
New Insights into the end-User Requirements for Remote Monitoring
for Aging at Home Contributions to the Third Digital Divide
Cosmina Paul
a
, Andreea Stamate
b
and Luiza Spiru
c
Ana Aslan International Foundation, Spatarului nr 3, Bucharest, Romania
Keywords: Older 47Adults, Gerontographics, Monitoring, Digital Divide, Data Ethics.
Abstract: Well-being and independence are highly valued in Western European countries. Though, we need a more in-
depth understanding of how older adults and their next of kin perceive how monitoring technologies can
support ageing at home. Older adults are the most heterogeneous population in terms of health and functional
status comparative to all the other age groups and their formal and informal caregivers need also to be
accounted for in this endeavor. Therefore, the understanding of the process of accepting and adopting new
monitoring products is cumbersome as the current low adoption rates show despite innovators promises. By
employing a gerontographics approach, we aim at understanding what are the older adults’ expectations from
remote monitoring, a growing industry but with a low adoption rate. Hence, we have concluded that a) all
categories are interested in alarm features rather than day to day monitoring, b) the more independent one is,
more interested is in controlling/ handling the device, c) those psychologically well are rather stressed about
monitoring and prefer not to trade their privacy for safety,) all next of kin are much interested in high data
accuracy. We have also noted that the first and second digital divides, related to costs and relevance, persist,
and they add up to the third one. The third digital divide is about to happen, with respect to data and ethics of
the technologies, the need of the older adults or their next of kin to control and understand the device.
1
INTRODUCTION
At the outburst of the Covid-19 pandemic, people
reacted emotionally by singing songs out of their
balconies – a strong emotional response to an
essentially medical issue. However, in time, due to
lockdown measures, these emotional responses faded
away and people adjusted to technology-mediated
communication. Placing our focus on the alleged
impact of technology on emotions, the overall aim of
our project is to contribute to the understanding of
how technology affects the way we care. What are the
challenges brought by new technologies – such as
diminishing human contact – to the way we are and
feel being cared for, and our capacity to care for
others?
On the same par, the world population is ageing
(Eurostat, Ageing Europe, 2020). Worldwide, there is
a sharp increasing in the need for care and the Covid-
19 pandemic exacerbated this need (Power, 2020;
a
https://orcid.org/0000-0003-3827-2290
b
https://orcid.org/0000-0002-3385-9714
c
https://orcid.org/0000-0002-5308-205X
Alharbi et al, 2020). It is not only that there are just
fewer family caregivers available to provide everyday
assistance, but many of them are experiencing their
own physical and mental health challenges, at a rate
that can be as high as 70-80% (Alex Mihailidis,
ICT4AWE, 24-26 April, 2021).
As the wide range of implications of increasing
numbers of the older population is becoming a public
agenda, the need for technology adoption, as a
solution to face this problem, increases as well.
Literature shows that remote monitoring
technology, coupled with care-coordination, has the
potential to revolutionize the way older adults are
“Aging in Place”. This belief led to a context where:
a) Remote patient-monitoring industry is growing
and there is still high demand and b) All these
technological solutions are designed to complement
the increasing need for care which is answered
through: at-home caregivers, nursing homes, or PERS
devices (PERS personal emergency response
Paul, C., Stamate, A. and Spiru, L.
New Insights into the end-User Requirements for Remote Monitoring for Aging at Home Contributions to the Third Digital Divide.
DOI: 10.5220/0012730400003699
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2024), pages 291-297
ISBN: 978-989-758-700-9; ISSN: 2184-4984
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
291

system).
The success of remote monitoring technology is
allegedly given by the degree of being perceived as
unobtrusive and/or non-stigmatizing. Hence,
independent older adults would prefer devices which
are not wearable but passive – (More passive, more
successful, Vedantam, 2021) and, more, able to
detect a range of emergencies, and require no or
minimal action on the part of the user (Rantz et al,
2013; de Bruin et al, 2008).
On the same part, the perception of the product by
the caregivers is equally relevant. They need to
clearly understand the degree to which the assistive
technologies give them peace of mind and ease their
burden. Hence, older adults’ monitoring is meant to
support reducing caregiver burden and preserving
well-being outcomes for older adults (Czarnuch and
Mihailidis, 2011; Marasinghe, 2016; Creber et al.,
2016).
With respect to the professional care providers,
beyond their effectiveness, performance also
increases as more time is allocated to implementing
interventions. Along these advantages there are also
some limitations of remote monitoring, which refer to
a) high costs, b) the impossibility to assess the
performance of an individual, and c) accuracy is
limited because the collected data is rather inferred.
If we closely look to the evolution of remote
monitoring, we see that it encompasses the
advantages and limitations of the first and second
grey digital divides, which have been already
discussed at large within the research milieu
(Karahasanovic´ et al, 2009; Delello et al, 2017;
Battersby et al, 2017). The first refers to the low
adoption of the technology by the elderly because of
high costs, while the second divide refers to the
suboptimal adoption of technology by the elderly
because of new products’ lack of relevance to them.
van Deursen et al (2015) are discussing the upcoming
of the third divide of technology adoption which
relates to a lack of theoretical development about
which types of people are most likely to benefit from
technological innovation.
In our view, the first and second digital divides
gave not been overcome but, more they contribute to
deepen the third one. The answer for understanding
the correct status of the digital divides relies in the
right older adult population segmentation and co-
creation process, specifically involving older adults to
contribute from the concept development phase,
rather than only in the stages of testing solution as
end-users.
2
RESEARCH METHODOLOGY
2.1 “Theoretical Framework”
We employ a gerontographics segmentation, which
suggests that rather than considering age per se, more
accurate and relevant data are to be obtained when
accounting for physical and psychological state of the
older adults. Geronthographics is an approach
developed by Moschis (1996) and it shows its
efficacy in analysing elderly’ consumer activity based
on their physically and psychologically state
(Nimrod, 2013; Sthienrapapayut et al, 2018).
Therefore, Moschis refers to four categories of older
adults which are selected based on their state of health
on a continuum from independency towards
dependency (Moschis and Mathur 1993; Moschis
1996, 2003;). The approach assumes that older adults
show similar behaviour consumer activity if they had
encountered similar circumstances, experiences and
past events, based on the type of aging experience.
Starting from the gerontographics segmentation,
we have found that in the case of older adults
psychologically well, the ‘Perceived Usefulness’ of a
new technology determines the acceptance or rejection
of a technology, while in the case of those psycholo-
gically unwell, the influence of the formal and/or
informal caregivers is decisive (Paul and Spiru, 2021).
For example, if a person is overall physically and
psychologically well, then the A4A Solution needs to
detect the transition towards either physically well
and psychologically unwell or physically unwell and
psychologically well.
MoSCoW Prioritization for Older adults
psychologically well. Must have: Limited usage: just
for a notification or alarm, The option to control the
device; Easy to install; Reliable alarm.
MoSCoW Prioritization for Older adults
psychologically NOT well: Pre-alarms; Basic ADL
identification, toileting or feeding; (Individualized)
Movement behaviour patterns.
Tak et al (2013) presents a meta-analysis of the
association between physical activity (PA) and the
incidence and progression of basic ADL disability
(BADL) positioning PA as the most effective
preventive strategy in preventing and reducing
disability, independence and health care cost in aging
societies. More, functional independence influences
emotional wellbeing, while emotional well-being
predicts subsequent functional independence and
survival. For example, Ostir et al (2015) support the
concept that positive affect, or emotional well-being,
is different from the absence of depression or
negative affect. Their study results show that positive
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
292

affect seems to protect individuals against physical
declines in old age. Katt et al (2009) shows that ability
to perform ADLs has little to do with cognitive well-
being, but is an influential factor in determining
emotional well-being.
Hence, to support aging at place and prolong
the independence of the elderly, we need to consider
both physical activity and emotional wellbeing for
functional independence.
But geriatric wellbeing, positive ageing, wellness
for the elderly or successful aging are, generally,
concepts assessed through both objective and
subjective indicators. Therefore, we define wellbeing
as the capacity of an older adults to at least
maintain/preserve their ADLs to the specific
gerontographics category to which they belong.
Hence, the transition to a different category is
prevented, slowed down or even reversed due to the
dyad of OA/NoKs and OA/PCP supported by A4A
remote monitoring system.
2.2 Methodology
Within the framework of the project “From Smart
Home to Care Home – AAL4All (A4A)”, co-funded
by the European Programme AAL (Active Assisted
Living – ICT), we have set up and undertook the
documentation and co-creation process from its very
inception and carried it out over the course of 2022.
We have taken a questionnaire-based survey
method, which is part of the Positivism research
approach, along with the explanatory design. The data
was collected through a semi-structured survey
questionnaire. The survey questionnaire was
circulated to respondents electronically through
internet and traditional hard copies. For electronic
distribution, Google Forms have been used and no
personal data have been collected.
However, each participant has been properly
informed on the purpose of the research and given the
possibility to withdrawn at any time. The data was
analysed using SPSS.
The survey was conducted by the end-user
organizations involved in the A4A project, in
Romania, Switzerland, Portugal and Denmark. The
survey was carried via online and face2face interviews
during the period of May to July 7, 2022, from a sample
of 202 adults. 107 participants are from Romania, 32
from Portugal, 27 from Switzerland, and 36 from
Denmark. Respondents ranged in age from 18 to 99
years (mean = 57.88 years, sd = 18.61 years), with
more than half (66.3%) female. Slightly more than one-
third of respondents (37.6%) reported living alone,
while nearly one third live with their spouse (27.7%).
Of those sampled, the adoption of the technology
which supports independence at home and quality of
living is low. 76% did not adopt any technology and
from those who did, smartphones and computers are
the most common adopted technologies.
The 7-Questions. Respondents were asked seven
questions relating to the relevance of various A4A
Solution features, in their quality as a care giver or a
care-receiver. The participants were asked to rate the
relevance of 7 features of the A4A Solution, on a
scale from 1 to 5. The mode (the most frequent value)
is 5 for each item (the participants rated the relevance
of each of the 7 features on a scale from 1 to 5).
The 7-question item which was asked is the
following:
How useful is the A4A device, for you or for
somebody you care for (e.g. your parents)? To send
a notification to a relative or carer if you (or your
care-receiver) did not get out of bed by a specific time
in the morning,
To know the Activities of daily living based on the
sound monitoring (eating, toileting, etc.), Proactively
generate an ALARM to the sounds” HELP" or
repetitive beats which might mean “HELP” to a next-
of-kin or professional carer, Identify the abnormal
movement behaviour (for example, overnight or high
toilet frequency, To switch off and on the device as
you (or your care-receiver) want, Early identification
of depression or anxiety, Early identification of
cognitive decline.
Participants
From the perspective of gerontographics
segmentation the population of people aged 65 and
over can be grouped in 4 categories, based on the
wellness or unwellness of their physical and
psychological status. Therefore, there are 4
categories:
1. Physically and Psychologically Well (Healthy
Indulgers)
2. Physically Unwell and Psychologically Well
(Ailing Outgoers)
3. Physically Well and Psychologically Unwell
(Healthy Hermits)
4. Physically and Psychologically Unwell (Frail
Recluses)
Individuals may move to the next life-stage due to
biophysical and psychosocial ageing process
(Moschis, 2019). That means that generally, someone
who is physically and psychologically well, through
the ageing process, in time, will become either
New Insights into the end-User Requirements for Remote Monitoring for Aging at Home Contributions to the Third Digital Divide
293

physically or psychologically unwell or both.
90 participants fell into the first category, (who
identify or self-identify as A4A beneficiary) being
physically and psychologically well. The group of
those who are physically and psychologically well is
over-represented comparative to the other groups.
44% live alone.
The second category comprises 30 participants,
who identify or self-identify as being physically
unwell and psychologically well. 70% are female.
The third category comprises 25 participants, who
identify or self-identify as being physically well and
psychologically unwell. 64% are female.
The fourth category comprises 23 participants,
who identify or self-identify as being physically and
psychologically unwell. 71% are female.
3
RESULTS
In line with other research findings, data show that
the first two hurdles of the digital divides have not
been fully past.
First Digital Divide: Costs
There is a sharp difference between those psychologi-
cally well and those psychologically unwell in the
decision of buying a monitoring product and assistive
technology in general. Those who are psychologically
well tend to adopt devices which are not specifically
designed for older adults and would tend to avoid
monitoring. Interestingly to note, when those
psychologically well are involved in testing or are
curious about the products, they would tend to feel
stressed about being monitored and to refuse
technology.
Whereas those psychological unwell would firstly
be influenced by others in this decision and tend to
accept any kind of monitoring or technology which
might support/ accompany/ or give a sense of being
secure.
For those psychologically well regardless of their
physical status, in the decision of NOT buying the
A4A Solution, the ‘technology alternatives on the
market’ is the less important factor, while all others
(price, privacy, not being monitored and false alarms)
are very relevant and relevant for about 60% of the
participants.
For those physically well and psychologically
unwell, the price matters the most in the decision for
not buying the product (60% rated 5 this reason in not
buying the A4A). Similar for the category of those
both physically and psychologically unwell, price is
the most important factor for not buying the product
(71%), followed by privacy (57,2%). Reticence for
being monitored is the least important factor in the
decision of not buying the product. A negative weak
correlation exists between the willingness to pay
more for the A4A Solution as long as they pay
themselves the price (Pearson correlation -.418).
Second Digital Divide: Relevance
The A4A Index
‘The A4A Index’ was conceived to assess the
robustness of the new technology proposed for the
seniors and their next of kin. The index puts together
7 key-measures of the new technology: ‘alarm’,
‘notification’, ‘anormal behaviour, ‘control
ON/OFF’, ‘ADLs’ cognitive decline’ and ‘mental
unwellness’.
A reliability test has been conducted, which
measures the internal consistency of the index, that is,
how closely related the set of 7 items are as a group.
The reliability test is conducted through Cronbach’s
Alpha, which is .917. That shows a high reliability
(significantly higher than .800).
On a scale from 1 to 5, the mean of the A4A Index
is 3.76 and the median is 4 and the mode, the most
common value, is 5 (19.5% rated with 5 each of the
A4A features). High relevance of the A4A Solution
was found among 48% (Those who rated 4 or 5 each
feature of A4A) and No relevance of the A4A
Solution was found among 20.7% (Those who rated
1 or 2 each feature of A4A).
The A4A Solution is seen as being very relevant
and relevant by the large majority of the participants.
The Alarm feature (‘Proactively generate an
ALARM to the sounds” HELP" or repetitive beats
which might mean “HELP” to a next-of-kin or
professional carer) is seen as being the most relevant.
The following 3 advantages: easy to install,
relevance of the alarm, and the price, are moderately
correlated to the relevance of the Index A4A (Pearson
Correlation .469; .468 and .405 respectively).
The advantage of ‘notifications of cognitive
decline’ is significantly stronger correlated to the
Index A4A (Pearson Correlation .679).
The Q4 Index “Worries” has a high reliability, and
weakly predicts the relevance of the A4A Solution
(Adjusted R Square= .208).
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
294
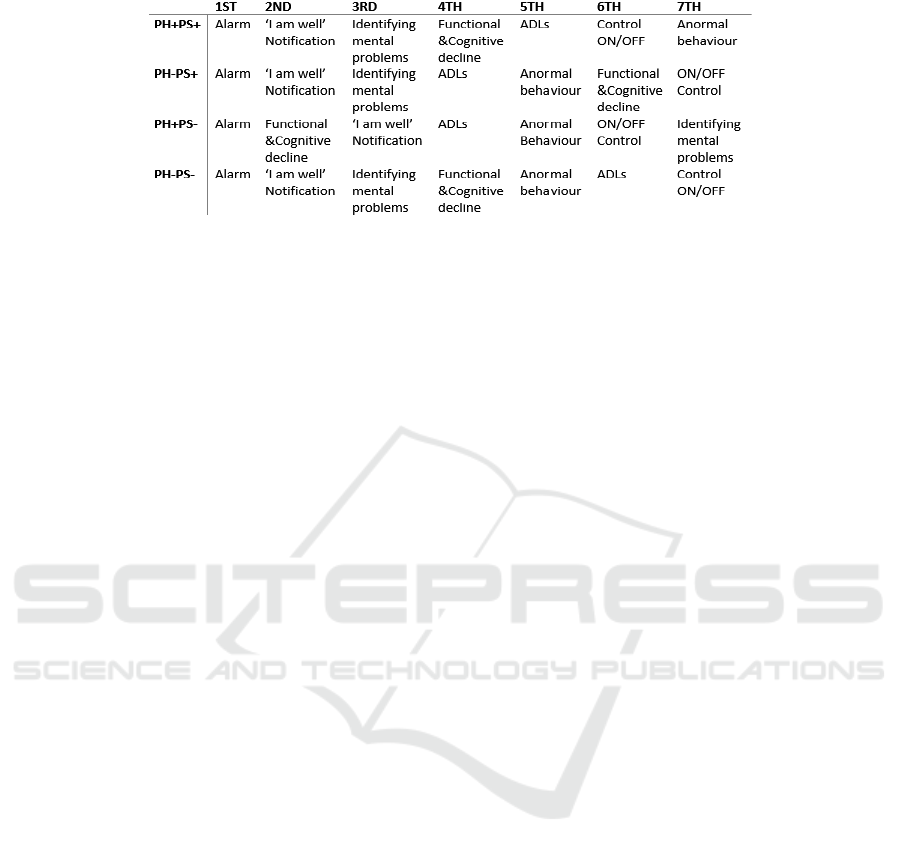
Table 1: The relevance of the A4A features.
The Q8 Index ‘the advantages which influence the
decision to buy the A4A Solution’ and The Q9 Index
‘the features which influence the decision NOT to
buy the A4A Solution’ are not reliable, meaning that
we cannot conclude on each advantage/feature of the
A4A Solution as counting in the decision to buy or
not to buy the product.
Therefore, we have decided to group the
participants in 4 groups, according to the
gerontographics segmentation in order to account for
more subtle preferences and characteristics of the
participants in relation to the A4A Solution. Hence,
the co-creation process was key in giving the right
direction towards the development of the new
technology
.
In line with literature review, the results show that
there is a wide range of requirements because older
adults (henceforth, OA) are a very heterogeneous
population, with many people over the age of 80
continuing to live independently, while others show
frailness and advanced cognitive impairment. The fact
that their next of kin (henceforth, NOK) and formal
care providers (henceforth PCP) are involved in the
A4A co-creation process as end-users and buyers
make the process more complex.
Those who exhibit psychological wellbeing and
have relatively good health conditions, regardless
of their age-related physical limitations and still
living independently would tend to adopt technology
which support their positive ageing. They look for
volunteering and community involvement as well as
new communication channels, and opt for
smartphone for tracking their physical activity (Paul
and Spiru, 2021). The healthy and independent older
adults and their professional and next of kin carers
think about A4A device as having some basic
functions:
-the control over the device and over the alarm,
-notification or pre-alarm to be sent to NoK or PCP if
they do not wake up,
-avoiding false alarms and easy to install.
They merely show that they want to keep their
independence and control over their life, while NoK
and PCP look to avoid overloading.
Those who Exhibit a Low Psychological Well-
Being. would tend to adopt technology who make
them feel more secure, have a feeling of being
supported and cared for. Hence, they would tend to
adopt remote sensors or wearables.
The Third Digital Divide: Ethics and More
As Ethics and data protection is a growing point of
concern for older adults. As people age and become
more and more accustomed to the new technologies
they are also more informed about the data protection
and ethics. Their next of kin claim more and more
transparency and information regarding data
collection and processing. Hence, they tend to refuse
monitoring until they reach the point of trading their
privacy for security.
Though, ethics and data protection is not the only
point of their concern. New monitoring products
require an ecosystem to be in place for them to
optimal function. Data interpretation is one point of
concern as current monitoring products add to the
burden of caring by asking their next of kin or
professionals to step in.
4
DISCUSSION
Research shows that there is a correlation between
physical activity and subjective well-being on the one
hand, and health and longevity on the other hand,
even there is still much more to learn about the
relation between the two. Growing evidence from
neuroscience, biology and social studies shows that
there is a strong connection between physical activity,
emotional wellbeing and functional independence but
more research is needed to establish the causation
direction and moderators.
New Insights into the end-User Requirements for Remote Monitoring for Aging at Home Contributions to the Third Digital Divide
295

With respect to monitoring technologies, the first
and second digital divides have not been yet
overcome. That is because one needs a whole system
in place for monitoring, such as the caregiver, the
system to run, data interpretation. All these further
restrict even the HAVEs to access monitoring
technologies because the ecosystems which allow
monitoring products to work are not in place. More,
even when they are, it is cheaper to opt for monitoring
only for accidents, i.e. fall alarms.
A4A Solution would infer on the ADLs and
IADLs to detect early anomalies in functional
independence. These early detected anomalies are
much related either to the deterioration of physical
activity, emotional or cognitive wellbeing.
5
CONCLUSIONS
We see that the first digital divide has not passed and
the costs of the assistive technologies and their
services stay high and widen the gap between the
have and have nots. With respect to the second digital
divide, we have also noted that the heterogeneity of
the older adult population leads to different
expectations based on the health and functional
status. A third digital divide is about to happen, with
respect to data and ethics of the technologies, the need
to control the device clearly expressed by the
participants.
To some extent, technology drives away emotions
in a process aimed at optimizing care. A nurse ceases
to hold someone’s hand because of the pulsometer,
children and older adults are monitored, surveillance
technologies are on the rise, doctors may gradually
become redundant due to AI of decision support
systems, and biometrics can tell you about subtle
changes in your body even before you can perceive
them (Harrari, 2018).
ACKNOWLEDGEMENTS
This work was performed in the frame of the national
project „Increasing research capacity and national
and international visibility of the Ana Aslan
International Foundation (FAAI), through promoting
research results”, SMART-BEAR, PN-III-P3-3.6-
H2020-2020-0174, nr. 61/2021 and EU project
AAL4All (AAL-2021-8-164-CP) funded by the AAL
Programme and co-funded by the European
Commission and the National Funding Authorities of
the partner countries.
REFERENCES
Battersby, L., Fang, M.L., Canham, S.L., Sixsmith, J.,
Moreno, S. and Sixsmith, A., 2017, July. Co-creation
methods: informing technology solutions for older
adults. In International Conference on Human Aspects
of IT for the Aged Population (pp. 77-89). Springer,
Cham.
Creber RM, Maurer MS, Reading M, Hiraldo G, Hickey
KT, Iribarren S. Review and analysis of existing mobile
phone apps to support heart failure symptom
monitoring and self-care management using the Mobile
Application Rating Scale (MARS). JMIR mHealth and
uHealth. 2016 Jun 14;4(2):e5882.
Czarnuch, S. and Mihailidis, A., 2011. The design of
intelligent in-home assistive technologies: Assessing
the needs of older adults with dementia and their
caregivers. Gerontechnology, 10(3), pp.169- 182.
De Bruin, E.D., Hartmann, A., Uebelhart, D., Murer, K. and
Zijlstra, W., 2008. Wearable systems for monitoring
mobility-related activities in older people: a systematic
review. Clinical rehabilitation, 22(10-11), pp.878-895.
Delello, J.A. and McWhorter, R.R., 2017. Reducing the
digital divide: Connecting older adults to iPad
technology. Journal of Applied Gerontology, 36(1),
pp.3- 28.
Grzes M, Hoey J, Khan S, Mihailidis A, Czarnuch S,
Jackson D, Monk A. Relational approach to knowledge
engineering for pomdp-based assistance systems with
encoding of a psychological model. KEPS 2011. 2011
Jun 12:77.
Istrate, D., Vacher, M. and Serignat, J.F., 2008. Embedded
implementation of distress situation identification
through sound analysis. The Journal on Information
Technology in Healthcare, 6(3), pp.204-211.
Karahasanović, A., Brandtzæg, P.B., Heim, J., Lüders, M.,
Vermeir, L., Pierson, J., Lievens, B., Vanattenhoven, J.
and Jans, G., 2009. Co-creation and user-generated
content–elderly people’s user requirements. Computers
in Human Behavior, 25(3), pp.655-678.
Katt JA, Speranza L, Shore W, Saenz KH, Witta EL. Doing
Well: A sem analysis of the relationships between
various activities of daily living and geriatric well-
being. The Journal of genetic psychology. 2009 Sep
30;170(3):213-26.
Madara Marasinghe K. Assistive technologies in reducing
caregiver burden among informal caregivers of older
adults: a systematic review. Disability and
Rehabilitation: Assistive Technology. 2016 Jul
3;11(5):353-60.
Moschis, G.P., 1996. Gerontographics: Life-stage
segmentation for marketing strategy development.
Greenwood Publishing Group. Moschis, G.P., 2003.
Marketing to older adults: an updated overview of
present knowledge and practice. Journal of Consumer
Marketing, 20(6), pp.516-525.
Moschis, G.P., Mathur, A. and Sthienrapapayut, T., 2020.
Gerontographics and consumer behavior in later life:
Insights from the life course paradigm. Journal of
Global Scholars of Marketing Science, 30(1), pp.18-33.
ICT4AWE 2024 - 10th International Conference on Information and Communication Technologies for Ageing Well and e-Health
296

Moschis, George P. 2019. Consumer Behavior over the Life
Course. Research Frontiers and New Directions,
Springer Nature.
Nimrod, G., 2013. Applying Gerontographics in the study
of older Internet users. Participations: Journal of
Audience & Reception Studies, 10(2), pp.46-64
Ostir GV, Berges IM, Ottenbacher KJ, Fisher SR, Barr E,
Hebel JR, Guralnik JM. Gait speed and dismobility in
older adults. Archives of physical medicine and
rehabilitation. 2015 Sep 1;96(9):1641-5.
Paul, C. and Spiru, L., 2021. From Age to Age: Key
Gerontographics Contributions to Technology
Adoption by Older Adults.
Rantz MJ, Zwygart-Stauffacher M, Flesner M, Hicks L,
Mehr D, Russell T, Minner D. The influence of teams
to
Spiru, L., Marzan, M., Paul, C., Velciu, M. and Garleanu,
A., 2019. The Reversed Moscow Method. A General
Framework for Developing age-Friendly Technologies.
In Multi Conference on Computer Science and
Information Systems, MCCSIS 2019–Proceedings of
the International Conference on e-Health 2019 (pp. 75-
81). Lisbon: IADIS Press
Tak, H.J., Curlin, F.A. and Yoon, J.D., 2017. Association
of intrinsic motivating factors and markers of physician
well-being: a national physician survey. Journal of
general internal medicine, 32(7), pp.739-746.
van Deursen, A.J.A.M. and Helsper, E.J. (2015), "The
Third-Level Digital Divide: Who Benefits Most from
Being Online?", Communication and Information
Technologies Annual (Studies in Media and
Communications, Vol. 10), Emerald Group Publishing
Limited, Bingley, pp. 29- 52
New Insights into the end-User Requirements for Remote Monitoring for Aging at Home Contributions to the Third Digital Divide
297
