
Eco-Sustainability and Efficiency of Healthcare Complex Systems
Ilaria Angela Amantea
1 a
and Marinella Quaranta
1,2 b
1
Computer Science Department, University of Turin, Turin, Italy
2
Department of Law, University of Bologna, Bologna, Italy
Keywords:
Healthcare, E-Health, Digitalization, Complex System, Simulation, BPM.
Abstract:
Healthcare is one of the most difficult complex systems to optimize. The challenge is in the multiple factors
to balance. Some are common to many other industries, while some are riskier, and the whole system must be
well-balanced to flow and ensure the functioning of a vital service for the citizens. The close interconnection
between the various factors means that making changes on one aspect will have cascading effects on many
other aspects. Therefore, the optimization must not be done considering a single parameter, but considering
the whole chain. According to the European objectives of digitalization and eco-sustainability, in this paper
we present an overview of the impact of digitalization of certain paper documents on process activities, times,
costs, and spaces of archives.
1 INTRODUCTION
Healthcare structures are ”complex systems”.
Namely, a complex system is a system made of
(i) interacting component parts and (ii) exhibits
dynamical behavior that cannot be inferred from
the behavior of the parts themselves (Motter, 2004).
Complex systems have also been defined as an
ensemble of many elements that interact in a dis-
ordered way, resulting in robust organization and
memory (Ladyman et al., 2013). Thus a complex
system is a collection of interconnected elements that
present emergent behavior, which means that a whole
system displays properties and behaviors that are not
directly predictable from each behavior of individual
parts. They also include non-linear dynamics (small
changes lead to impacting effects), and properties
that may be difficult to anticipate or control. This
also makes them vulnerable to some failures (e.g.
cascading failures) and unpredictable behavior.
Generally, in healthcare, there are a relevant
amount of features to take into account. There are
medical norms, medical guidelines, and medical pro-
tocols that are strictly related to the diagnosis, cure
and prevention of conditions, diseases and patholo-
gies. These elements are not only regulated by the law
but also by practical elements, e.g. the ability to man-
a
https://orcid.org/0000-0003-1329-1858
b
https://orcid.org/0000-0003-2691-0611
age emergencies and criticalities that fall outside the
guidelines. Healthcare structures have a large number
of variables, thus, there is a multitude of tasks that
could suffer from bad management, as for less visi-
ble criticalities and bottlenecks. Once they become
visible, they can be optimized.
Time can be pivotal in healthcare structures, but
reducing time in tasks generally leads to an increase
in number of patients to be taken care of. With a
new load of patients, staff get overloaded with work
or might have to work under pressure, as usually an
increase in workload does lead to a congruent ad-
justment in staff employment. Human staff cannot
be subject to machine-like rhythms, they need and
have the right to rest. They are also entitled to bal-
anced and reasonable work shifts. Such conditions
are needed not only to be compliant with contracts
but also because a tired physician could make mis-
takes in treating patients. Less rest impacts on risk of
clinical and treatment errors. Cost is also pivotal in
healthcare structures. Normally cost optimization is
linked to cutting staff or services, but this enhances
the issue of the quantity and quality of care services
provided to the citizen, and again, it impacts the work-
load of the remaining staff. Times, costs, and quali-
ties are the three features to be balanced in healthcare
structures. Depending on the goal, it is possible to
optimize two of such features, which inevitably de-
teriorates the third feature. It is not possible to opti-
mize all three features if available resources continue
Amantea, I. and Quaranta, M.
Eco-Sustainability and Efficiency of Healthcare Complex Systems.
DOI: 10.5220/0012857400003758
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 14th International Conference on Simulation and Modeling Methodologies, Technologies and Applications (SIMULTECH 2024), pages 423-430
ISBN: 978-989-758-708-5; ISSN: 2184-2841
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.
423

to stay the same. This scenario could lead to new gen-
eralized problems (long attendance lists, delays, daily
errors, etc.). Optimizing all three features only be-
come possible in case available resources increase.
The European Union has been pushing for years
towards the digitalization of public systems, public
administration, courts, healthcare etc. and member
states are following along.
The European Union prioritizes digitalization,
particularly in public administrations, and has made
significant progress through the ”NextGenerationEU”
recovery plan, which includes numerous digitaliza-
tion projects(Amantea et al., 2023). In the e-health
sector, the European Commission has proposed the
European Health Data Space, aiming to facilitate the
free movement of citizens by ensuring health data ac-
cessibility across member states. Despite high-level
legal norms and national legislation supporting digi-
talization, effective implementation requires internal
protocols within healthcare infrastructures. Without
these protocols, traditional paper processes may per-
sist(Amantea et al., 2022a). Therefore, especially
for public facilities like hospitals, digitalization will
mean compliance with European prescriptions.
In Italy, hospitals currently print an enormous
amount of paper for prescriptions, informed consents,
medical forms, clinical documents, reports, internal
organizational documents, etc. In terms of costs,
these printing costs in the long run can weigh on the
total budget of a hospital, while in time terms, the
time used in printing these papers significantly length-
ens waiting times for patients. These documents must
be kept in the possession of healthcare facilities for
a certain amount of time set by the law (on average
from 2 to 10 years depending on the type of docu-
ment). This also means that several rooms must be
saved as archives and cannot be used for clinical care.
There are further obligations set by the law on these
kinds of documents: paper documents (such as med-
ical reports) must be physically collected from the
patient, while the physical search and distribution of
medical reports implies additional time for the admin-
istrative staff of the hospital, the existence of an office
with designated personnel, an archive, the presence
of patients and physical waiting queues in structure.
Also, in case long-archived documents are needed, a
manual search through a considerable amount of pa-
per is needed.
Our research is based on a collaboration with
healthcare facilities in Piedmont, our collective aim is
to ease the digitalization process. We will refer to the
digitalization of the “Azienda Sanitaria Locale Torino
3 - ASLTO3”, which is a local health care service, a
public health entity working in the Piedmont Region.
The goal of this paper is to show how digitalization
could come as a solution: by digitizing some docu-
ments that are currently on paper, it could be possible
to maintain the same quality of service while reducing
costs. This would also be possible due to the already
existing server and information system. However, this
specific function of the system is not yet in use.
The savings in costs could be used to increase hu-
man resources or equipment, which would lead to an
improvement in the workload, an increase in the well-
being of the working environment, and could lead to
a decrease in times (e.g. printing times and times for
searching in the archives). Finally, it could also in-
crease the total number of visited patients.
The paper is structured as follows: Section 2 will
outline the methodology and the background; Sec-
tion 3 shows the case study experiments that imply
processes, simulations, results, and related comments
and observations; finally, Section 4 presents some
conclusions.
2 METHODOLOGY
In medicine, the organization of health processes is a
fundamental aspect to examine and it should be exam-
ined by taking a holistic and systemic approach. Also,
computer science gained a relevant role in techni-
cal hardware and information systems improvements
(Dumas et al., 2005).
To analyze the healthcare facilities’ business pro-
cesses, we used the business process management
methodology (BPM) (Dumas et al., 2018) a discipline
combining data science and management studies to
perform business process improvement, modeling and
simulation (Sulis and Di Leva, 2017). A key objective
within BPM is change management (Amantea et al.,
2020a). By emphasizing a process-centric method-
ology, we illustrate the business process through the
standardized language of the Business Process Model
and Notations (BPMN). The methodology takes a
process-centric stance and involves a process-aware
information system alongside the iGrafx simulation
tool. These tools are used to reshape their business
processes. Through the integration of these meth-
ods, we can scrutinize activities, resource allocation,
timeframes, costs, delays, and bottlenecks (Martinho
et al., 2016). These information are based on au-
thentic data stored within the information system (IS).
For all these reasons BPM methodology is one of the
most used methodologies to optimize many aspects of
healthcare system and/or regarding the e-health sys-
tem processes (Amantea et al., 2020b; Amantea et al.,
2022b; Amantea et al., 2021; Sulis et al., 2019).
SIMULTECH 2024 - 14th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
424

The reorganization of processes involves three
main stages:
• The analysis of the context: the analysis is
needed to examine the current context of a pro-
cess, in order to grasp which improvements are
needed at different levels.
• The business process analysis and simulation:
the analysis examines step by step a chosen pro-
cess with the aim of creating the As-Is model of
the process. The As-Is model is used for simu-
lation and its performance indicators are used for
validation.
• The re-engineering and scenario analysis: with
the knowledge of delays, bottlenecks, and errors
in the process, a new scenario (To-Be model) is
proposed by building a process proposing differ-
ent configurations in a what-if analysis. The final
purpose is the optimization of the chosen process.
The specific functions and tasks of the process can
be addressed by a set of process performance mea-
sures (also called key performance indicators or KPIs)
(Van Looy and Shafagatova, 2016). These perfor-
mance measures usually include time, costs and re-
sources. The goal of business process analysis is
to create and specify a visual representation of pro-
cesses, such as a flowchart or a process map. The As-
Is model depicts the state of the business process as it
now exists, the graphics help in visualizing the flow
of activities and several crossroads, which are called
gateways. The gateways lead to different paths as a re-
sult of the decisions made. There is further integrated
information such as the number of human resources
carrying out the tasks, their attributes (aka schedule,
expenses, and capacity), the duration of tasks, the pol-
icy management, and the real-life workload. As a re-
sult, the stakeholders may be able to test and validate
the model by using the simulation to get an assess-
ment of the performance metrics.
3 EXPERIMENTS AND RESULTS
The context of our experiment is the “Azienda San-
itaria Locale - Torino 3 (ASLTO3), which is one lo-
cal healthcare service, a typical public health entity in
Italy. It involves a number of hospitals and territorial
hubs in specific areas of Italian regions. They provide
public health services to the population of a specific
area in Piedmont. In this paper we only take into con-
sideration a department, the radiology department, of
the ASLTO3. This means that our experiment has
been conducted on all the radiology departments of
hospitals and territorial hubs that fall under the au-
thority of the ASLTO3. The digitalization experiment
will take into consideration the paper process of ad-
ministrative documents, not diagnostic documents or
medical records. The medical staff is shared between
hospitals and territorial hubs. All the medical staff
pertain to the ASLTO3 as a whole and thus it operates
in every structure. As for this centralization, the cost
center and the archive are the same for all the radiol-
ogy departments.
3.1 The Processes
Figure 2 shows the the current (As-Is) administrative
process carried out both in the hospital and in the terri-
torial hub in the radiology department. In both cases,
they need to print the prescriptions and the informed
consent for the exams in order to archive them. In
particular, at administrative level, when the patient ar-
rives he/she is asked what exam should be done, the
identity documents, and the prescription. The patient
can have printed or online prescription. If it is printed
on paper, a code is printed for the specifications of
the exam and the procedure of acceptance records the
presence of the patient in the ward. If the prescription
is digital, the administrative workers still have to print
a paper version as the current legislation provides for
the retention in paper of the prescriptions of any the
exams carried out at the hospital. In the hospital and
in the territorial hub the administrative procedure is
almost the same, the difference is the amount of staff
dedicated to such task. In the hospital 2 or 3 adminis-
trative workers are dedicated to it, while in the territo-
rial hub there is just 1 administrative or even just the
X-ray technician. Finally, there are different typolo-
gies of exams.
Figure 1 shows the To-Be process, an optimized
version of the current process with the time, printing,
and archiving adjustments. This scenario implies that
the internal protocol is updated and harmonized with
national and EU standards on digitalization, making
full digitalization possible.
In detail, there can be two different scenarios be-
cause we are trying to digitalize two types of docu-
ments: the prescriptions and the informed constent.
The prescriptions are easier to digitalize because they
need a server for the storage (complying with the
GDPR), some protocols and legal documents just at
an internal level. The server already exists and in-
formed consents need more legal adjustments at re-
gional and national level. Therefore, being two differ-
ent procedures, if we can digitalize the prescriptions,
it does not automatically mean that informed consent
can be digitalized as well. In conclusion, if everything
Eco-Sustainability and Efficiency of Healthcare Complex Systems
425
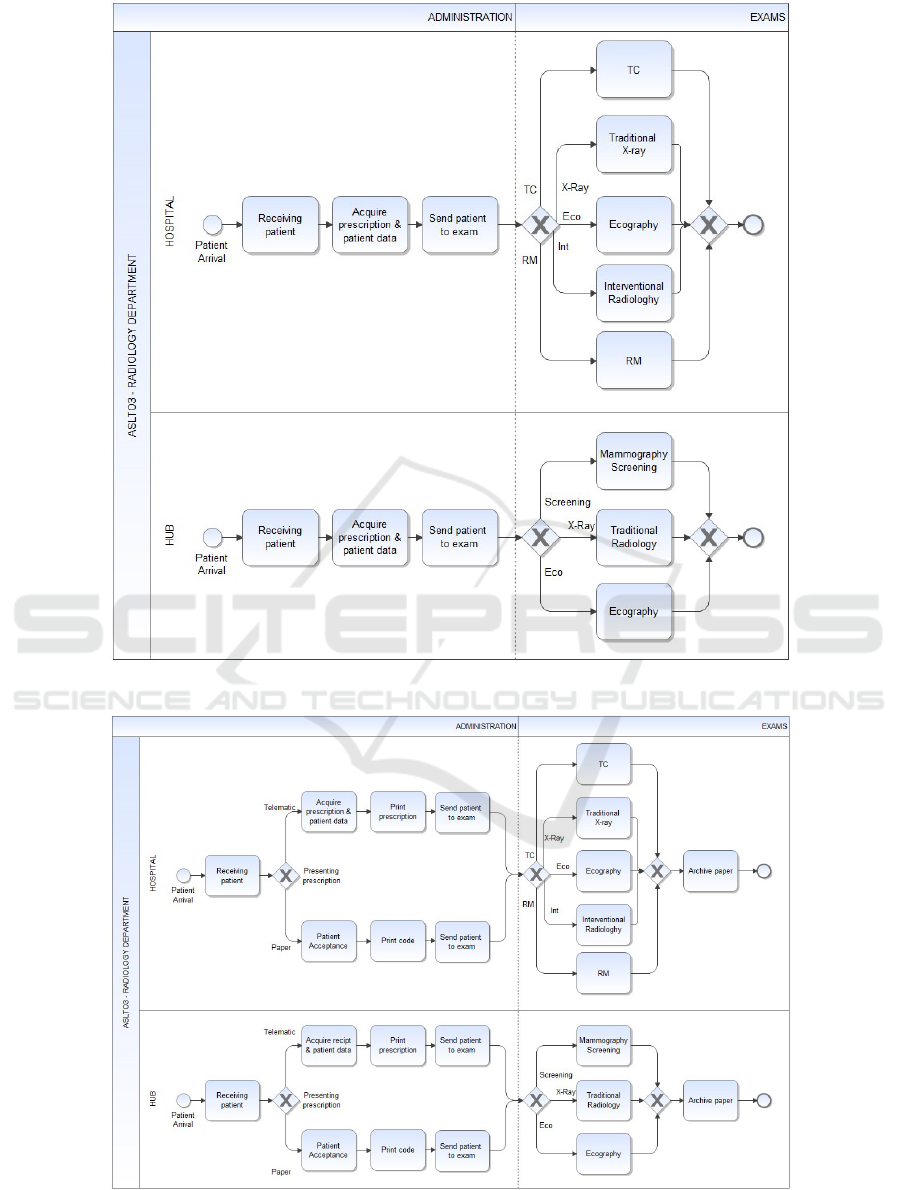
Figure 1: Digital process. To-Be process.
Figure 2: Paper process. As-Is process.
SIMULTECH 2024 - 14th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
426
will be digitalized the process will appear exactly as
Figure 1, else the activity “Archive paper” will still
appear.
3.2 The Simulations Setup
The ASLTO3 is made by 3 hospitals and 4 territorial
hub. For reasons of space, we decided to take into
consideration the data of the radiology department re-
lated to one of the hospitals and one of the territorial
hubs.
The generators of simulations are set up with an
average of 29,694 incoming patients for the hospi-
tal and an average of 14,080 patients for the territo-
rial hub in one year. Finally, in Table 1 there is the
percentage of each type of exam conducted in a year
in the hospital, while territorial hub percentages are
shown in Table 2.
Table 1: Percentage of each type of exam made in Hospital.
Exams type Percentage
X-Rey 45.6%
TC 28.8%
Eco 20%
RM 4%
Interventional 1.6%
Table 2: Percentage of each type of exam made in territorial
hub.
Exams type Percentage
X-Rey 92.2%
Eco 7.3%
Screening 0.5%
The considered paper cost is related to the pre-
scriptions and the informed consent.
The prescriptions are needed for most of the ex-
ams, but not all the exams. The same goes for in-
formed consent, it is not always needed as it is related
to the level of risk of the medical exam. The informed
consent does not always have the same format, it can
change in relation to the exam.
3.3 Comparisons and Results
In the healthcare sector, in our case in the radiol-
ogy department, there are many interconnected fac-
tors that impact and depend on each other, such as
activities, time, costs, number of papers, and archive
space. Below we will analyze them individually and
then follow with final observations.
3.3.1 Activities and Time in the Processes
Activities. Comparing Figure 2 and Figure 1 is vis-
ible that if the prescriptions can be just digital, the
paper branch will disappear and, in the digital branch,
of course, will disappear also the activity “Print pre-
scription”.
Finally, at the end of the To-Be process, the ac-
tivity “Archive paper” will disappear. This, however,
will only come as a consequence of several adjust-
ments.
To make such activity disappear both the digital-
ization of the prescriptions and the digitalization of
the informed consents are needed. In case only pre-
scriptions are digitalized the archive activity would
remain. Also, this scenario is only possible if there
were legal interventions at the national level to har-
monize the digitalization of informed consents, which
would as well make them visible in the electronic
health record of each patient. Only in this scenario
it would be possible to delete the storage task.
Time. With the change of the activities, the working
time will be affected. In this case, the simulation is
related to the working time of the administrative staff
and not to the working time of exams themselves. The
working time of exams can only be affected by clini-
cal variables.
Excluding first-aid patients, the radiology exams
considered in this paper, exclusively cover booked pa-
tients and hospital patients. Patients tend to have an
order of arrival staggered according to the established
time of the clinical exams. Therefore, those waiting
times are not so representative. They are mostly re-
lated to delays in the arrival of external patients or
delays in the transport of patients from the hospital
wards.
What is affected is the time in the sequence of the
activities of acceptance:
1. “Receiving patient” + “Acquire prescription &
patient data” + “Print prescription” + “Send pa-
tient to exam”
2. “Receiving patient” + “Patient Acceptance” +
“Print code” + “Send patient to exam”
3. “Receiving patient” + “Acquire prescription &
patient data” + “Send patient to exam”
The first two are related to the current paper process
(As-Is) branches and the last one is related to the dig-
ital process (To-Be).
Table 3 shows a comparison between the current
process (As-Is) and the digital process (To-Be). The
simulation results of both processes is expressed in
the administratives’ working time (in minutes) per pa-
tient.
Eco-Sustainability and Efficiency of Healthcare Complex Systems
427
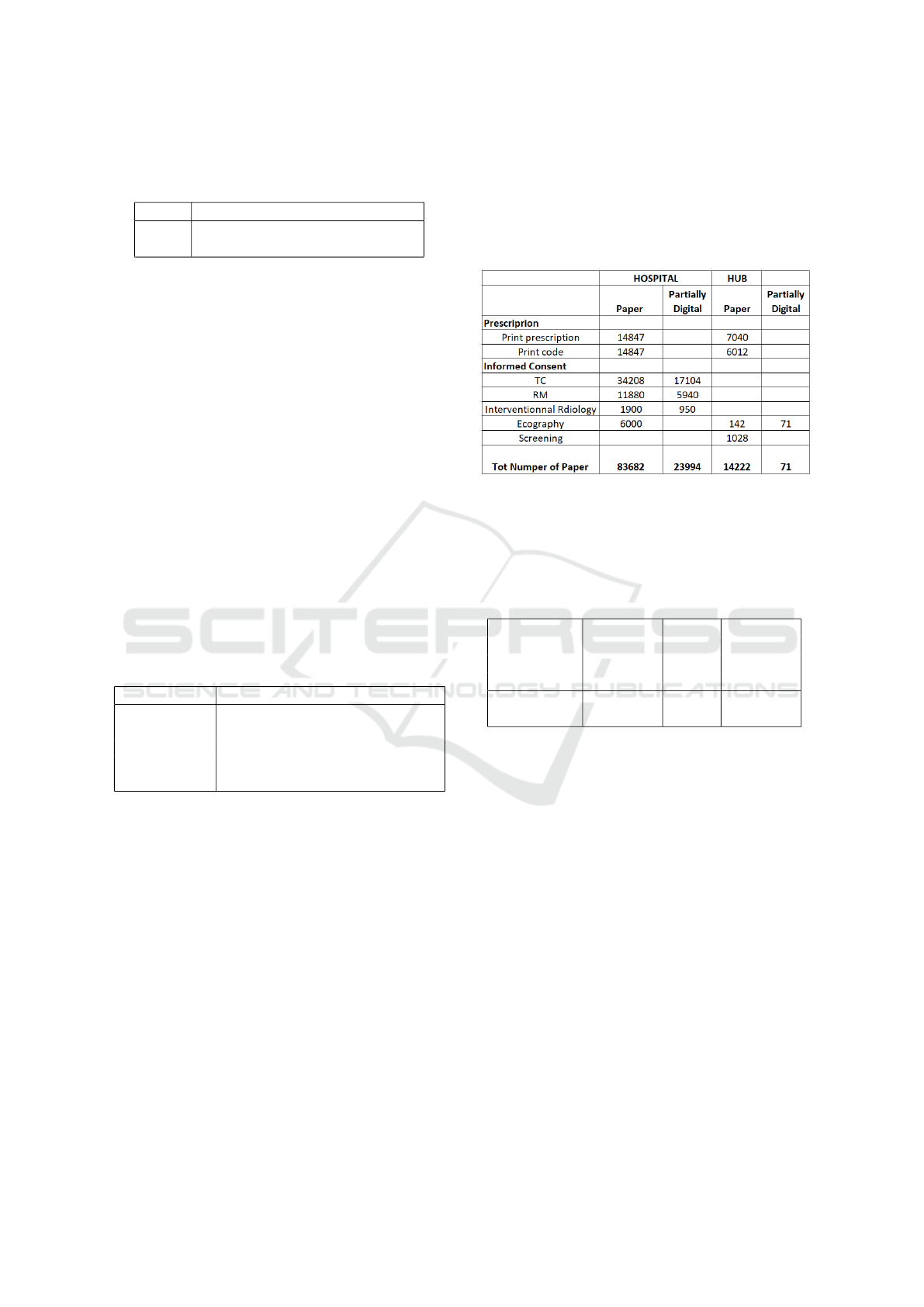
Table 3: Comparison between the current process (As-Is)
and the digital process (To-Be) simulations results of the
administrative working time (in minutes) per patient.
Average Working Time per patient
As-Is 2.37 minutes
To-Be 1.66 minutes
3.3.2 Number of Paper Prints and Costs
Number of Paper Print. To understand this point we
need to make two premises:
• Prescriptions are required for each exam except
for preventive screenings, where patients receive
invitations at home. If a patient arrives with a dig-
ital prescription, administrative staff must print it
for archiving purposes. If the patient has a pa-
per receipt, a code must be printed and stapled to
the prescription, counting as a second sheet. Le-
gal compliance for prescriptions can be managed
with internal adjustments.
• Informed Consents are not required for all ex-
ams, and for those that do, the format and number
of pages vary. Informed consent forms must be
printed in duplicate: one copy for the patient and
one for the healthcare facility. Table 4 provides a
summary of this information.
Table 4: Paper pages needed for the informed consent for
type of exam.
Exams type Printed pages for informed consent
TC 2 (X2)
Interventional 2 (X2)
Eco 2 (not for all exams) (X2)
Screening 1 (X2)
RM 5 (X2)
In this case, the simulation helps us to understand the
extent of the potential savings and present an argu-
ment in support of the legislative harmonization for
digitalization of informed consent and prescription.
If the harmonization becomes effective, the simulated
savings will become effective.
The simulation results reported in Figure 3 show
the number of papers that are printed on average in
one year for the prescription, and the same for in-
formed consent. They both are presented in relation
to the hospital and to the territorial hub.
The digitalization of the prescriptions and of the
informed consent are two different procedures. Thus,
there will likely be an intermediate situation (i.e. the
“Partially Digital” scenario) in which all the prescrip-
tions are digital but not the informed consent. The
informed consent could be sent online to the patient,
while it should be archived in a paper format. This
means that there is still a paper copy to be taken into
consideration for the informed consent. However,
there would be a relevant reduction in paper which
is evident in Figure 3.
Of course, in case of fully digitalization the
amount of paper would be zero.
Figure 3: Number of paper used in the hospital and in
the hub in the AS-IS (“Paper”) situation and in the To-Be
(“Partially Digital”) situation. Related to the prescriptions
and to the informed consents.
Table 5: Paper pages saved using the partial digitalization
and the full digitalization, expressed in number of pages and
in percentage concerning the current situation.
Saving N. in% Saving N.
of paper of paper
Partially Fully
Digital Digital
Tot Hospital 59,688 71.3% 83,682
Tot hub 14,151 99.5% 14,222
In conclusion, starting from Figure 3, Table 5
shows that just with partial digitalization, i.e. dig-
italize the prescriptions and the informed consents
for the hospital, printing just the copy for the hospi-
tal archive, “Partially Digital”) almost 60,000 paper
sheets will be saved in the hospital and almost 1,500
in the hub. With a full digital system, almost 85,000
paper sheets will be saved in the hospital and almost
14,000 in the hub.
Costs. Figure 4 reports the results of the simulation
on costs for the hospitals and the hub. These are re-
lated to the cost of the paper and the printing costs
in proportion to hard copies. The Figure also shows
a comparison between the As-Is and the To-Be “Par-
tially Digital ” scenario.
Also in this case, if all informed consents can be
filled out, signed, and kept totally in digital, the cost
of printing and paper would be zero.
In conclusion, starting from Figure 4, Table 6
shows that just with partial digitalization, i.e. digi-
talize the prescriptions and the informed consents for
SIMULTECH 2024 - 14th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
428
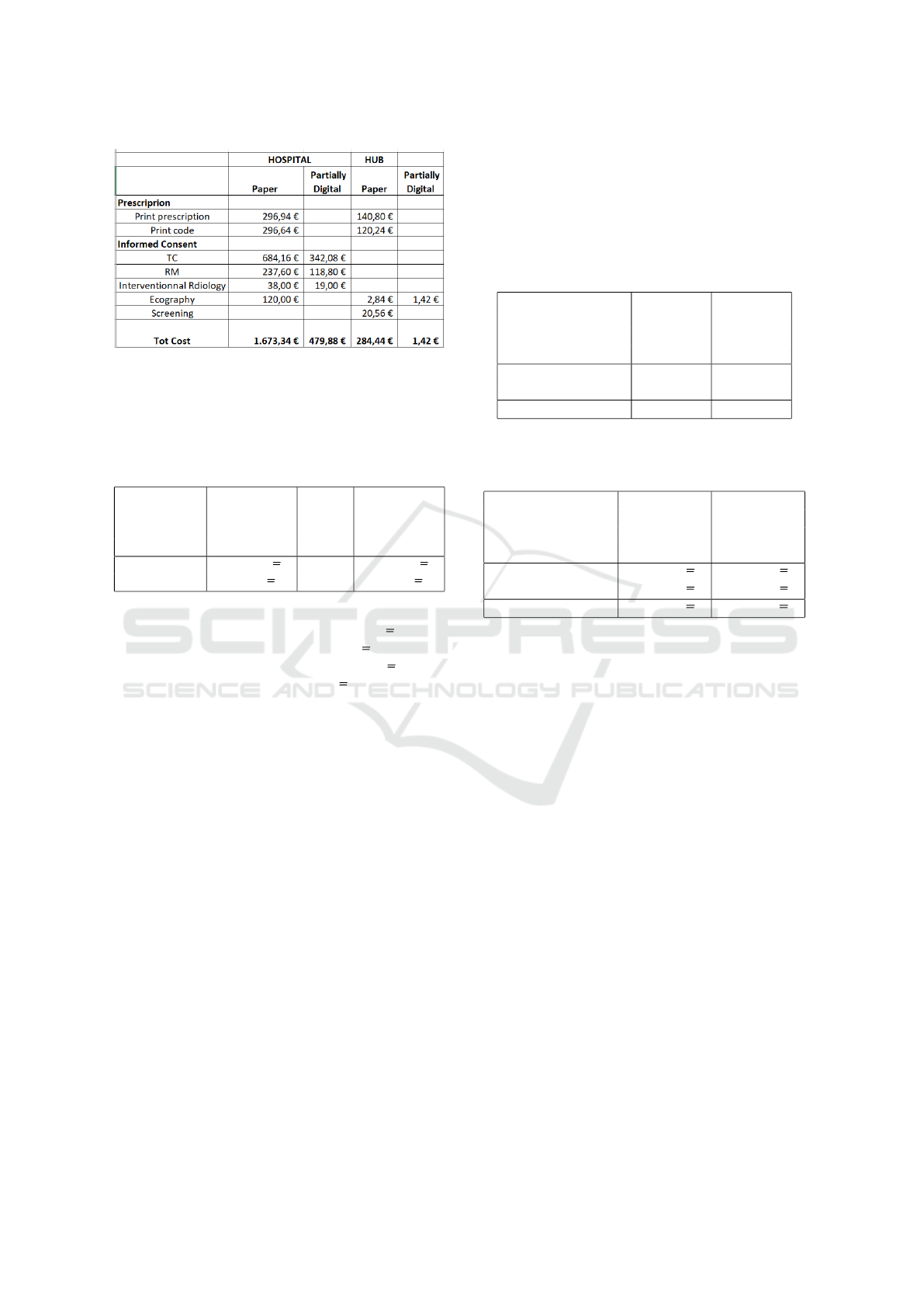
Figure 4: Cost of paper consuming and printing costs re-
lated to the AS-IS (“Paper”) situation and in the To-Be
(“Partially Digital”) situation, divided for prescriptions and
informed consents.
Table 6: Costs saved using the partial digitalization and the
full digitalization, expressed in Euro and in percentage con-
cerning the current situation.
Saving Cost in% Saving Cost
in euro in in euro in
Partially Fully
Digital Digital
Tot Hospital 1,193.46C 71.3% 1,673.34C
Tot hub 283.02C 99.5% 284.44C
the patient, so printing just the copy for the hospital
archive (“Partially digital”) almost 1193.46 C will be
saved in the hospital and almost 283.02C in the hub.
While with a full digital system almost 1600 C will be
saved in the hospital and almost 300 C in the hub.
3.3.3 Archive
Removing physical storage in healthcare facilities
has several benefits. It eliminates the need for file
placement and manual searching, which can be time-
consuming and require multiple staff members. Dig-
ital databases allow for quick retrieval of files within
seconds. Physical storage demands large spaces in
healthcare buildings and poses risks such as docu-
ment loss, damage from fires or flooding, and the
need for regular disposal to make room for new doc-
uments. With the increasing number of required doc-
uments due to technological advancements, the need
for larger storage spaces is growing
3.3.4 Final Remarks
All the simulations shown until now are related to one
hospital and one hub of the radiology department.
As remarked before, the ASLTO3 involves 3 hos-
pitals and 4 hubs, which implies that both the cost
center and the archive are centralized for all the radi-
ology departments. Our aim is to show the impact of
the digitalization of just these two documents of one
department on the cost center and the archive of the
ASLTO3. Table 7 and Table 8 show respectively the
possible number of saving sheets paper and the possi-
ble saving costs for the ASLTO3.
Table 7: Paper pages saved using the partial digitalization
and the full digitalization, expressed in number of pages and
in percentage concerning the current situation.
Saving N. Saving N.
of paper of paper
Partially Fully
Digital Digital
Tot ASL Hospitals 179,064 251,046
Tot ALS hubs 56,604 56,888
Tot ASL 235,668 307,934
Table 8: Costs saved using the partial digitalization and the
full digitalization, expressed in euro concerning the whole
ASLTO3.
Saving Cost Saving Cost
in euro in in euro in
Partially Fully
Digital Digital
Tot ASL Hospitals 3,580.38C 5,020.02C
Tot ALS hubs 1,132.08 C 1,137.76C
Tot ASL 4,712.46C 6,157.78 C
Although the single results shown may not be im-
pressive, the impact of all these interconnected factors
is relevant. We only took into consideration two ad-
ministrative documents among all administrative doc-
uments, we excluded medical documents, and our
scope got as far as only one hub and one hospital
among all the ASLTO3. Also, these administrative
documents only came from the radiology department
of the chosen hospital and hub. This means that what
is saved in terms of time and costs in this scenario ex-
ponentially grows if adopted in the whole ASL TO3.
This is shown in Table 7 and Table 8. Table 7 refers
to savings in number of hard copies, wheres Table 8
refers to saving in costs. Using paper not only creates
a physical and printing cost but also creates a storage
space problem.
Saving time in healthcare facilities leads to a cas-
cading effect by freeing up staff to handle other tasks,
address bottlenecks, and increase available human re-
sources. Cost savings can be redirected to invest in
medical equipment or additional staff, improving both
care quality and work conditions by reducing over-
time and balancing workloads. This results in better
patient care, fewer errors, and higher patient satisfac-
tion, which can reduce legal complaints.
With technological advancements come new legal
standards, particularly for health data, requiring more
Eco-Sustainability and Efficiency of Healthcare Complex Systems
429

administrative documents and storage space. Switch-
ing to digital databases eliminates the need for addi-
tional storage, repurposing current storage areas for
medical use and cutting costs. Additionally, new doc-
uments require more storage space, increasing the
costs of renting adequate places. Digital databases
cut these costs, eliminating the need for new storage
spaces and allowing current storage areas to be repur-
posed for medical rooms or storage.
In Italy, the healthcare system is public, which
means it is publicly funded. If optimizing document
management in just one department can have a sig-
nificant positive impact on public services and funds,
it also has the potential to bring massive benefits on
a national scale. This optimization currently involves
only 1 ASL out of 12. Considering that Italy has 20
Regions, and Piedmont is just one region, this type of
optimization could bring to the whole public service
and public funds a great impact in scale.
4 CONCLUSIONS AND
IMPLICATIONS
This work shows the interconnection, the analysis,
and the impact of multiple factors in the complex ter-
ritorial health system.
It has been demonstrated that in the medical field,
digitalizing just two administrative documents (non-
clinical) of just one department would have a consid-
erable impact on activities, time, costs, number of pa-
per files, and storage spaces throughout the territory.
The successful optimization of administrative health-
care activities is fundamental as it can be expanded
proportionally and exponentially throughout the en-
tire national territory. The interconnection of factors
brings a cascading optimization effect, bettering the
entire health service on multiple fronts. Last but not
least, these kinds of optimizations are indispensable
to align with the digitization and eco-friendliness re-
quired by the European Union. In the next future, we
will continue this collaboration with ASLTO3 to try
to implement the digitalization of the prescriptions.
REFERENCES
Amantea, I. A., Di Leva, A., and Sulis, E. (2020a). A
simulation-driven approach to decision support in pro-
cess reorganization: A case study in healthcare. In Ex-
ploring Digital Ecosystems, pages 223–235. Springer.
Amantea, I. A., Quaranta, M., Molinari, M., Peduto, C.,
and Demarchi, F. (2023). The e-dossier as a tool to
optimize civil courts: The cuneo case. In In Proceed-
ings of the 13th International Conference on Simula-
tion and Modeling Methodologies, Technologies and
Applications, pages 425–431.
Amantea, I. A., Robaldo, L., Sulis, E., Boella, G., and
Governatori, G. (2021). Semi-automated checking for
regulatory compliance in e-health. In 2021 ieee 25th
international enterprise distributed object computing
workshop (edocw), pages 318–325. IEEE.
Amantea, I. A., Robaldo, L., Sulis, E., Governatori, G.,
and Boella, G. (2022a). Business process modelling
in healthcare and compliance management: a logi-
cal framework. Journal of Applied Logics—IfCoLog
Journal of Logics and their Applications, 9(4).
Amantea, I. A., Sulis, E., Boella, G., De Marchi, F., Mazz-
ini, L., Alloatti, F., and Bolioli, A. (2020b). Adopting
assistive technologies in healthcare processes: a chat-
bot for patients with amyotrophic lateral sclerosis. In
Italian forum of ambient assisted living, pages 163–
174. Springer.
Amantea, I. A., Sulis, E., Boella, G., Marinello, R., Grosso,
M., and Crespo, A. (2022b). A modeling frame-
work for an innovative e-health service: the hospi-
tal at home. In Simulation and Modeling Method-
ologies, Technologies and Applications: 10th Inter-
national Conference, SIMULTECH 2020 Lieusaint-
Paris, France, July 8-10, 2020 Revised Selected Pa-
pers 10, pages 111–132. Springer.
Dumas, M., La Rosa, M., Mendling, J., and Reijers, H.
(2018). Fundamentals of business process manage-
ment, volume 1. Springer, 2nd edition.
Dumas, M., van der Aalst, W. M., and ter Hofstede, A. H.
(2005). Process-aware Information Systems: Bridg-
ing People and Software Through Process Technology.
John Wiley & Sons, Inc., New York, NY, USA.
Ladyman, J., Lambert, J., and Wiesner, K. (2013). What is
a complex system? European Journal for Philosophy
of Science, 3:33–67.
Martinho, R., Domingos, D., and Resp
´
ıcio, A. (2016). Eval-
uating the reliability of ambient-assisted living busi-
ness processes. In ICEIS (2), pages 528–536.
Motter, A. E. (2004). Cascade control and defense
in complex networks. Physical Review Letters,
93(9):098701.
Sulis, E., Amantea, I. A., Boella, G., Marinello, R., Bianca,
D., Brunetti, E., Bo, M., Bianco, A., Cattel, F., Cena,
C., et al. (2019). Monitoring patients with fragilities in
the context of de-hospitalization services: an ambient
assisted living healthcare framework for e-health ap-
plications. In 2019 IEEE 23rd International Sympo-
sium on Consumer Technologies (ISCT), pages 216–
219. IEEE.
Sulis, E. and Di Leva, A. (2017). An agent-based model
of a business process: The use case of a hospital
emergency department. In International Conference
on Business Process Management, pages 124–132.
Springer.
Van Looy, A. and Shafagatova, A. (2016). Business process
performance measurement: a structured literature re-
view of indicators, measures and metrics. Springer-
Plus, 5(1):1797.
SIMULTECH 2024 - 14th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
430
