
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care
Planning
Seyedamirhossein Salehiamiri
a
, Richard Allmendinger
b
and Arijit De
c
Alliance Manchester Business School, University of Manchester, Manchester, M15 6PB, U.K.
Keywords:
Home Health Care, Internet of Medical Things, Computational Intelligence, Care Planning.
Abstract:
The number of home caretakers is rising rapidly due to an increasing number of elderly people, recent pan-
demics, and the advancement of home health care facilities. Wearable medical devices and the Internet of
Medical Things (IoMT) help health care managers monitor patients in real-time and provide remote medical
care. This reduces home visits and helps Home Health Care (HHC) companies plan their resources. The paper
addresses the HHC planning problem of allocating the optimal number of experts to patients while minimising
the delay in visiting the patient, matching medical expertise with patient needs, and identifying the patient’s
visit sequence. To tackle this, a new mixed-integer mathematical problem is proposed to reduce the total visit
time for patients. This paper makes three key contributions towards tackling this plan, including (i) providing
a formal definition of the problem and putting it in context with related work, (ii) proposing multiple problem
instances varying in complexity, and (iii) an initial analysis of several heuristics and an exact solver (CPLEX)
on these problem instances. The results indicated that the application of computational intelligence combined
with IoMT can reduce patient visitation time significantly in a daily plan and therefore lead to 3.7 percent
improved care for HHC patients.
1 INTRODUCTION
Supply chain management is an important component
of sustainable development and plays a key role in
optimising various systems. The Home Health Care
(HHC) system has recently attracted the attention of
various systems and settings since it deals with hu-
man lives and supply chain considerations (Reddy
et al., 2022). Inefficiencies in home health care sys-
tems and their supply chain operations have signifi-
cant impacts on human lives worldwide. In the con-
text of home health care, research has shown that
nurses spend a considerable amount of time on non-
clinical supply chain duties, indicating inefficiencies
in the system (De Vries and Huijsman, 2011; Vervoort
et al., 2021). This system could save a human life, es-
pecially when patients with traumatic diseases need
timely and justified services from the comfort of their
homes (Nikzad et al., 2021). Hence, efficient use of
supply chain networks (including expert home carers,
patients, and HHC organisations) could improve the
a
https://orcid.org/0000-0001-5980-8192
b
https://orcid.org/0000-0003-1236-3143
c
https://orcid.org/0000-0002-0361-5911
effectiveness of HHC systems, since the daily demand
for home care is increasing.
Nowadays, patient monitoring and care are crucial
to recovery. Some organisations offer real-time pa-
tient monitoring and data recording by employing ap-
plications to both reduce their costs and face the chal-
lenges of meeting the growing demands of patients.
Technologies used to monitor patients with HHC
have shown significant benefits in reducing mortal-
ity rates (Polisena et al., 2010). Athelas is a lead-
ing provider of patient monitoring systems (Athelas,
2003). Patients carry sensitive data about their health,
which requires more layers of protection. Therefore,
a new form of IoT (Internet of Things) for health care
has emerged: IoMT (Internet of Medical Things). If
any results are beyond the normal range, the patient
immediately receives an alert from the nursing staff
for further follow-up medical treatments (Dwivedi
et al., 2022).
The motivations behind using the IoMT concept
are to perform real-time patient monitoring and plan
patient visits. A real-time device is attached to the pa-
tient’s body according to their chronic diseases. This
device not only monitors patients daily, but can also
perform certain health care activities, such as remote
72
Salehiamiri, S., Allmendinger, R. and De, A.
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care Planning.
DOI: 10.5220/0012938900003837
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 16th International Joint Conference on Computational Intelligence (IJCCI 2024), pages 72-83
ISBN: 978-989-758-721-4; ISSN: 2184-3236
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.

monitoring of the patient’s heart rate and administer-
ing certain types of medicine. In contrast to earlier re-
search on HHC supply chain network planning (see,
e.g., (Ait Haddadene et al., 2019; Goodarzian et al.,
2021; Fathollahi-Fard et al., 2022)), IoMT responds
quickly to changes in the schedule and can resched-
ule the current plan as needed.
The contributions of the study include a new math-
ematical model considering allocating skill-based
nurses to HHC patients based on different service
menu, developing multiple metaheuristic algorithms
suitable to solve the problem, and considering real-
time changes to verify the applicability of the IoMT
plan.
Therefore, in this study, a methodology for IoMT
wearable devices is first proposed. The problem aims
to assign an optimal number of experts to various pa-
tients requiring service while minimising the total vis-
itation time, determining the daily plan and visitation
intervals. The term “threshold intervention level” is
used to identify patients with conditions of the high-
est severity. Finally, several metaheuristics that de-
pend on different concepts are adapted to the prob-
lem and benchmarked on several realistic problem in-
stances that vary in complexity.
The proposed mathematical problem considers
various inputs and settings, such as using con-
straints considering the patient’s time window, mul-
tiple choices to assign nurses, the Patient’s Service
Menu (PSM), and the uncertain nature of the pro-
posed IoMT plan. In contrast to previous studies,
each patient has its own unique time window for the
visit and requires specific services among the range
of services. First, we adapt the well-established Sim-
ulated Annealing (SA) and Particle Swarm Optimisa-
tion (PSO) to tackle the problem and serve as base-
lines. We then introduce a new co-evolutionary Parti-
cle Swarm Optimisation (CPSO) algorithm to explore
if a more sophisticated approach translates into better
performance (measured in terms of solution quality).
Several problem instances, varying in size, are intro-
duced to validate the performance of the three search
algorithms and an exact solver (CPLEX).
The organisation of the paper is as follows. The
next section provides the reader with a comprehen-
sive literature review of related works. The proposed
IoMT methodology and mathematical modelling are
presented in Section 3. Section 4 includes the opti-
misation strategy and the experimental results of the
metaheuristics. Finally, Section 6 concludes the paper
and discusses future work.
2 LITERATURE REVIEW
The research field on HHC management is not new.
However, there is a growing trend in HHC research
to consider decision-making and management science
approaches.Most HHC supply chain papers have fo-
cused on creating a strategic framework. According
to (Landers et al., 2016), 52 percent of patient trans-
actions are conducted online, virtual or through an
app. As a result, more studies are needed to fill this
gap and address the transition from traditional care to
HHC. This section represents an overview of the rel-
evant literature on HHC followed by a discussion of
research gaps in HHC.
Routing and Scheduling Problems. Most cur-
rent studies in the field of HHC supply chain net-
work design employ new algorithms or introduce new
methodologies to solve their proposed mathematical
modelling. The study of Fard et al. (Fathollahi-Fard
et al., 2018) addressed a green HHC vehicle rout-
ing problem by using a mixed-integer linear program-
ming model to reduce expenses and green emissions.
Using the Lagrangian relaxation procedure, Decerle
et al. (Decerle et al., 2018) solved HHC routing and
scheduling for many time windows using a memetic
algorithm. The results of the problems were promis-
ing. Shi et al. (Shi et al., 2019) proposed a ro-
bust optimisation problem for an HHC plan and com-
pared the results in a deterministic setting. Math-
ematical programming was used to minimise vehi-
cle route logistics expenses per visitation. Bahadori
et al. (Bahadori-Chinibelagh et al., 2022) addressed
multi-depot routing programming for HHC optimi-
sation to reduce transportation costs. The study as-
sumed that routing rates must be limited. The model
was flexible and effective under different conditions
due to two constructive algorithms. The scheduling
of HHC staff under uncertain conditions was inves-
tigated in (Restrepo et al., 2020). The objective was
to minimise work shift costs by achieving optimal al-
location, reducing shift-changing penalties, and ex-
pecting recourse. Having an optimised routing and
scheduling plan can be most beneficial when having
access to the required resources. Therefore, alloca-
tion models are needed to overcome problems such as
nurse workloads, time window, and fair distribution
of resources. However, assigning the optimal number
of resources based on the patient’s condition has been
overlooked.
Allocation Problems. The use of location-allocation
problems can be seen in the design of recent HHC
supply chain networks. For instance, in (Rodriguez-
Verjan et al., 2018; Lin et al., 2018) a location-
allocation problem is proposed to both locate the
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care Planning
73

HHC centres and reduce the total cost of resources
and facilities. The authors used mixed-integer lin-
ear programming, as in (Xiao et al., 2018), to ad-
dress the HHC problem. However, the utilised time
window is not able to address real-time changes as
it is assumed to be fixed. The application of location-
allocation problems is quite limited in the literature of
HHC. In addition, allocating nurses to patients based
on the PSM is ignored in this sense.
Metaheuristics for HHC Applications. The appli-
cation of metaheuristics has been highlighted in pre-
vious studies. Erdam et al. (Erdem and Koc¸, 2019)
addressed HHC patients with electronic vehicle rout-
ing challenges and their limitations. The problem was
to optimise travel time and the number of nurses. In
the analysis, metaheuristics based on genetic algo-
rithms and variable neighbourhood search performed
better. Other studies (eg (Decerle et al., 2019b; De-
cerle et al., 2019a)) considered using metaheuristics
such as non-dominated sorting genetic algorithm II
(NSGA-II) and an evolutionary approach like multi-
directional local search (MDLS) to optimise working
time and quality of service, respectively.
Bi-objective programming could reduce routing
time and reduce costs in an HHC system, according
to (Khodabandeh et al., 2021). The epsilon-constraint
method verifies the results of the problem. In (Er-
dem and Koc¸, 2022) a hybrid algorithm is proposed
to address the problem of HHC with electronic ve-
hicles. Promising results were reported for complex
routing problems. In (Xiang et al., 2023) a routing
and scheduling HHC problem that accounts for the
patient’s preference was considered. The cost ob-
jective is minimised using hybrid NSGA-II, which
proved to be better than the e-constraint method.
In summary, there is a research gap in that the ap-
plication of IoMT and real-time changes has not yet
been considered in the existing literature (Fikar and
Hirsch, 2017; Emiliano et al., 2017; Dwivedi et al.,
2021). This study first proposes a dynamic and real-
time plan using IoMT in a smart platform environ-
ment to enable online and instant decision-making
during an unexpected patient emergency scenario.
Previous studies insisted on routing and scheduling,
such as (Di Mascolo et al., 2021), or defined a new so-
lution strategy to address HHC problems, such as (Liu
et al., 2021). Only a few studies have used an alloca-
tion strategy to assign the optimal number of nurses
to each patient. Furthermore, this work is the first to
propose (and account for in optimisation) a combina-
tion of different time windows, patient service menus,
and service levels for experts.
3 FORMAL PROBLEM
DEFINITION
HHC monitors and improves patient care using med-
ical records, such as age, sex, symptoms, vital signs,
trauma, and others. HHC technologies, including
wearable devices, allow real-time patient monitor-
ing, medical data storage, and remote care (McGillion
et al., 2020). Therefore, HHC resources are allocated
when needed and patients are served more efficiently.
Each patient starts the day with the expectation of cer-
tain services. The HHC sector has many experts that
can be assigned to these patients, but each expert can
only provide specific medical care.
In summary, the proposed methodology has the
following steps:
• Phase one - System installation: The phase is
centred on using the HHC system with IoMT,
which calls for the mobilisation of actual indus-
try 4.0 systems—computers, software, and wear-
ables—for patient programming, monitoring, and
analysis.
• Phase two - Diagnosis: Wearable Internet of
Things (IoMT) devices can diagnose symptoms,
monitor patient status, and provide remote med-
ical treatment, therefore saving time and money.
They are able to forecast when to intervene and
alert medical staff before the patient’s condition
deteriorates. A specified Threshold Intervene
Level (TIL) enables the wearable device to proac-
tively assess and store real-time patient conditions
in a cloud-based data centre. With expert des-
ignations for every patient, this system uses past
data, real-time diagnosis, and patient observation
to identify and forecast urgent conditions.
• Phase three - Provide healthcare: Depending on
TIL, the IoMT wearable devices distinguish be-
tween patient severity levels. The technology
tracks and saves real-time data if the level is less
than TIL. Patients can also push a button to re-
quest assistance if it goes beyond TIL, and an ex-
perienced home health carer is dispatched.
Considering the proposed methodology, IoMT in
HHC is a network of connected devices in which
patient monitoring is done using secured network
based on internet. This provides online and instant
monitoring of each patient. On the other hand,
TIL is a critical parameter in which determines the
health condition of each patient separately. IoMT
and TIL are interconnected in the proposed HHC
problem since IoMT alerts the HHC staff based
on instant changes of patient’s condition given
the TIL level. Current study only focuses on the
ECTA 2024 - 16th International Conference on Evolutionary Computation Theory and Applications
74

scheduling aspect of the HHC as the main prob-
lem that HHC companies dealing with specially in
Canada. Therefore, this study considers schedul-
ing for the HHC patient without taking into ac-
count machine learning or triggering mechanism.
However, these will be a part of future develop-
ment of the current study. Given the current nature
of the problem and considering the IoMT changes
in a real-time manner, this setup can be utilised
in US and UK considering their challenges in the
HHC sector (Statista, 2020).
The objective of the HHC planning problem is to
assign experts to HHC patients based on their ser-
vice requirements. Patients expect the HHC system
to provide home medical care, and accordingly the
HHC manager matches experts who possess a par-
ticular medical expertise with patients requiring that
specific medical care. In other cases, interventions
such as prompt visits to patients in extreme cases are
allocated by the HHC system. The HHC system pro-
vides remote medical care in specific cases, thereby
reducing patient visit costs and time.
Following discussions with carers and medics, we
have developed the following (formal) problem state-
ment to capture the essence of the problem: In this
problem, two factors determine the number of home
health carers to be assigned per day based on the pa-
tient’s service requirement and time window. The ob-
jective is to reduce the visitation time associated with
the experts serving the patients. It should be noted
that the assignment of experts takes place only if they
have the required skills to serve patients. In addition,
only a limited number of resources are available each
day. Therefore, based on the structure of the proposed
HHC, the following assumptions can be considered:
• Each patient has a specific service menu that must
be served during the day.
• Only one expert home carer must be assigned to
each patient.
• An expert would be assigned to a patient only if
the person has the required medical skill to serve
the patient.
• An expert is sent to a patient only if the threshold
severity level goes beyond the real-time severity
level.
• The number of experts available is fixed and lim-
ited each day.
Table 1 provides an overview of the problem pa-
rameters: Lim
Tr
is based on time and signifies the
travel time that has to be bounded due to the suppo-
sitions of the problem. Furthermore, INT
i
defines the
Table 1: Problem parameters and definitions.
Notations Definition
e = 1,.. . ,E Set of expert home caregivers
i, j,h = 1,... , P Set of patients
k = 1, . .. , K Set of all periods (days)
ϕ = 1, ... , j Set of all visits
Parameters Definition
TrT
i, j
Travel time visits of patients i and j
ViT
i
The time duration in which patient i must be visited
PT The penalty time
EV
i
The earliest visit of patient i
LV
i
The latest visit of patient i
Ne
i
The total number of experts
SE
ei
The skill of the expert caregiver e to visit patient i
Lim
Tr
Distance parameter to limit the travel time
DU
max
Maximum available time for expert home caregivers
λ
i
The real-time severity level of patient i
INT
i
INT
i
≥ λ
i
,1 Otherwise, 0
V B A very big number (without dimension)
Variables Definition
A
e,i, j,k
1, if expert home caregiver e is assigned to patient j
after visiting patient i in period k
ST
e,i
Starting time of in-home patient i for visitation
AT
e,i,k
The arrival time of an expert home caregiver e
threshold intervention level of the patient by a num-
ber (derived from the IoMT system and wearable de-
vices in real-time). If its value goes above λ
i
, an ex-
pert must be sent to visit the patient. Considering 1,
the proposed objective function and constraints of the
HHC problem can be expressed as below:
MinZ =
∑
e∈E
∑
i∈P
∑
j∈P−i
∑
k∈K
A
e,i, j,k
∗ (TrT
i, j
+ViT
i
) +
∑
e∈E
∑
i∈P
ST
e,i
(1)
Equation 1 defines the objective function, which
minimises visit time based on the patient’s time win-
dow. Expert home carers must adhere to the patient’s
schedule.
AT
e, j,k
≤ LV
j
∀e ∈ E, j ∈ P,k ∈ K (2)
EV
j
≤ AT
e, j,k
∀e ∈ E, j ∈ P,k ∈ K (3)
Constraints 2– 3 highlight that the unique time
window for a patient needs to be taken into consider-
ation while performing the allocation of HHC experts
to the respective patient.
∑
e∈E
∑
i∈P
∑
j∈P−i
∑
k∈K
A
e,i, j,k
= Ne
i
∀e ∈ E,i ∈ P,k ∈ K
(4)
∑
e∈E
∑
i
A
e,i, j,k
∗ SE
ei
≥ 1 ∀ j ∈ P − i,k ∈ K (5)
Constraint 4 requires all skilled expert workers to
organise and comply with expert plan visits. Whilst
Constraint 5 ensures that all skilled home carers are
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care Planning
75

assigned based on their competence and the PSM.
AT
e,i,k
+ViT
i
+ TrT
i, j
+
A
e,i, j,k
− 1
∗V B ≤ AT
e, j,k
∀e ∈ E,i ∈ P,k ∈ K
(6)
AT
e, j,k
− AT
e,i,k
−ViT
i
≤ Lim
Tr
+
1 − A
e,i, j,k
∗V B
∀e ∈ E,i ∈ P,k ∈ K
(7)
AT
e,i,k
+ViT
i
+ TrT
i,0
≤ DU
max
∀e ∈ E,i ∈ P,k ∈ K
(8)
Constraint 6 determines the time it takes an expe-
rienced home carer to reach a patient requiring medi-
cal service. It is necessary to divide expert home car-
ers by time gap to assign them to patient homes. Thus,
expert home carers must maintain a time between vis-
its. It must be noted that this is not a routing constraint
and it only divides experts using time; Constraint 7
accounts for this. Constraint 8 requires expert home
carers to work a certain number of hours each day.
∑
e∈E
∑
i∈ϕ
A
e,i, j,k
=
∑
e∈E
∑
j∈ϕ
A
e, j,h,k
∀k ∈ K,h ∈ ϕ (9)
∑
e
′
∈E
′
∑
i∈ϕ
A
e
′
,i, j,k
=
∑
e
′
∈E
∑
h∈P
A
e
′
, j,h,(k+1)
∀k ∈ K,i, j ∈ P
(10)
Here, the set ϕ = {0,1,... ,n + m} is defined to
show the total number of visits n and visit breaks
from one home to another m. If we consider pa-
tients from the set {0,1,.. ., i, j, h,..., m}, it is impor-
tant for an expert home carer to finish his/her work
at a patient’s home before visiting another patient.
Hence, Constraint 9 is utilised to overcome this is-
sue. Constraint 10 is shaped to ensure the continuity
of the assigned home care to all the expert home care-
givers.Once an expert is assigned and served a patient,
it must continue the service to other patients if possi-
ble.
∑
i∈P
A
e,i,0,k
= 1 ∀e ∈ E, k ∈ K (11)
∑
J∈P
A
e,0, j,k
= 1 ∀e ∈ E, k ∈ K (12)
ST
e,1
=
∑
i∈P
∑
j∈P
TrT
0,1
∗A
e,0,1,k
∗INT
1
∀i, j = 1 (13)
A
e,i, j,k
∈ {0, 1} ∀e ∈ E, ∀i, j ∈ P,k ∈ K (14)
AT
e,i,k
≥ 0 ∀e ∈ E, ∀i ∈ P, k ∈ K (15)
Constraints 11– 12 ensure that experts must return
to the HHC centre after visiting their patients. Con-
straint 13 defines the start time of the plan. Finally,
Constraints 14– 15 indicate binary and non-negative
decision variables, respectively.
The following methodology addresses real-time
changes in the proposed HHC planning problem:
First, the model initialises by setting the values of
TrT
i, j
, ViT
i
, PT , EV
i
, LV
i
, Lim
Tr
, and DU
max
. In each
search, it sets i = P if INT
i
≥ λ
i
. The model is then
optimised based on λ
i
to achieve an efficient assign-
ment. However, if λ
i
changes, the problem sets i = P
and e = E to their new values. Then the input value
of the model will be updated and solved.
4 EXPERIMENTAL SETUP
This section motivates and defines the experimental
setup pertaining to optimisation algorithms, their pa-
rameter settings, and test problems as used for the
subsequent experimental study.
4.1 Optimisation Strategies
To tackle the IoMT-based HHC planning problem
proposed in Section 3, we consider four different
algorithms: two established metaheuristics used as
a baseline, Simulated Annealing (SA) and Particle
Swarm Optimisation (PSO); a more recent method,
Co-evolutionary PSO (CPSO), used to understand if
we can achieve improved performance; finally, an ex-
act optimizer, CPLEX, will be used to understand the
applicability and limits of exact optimisation to the
problem.
We would expect the exact solver to do well on
small and medium-sized versions of the problem but
to be computationally intractable for larger problems,
providing a sweet spot for metaheuristics. The imple-
mentation of algorithms, test problems, and visualisa-
tions can be downloaded at xxx.
1
SA and PSO Algorithms.The complexity of prob-
lems in the HHC domain means that there is scope
for the application of metaheuristics (Liu et al., 2021;
Hiermann et al., 2015; Goodarzian et al., 2021).
We consider the application of two well-known and
widely used algorithms to solve problems of the type
considered here, SA and PSO (Kennedy and Eberhart,
1995). SA has shown to be a promising approach for
discrete mathematical problems (Yuan et al., 2009),
while PSO was originally proposed for continuous
problems but has been adapted to different types of
problems since then. In our case, each discrete vari-
able is represented by a binary string, which means
that our PSO algorithm searches over a binary space.
In solving the problem, these algorithms use the same
approach to create an initial solution. The results of
these two metaheuristics are then compared with the
1
The link will be made available upon acceptance of the
paper.
ECTA 2024 - 16th International Conference on Evolutionary Computation Theory and Applications
76

baseline using the GAMS CPLEX solver in terms of
the improved performance of the proposed HHC plan.
Penalization is used as the constraint-handling strat-
egy with the penalty term simply counting the number
of violated constraints; more advanced strategies are
part of future research.
CPSO Algorithm. CPSO (He and Wang, 2007) is
a multi-population version of classic PSO aimed at
tackling complex multi-modal problems more effi-
ciently. This is addressed for the first time in (He
and Wang, 2007). CPSO uses multiple populations of
particles, allowing the algorithm to explore the search
space more thoroughly and find a better balance be-
tween exploitation and exploration. The chromosome
design is shown below:
According to Figure 1, a chromosome represents
a set of patients who must be served by an expert with
a corresponding service level. This will form a set of
patients (P) followed by experts (E), in which they
must be served according to their service menu (S).
To form this, a heuristic method based on the stair-
case method is applied using the north-west corner.
Based on this method, suppliers (experts) and cus-
tomers at demand points (patients) form a matrix in
which their demands must be met given their required
services (Holmberg and Ling, 1997). This method
guarantees the feasibility of the HHC plan and as-
signs each expert to a patient based on their daily
needs (Bazaraa et al., 2011). Therefore, multiple rows
are formed based on the total number of patients and
experts in the HHC, as shown in Figure 1. To simplify
services and differentiate them, services 1 through 3
are denoted by A,B, and C. Consequently, a corre-
sponding value of 0 and 1 is assigned to show whether
a patient needs a certain service or not (for example,
AB equals (1,1,0), showing that the patient requires
services one and two). Based on the north-west corner
method, experts are assigned to patients to fully meet
their demands. The north-west corner method works
as follows: A matrix is created in which rows respon-
sible for experts and columns are responsible for pa-
tients. each cell of the matrix represents the allocation
of experts to patients. The method begins with the
north-west corner of the matrix and allocates the units
as much as possible, then it moves to the next row, this
process is continues until the resources are exhaust in
each row and assignments are done. Given an hour to
complete each task, the assigned patients and their re-
quired time for treatment form the right-hand side of
the expert column. Finally, the assignment of each ex-
pert is shown. Once allocated (red brackets) using the
north-west corner, the required skills are assigned and
therefore deducted from the PSM. This process will
continue until every patient has an assigned expert to
visit.
Figure 1: Representation of chromosome and allocation of
experts using heuristic staircase method (P: Patients; E: Ex-
perts; PSM: Patient’s Service Menu (a tuple consisting of 0
and 1 digit, representing three services); EE: Expert’s Ex-
pertise, (eight patients, four experts, and three services)).
Table 2: Parameter setting for SA, PSO, and CPSO algo-
rithms.
Alg. Parameter Setting
SA Maximum iteration MaxIt 100
Sub iteration SubIt 50
Initial Temperature 15000
Rate of reduction 0.99
PSO & Population size N 100
CPSO Interia weight W 1
Weight Damping Ratio W damp 0.99
Accelaration coefficient c
1
1.3
Accelaration coefficient c
2
1.3
Internal swarm value (CPSO) w
1
0.22
External swarm value (CPSO) w
2
0.42
4.2 Test Problems
To better understand the complexity of the problem
and the performance of the solution methods, we
propose case studies (problem instances) of varying
problem sizes and parameter values, including small,
medium, and large problems; in practice, this could
translate to HHC services of varying size (eg due to
geographical differences) (AlayaCare, ). In addition,
the following setting in Table 2 is used for algorithm
parameters:
SA uses a reduction rate of 0.99. The reduction
rate signifies the reduced value of the initial tempera-
ture (15000) in each iteration. In each iteration, a new
solution is found and if the new solution is inferior to
the best solution, then it will be retained as the best so-
lution discovered. Otherwise, exp(−δ/temperature)
is solved, where δ is the difference between the cur-
rent solution and the best solution. The parameters
values are derived from (Kirkpatrick et al., 1983)
as one of the best practices for this problem. For
the CPSO algorithm, the settings have been taken
from (Kou et al., 2009). It must be noted that, to
consider the same condition when evaluating the pro-
posed metaheuristics, the number of function evalua-
tions is set to 1000 as stopping criteria.
The values of the problem parameters can vary
within a range in practice; however, following (Alay-
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care Planning
77

aCare, ) we set the parameters as follows: TrT
i, j
= 25,
LV
i
= 18, ViT
i
= 65, Lim
Tr
= 75, PT = 300, DU
max
=
45, EV
i
= 10, and λ
i
is verified by our IoMT. The ex-
perimental study presented in the next section will ini-
tially use these settings to evaluate the performance of
each metaheuristic used.
5 EXPERIMENTAL RESULTS
This section evaluates the proposed HHC network for
different problem sizes using various parameter val-
ues and settings. Table 3 displays the mean of the best
objective score (BOS), computational time, and the
standard deviation over 50 runs of the solution meth-
ods. For CPLEX we use the lower bound obtained by
using GAMS.
Table 3 Column 1 contains the problem instance’s
identifier, in which the first number is patients, the
second and third are the number of internal and ex-
ternal experts, and the fourth number is the number
of required services. Column 2 presents the lower
bounds for the problem instances that arise from solv-
ing the model using the CPLEX solver in GAMS.The
best results over 50 trials of each algorithm is taken.
The CPU time is in seconds, and the mean standard
deviation is the amount of variation between prob-
lem solutions. It is observed that CPLEX was able
to solve the problem with up to 45 patients, 15 in-
ternal and 8 external caregivers within the time limit
of 7200 seconds. No significant improvement was
observed by increasing the time limit or employing
additional RAM and CPU (the initial computation is
performed on Windows OS 10, 16 Gigabyte RAM,
and 4 Gigabyte GPU). However, SA was able to solve
the problem faster, especially for larger problems.
PSO needed more CPU time and achieved a lower
BOS when compared to SA. However, in the case
of CPSO, the results are more promising. For prob-
lems in which 15 and 10 internal and external home
caregivers we employed to serve 35 and 45 patients,
CPSO showed better results compared to both SA and
PSO. Moreover, the mean CPU time to find the best
solution and the standard deviation for CPSO is sig-
nificantly shorter compared to the SA algorithm.
Figure 2 shows the variance of the BOS obtained
in 50 runs for the metaheuristics (CPLEX is determin-
istic). For small problems (Samples 1-4) (Figure (a)),
both the SA and CPSO algorithm work well in terms
of the optimal solution. Furthermore, PSO presented
a good solution and, with a slight difference, placed it-
self after SA and CPSO. For medium-sized problems
(Samples 5-10) (Figure (b)), the SA algorithm is sta-
tistically the best performing algorithm among meta-
(a)
(b)
(c)
Figure 2: Box plot of the different metaheuristics (a) small
(Samples 1-4), (b) medium (Samples 5-10), (c) large (Sam-
ples 11-16).
heuristics and in some samples close to the CPLEX
results. It is interesting to note that the CPSO algo-
rithm provides the second-best solution. However, for
large problems (Samples 11-16) (Figure (c)), CPSO is
able to obtain a good objective function solution with
a relatively lower standard deviation value compared
to SA and PSO. It might be noted that the CPSO takes
slightly higher computational time than SA and PSO,
due to the additional operators which CPSO employs
for obtaining a good solution in every test run. The
additional operators helps to obtain a better solution
in every test run, and hence the standard deviation is
higher for 50 trials compared to SA and PSO. In three
larger problem instances, CPLEX was unable to ob-
tain a result in the given 7200 seconds (as indicated
by ‘-’ in the table). Also, the convergence plot in
Figure 3 indicates that all algorithms have a similar
convergence behaviour with SA converging slightly
faster than others.
The current study uses three metaheuristics, which
are compared in a paired fashion, and performance
outputs do not follow a normal distribution. There-
fore, we can use the Friedman’s test (Marusteri and
ECTA 2024 - 16th International Conference on Evolutionary Computation Theory and Applications
78
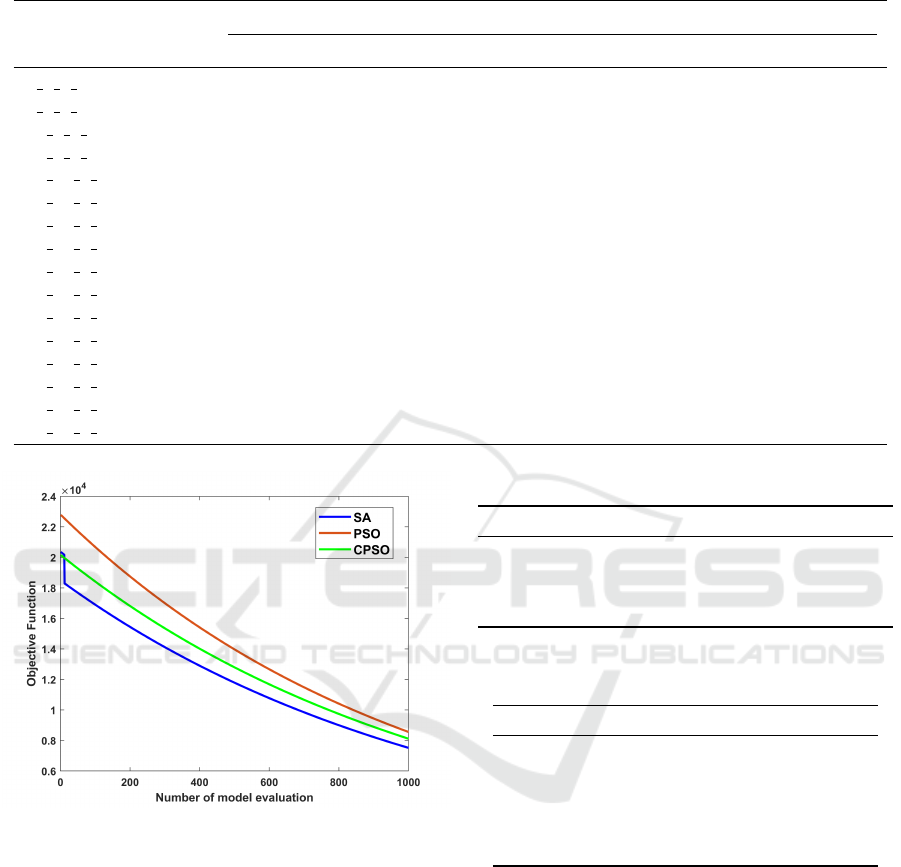
Table 3: Summary of the average result obtained from different algorithms for set
1
instance over 50 runs (Instance ID,
respectively: Number of patients, internal experts, external experts, required services; CPLEX: The lower bound from GAMS;
BOS: Best objective score; Std.dv: The standard deviation; Time: Computational time in seconds.)
Instance ID CPLEX SA PSO CPSO
BOS Std.dv Time BOS Std.dv Time BOS Std.dv Time
6 2 2 5 311.2 323.2 1.1 25.3 323.7 4.1 32.5 317.7 4.8 24.1
6 3 3 5 331.4 350.6 2.2 37.3 359.9 2.1 41.1 353.8 2.6 35.1
10 2 2 5 350.3 363.7 4.2 39.6 374.8 4.3 51.1 369.4 5.4 40.1
10 3 3 5 371.4 380.1 2.8 35.3 382.8 5.1 64.1 368.7 9.9 38.1
15 10 5 5 2264.8 2149.5 51.4 437.7 2252.9 26.4 512.6 2248.1 11.5 412.7
15 15 8 5 2353.9 2333.2 45.1 354.5 2395.1 27.4 408.9 2357.8 35.6 418.1
25 10 5 5 2430.8 2437.8 46.7 323.4 2467.4 47.5 503.2 2458.3 52 400.4
25 15 8 5 2562.6 2568.4 38.3 447.7 2588.9 26.9 506.7 2586.5 27.9 423.1
35 10 5 5 2704.2 2718.3 17.9 444.2 2759.8 40.8 478.8 2757.1 37.6 443.1
35 15 8 5 2956.5 2965.9 52.2 451.3 2990.4 51.9 504.3 2962.8 55.3 521.1
45 10 5 5 8099.1 6237.1 59.4 439.6 6280.1 87.9 401.5 6285.9 72.6 420.8
45 15 8 5 - 6132.3 101.6 455.6 6143.1 96.9 549.3 6142.8 105.4 513.5
65 10 5 5 10033.3 6830.7 34.7 424.5 6882.1 38.7 554.2 6876.6 32.5 418.4
65 15 8 5 - 6822.5 49.1 490.3 6891.1 58.8 497.5 6932.3 47.7 478.1
85 10 5 5 19092.8 7023.1 97.5 486.2 7307.1 47.7 507.3 7300.6 52.1 462.9
85 15 8 5 - 7838.4 50.3 438.5 7903.9 89.7 472.5 7907.2 44.9 487.1
Figure 3: Convergent level of the metaheuristic algorithms
based on objective function and number of model evaluation
for large (85-15-8-5 problem).
Bacarea, 2010) to determine whether there are statisti-
cally significant differences among the performances
of these algorithms. Table 4 shows the result of the
Friedman’s test for the metaheuristics considering the
large problem (to evaluate the performance of the al-
gorithms in real-world-size problems), which had the
greatest impact on algorithm performance, consisting
of 85 patients, 15 internal and 8 external experts, with
a significance level equal to 0.05. Since the p − value
is less than the significance level, the result implies
that there is a significant difference in the perfor-
mance of these algorithms.
Table 4: Friedman’s ANOVA for significance level 0.05.
Source SS df MS Chi-sq Prob>Chi-sq
Columns 171.04 2 85.52 48.87 2.44526e-11
Interaction 98.96 48 2.0617
Error 167.5 75 2.2333
Total 437.5 149
Table 5: Sensitivity analysis on PSM (Before the IoMT
plan).
Scenario A (Before) Visit time
Before any changes (A-a) 734
Changes four hours before IoMT plan starts (A-b) 734
Changes three hours before IoMT plan starts (A-c) 760
Changes two hours before IoMT plan starts 760
Changes one hour before IoMT plan starts 760
Changes one hour without IoMT plan 789
5.1 A More in Depth Analysis of a
Single Case Study
The HHC centre service menu is shown in Table 6.
In addition, Expert’s skills can be summarised as fol-
lows: Expert 1 (S1,S2,S4), Expert 2: (S2,S4,S5), Ex-
pert 3: (S1,S2,S3,S4), Expert 4: (S2,S3,S4,S5), Ex-
pert 5: (S5), Expert 6: (S1-S5), Expert 7: (S2,S4,S5),
Expert 8: (S5), Expert 9: (S1,S2,S3,S4), Expert 10:
(S1-S5). S1-S5 defines their ability to perform a ser-
vice.
Table 6 assumes that patients (1–15) are chosen
from a group of patients with INT
i
≥ λ
i
. The real-life
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care Planning
79

Figure 4: Patient’s visitation sequence and assignments of experts to patients in scenario A; A-a: Before any change; A-b:
Changes four hours before the start of IoMT plan; A-c: Changes three hours before the start of IoMT plan (E: Internal experts;
EE: External experts; P: Patients; ST: Start time; FT: Finish time).
experience of similar HHC companies (AlayaCare, )
combined with available resources motivated this ar-
ticle to use current settings.
Table 6: PSM; P:Patients; S: Services; λ: Current condition
of each patient.
ID λ S1 S2 S3 S4 S5 Time Window
P1 0.86 1 1 0 1 0 (11:00-16:00)
P2 0.95 0 0 1 1 0 (16:00-22:00)
P3 0.92 1 1 1 0 1 (10:00-15:00)
P4 0.99 1 0 1 1 0 (9:00-22:00)
P5 0.94 0 0 0 0 1 (9:00-17:00)
P6 0.78 0 0 1 0 0 (9:00-15:00)
P7 0.99 0 0 0 1 0 (15:00-19:00)
P8 0.78 0 1 1 0 0 (9:00-12:00)
P9 0.93 0 0 0 0 1 (13:00-16:00)
P10 0.82 0 0 1 1 0 (11:00-21:00)
P11 0.98 0 1 0 1 0 (13:00-20:00)
P12 0.95 1 0 0 1 0 (8:00-19:00)
P13 0.78 1 0 0 1 0 (11:00-20:00)
P14 0.76 0 0 1 1 0 (10:00-21:00)
P15 0.84 0 1 0 0 1 (13:00-22:00)
Using the large problem settings and CPSO algo-
rithm, the scheduling plan and optimal solutions are
presented in Table 7. It shows the expert’s alloca-
tion to the patients alongside their intervals. In ad-
dition, the visitation time of each expert for the entire
day (including start and finish times for each expert;
10 experts, 15 patients, and 5 services) is provided.
Table 7: The IoMT plan and assignment of experts for E:10,
P:15, and S:5.
Assignments Visitation Intervals
Expert 9 (11:00-16:00) P1 → P13
Expert 6 (10:00-18:00) P3 → P2
Expert 3 (9:00-12:00) P4
Expert 10 (9:00-18:00) P5 → P8 → P11 → P12 → P14
Expert 4 (9:00-13:00) P6 → P10
Expert 2 (15:00-20:00) P7 → P15
Expert 7 (13:00-14:00) P9
Given the skill level and time window of both patients
and experts, it is clear that expert 10 visits most of the
patients, while other experts are only eligible to visit
either one or two patients within the considered plan.
5.2 Sensitivity Analyses Based on IoMT
Real-Time Changes
The proposed IoMT plan considers three phases, in-
cluding service installation, diagnosis, and perform-
ing home care for patients. System installation is per-
formed using wireless wearable sensors and the con-
dition of the patients is monitored in real time. The
plan is dynamically responsive to changes and offers
a new plan rapidly when a change occurs. Here, sce-
nario A is defined as follows: In scenario A, we con-
sider that a change has occurred in the PSM before the
ECTA 2024 - 16th International Conference on Evolutionary Computation Theory and Applications
80

plan starts. In this scenario, it is assumed that patient
4 (P4) has changed their service plan from (10110)
to (11110), which means that this patient changed his
services from services 1, 3, and 4 to services 1, 2, 3,
and 4 before the start of the IoMT plan.
Based on Figure 4 and Table 5, the sensitivity
analysis is conducted on the original plan, consider-
ing the change in PSM for patient 4. Changes are ob-
served four to one hour before the IoMT plan starts. In
addition, the original plan (A-a), changes four hours
before the start of the IoMT plan (A-b), changes three
hours before the start of the IoMT plan (A-c), changes
two hours before the start of the IoMT plan, and
changes one hour before the start of the IoMT plan
are identified in this table. Four hours before the plan
starts, the assignments are distributed with more flex-
ibility and a reduction in total visitation time is ob-
served. Last but not least, the problem shows a 3.7
percent difference from the original IoMT plan, con-
sidering one hour before changes and no IoMT plan
is implemented ((788-760)/760=0.037).
By tightening this time to three and two hours,
fewer options remain to assign experts to care for pa-
tients; therefore, an increase in total visitation time
is predictable (see Figure 4 (A-b)). Here, the model
avoided ignoring patient 11 and tried to assign it to
an expert. Since the model assigned E8 to this patient
in Figure 4 (A-c), the patients previously assigned to
internal experts now must be assigned to external ex-
perts for visitation; therefore, an increase in total vis-
itation time has occurred here. One hour before the
start of the IoMT plan, the total visitation time re-
mains constant since there is no flexibility to change
the sequence of assignments based on the patient’s
service menu and time window. It is observed from
this figure that even a slight change in PSM can ulti-
mately result in allocation of different experts or util-
isation of more external experts, which may result in
an increase in the total number of visitation hours in a
daily HHC plan. Another interesting point to mention
here is the CPSO’s role to respond (re-solve) the prob-
lem when having immediate changes. The algorithm
updates the input according to the current changes
and solves the new problem in the least possible time.
This shows the adaptability and responsiveness of the
proposed algorithm and the suggested IoMT plan to
any real-time changes.
6 CONCLUSIONS AND FUTURE
WORK
The proposed IoMT methodology controls, monitors
and records the real-time condition of patients. A
structured plan by IoMT is suggested to assign the
optimal number of experts to a set of available home
carers. Real-time monitoring of a patient’s condition
is a crucial tool for HHC managers to identify current
and real-time conditions and decide accordingly how
to react. If changes occur before the plan, the changes
can be made only three hours in advance. However,
applying instant changes is more challenging during
the final hours, when many patients are scheduled to
be visited by experts.
The experiments carried out revealed that the
HHC planning problem is difficult due to the large
number of variables and constraints. In addition, us-
ing multiple metaheuristics allowed us to evaluate the
efficiency of the methods under various conditions
and settings. SA and CPSO both proved to be ef-
ficient when faced with medium-sized problems. In
terms of dealing with large problems, CPSO has been
statistically proven to be better. In terms of objective
function of the problem, both SA and CPSO have sim-
ilar results, with SA slightly working better; however,
by the means of the overall time spent to reach their
best solutions, CPSO performed better when CPLEX
was bound to 7200 seconds in large-size problems.
This result can be meaningful, especially when work-
ing with patients with more serious symptoms.
The current results of the problem enable man-
agers to make better decisions in severe conditions.
Considering real-time changes, it adds another layer
of credibility and reliability among the patients and
the HHC’s medical staff. This study sets the ground-
work for future research to evaluate optimal experts
for the IoMT plan. Future work will look at find-
ing a more efficient way to optimise the HHC prob-
lem. In addition, the mathematical formulation can
be extended to include external experts, risk-related
elements, and algorithm’s parameter adjustments.
REFERENCES
Ait Haddadene, S. R., Labadie, N., and Prodhon, C. (2019).
Bicriteria vehicle routing problem with preferences
and timing constraints in home health care services.
Algorithms, 12(8):152.
AlayaCare, H. H. C. A. personal communication.
Athelas (2003). Digital tools made for modern healthcare
organisations. http://https://www.athelas.com/.
Bahadori-Chinibelagh, S., Fathollahi-Fard, A. M., and
Hajiaghaei-Keshteli, M. (2022). Two constructive
algorithms to address a multi-depot home health-
care routing problem. IETE Journal of Research,
68(2):1108–1114.
Bazaraa, M. S., Jarvis, J. J., and Sherali, H. D. (2011). Lin-
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care Planning
81

ear programming and network flows. John Wiley &
Sons.
De Vries, J. and Huijsman, R. (2011). Supply chain man-
agement in health services: an overview. Supply chain
management: An international journal, 16(3):159–
165.
Decerle, J., Grunder, O., El Hassani, A. H., and Barakat, O.
(2018). A memetic algorithm for a home health care
routing and scheduling problem. Operations research
for health care, 16:59–71.
Decerle, J., Grunder, O., El Hassani, A. H., and Barakat, O.
(2019a). A hybrid memetic-ant colony optimization
algorithm for the home health care problem with time
window, synchronization and working time balancing.
Swarm and Evolutionary Computation, 46:171–183.
Decerle, J., Grunder, O., El Hassani, A. H., and Barakat,
O. (2019b). A memetic algorithm for multi-objective
optimization of the home health care problem. Swarm
and evolutionary computation, 44:712–727.
Di Mascolo, M., Martinez, C., and Espinouse, M.-L.
(2021). Routing and scheduling in home health care:
A literature survey and bibliometric analysis. Com-
puters & Industrial Engineering, 158:107255.
Dwivedi, R., Mehrotra, D., and Chandra, S. (2021). Poten-
tial of internet of medical things (iomt) applications
in building a smart healthcare system: A systematic
review. Journal of oral biology and craniofacial re-
search.
Dwivedi, R., Mehrotra, D., and Chandra, S. (2022). Poten-
tial of internet of medical things (iomt) applications
in building a smart healthcare system: A systematic
review. Journal of oral biology and craniofacial re-
search, 12(2):302–318.
Emiliano, W., Telhada, J., and do Sameiro Carvalho, M.
(2017). Home health care logistics planning: a review
and framework. Procedia Manufacturing, 13:948–
955.
Erdem, M. and Koc¸, C¸ . (2019). Analysis of electric vehi-
cles in home health care routing problem. Journal of
Cleaner Production, 234:1471–1483.
Erdem, M. and Koc¸, C¸ . (2022). Home health care and dialy-
sis routing with electric vehicles and private and pub-
lic charging stations. Transportation Letters, pages
1–16.
Fathollahi-Fard, A. M., Hajiaghaei-Keshteli, M., and
Tavakkoli-Moghaddam, R. (2018). A bi-objective
green home health care routing problem. Journal of
Cleaner Production, 200:423–443.
Fathollahi-Fard, A. M., Hajiaghaei-Keshteli, M., Tavakkoli-
Moghaddam, R., and Smith, N. R. (2022). Bi-level
programming for home health care supply chain con-
sidering outsourcing. Journal of Industrial Informa-
tion Integration, 25:100246.
Fikar, C. and Hirsch, P. (2017). Home health care routing
and scheduling: A review. Computers & Operations
Research, 77:86–95.
Goodarzian, F., Abraham, A., and Fathollahi-Fard, A. M.
(2021). A biobjective home health care logistics con-
sidering the working time and route balancing: a
self-adaptive social engineering optimizer. Journal
of Computational Design and Engineering, 8(1):452–
474.
He, Q. and Wang, L. (2007). An effective co-evolutionary
particle swarm optimization for constrained engineer-
ing design problems. Engineering applications of ar-
tificial intelligence, 20(1):89–99.
Hiermann, G., Prandtstetter, M., Rendl, A., Puchinger, J.,
and Raidl, G. R. (2015). Metaheuristics for solv-
ing a multimodal home-healthcare scheduling prob-
lem. Central European Journal of Operations Re-
search, 23(1):89–113.
Holmberg, K. and Ling, J. (1997). A lagrangean heuristic
for the facility location problem with staircase costs.
European journal of operational research, 97(1):63–
74.
Kennedy, J. and Eberhart, R. (1995). Particle swarm opti-
mization. In Proceedings of ICNN’95-international
conference on neural networks, volume 4, pages
1942–1948. IEEE.
Khodabandeh, P., Kayvanfar, V., Rafiee, M., and Werner,
F. (2021). A bi-objective home health care routing
and scheduling model with considering nurse down-
grading costs. International Journal of Environmental
Research and Public Health, 18(3):900.
Kirkpatrick, S., Gelatt Jr, C. D., and Vecchi, M. P.
(1983). Optimization by simulated annealing. science,
220(4598):671–680.
Kou, X., Liu, S., Zhang, J., and Zheng, W. (2009). Co-
evolutionary particle swarm optimization to solve
constrained optimization problems. Computers
& Mathematics with Applications, 57(11-12):1776–
1784.
Landers, S., Madigan, E., Leff, B., Rosati, R. J., Mc-
Cann, B. A., Hornbake, R., MacMillan, R., Jones, K.,
Bowles, K., Dowding, D., et al. (2016). The future of
home health care: a strategic framework for optimiz-
ing value. Home health care management & practice,
28(4):262–278.
Lin, C.-C., Hung, L.-P., Liu, W.-Y., and Tsai, M.-C.
(2018). Jointly rostering, routing, and rerostering for
home health care services: A harmony search ap-
proach with genetic, saturation, inheritance, and im-
migrant schemes. Computers & Industrial Engineer-
ing, 115:151–166.
Liu, W., Dridi, M., Fei, H., and El Hassani, A. H. (2021).
Hybrid metaheuristics for solving a home health care
routing and scheduling problem with time windows,
synchronized visits and lunch breaks. Expert Systems
with Applications, 183:115307.
Marusteri, M. and Bacarea, V. (2010). Comparing groups
for statistical differences: how to choose the right sta-
tistical test? Biochemia medica, 20(1):15–32.
McGillion, M., Ouellette, C., Good, A., Bird, M., Henry,
S., Clyne, W., Turner, A., Ritvo, P., Ritvo, S., Dvirnik,
N., et al. (2020). Postoperative remote automated
monitoring and virtual hospital-to-home care system
following cardiac and major vascular surgery: user
testing study. Journal of Medical Internet Research,
22(3):e15548.
ECTA 2024 - 16th International Conference on Evolutionary Computation Theory and Applications
82

Nikzad, E., Bashiri, M., and Abbasi, B. (2021). A
matheuristic algorithm for stochastic home health care
planning. European Journal of Operational Research,
288(3):753–774.
Polisena, J., Tran, K., Cimon, K., Hutton, B., McGill, S.,
Palmer, K., and Scott, R. E. (2010). Home telemoni-
toring for congestive heart failure: a systematic review
and meta-analysis. Journal of telemedicine and tele-
care, 16(2):68–76.
Reddy, K. N., Kumar, A., Choudhary, A., and Cheng, T. E.
(2022). Multi-period green reverse logistics network
design: An improved benders-decomposition-based
heuristic approach. European Journal of Operational
Research.
Restrepo, M. I., Rousseau, L.-M., and Vall
´
ee, J. (2020).
Home healthcare integrated staffing and scheduling.
Omega, 95:102057.
Rodriguez-Verjan, C., Augusto, V., and Xie, X. (2018).
Home health-care network design: Location and con-
figuration of home health-care centers. Operations re-
search for health care, 17:28–41.
Shi, Y., Boudouh, T., and Grunder, O. (2019). A robust op-
timization for a home health care routing and schedul-
ing problem with consideration of uncertain travel and
service times. Transportation Research Part E: Logis-
tics and Transportation Review, 128:52–95.
Statista (2020). Home health care demand.
Vervoort, D., Guetter, C. R., and Peters, A. W. (2021).
Blockchain, health disparities and global health. BMJ
Innov, 7(2):506–514.
Xiang, T., Li, Y., and Szeto, W. Y. (2023). The daily
routing and scheduling problem of home health care:
based on costs and participants’ preference satisfac-
tion. International Transactions in Operational Re-
search, 30(1):39–69.
Xiao, L., Dridi, M., and El Hassani, A. H. (2018). Math-
ematical model for the home health care scheduling
and routing problem with flexible lunch break require-
ments. IFAC-PapersOnLine, 51(11):334–339.
Yuan, X., Nie, H., Su, A., Wang, L., and Yuan, Y. (2009).
An improved binary particle swarm optimization for
unit commitment problem. Expert Systems with ap-
plications, 36(4):8049–8055.
Real-Time IoMT-driven Optimisation for Large-Scale Home Health Care Planning
83
