priority. The report
mentions that some of the transformation goals
expected to be taken include providing a solid digital
foundation for health and social care by ensuring that
integrated care systems are digitally mature,
promoting the independence of people by digitalising
health and social care channels, facilitate the adoption
of trusted DHT devices across the board and
providing relevant regulations in places to help
integrated care systems reach full adoption.
DHT has been a core part of patient management,
as it has increased access to healthcare services and
helped healthcare practitioners communicate better
within the system (NIHR, 2022). Hutchings and
Morris (2022) state that 87% of the public and 94%
of clinicians favoured video consultation for
scheduling health and care appointments when a
digital maturity assessment was conducted in
Scotland. However, despite the several benefits of
DHT to the NHS, data privacy and security concerns
were also raised (GOV.UK, 2022b). Subsequently,
learning is one of the critical areas of using digital
health solutions in NHS settings nationwide.
Another critical aspect of using DHT in the NHS
is the electronic prescription service (EPS) which
reduced the number of unsigned prescriptions to
pharmacies in the UK (Franklin et al., 2013). The
introduction of the NHS app is another beneficial
digital solution launched in 2019. The NHS app has
received many credits for playing a significant role
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
182

during the pandemic (Cassels, 2022). According to
the 2022 data, the NHS app had over 22 million users
and helped to manage over 1.1 million GP
appointments and generated over 140 million
vaccination passes. In addition, DHT has also been
beneficial in diagnosing and managing diseases
(NIHR, 2022). Also, evidence supports using DHT in
older residents to enhance their mental health in areas
such as fighting loneliness, promoting independence,
and improving moods (Leigh et al., 2020; NIHR,
2022). However, despite this benefit, there are
concerns such as low mood and fear of results from
using DHT which may become barriers to their use.
Another vital area where care homes have
implemented DHT is electronic health recording
(EHR). Using EHR systems across the UK showed
improved communications between care homes and
health centres, enhanced residents’ registrations, and
optimised access to residents’ health records (NHS
2022; Lapp et al. 2022). Another important aspect is
the use of assistive technologies. Sharif et al. (2018)
suggests that due to the ageing population in the UK,
many senior citizens in care homes require assistive
technologies to improve the quality of their lives.
Assistive technologies such as adaptive keyboards
and mobility aids benefit residents; and suggests that
user-centred research is vital in determining a
resident’s choice of assistive technology. Alzheimer
Society’s (2015) factsheet indicates that the
application of assistive technology in the care of
residents with dementia can help their daily living,
such as speech and cognitive functions.
2.2 Barriers and Challenges
DHT has been increasingly implemented in care
homes to support care delivery. These technological
interventions include telehealth, telemedicine,
telemonitoring devices, digital recording systems and
digital games for the residents’ leisure among others
(Shah et al., 2022). However, despite the benefits of
telemedicine and telehealth application in care
homes, privacy concerns and other barriers were
highlighted in the literature (McGee et al. 2020). One
of the main barriers to adopting DHT in supported
living services is the need for digital skills and
literacy among staff and service users. Cummins and
Schuller (2020) suggest that a low level of digital and
health literacy is a crucial barrier to adopting DHT in
health and social care settings. This issue is prevalent
among the elderly population in most cases. This
barrier could be addressed by providing training and
support for staff and service users to increase their
digital skills and literacy.
In addition, funding constraints, lack of IT
infrastructures, weak information governance and
interoperability issues have been highlighted to be
significant barriers to adopting DHT in social care
settings (Lennon et al., 2017). According to Vaportzis
et al. (2017), the complexity of operating most digital
health devices, especially with older residents, can
slow the adoption of DHT. Furthermore, ethical, data
privacy and security concerns are other barriers to
adopting DHT in the supported living service
(Whitelaw et al., 2021). This barrier can be addressed
by ensuring that DHT complies with data protection
regulations and that users have clear information
about how their personal information will be used.
2.3 Facilitators and Opportunities
Regarding the facilitators, user-friendliness and
personalised design to fit into users’ needs are
essential ways of easing the use of digital health
solutions (Whitelaw, 2021). Carrying out user
research before choosing DHT is essential as this will
promote the ease of adopting user-centred
technologies in social care.
Additionally, Tyrell (2021) highlights improved
funding as a primary facilitator because most digital
health solutions patients and residents use come with
a price. Therefore, proper reimbursement of clients
will encourage the adoption of DHT. Similarly,
Ainsworth (2021) mentions the need for accessible
funds to drive the digital transformation agenda in
social care and explains that NHS has set up a united
tech fund as part of the Who Pays for What (WPfW)
approach to fund social care players such as
supported living services.
Training programmes to upskill staff and
residents alike have facilitated the adoption of DHT
in care settings (Whitelaw et al., 2021). Adopting
strategies such as creating a robust IT infrastructure,
tackling interoperability issues, establishing a
practical framework for information governance can
help to increase the use of DHT in social care.
3 RESEARCH METHODOLOGY
3.1 Data Collection
We adopted a case study mixed method approach in
this research (Yin, 2014). In this research, we also
adopted the Technology Acceptance Model (TAM)
theoretical framework which models how users
accept, use and adopt a technology. We employed the
standard scientific research process that defines the
Adoption of Digital Health Technologies in Supported Living Services
183
steps for conducting research. This study was
conducted according to the ethical guidelines of
Bournemouth University in the UK. Two supported
living services in Bournemouth supported the study
at an operational level. Informed consent was
obtained from all subjects involved in the study.
3.2 Methods
The primary data collection for this study was done
using an online questionnaire distributed to the
participants from the support living houses via social
media platforms and emails after obtaining approval
from the participants. The online questionnaire was
designed using Google Forms as it is easy to use and
supports rapid analysis of responses at no cost.
Correspondingly, a mixed methods questionnaire
with 26 questions was designed to have open-ended
questions aimed at gathering qualitative data and
close-ended questions aimed at gathering quantitative
data. Combining qualitative and quantitative data
provides a broader and better perspective for a
researcher to delve into new insights.
After obtaining approval from the relevant
services, participants were provided with a link to the
online questionnaire between 25
th
March and 10
th
April 2023. The questionnaire consists of questions
about demographic information, the participants’
perceptions and experiences with DHT, the impact of
DHT on the quality-of-care delivery, medication
management, and the recommendation of features for
the design of a medication reminder app.
The convenience/purposive sampling method was
chosen for its appropriateness in capturing insights
from specific individuals within supported living
services who have direct experience with digital
health devices. Given the unique characteristics of
service users in supported living services,
predominantly individuals with learning disabilities
and mental health issues who require some level of
support from professional support workers (CQC,
2022; NHS, 2022). This targeted approach ensures
that the chosen participants possess valuable insights
into the impact of digital health technologies.
Table 1 shows the details about the participants’
roles. Eligibility criteria is as follows: participants are
above 18 years of age, they are members of the
support team, and they have worked with residents
that required digital support; the service must be
situated in Bournemouth, the UK and the service must
be regulated by the CQC (Care Quality Commission),
NHS or BCP council.
Table 1: Participants’ roles.
# of
participants
Role
Supported
living house 1
3 staff
members
Service Manage
r
Team leade
r
Su
pp
ort worke
r
Supported
living house 2
3 staff
members
Service Mana
g
e
r
Social worke
r
Support worke
r
3.3 Questionnaire Coding
In qualitative research, the purpose of coding is to
convert qualitative data into a convenient format for
analysis. A codebook is often used as an essential
component of this process, where codes are assigned
to each response option, and instructions are provided
on handling missing data and coding open-ended
responses. This study adopts a hybrid coding
approach which combines the deductive and
inductive coding approaches to analyse the
qualitative component of the mixed method
questionnaire results. The deductive codes involve
coding qualitative data around the themes drawn from
the literature review. The inductive coding uses
themes created from the answers provided by the
participants and can be used for qualitative and
mixed-method research (Swain, 2018).
4 RESULTS
The collected data was analysed by using a hybrid
approach combining statistical and thematic methods.
(Swain, 2018). The quantitative data was analysed
using statistical methods, while the qualitative data
was analysed using the thematic approach. To
simplify the analysis, the supported living services
have been assigned terms, with first supported living
service termed House 1 and second one as House 2.
4.1 Quantitative Data Analysis
The quantitative data was analysed by using Google
Forms’ inbuilt statistical analysis tool which
generates an immediate analysis of participant
responses. This section presents the quantitative data
provided by participants residing in House 1 and
House 2. Regarding the demographic information, all
six participants were over 18 years and females.
Among the participants, four of them have (66.7%)
more than 5 years of experience in supported living,
while two participants have experience ranging from
1 to 3 years.
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
184
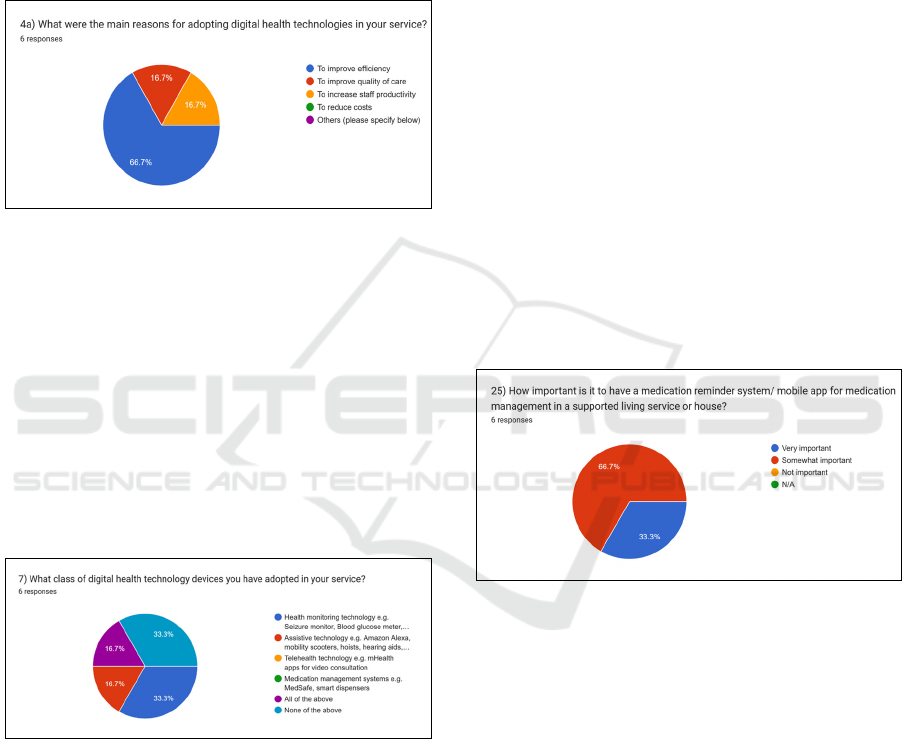
According to the results, four participants (66.7%)
acknowledged utilising DHT in their services while
the remaining two were uncertain. When questioned
about the reason for implementing DHT in their
respective services, participants selected the main
reasons being improving efficiency, improving
quality of care and increasing productivity. Figure 1
shows the presence of DHT and the motivation for
using it in their respective services.
Figure 1: The reasons for adopting DHT in the services.
Regarding the technology acceptance, 5 out of 6
participants (83.3%) agreed that service users widely
accept digital health technologies. This suggests that
there is no resistance to technology from the
residents.
After a thorough review of relevant literature, it
has been established that various classes and types of
DHT are being deployed in social care nationwide. To
better understand this, participants were questioned
about the types of DHT devices utilised in their
services as indicated in Question 7 and results are
shown in Figure 2.
Figure 2: Classes and types of DHT in supported living
services.
Regarding to the questions asking participants to
share any challenges they faced while adopting DHT
for their services and if they encountered difficulties
using DHT to improve care delivery, 66.7% of the
participants reported that they did not experience any
barriers during the process, yet they agreed that
certain factors have contributed to implementing
DHT in their services where they listed the specific
factors in the qualitative data. In terms of the quality
of care, all participants agreed that adopting DHT in
their services has significantly or somehow improved
the quality of care.
Participants were also asked how DHT is adopted
in their services and how it is regulated. They
reported that they are using NHS, CQC or council
guidelines. Most of the participants agreed that
guidelines were helpful and had a significant or some
impact in the adoption process. Participants were
asked questions related to medication administration
and regarding using a medication reminder system.
The answers from the participants revealed that all
participants administer four or more medications
daily and they do not use an app at that time. When
asked about missing or forgetting the doses or
medication, 5 participants reported this as a risk and
may happen rarely.
Participants were asked about their opinions on
the significance of medication reminder apps in
supported living services. Question 25 revealed that 4
participants (66.7%) considered it important, while 2
(33.3%) believed it is very important, as depicted in
Figure 3. Finally, in response to question 26, all
participants agreed that they have no concerns about
using medication reminder apps.
Figure 3: Level of importance of medication reminders to
the services.
Quantitative data from the case study from the two
supported living services has been compared to see if
there is any significant difference. There was not any
significant difference in the results but only a slightly
high acceptance and usage of DHT in House 1.
4.2 Qualitative Analysis
The qualitative data gathered from the study were
coded and analysed using the thematic analysis
approach. After generating the initial codes and
defining the themes, the qualitative data was collected
from patterns and trends in the participants’
responses. Then, they were arranged into themes to
align with the research questions, aims and
Adoption of Digital Health Technologies in Supported Living Services
185

objectives. There were 14 open-ended questions in
the questionnaire from where the data were drawn.
Participants were asked about the digital health
solutions currently used in their respective services
and the ones they plan on adopting. Codes identified
from the data helped to define the DHT Types theme
are listed below:
Health monitoring devices: blood pressure
monitor, blood glucose monitor, etc.
Assistive technologies: virtual voice assistants,
mobility scooters, electric wheelchairs, etc.
Health information systems: electronic health
records (EHR), digital recording systems,
integrated health management systems, etc.
Healthcare applications: phone applications,
online systems for residents, etc.
Positive Impacts theme was defined from the
responses the participants gave to questions 12 and 13
when asked to state how DHT has improved the
quality of care in their services and how it has
benefitted them. The answers were carefully
organised into codes to form the Positive Impacts of
DHT on the quality of care as below:
Improved quality of life of service users:
improved safety and independence of service
users, reduced incidents of clinical
emergencies because of the effective use of
health monitoring devices.
Increased operational efficiency: promoting
self-management of service users, service users
can take the lead in their support plan, resulting
in effective time management and cutting
operating costs.
Increased productivity: using digital health
interventions ensures that workers can do so
much within a considerable period.
Effective management of data: DHT such as
digital recording promote information accuracy
and effective data sharing within the care and
management team of service users.
Enhanced person-centred support: the
deployment of DHT ensures service users are
supported according to their peculiar needs, it
promotes using the right digital solution for the
right person for the proper purpose.
Improved collaborations with external
partners: The participants revealed that DHT
helps information sharing with relevant
partners as quickly and effectively as possible.
The participant’s responses to questions about the
challenges experienced during previous adoption and
those anticipated in future adoption (questions 9b,
14b and 19), and the personal contribution of one of
the respondents in question 20b, were coded and used
to form Barriers theme. Identified codes for the
Barriers to DHT adoption are as follows:
Cost of DHT implementation: some services
might find the cost of implementing DHT
expensive, the need for sufficient funding to
purchase and maintain DHT.
Low digital literacy among staff and service
users: some staff and residents may not be
familiar with the technologies.
Resistance to change: some staff and residents
may be slow in integrating new systems and
may lack the motivation to use DHT.
Data privacy and security concerns: staff and
residents may have reservations about the
integrity of the systems’ data and information
security, resulting in low motivation to use
digital health devices.
Technical challenges: organisations may lack
robust information technology and software to
accommodate the flawless operation of digital
health solutions.
The participant’s responses to questions about the
facilitating factors to DHT in their respective
services, the essential guidelines, and best practices
for adopting DHT (questions 10b, 15 and 16) were
coded and used to form Facilitators theme. Identified
codes are as follows:
Training for staff and service users: this
involves training for technicians and workers
reading the user or operating manuals of digital
devices, learning how to use the equipment.
Supportive organisational culture: entails
management support, GP recommendations,
and local policy.
Gradual integration of DHT: gradually
incorporating digital technology user-centred
approach, teaching workers how to use it best.
Adherence to relevant guidelines: this includes
adhering to professional and manufacturer
guidelines, as well as local policy, professional
guidance, risk assessments, and GDPR.
The participant’s responses to questions about
their opinions about the guidelines and best practices
for adopting DHT in supported living services
(questions 15 and 16) were coded and used to form
Guidelines theme. Identified codes are as follows:
Training programmes for staffs and service
users: ensuring staff members are trained on
using DHT before and periodically after use.
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
186

Assessment of user experience: before
implementing DHT, assess the users’ needs and
the site’s capabilities to ensure they are
compatible with the technology, introducing
DHT gradually with relevant staff training.
Adherence to relevant guidelines: following
guidelines, local policy, and risk assessments to
ensure compliance with regulations.
Ensure designated use of DHT: ensuring DHT
are used properly and only when necessary for
applicable users.
Privacy and security compliance: Ensure
compliance with GDPR guidance and relevant
security procedures.
Finally, participants were asked to share their
desired features for a potential medication reminder
app in question 24b as part of the study's objectives.
Participants’ responses from these questions were
organised to form the codes below for the Application
Design theme, which were also used to develop the
functional and non-functional requirements partially.
Customisable and flexible design: the app must
offer a function that enables users to enter and
modify their medication information by their
requirements, the app should provide users
with customisation options such as
personalised reminders and notifications.
User-friendly interface: the app should be easy-
to-use, straightforward, and intuitive, making it
accessible to many users, the ability to create
and manage user profiles, calendar view of the
medication administration record (MAR).
Responsive design: to ensure users can access
their information from anywhere, the app
should be designed to work effortlessly across
multiple devices.
Enhanced data security: the app should have
robust security structures to secure user data
such as encrypted and other data protections.
4.3 Discussion
There were notable findings from the patterns
observed from the data analysis of the houses. The
data collected from six participants who have
working experience in their roles for at least one year.
This ensures that they understand the support needs
and support plans of the service users of their various
services. Therefore, the information they provided on
the questionnaire can be regarded as expert opinions.
The data analysis shows a broad acceptance of
digital health in the services, and the majority
(83.3%) of participants use at least one digital health
device in their services. Similarly, the result shows
that the main reasons for adopting DHT in the
services is to improve operational efficiency and
improve the quality of care provided. The data
analysis revealed that most participants know
relevant guidelines and requirements for adopting
DHT, and they follow recommendations from NHS,
CQC or local council, which is BCP in this case.
Finally, the results showed that participants are keen
to use a medication reminder application and they
find it important to supported living services.
5 AN EXAMPLE APP
Medication non-adherence is a significant problem,
leading to adverse health outcomes and increased
healthcare costs. Applying digital health solutions,
such as medication reminder apps, can help with this
problem. Mobile applications are the most common
type of medication reminder software, e.g. Medisafe,
Medbuddy, etc., which combines reminder
functionality with features such as medication
tracking and ability to communicate with healthcare
professionals (Corbett et al. 2021). However,
evaluations on medication apps show that the
complexity of multifunctional apps can be
overwhelming for some users.
In this study, a mobile medication reminder app is
designed to enhance medication adherence among
residents of supported living services. The app is
designed using the design thinking approach which
prioritises user experience in every step of the design
process. The app features a user-friendly interface
that enables different tasks, such as scheduling and
managing medication reminders, viewing existing
reminders for medication schedules, ordering, and
tracking medications from the pharmacy, customising
reminder tones, and accessing weekly medication
adherence reports. Potential users of the system are
managers, support workers and self-medicating
service users. We defined three user personas
accordingly. In this study, a use case diagram was
utilised in modelling the major features of the app as
shown in Figure 4.
We designed wireframes and an interactive
prototype as they are useful in presenting the scope of
the system functionality to intended users. They were
designed using the proto.io cloud-based prototyping
tool.
The design includes the onboarding screen,
authentication screen, menu screen, and screens for
setting up medication schedules, displaying
reminders, tracking progress, displaying service users
Adoption of Digital Health Technologies in Supported Living Services
187
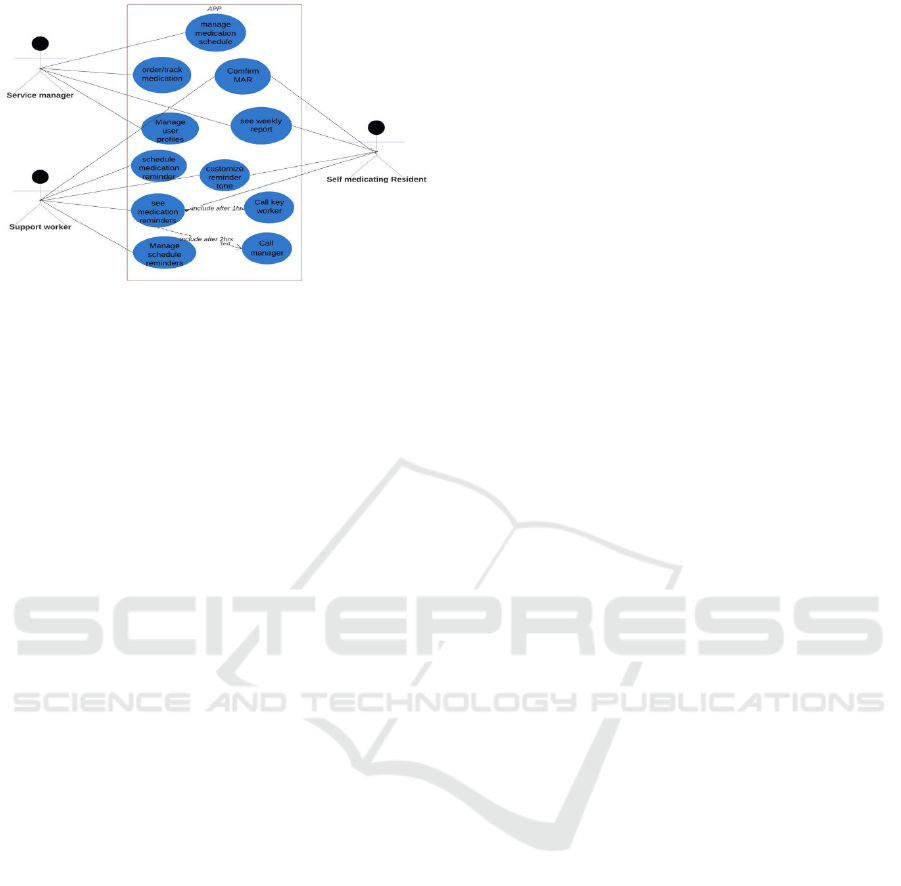
Figure 4: Use case diagram for the proposed app.
(residents) profiles, and managing user accounts. The
design models are available upon request.
6 EVALUATION
The evaluation for this study was done by designing
evaluation forms to assess the written artefact by the
participants and doing a cognitive walkthrough on the
interactive prototype of the medication reminder
application. These steps helped validating the
outcomes of this research and collecting feedback.
The written artefact is designed to be a document
containing the findings and recommendations to ease
the adoption of DHT in supported living services. It
was sent to the two houses participated in the study
together with an evaluation questionnaire, which is
aimed at getting the participants’ observations,
reservations, suggestions, and recommendations on
the written solution.
The evaluation report from House 1 stated the
document being useful to the service, with a special
commendation on the study findings which revealed
from the comparative analysis of both houses, that
every house and its service users are different.
The evaluation report from House 2 indicated that
they are satisfied with the written artefact presented
to the management after due consultation with the
project supervisor. The management confirmed that
the study findings are true reflections of the reality of
DHT in the service. They also agreed that digital
solutions could promote independence and improve
medication administration and record keeping.
We used the cognitive walk-through approach to
evaluate the medication reminder app design. A
usability evaluation form was designed and sent to the
services with the link to the interactive prototype. The
evaluation form included tasks to navigate on the
prototype for different type of users and step by step
control sequence such as clicking buttons, entering
data, etc. The managements of both supported living
houses expressed satisfaction with the app design as
they found it useful to their services according to their
responses in the evaluation report.
7 CONCLUSIONS
The findings of this study reveal that the use of DHT
and health informatics varies based on the service and
the service users living in the care homes. However,
this study also highlights the numerous benefits of
adopting DHT, including improved quality of life for
service users, enhanced operational efficiency,
increased productivity of workers, and practical
information management of staff and service users.
Providing guidelines and best practices that supported
living services could leverage can help with
promoting the adoption of these technologies and
tools. As a future work, a larger sample size of
supported living services and participants can be
employed to gather the perspectives and experiences
of more services which could increase the chances of
generalisation of the findings. Additionally, this study
focused on the inputs and contributions of staff
members only. Future research can include the
service users and other relevant stakeholders to
understand better the factors influencing the adoption
of technology in supported living services.
ACKNOWLEDGEMENTS
Authors would like to thank the two supported living
house residences in Bournemouth, the UK and the
participants who joined in this study.
REFERENCES
Ainsworth, A., 2021. Supporting social care providers to
adopt care technologies through a new investment fund
- NHS Transformation Directorate [online]. Available
from: https://transform.england.nhs.uk/-blogs/support
ing-social-care-providers-to-adopt-care-technologies-
through-a-new-investment-fund/ [Accessed 29 Apr
2023].
Alzheimer’s Society, 2015. Assistive technology-devices to
help with everyday living, Factsheet 437LP.
BCP, 2021. Bournemouth, Christchurch and Poole Council
Care Homes for Older People Commissioning [online].
Available from: https://democracy.bcpcouncil.gov.uk/
documents/s27735/Enc.%201%20for%20Older%20Pe
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
188

oples%20Care%20Home%20Strategy.pdf [Accessed
30 Mar 2023].
Cassels, B., 2022. The NHS App and its central role in the
fight against COVID-19 - NHS Digital [online].
Available from: https://digital.nhs.uk/blog/inside-
story/2022/the-nhs-app-and-its-central-role-in-the-
fight-against-covid-19 [Accessed 2 Jan 2024].
Corbett, C.F., Combs, E.M., Chandarana, P.S., et al., 2021.
Medication adherence reminder system for virtual
home assistants: mixed methods evaluation study.
JMIR Formative Research, 5 (7).
CQC, 2022. The impact of digital solutions and technology
[online]. Available from: https://www.cqc.org.uk/-
publications/major-report/soc201920_3d_impact-of-
technology [Accessed 16 Apr 2023].
Cummins, N. and Schuller, B. W., 2020. Five Crucial
Challenges in Digital Health. Frontiers in digital health,
2, 536203.
Franklin, B. D., Reynolds, M. J., Hibberd, R., Sadler, S. and
Barber, N., 2013. Community pharmacists’
interventions with electronic prescriptions in England:
an exploratory study. International journal of clinical
pharmacy, 35 (6), 1030–5.
GOV.UK, 2022a. A plan for digital health and social care
[online]. Department of Health and Social Care.
Available from: https://www.gov.uk/government/publi
cations/a-plan-for-digital-health-and-social-care/a-plan
-for-digital-health-and-social-care [Accessed 28 Mar
2023].
GOV.UK, 2022b. Digital revolution to bust COVID
backlogs and deliver more tailored care for patients -
GOV.UK [online]. Available from: https://www.
gov.uk/government/news/digital-revolution-to-bust-
covid-backlogs-and-deliver-more-tailored-care-for-
patients [Accessed 30 Apr 2023].
HCPC, 2018. Service user and carer involvement [online].
Available from: https://www.hcpc-uk.org/education/
resources/education-standards/service-user-and-carer-
involvement/ [Accessed 19 Apr 2023].
Hutchings, R. and Morris, J., 2022. Digital health care
across the UK: where are we now? [online]. Nuffield
Trust. Available from: https://www.nuffield-trust.org.
uk/resource/digital-health-care-across-the-uk-where-
are-we-now [Accessed 25 Apr 2023].
Lapp, L., Egan, K., McCann, L., Mackenzie, M., Wales, A.
and Maguire, R., 2022. Decision Support Tools in
Adult Long-term Care Facilities: Scoping Review.
Journal of medical Internet research, 24 (9), e39681.
Leigh, S., Ashall-Payne, L. and Andrews, T., 2020. Barriers
and Facilitators to the Adoption of Mobile Health
among Health Care Professionals from the United
Kingdom: Discrete Choice Experiment. JMIR mHealth
and uHealth, 8 (7).
Lennon, M. R., Bouamrane, M.-M., Devlin, A. M., et al.,
2017. Readiness for delivering digital health at scale:
lessons from a longitudinal qualitative evaluation of a
national digital health Innovation Program in the UK.
Journal of Medical Internet Research, 19 (2), e42.
McGee, M., Potter, C. and Kane, J., 2020. Are UK care
homes ready for the telemedicine revolution? British
Journal of Psychiatry (BJPsych), 44 (5), 222.
NIHR (National Institute for Health and Care Research),
2022. What is digital health technology and what can it
do for me? [online]. Available from: https://doi.org/
10.3310/nihrevidence_53447 [Accessed 18 Dec 2023].
NHS, 2021. Supported living services - Social care and
support guide - NHS [online]. Available from:
https://www.nhs.uk/conditions/social-care-and-support
-guide/care-services-equipment-and-care-homes/suppo
rted-living-services/ [Accessed 18 Apr 2023].
NHS, 2022. Personal alarms, monitoring systems (telecare)
and key safes - Social care and support guide - NHS
[online]. Available from: https://www.nhs.uk/condi
tions/social-care-and-support-guide/care-services-equi
pment-and-care-homes/personal-alarms-security-syste
ms-and-keysafes/ [Accessed 22 May 2023].
NHS Digital, 2022. Why digital inclusion matters to health
and social care [online]. Available from:
https://digital.nhs.uk/about-nhs-digital/corporate-
information-and-documents/digital-inclusion/digital-
inclusion-in-health-and-social-care#document-content
[Accessed 14 May 2023].
Shah, B., Allen, J. L. Y., Chaudhury, H., O’Shaughnessy,
J. and Tyrrell, C. S. B., 2022. The role of digital health
in the future of integrated care. Clinics in Integrated
Care, 15, 100131.
Sharif, M. S., Alsallal, M. and Herghelegiu, L., 2018. An
Effective TeleHealth Assistive System to Support
Senior Citizen at Home or Care-Homes. In: 2018
International Conference on Computing, Electronics &
Communications Engineering. IEEE, 113–117.
Swain, J., 2018. A Hybrid Approach to Thematic Analysis
in Qualitative Research: Using a Practical Example,
SAGE Publications Ltd.
Tyrrell, C. S. B., Mytton, O. T., Gentry, S. V, et al., 2021.
Managing intensive care admissions when there are not
enough beds during the COVID-19 pandemic: a
systematic review. Thorax, 76 (3), 302–312.
Vaportzis, E., Giatsi Clausen, M. and Gow, A. J., 2017.
Older Adults Perceptions of Technology and Barriers to
Interacting with Tablet Computers: A Focus Group
Study. Frontiers in Psychology, vol. 8.
Whitelaw, S., Pellegrini, D. M., Mamas, M. A., Cowie, M.
and Van Spall, H. G. C., 2021. Barriers and facilitators
of the uptake of digital health technology in
cardiovascular care: a systematic scoping review.
European Heart Journal - Digital Health, 2 (1), 62–74.
Yin, R. K., 2014. Case Study Research Design and Methods
(5th ed.). Thousand Oaks, Sage.
Adoption of Digital Health Technologies in Supported Living Services
189
